
Sociobehavioral, Biological, and Health Characteristics of Riverside People in the Xingu Region, Pará, Brazil

 and
and
Abstract
1. Introduction
2. Materials and Methods
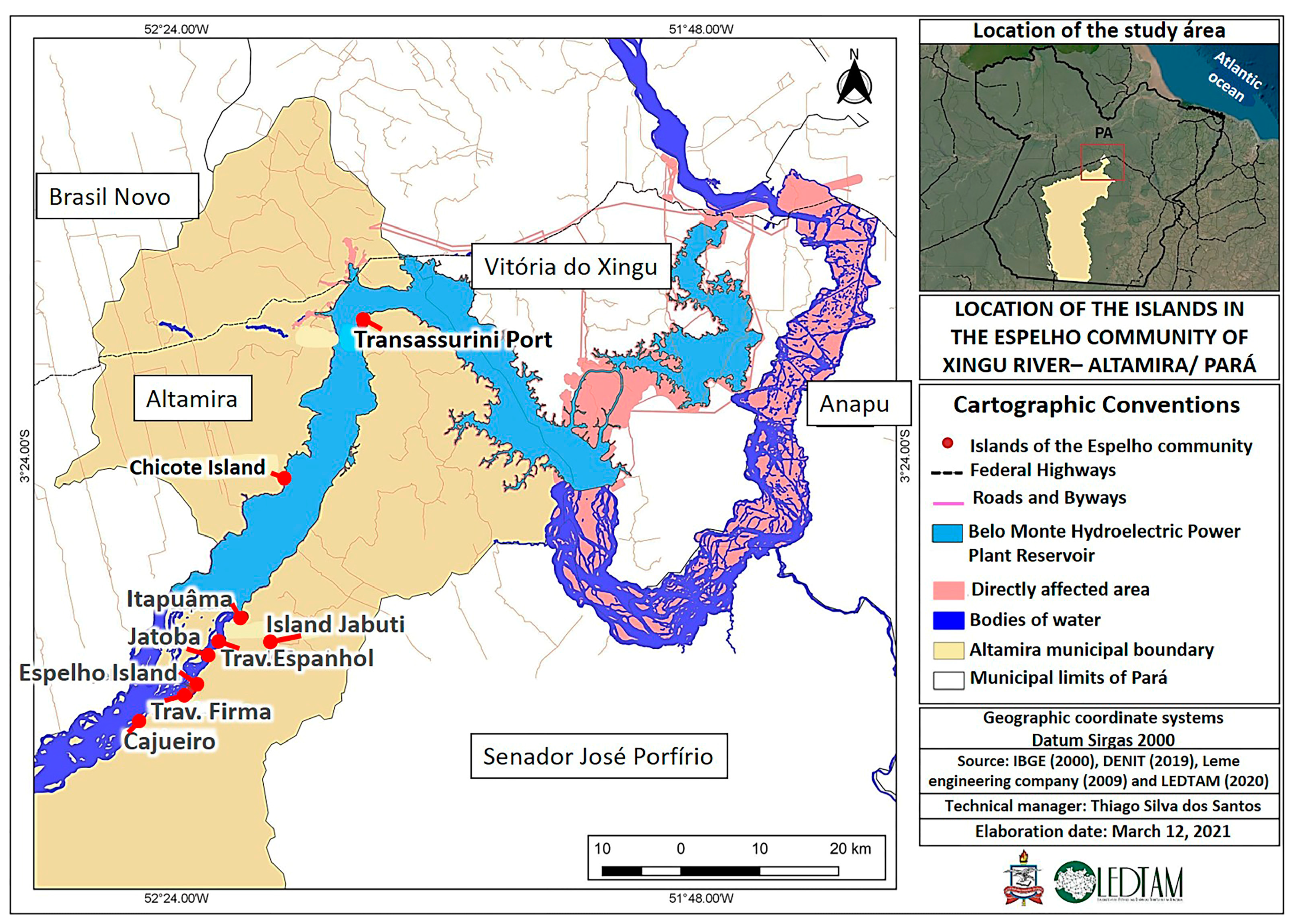
2.1. Participants
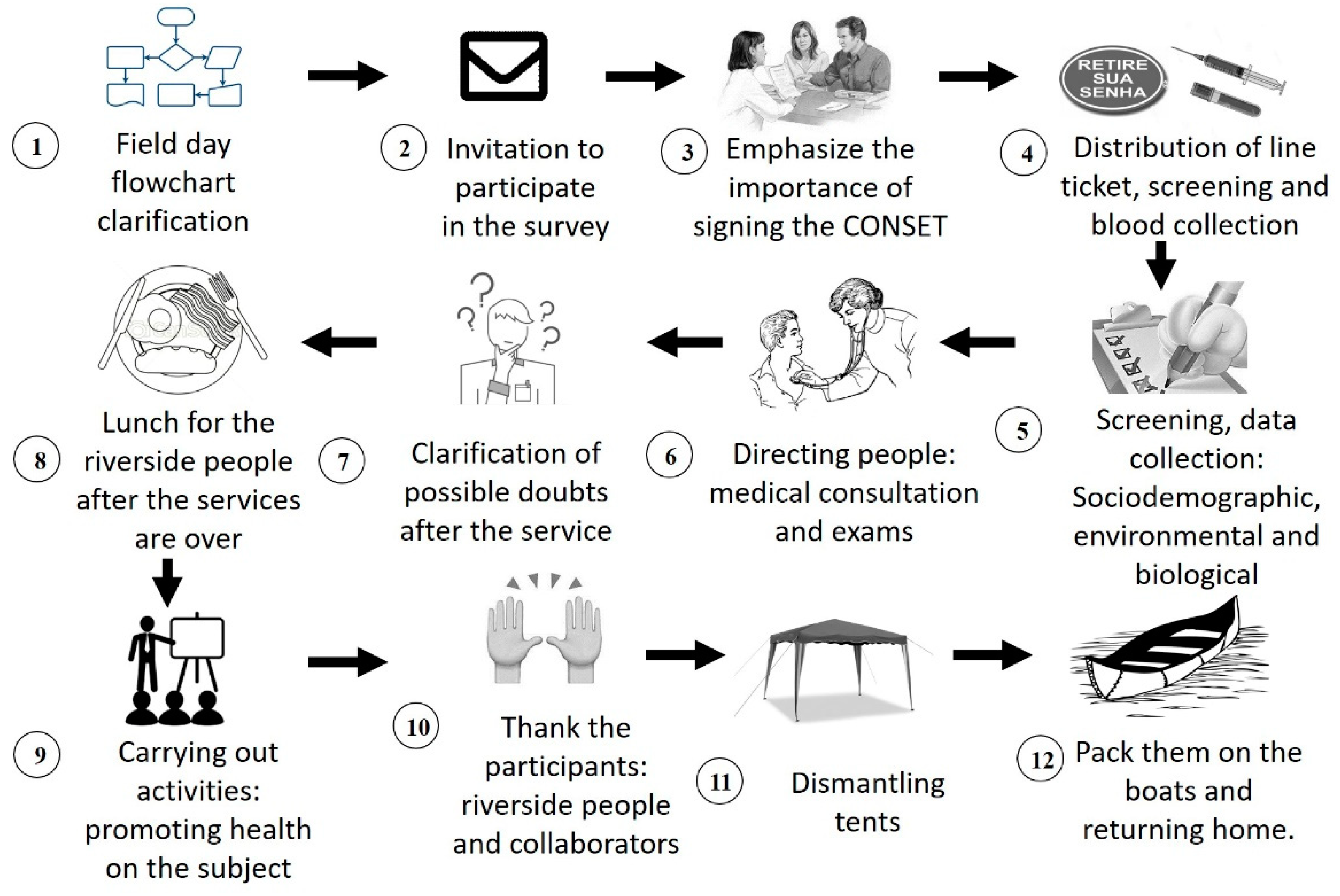
2.2. Procedures
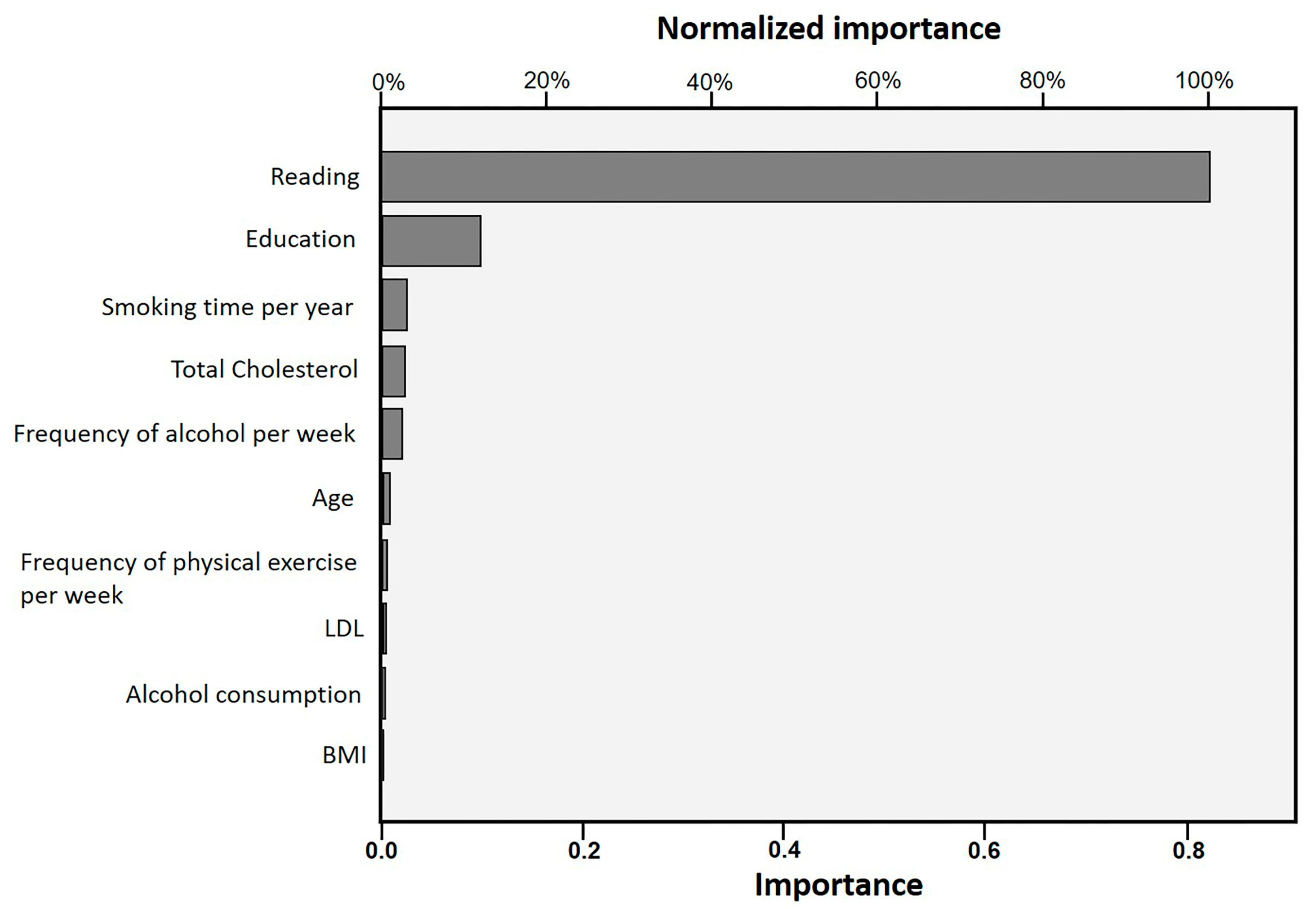
2.3. Data Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brasil, M.S. Guidelines for the Care of People with Chronic Diseases in Health Care Networks and in Priority Lines of Care; Health Care Department, Department of Primary Care, Ministry of Health Brasilia: Brasilia, Brazil, 2013. Available online: https://bvsms.saude.gov.br/bvs/publicacoes/diretrizes%20_cuidado_pessoas%20_doencas_cronicas.pdf (accessed on 15 January 2021).
- GBD. Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [PubMed]
- Singhal, A. The global epidemic of noncommunicable disease: The role of early-life factors. J. Int. Nutr. Achiev. Millenn. Goals Beyond 2014, 78, 123–132. [Google Scholar] [CrossRef]
- Oliveira, B.F.A.; Mourão, D.S.; Gomes, N.; Costa, J.M.C.; Souza, A.V.; Bastos, W.R.; Fonseca, M.F.; Mariani, C.F.; Abbad, G.; Hacon, S.S. Prevalence of arterial hypertension in riverside communities on the Madeira River, Western Brazilian Amazon. J. Cad. De Saude Publica 2013, 29, 1617–1630. [Google Scholar] [CrossRef]
- Hacon, S.S.; Dórea, J.G.; Fonseca, M.F.; Oliveira, B.A.; Mourão, D.S.; Ruiz, C.; Gonçalves, R.A.; Mariani, C.F.; Bastos, W.R. The influence of changes in lifestyle and mercury exposure in riverine populations of the Madeira River (Amazon Basin) near a hydroelectric project. Int. J. Environ. Res. Public Health 2014, 11, 2437–2455. [Google Scholar] [CrossRef] [PubMed]
- Arrifano, G.P.F.; Martin-Doimeadios, R.D.C.R.; Jiménez-Moreno, M.; Augusto-Oliveira, M.; Souza-Monteiro, J.R.; Paraense, R.; Machado, C.R.; Farina, M.; Macchi, B.; Do Nascimento, J.L.M. Assessing mercury intoxication in isolated/remote populations: Increased S100B mRNA in blood in exposed riverine inhabitants of the Amazon. J. Neurotoxicol. 2018, 68, 151–158. [Google Scholar] [CrossRef]
- Franco, E.C.; Santo, C.E.; Arakawa, A.M.; Xavier, A.; França, M.d.L.; De Oliveira, A.N.; Machado, M.A.M.P.; Bastos, R.S.; Bastos, J.R.M.; Caldana, M.L. Health promotion on amazonic riverside population: Experience report. J. Rev. CEFAC 2015, 17, 1521–1530. [Google Scholar] [CrossRef]
- Gama, A.S.M.; Fernandes, T.G.; Parente, R.C.P.; Secoli, S.R. Health survey in riverside communities in Amazonas, Brazil. J. Cad. De Saúde Pública 2018, 34, e00002817. [Google Scholar] [CrossRef]
- Magalhães, S.B.; Cunha, M.C. Study on the Compulsory Displacement of Riverside Dwellers in Belo Monte: SBPC Report; SBPC: São Paulo, Brazil, 2017; p. 448. Available online: http://portal.sbpcnet.org.br/publicacoes/a-expulsao-de-ribeirinhos-em-belo-monte-relatorio-da-sbpc (accessed on 1 November 2022).
- Santos Sousa, I.; Sousa, F.C.; Sousa, R.M.S. Living condition and water and sanitary situation in communities in the sphere of incluence of the gas pipeline Coari-Manaus in Macacapuru, state of Amazon, Brazil. J. Hygeia-Rev. Bras. De Geogr. Médica E Da Saúde 2009, 5, 88–98. [Google Scholar]
- Weißermel, S. Towards a conceptual understanding of dispossession—Belo Monte and the precarization of the riverine people. J. Novos Cad. NAEA 2020, 23, 11–34. [Google Scholar] [CrossRef]
- Gonçalves, A.C.O.; Cornetta, A.; Alves, F.; Barbosa, L.J.G. Belém and Abaetetuba. In The Socio-Environmental Function of the Union’s Heritage in the Amazon; Alves, F., Ed.; Instituto de Pesquisa Econômica Aplicada (Ipea): Brasília, Brazil, 2016; p. 359. Available online: http://repositorio.ipea.gov.br/handle/11058/6619 (accessed on 14 November 2022).
- Lucas, E.W.M.; De Sousa, F.A.S.; Dos Santos, F.D.S.; Rocha-Júnior, R.L.; Pinto, D.D.C.; Da Silva, V.P.R. Trends in climate extreme indices assessed in the Xingu river basin-Brazilian Amazon. J. Weather Clim. Extrem. 2021, 31, 100306. [Google Scholar] [CrossRef]
- Siqueira, J.M.; Dal’Asta, A.P.; Amaral, S.; Escada, M.I.S.; Monteiro, A.M.V. The Middle and Lower Xingu: The response to the crystallization of different temporalities in the production of regional space. J. Rev. Bras. De Estud. Urbanos E Reg. 2017, 19, 148–163. [Google Scholar] [CrossRef]
- De Francesco, A.; Carneirom, C. Atlas of the Impacts of HPP Belo Monte on Fisheries; Socio-Environmental Institute: São Paulo, Brazil, 2015; Available online: https://ox.socioambiental.org/sites/default/files/ficha-tecnica/node/202/edit/2018-06/atlas-pesca-bm.pdf (accessed on 21 June 2021).
- Silveira, M. The Implementation of Hydroelectric Plants in the Brazilian Amazon, Socio-Environmental and Health Impacts with the Transformations in the Territory: The Case of the Belo Monte HPP. Ph.D. Thesis, University of Brasilia, Brasilia, Brazil, 2016. Available online: https://repositorio.unb.br/handle/10482/20534 (accessed on 5 June 2021).
- Brasil, M.S. The National Policy for the Comprehensive Health of Rural, Forest and Water Populations and the Environment; Support for Participatory Management (DAGEP), Ministry of Health: Brasília, Brazil, 2015. Available online: https://www.arca.fiocruz.br/bitstream/icict/42147/2/Cap_A%20Pol%C3%ADtica%20Nacional%20de%20Sa%C3%BAde%20Integral%20das%20Popula%C3%A7%C3%B5es%20do.pdf (accessed on 14 January 2022).
- Pontes, F.A.R.; Silva, S.S.d.C.; Bucher-Maluschke, J.S.; Reis, D.C.d.; Silva, S.D.B.d. The ecological engagement in the context of an Amazon river Village. Interam. J. Psychol. 2008, 42, 1–10. [Google Scholar]
- De Rodrigues, L.R. Accessibility in the modular teaching organization system in elementary schools in riverside communities in the municipality of Abaetetuba. Braz. J. Dev. 2020, 6, 13147–13161. [Google Scholar] [CrossRef]
- Machado, F.S.N.; de Carvalho, M.A.P.; Mataresi, A.; Mendonça, E.T.; Cardoso, L.M.; Yogi, M.S.; Rigato, H.M.; Salazar, M. Use of telemedicine technology as a strategy to promote health care of riverside communities in the Amazon: Experience with interdisciplinary work, integrating NHS guidelines. J. Cienc. Saude Coletiva 2010, 15, 247–254. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Arrifano, G.P.; Alvarez-Leite, J.I.; Macchi, B.M.; Campos, N.F.; Augusto-Oliveira, M.; Santos-Sacramento, L.; Lopes-Araújo, A.; Souza-Monteiro, J.R.; Alburquerque-Santos, R.; Do Nascimento, J.L.M. Living in the southern hemisphere: Metabolic syndrome and its components in Amazonian riverine populations. J. Clin. Med. 2021, 10, 3630. [Google Scholar] [CrossRef]
- Anjana, R.M.; Baskar, V.; Nair, A.T.N.; Jebarani, S.; Siddiqui, M.K.; Pradeepa, R.; Unnikrishnan, R.; Palmer, C.; Pearson, E.; Mohan, V.; et al. Novel subgroups of type 2 diabetes and their association with microvascular outcomes in an Asian Indian population: A data-driven cluster analysis: The INSPIRED study. BMJ Open Diabetes Res. 2020, 8, e001506. [Google Scholar] [CrossRef] [PubMed]
- Hillesheim, E.; Ryan, M.F.; Gibney, E.; Roche, H.M.; Brennan, L. Optimisation of a metabotype approach to deliver targeted dietary advice. J. Nutr. 2020, 17, 82. [Google Scholar] [CrossRef] [PubMed]
- Tallman, D.A.; Latifi, E.; Kaur, D.; Sulaheen, A.; Ikizler, T.A.; Chinna, K.; Mat Daud, Z.A.; Karupaiah, T.; Khosla, P. Dietary patterns and health outcomes among African American maintenance hemodialysis patients. J. Nutr. 2020, 12, 797. [Google Scholar] [CrossRef] [PubMed]
- Ryan, T.P. Sample Size Determination and Power; John Wiley & Sons: Hoboken, NJ, USA, 2013; p. 400. ISBN 1118439241. [Google Scholar] [CrossRef]
- Yamane, T. Statistics, an Introductory Analysis, 1967; Harper Row Co.: New York, NY, USA, 1967; p. 919. [Google Scholar]
- Cabral, M.M.; Venticinque, E.M.; Rosas, F.C.W. Perception of riverine people in relation to the performance and management of two distinct categories of protected areas in the Brazilian Amazon. J. Biodivers. Bras.-BioBrasil 2014, 1, 199–210. [Google Scholar]
- Feio, C.M.A.; Fonseca, F.A.; Rego, S.S.; Feio, M.N.; Elias, M.C.; Costa, E.A.; Izar, M.C.; Paola, Â.A.; Carvalho, A.C. Lipid profile and cardiovascular risk in Amazonians. Arq. Bras. Cardiol. 2003, 81, 592–595. Available online: https://www.scielo.br/j/abc/a/kcz8gg3kBQQWJyLFbrWKFKw/?format=pdf&lang=pt (accessed on 11 January 2023). [CrossRef]
- Murrieta, R.S.S. Dialectic of flavor: Food, ecology and daily life in riverside communities on the island of Ituqui, Baixo Amazonas, Pará. J. Rev. Antropol. 2001, 44, 39–88. [Google Scholar] [CrossRef]
- Pulvers, K.; Scheuermann, T.S.; Romero, D.R.; Basora, B.; Luo, X.; Ahluwalia, J.S. Classifying a smoker scale in adult daily and nondaily smokers. J. Nicotine Tob. Res. 2014, 16, 591–599. [Google Scholar] [CrossRef]
- SBAC. Brazilian Consensus for the Standardization of Laboratory Determination of Lipid Profile. Brazilian Society of Clinical Analysis. 2016. Available online: https://www.sbac.org.br/blog/2016/12/10/consenso-brasileiro-para-a-normatizacao-da-determinacao-laboratorial-do-per%EF%AC%81l-lipidico/ (accessed on 27 April 2021).
- SBD. Guidelines of the Brazilian Society of Diabetes 2017–2018; Brazilian Society of Diabetes, Publisher Clannad: São Paulo, Brazil, 2017; Available online: https://edisciplinas.usp.br/pluginfile.php/4925460/mod_resource/content/1/diretrizes-sbd-2017-2018.pdf (accessed on 20 April 2021).
- Teknomo, K. K-Means Clustering Tutorials 2007. Available online: http://sigitwidiyanto.staff.gunadarma.ac.id/Downloads/files/38034/M8-NotekMeans (accessed on 5 May 2021).
- Mahmoud, P. K-Means Clustering—Data Algorithms; Beaugureau, A.S.a.M., Ed.; O’Reilly Media, Inc.: Sebastopol, CA, USA, 2015; p. 725. [Google Scholar]
- Chatterji, P.; Joo, H.; Lahiri, K. Racial/ethnic-and education-related disparities in the control of risk factors for cardiovascular disease among individuals with diabetes. Diabetes Care 2012, 35, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Machado, P.A.N.; Sichieri, R. Waist-hip ratio and dietary factors in adults. J. Rev. Saúde Pública 2002, 36, 198–204. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Merz, C.N.B.; Ramineni, T.; Leong, D. Sex-specific risk factors for cardiovascular disease in women-making cardiovascular disease real. J. Curr. Opin. Cardiol. 2018, 33, 500–505. [Google Scholar] [CrossRef]
- Khan, S.U.; Lone, A.N.; Khan, M.S.; Virani, S.S.; Blumenthal, R.S.; Nasir, K.; Miller, M.; Michos, E.D.; Ballantyne, C.M.; Boden, W.E. Effect of omega-3 fatty acids on cardiovascular outcomes: A systematic review and meta-analysis. EClinicalMedicine 2021, 38, 100997. [Google Scholar] [CrossRef] [PubMed]
- Santos-Sacramento, L.; Arrifano, G.P.; Lopes-Araújo, A.; Augusto-Oliveira, M.; Albuquerque-Santos, R.; Takeda, P.Y.; Souza-Monteiro, J.R.; Macchi, B.M.; do Nascimento, J.L.M.; Lima, R.R. Human neurotoxicity of mercury in the Amazon: A scoping review with insights and critical considerations. J. Ecotoxicol. Environ. Saf. 2021, 208, 111686. [Google Scholar] [CrossRef] [PubMed]
- Basta, P.C.; Viana, P.V.d.S.; Vasconcellos, A.C.S.d.; Périssé, A.R.S.; Hofer, C.B.; Paiva, N.S.; Kempton, J.W.; Ciampi de Andrade, D.; Oliveira, R.A.A.d.; Achatz, R.W. Mercury exposure in Munduruku indigenous communities from Brazilian Amazon: Methodological background and an overview of the principal results. Int. J. Environ. Res. Public Health 2021, 18, 9222. [Google Scholar] [CrossRef] [PubMed]
- Meneses, H.N.M.; Oliveira-da-Costa, M.; Basta, P.C.; Morais, C.G.; Pereira, R.J.B.; De Souza, S.M.S.; Hacon, S.S. Mercury contamination: A growing threat to riverine and urban communities in the Brazilian Amazon. Int. J. Environ. Res. Public Health 2022, 19, 2816. [Google Scholar] [CrossRef] [PubMed]
- Souza-Araujo, J.; Andrades, R.; Hauser-Davis, R.; Lima, M.; Giarrizzo, T. Before the Dam: A Fish-Mercury Contamination Baseline Survey at the Xingu River, Amazon Basin before the Belo Monte Dam. J. Bull. Environ. Contam. Toxicol. 2022, 108, 861–866. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Academic Press: Cambridge, MA, USA, 2013; p. 579. ISBN 1483276481. [Google Scholar]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef]
- Russell, S.; Norvig, P. Artificial Intelligence: A Modern Approach, 3rd ed.; Prentice Hall Press: Upper Saddle River, NJ, USA, 2010; p. 1132. ISBN 9780132071482. [Google Scholar]
- SBC. Brazilian Society of Cardiology—7th Brazilian Guideline on Arterial Hypertension. Arq. Bras. Cardiol. 2016, 107, 1–83. Available online: http://publicacoes.cardiol.br/2014/diretrizes/2016/05_HIPERTENSAO_ARTERIAL.pdf (accessed on 3 March 2021).
- WHO. Waist Circumference and Waist—Hip Ratio: Report of a WHO Expert Consultation; World Health Organization: Geneva, Italy, 2008. Available online: https://apps.who.int/iris/bitstream/handle/10665/44583/9789241501491_eng.pdf;jsessionid=2BE502B0C60142042631C73640261857?sequence=1 (accessed on 15 January 2022).
- Mariosa, D.F.; Ferraz, R.R.N.; Santos-Silva, E.N. Influence of socio-environmental conditions on the prevalence of systemic arterial hypertension in two riverside communities in the Amazon, Brazil. J. Ciênc. Saúde Coletiva 2018, 23, 1425–1436. [Google Scholar] [CrossRef]
- Ohlsson, A.; Eckerdal, N.; Lindahl, B.; Hanning, M.; Westerling, R. Non-employment and low educational level as risk factors for inequitable treatment and mortality in heart failure: A population-based cohort study of register data. J. BMC Public Health 2021, 21, 1040. [Google Scholar] [CrossRef] [PubMed]
- Rarau, P.; Pulford, J.; Gouda, H.; Phuanukoonon, S.; Bullen, C.; Scragg, R.; Pham, B.N.; McPake, B.; Oldenburg, B. Socio-economic status and behavioural and cardiovascular risk factors in Papua New Guinea: A cross-sectional survey. PLoS ONE 2019, 14, e0211068. [Google Scholar] [CrossRef]
- Rosengren, A.; Smyth, A.; Rangarajan, S.; Ramasundarahettige, C.; Bangdiwala, S.I.; AlHabib, K.F.; Avezum, A.; Boström, K.B.; Chifamba, J.; Gulec, S. Socioeconomic status and risk of cardiovascular disease in 20 low-income, middle-income, and high-income countries: The Prospective Urban Rural Epidemiologic (PURE) study. Lancet Glob. Health 2019, 7, e748–e760. [Google Scholar] [CrossRef]
- Fard, N.A.; Morales, G.F.; Mejova, Y.; Schifanella, R. On the interplay between educational attainment and nutrition: A spatially-aware perspective. EPJ Data Sci. 2021, 10, 18. [Google Scholar] [CrossRef]
- Arrighi, E.; Ruiz de Castilla, E.; Peres, F.; Mejía, R.; Sørensen, K.; Gunther, C.; Lopez, R.; Myers, L.; Quijada, J.; Vichnin, M. Scoping health literacy in Latin America. Glob. Health Promot. 2022, 29, 78–87. [Google Scholar] [CrossRef]
- De Azevedo, P.L.; Freitas, S.R.S. Prevalence of major cardiometabolic diseases in the riverine populations from the interior of the State of Amazonas, Brazil. Acta Sci. Health Sci. 2018, 40, 34264. [Google Scholar] [CrossRef]
- Machado, C.L.R.; Crespo-Lopez, M.E.; Augusto-Oliveira, M.; Arrifano, G.P.; Macchi, B.M.; Lopes-Araújo, A.; Santos-Sacramento, L.; Souza-Monteiro, J.R.; Alvarez-Leite, J.I.; De Souza, C.B.A. Eating in the Amazon: Nutritional status of the riverine populations and possible nudge interventions. J. Foods 2021, 10, 1015. [Google Scholar] [CrossRef]
- Azevedo, P.L. Prevalence of the Main Chronic Non-Communicable Diseases in Riverside Populations in the Interior of Amazonas. Bachelor’s thesis, State University of Amazonas, Manaus, Brazil, 2017. Available online: http://repositorioinstitucional.uea.edu.br/handle/riuea/523 (accessed on 15 January 2022).
- Relvas, A.; Camargo, J.; Basano, S.; Camargo, L.M.A. Prevalence of chronic noncommunicable diseases and their associated factors in adults over 39 years in riverside population in the western Brazilian amazon region. J. Hum. Growth 2022, 32, 55–63. [Google Scholar] [CrossRef]
- Omare, M.O.; Kibet, J.K.; Cherutoi, J.K.; Kengara, F.O. A review of tobacco abuse and its epidemiological consequences. J. Public Health 2021, 30, 1485–1500. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Burgess, S. Appraising the causal role of smoking in multiple diseases: A systematic review and meta-analysis of Mendelian randomization studies. EBioMedicine 2022, 82, 104154. [Google Scholar] [CrossRef] [PubMed]
- Huerta, M.C.; Borgonovi, F. Education, alcohol use and abuse among young adults in Britain. Soc. Sci. Med. 2010, 71, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Jefferis, B.; Manor, O.; Power, C. Cognitive development in childhood and drinking behaviour over two decades in adulthood. J. Epidemiol. Community Health 2008, 62, 506–512. [Google Scholar] [CrossRef]
- Silva, L.E.S.; Helman, B.; Luz e Silva, D.C.; Aquino, É.C.; Freitas, P.C.; Santos, R.O.; Brito, V.C.A.; Garcia, L.P.; Sardinha, L.M.V. Prevalence of heavy episodic drinking in the Brazilian adult population: National Health Survey 2013 and 2019. J. Epidemiol. E Serviços De Saúde 2022, 31, e2021379. [Google Scholar] [CrossRef]
- Plens, J.A.; Valente, J.Y.; Mari, J.J.; Ferrari, G.; Sanchez, Z.M.; Rezende, L.F. Patterns of alcohol consumption in Brazilian adults. Sci. Rep. 2022, 12, 8603. [Google Scholar] [CrossRef]
- Nogueira, W.P.; Caetano, K.A.A.; Brandão, G.C.G.; Freire, M.E.M.; Reis, R.K.; Oliveira e Silva, A.C. Harmful alcohol consumption and associated factors in riverine communities. Rev. Eletrônica De Enferm. 2022, 24, 68602. [Google Scholar] [CrossRef]
- Macinko, J.; Mullachery, P.; Silver, D.; Jimenez, G.; Neto, O.L.M. Patterns of alcohol consumption and related behaviors in Brazil: Evidence from the 2013 National Health Survey (PNS 2013). PLoS ONE 2015, 10, e0134153. [Google Scholar] [CrossRef]
- Sales, F.M.A.M.; Silva, L.M.C.; Oliveira, A.P.P.; Reis, R.C.; Guerreiro, J.F. Risk of excess weight/body fat and dyslipidemia associated with hemoglobin A2 levels. Rev. Para. De Med. 2014, 28, 57–64. [Google Scholar]
- Adams, C.; Murrieta, R.; Neves, W.A. Amazonian Caboclo Societies: Modernity and Invisibility; Annablume: São Paulo, Brazil, 2006; p. 364. ISBN 8574196444. [Google Scholar]
- Tomita, L.Y.; Cardoso, M.A. Assessment of the food list and serving size of a Food Frequency Questionnaire in an adult population. Cad. De Saúde Pública 2002, 18, 1747–1756. [Google Scholar] [CrossRef]
- Silva, A.L.; Begossi, A. Biodiversity, food consumption and ecological niche dimension: A study case of the riverine populations from the Rio Negro, Amazonia, Brazil. J. Environ. Dev. Sustain. 2009, 11, 489–507. [Google Scholar] [CrossRef]
- Nyberg, S.T.; Singh-Manoux, A.; Pentti, J.; Madsen, I.E.; Sabia, S.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; Goldberg, M. Association of healthy lifestyle with years lived without major chronic diseases. JAMA Intern. Med. 2020, 180, 760–768. [Google Scholar] [CrossRef] [PubMed]
- Peres, M.A.C. Old age and illiteracy, a paradoxical relationship: Educational exclusion in rural contexts in the Northeast region. J. Soc. E Estado 2011, 26, 631–662. [Google Scholar] [CrossRef]
- Vasquez-Rojas, W.V.; Martín, D.; Miralles, B.; Recio, I.; Fornari, T.; Cano, M.P. Composition of Brazil Nut (Bertholletia excels HBK), Its Beverage and By-Products: A Healthy Food and Potential Source of Ingredients. J. Foods 2021, 10, 3007. [Google Scholar] [CrossRef]
- Matos, Â.P.; Matos, A.C.; Moecke, E.H.S. Polyunsaturated fatty acids and nutritional quality of five freshwater fish species cultivated in the western region of Santa Catarina, Brazil. Braz. J. Food Technol. 2019, 22, e2018193. [Google Scholar] [CrossRef]
- Arrifano, G.P.; Martín-Doimeadios, R.C.R.; Jiménez-Moreno, M.; Ramírez-Mateos, V.; da Silva, N.F.; Souza-Monteiro, J.R.; Augusto-Oliveira, M.; Paraense, R.S.; Macchi, B.M.; Do Nascimento, J.L.M. Large-scale projects in the amazon and human exposure to mercury: The case-study of the Tucuruí Dam. J. Ecotoxicol. Environ. Saf. 2018, 147, 299–305. [Google Scholar] [CrossRef]
- Hu, X.F.; Singh, K.; Chan, H.M. Mercury exposure, blood pressure, and hypertension: A systematic review and dose—Response meta-analysis. J. Environ. Health Perspect. 2018, 126, 076002. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Pan, Y.; Tang, Z.; Song, Y. Mercury poisoning presenting with hypertension: Report of 2 cases. Am. J. Med. 2019, 132, 1475–1477. [Google Scholar] [CrossRef]
- Hu, X.F.; Lowe, M.; Chan, H.M. Mercury exposure, cardiovascular disease, and mortality: A systematic review and dose-response meta-analysis. J. Environ. Res. 2021, 193, 110538. [Google Scholar] [CrossRef]
- Rocha, J.P.S.; Lopes, I.S.S.; Henriques, C.E.L.; Minekawa, T.B.; Bastos, M.S.C.B.O. Katuana from Baía do Guajará: Diabetes and self-reported arterial hypertension in a riverside population of Combú. In Proceedings of the III Congress on Health Education in the Amazon (COESA), Pará, Brazil, 12–14 November 2014. [Google Scholar]
- Rodrigues, D.N.; Mussi, R.F.d.F.; Almeida, C.B.d.; Nascimento Junior, J.R.A.; Moreira, S.R.; Carvalho, F.O. Sociodemographic determinants associated with the level of physical activity of Bahian quilombolas, 2016 survey. J. Epidemiol. E Serviços De Saúde 2020, 29, e2018511. [Google Scholar] [CrossRef]
- Wanzeler, F.S.d.C. Physical Activity and Associated Factors in Riverside Adolescents in the Amazon. Master’s Thesis, University of Brasilia, Brasília, Brazil, 2017. Available online: https://repositorio.unb.br/handle/10482/24652 (accessed on 15 January 2021).
- Wanzeler, F.S.d.C.; Nogueira, J.A.D. Physical activity in rural populations of Brazil: A review of literature. Rev. Bras. De Ciência E Mov. 2019, 27, 228–240. [Google Scholar] [CrossRef]
- Brasil, M.S. Protocols of the Food and Nutrition Surveillance System—SISVAN in Health Care; Primary Care, Health Care Secretariat, Ministry of Health: Brasília, Brazil, 2008. Available online: http://189.28.128.100/dab/docs/portaldab/publicacoes/protocolo_sisvan.pdf (accessed on 10 February 2022).
- de Araújo, I.M.; Antunes Paes, N. Quality of anthropometric data of hypertensive users seen at the family health program and its correlation with risk factors. Texto Contexto Enferm. 2013, 22, 1030–1040. [Google Scholar]
- Pereira, R.A.; Sichieri, R.; Marins, V.M. Razão cintura/quadril como preditor de hipertensão arterial. J Cad. De Saúde Pública 1999, 15, 333–344. Available online: https://www.scielo.br/j/csp/a/QL4w8KBLPPh9sTds769ZS9g/?lang=pt&format=pdf (accessed on 20 April 2021). [CrossRef] [PubMed][Green Version]
- Rodrigues, J.M.P.; Da Silva, G.P. The Modular Teaching Organization System (MTOS) from the perspective of graduates in the municipality of Breves—Pará. J. Rev. Bras. De Educ. Do Campo 2018, 3, 260–286. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Descriptors | Group 1 n = 39 | Group 2 n = 47 | Effect Size | p |
|---|---|---|---|---|
| Sociodemographic | ||||
| Sex | F = 51.3% | F = 48.9% | Φ = 0.02 | 0.83 |
| M = 48.7% | M = 51.1% | |||
| Ethnicity | ||||
| Asian | 2.6% | 4.3% | V = 0.23 ++ | 0.35 |
| White | 17.9% | 21.3% | ||
| Indigenous | 2.6% | 6.4% | ||
| Mixed race | 43.6% | 53.2% | ||
| Black | 33.3% | 14.9% | ||
| Education | ||||
| No education | 59.0% a | 0.0% a | V = 0.77 +++ | < 0.001 *** |
| Initial Elementary School | 41.0% | 40.5% | ||
| Final Elementary School | 0.0% b | 46.8% b | ||
| High School | 0.0% c | 10.6% c | ||
| University graduate | 0.0% | 2.1% | ||
| Reading | ||||
| No | 100.0% | 0.0% | Φ = 1.00 +++ | < 0.001 *** |
| Yes | 0.0% | 100.0% |
| Descriptors | Group 1 n = 39 | Group 2 n = 47 | Effect Size | p |
|---|---|---|---|---|
| Behavioral | ||||
| Smoking Time/year | 0.0 (0–15) | 0.0 (0–0) | 0.04 | <0.05 * |
| Number of cigarettes/day | 0.0 (0–0) | 0.0 (0–0) | 0.00 | 0.50 |
| Frequency Alcohol/week | 0.0 (0–0) | 0.0 (0–3) | 0.04 | <0.05 * |
| Exercise Frequency | 0.0 (0–0) | 1.5 (0–4) | 0.11 + | <0.01 ** |
| Fish Consumption/week | 3.0 (2–6) | 4.0 (2–6) | 0.01 | 0.32 |
| Biological | ||||
| SBP | 130.0 (120–142) | 130.0 (120–140) | 0.01 | 0.30 |
| DBP | 80 (80–90) | 80 (80–92) | 0.00 | 0.80 |
| WHR | 1.0 (0.9–1.0) | 0.9 (0.9–1.0) | 0.01 | 0.27 |
| BMI kg/m2 | 29.4 (25–34) | 27 (24–30) | 0.05 | <0.05 * |
| Total Cholesterol mg/dL | 185 (165–215) | 166 (140–200) | 0.07 | <0.05 * |
| HDL mg/dL | 55 (50–68) | 54 (41–65) | 0.02 | 0.23 |
| LDL mg/dL | 103 (81–123) | 83.8 (72–104) | 0.08 | <0.05 * |
| Triglycerides mg/dL | 120 (85–159) | 115 (80–183) | 0.00 | 0.90 |
| Blood glucose mg/dL | 70 (68–85) | 72 (70–84) | 0.01 | 0.40 |
| Age | 55.0 (49–62) | 40.0 (32–48) | 0.29 + | <0.001 *** |
| Descriptors | Group 1 n = 39 | Group 2 n = 47 | Effect Size | p |
|---|---|---|---|---|
| Behavioral | ||||
| Smoker | ||||
| No | 89.7% | 95.7% | Φ = 0.12 + | 0.40 |
| Yes | 10.3% | 4.3% | ||
| Ex-smoker | ||||
| No | 64.1% | 85.1% | V = 0.24 ++ | 0.09 |
| Yes | 25.6% | 10.6% | ||
| No reply | 10.3% | 4.3% | ||
| Alcohol consumption | ||||
| No | 79.5% | 57.4% | Φ = 0.23 + | <0.05 * |
| Yes | 20.5% | 42.6% | ||
| Healthy eating | ||||
| No | 38.5% | 29.8% | Φ = 0.09 | 0.40 |
| Yes | 61.5% | 70.2% | ||
| BIOLOGICAL | ||||
| SAH | ||||
| No | 74.4% | 83.3% | Φ = 0.10 + | 0.33 |
| Yes | 25.6% | 17.0% | ||
| Diabetes | ||||
| No | 94.9% | 95.7% | Φ = 0.02 | 1.00 |
| Yes | 5.1% | 4.3% | ||
| Stroke | ||||
| No | 100% | 97.9% | Φ = 0.10 + | 1.00 |
| Yes | 0.0% | 2.1% | ||
| CVD | ||||
| No | 84.6% | 85.1% | V = 0.10 + | 0.87 |
| Don’t know | 15.4% | 12.8% | ||
| Other | 0.0% | 2.1% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lucianelli Junior, D.; Pereira, A.L.; Santos, O.S.; Paes, M.d.C.F.; Ikuta, Y.M.; Silveira, R.; Valentin, F.N. Sociobehavioral, Biological, and Health Characteristics of Riverside People in the Xingu Region, Pará, Brazil. Int. J. Environ. Res. Public Health 2023, 20, 5542. https://doi.org/10.3390/ijerph20085542
Lucianelli Junior D, Pereira AL, Santos OS, Paes MdCF, Ikuta YM, Silveira R, Valentin FN. Sociobehavioral, Biological, and Health Characteristics of Riverside People in the Xingu Region, Pará, Brazil. International Journal of Environmental Research and Public Health. 2023; 20(8):5542. https://doi.org/10.3390/ijerph20085542
Chicago/Turabian StyleLucianelli Junior, Dalberto, Adenilson Leão Pereira, Ozélia Sousa Santos, Maria do Carmo Faria Paes, Yuji Magalhães Ikuta, Rodrigo Silveira, and Fernanda Nogueira Valentin. 2023. "Sociobehavioral, Biological, and Health Characteristics of Riverside People in the Xingu Region, Pará, Brazil" International Journal of Environmental Research and Public Health 20, no. 8: 5542. https://doi.org/10.3390/ijerph20085542
APA StyleLucianelli Junior, D., Pereira, A. L., Santos, O. S., Paes, M. d. C. F., Ikuta, Y. M., Silveira, R., & Valentin, F. N. (2023). Sociobehavioral, Biological, and Health Characteristics of Riverside People in the Xingu Region, Pará, Brazil. International Journal of Environmental Research and Public Health, 20(8), 5542. https://doi.org/10.3390/ijerph20085542