
Epidemiological Characteristics of Cancer Patients Attending at Felege Hiwot Referral Hospital, Northwest Ethiopia


Abstract
1. Background
2. Methods
3. Results
4. Discussion
5. Conclusions
5.1. What Is Already Know on This Topic
- There is variation in the cancer types between sex and districts;
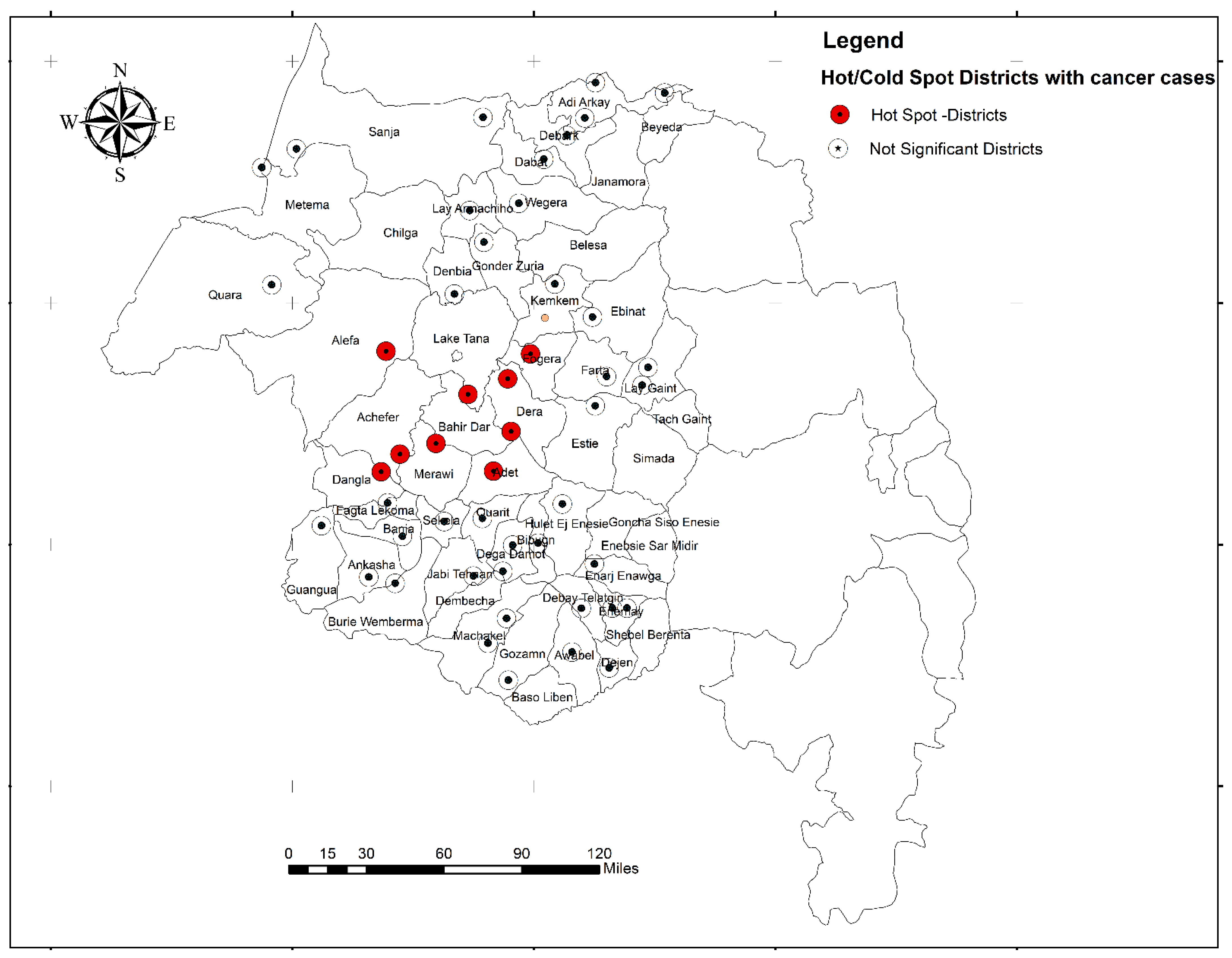
- Hot spot districts with cancer cases were identified
5.2. What This Study Adds
- The most common cancer types for women and men were identified in the study area;
- Hot spot districts with cancer cases were identified using spatial analysis, which provides an insight for further exploration of exposure-related factors for cancer, in order to guide future cancer prevention and control programs
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Dey, S.; Dhillon, P.K.; Rajaraman, P. Cancer Prevention in Low- and Middle-Income Countries. J. Cancer Epidemiol. 2017, 2017, 2. [Google Scholar] [CrossRef]
- Fitzmaurice, C.; Akinyemiju, T.F.; Al Lami, F.H.; Alam, T.; Alizadeh-Navaei, R.; Allen, C.; Alsharif, U.; Alvis-Guzman, N.; Amini, E.; Anderson, B.O. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: A systematic analysis for the global burden of disease study. JAMA Oncol. 2018, 4, 1553–1568. [Google Scholar]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Jemal, A. Cancer in Africa 2012. Cancer Epidemiol. Biomark. Prev. 2014, 23, 953–966. [Google Scholar] [CrossRef]
- Torre, L.A.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global Cancer Incidence and Mortality Rates and Trends—An Update. Cancer Epidemiol. Biomark. Prev. 2016, 25, 16–27. [Google Scholar] [CrossRef]
- Tefera, B.; Assefa, M.; Abebe, B.; Rauch, D. Patterns of Cancer in University of Gondar Hospital: North-West Ethiopia. J. Oncol. Med. Pract. 2016, 1, 2. [Google Scholar]
- Deressa, B.T.; Cihoric, N.; Badra, E.V.; Tsikkinis, A.; Rauch, D. Breast cancer care in northern Ethiopia—Cross-sectional analysis. BMC Cancer 2019, 19, 393. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer. GLOBOCAN 2012: Estimated Cancer Incidence, Mortality and Prevalence Worldwide in 2012; International Agency for Research on Cancer: Lyon, France, 2012. [Google Scholar]
- Memirie, S.T.; Habtemariam, M.K.; Asefa, M.; Deressa, B.T.; Abayneh, G.; Tsegaye, B.; Abraha, M.W.; Ababi, G.; Jemal, A.; Rebbeck, T.R. Estimates of Cancer Incidence in Ethiopia in 2015 Using Population-Based Registry Data. J. Glob. Oncol. 2018, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.M.; Kim, H.C.; Lee, S. Psychosocial impact of cancer patients on their family members. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2013, 45, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Morgan, G.W.; Foster, K.; Healy, B.; Opie, C.; Huynh, V. Improving Health and Cancer Services in Low-Resource Countries to Attain the Sustainable Development Goals Target 3.4 for Noncommunicable Diseases. J. Glob. Oncol. 2018, 4, 1–11. [Google Scholar] [CrossRef]
- Sebri, V.; Pravettoni, G. Tailored Psychological Interventions to Manage Body Image: An Opinion Study on Breast Cancer Survivors. Int. J. Environ. Res. Public Health 2023, 20, 2991. [Google Scholar] [CrossRef]
- Durosini, I.; Triberti, S.; Savioni, L.; Sebri, V.; Pravettoni, G. The Role of Emotion-Related Abilities in the Quality of Life of Breast Cancer Survivors: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 12704. [Google Scholar] [CrossRef]
- Avancini, A.; Pala, V.; Trestini, I.; Tregnago, D.; Mariani, L.; Sieri, S.; Krogh, V.; Boresta, M.; Milella, M.; Pilotto, S. Exercise levels and preferences in cancer patients: A cross-sectional study. Int. J. Environ. Res. Public Health 2020, 17, 5351. [Google Scholar] [CrossRef]
- Gonzalez-Saenz de Tejada, M.; Bilbao, A.; Baré, M.; Briones, E.; Sarasqueta, C.; Quintana, J.; Escobar, A.; Group, C.C. Association between social support, functional status, and change in health-related quality of life and changes in anxiety and depression in colorectal cancer patients. Psycho-oncology 2017, 26, 1263–1269. [Google Scholar] [CrossRef] [PubMed]
- Federal Ministry of Health Ethiopia. National Cancer Control Plan 2016–2020. In Disease Prevention and Control Directorate; Federal Ministry of Health Ethiopia: Addis Ababa, Ethiopia, 2015. [Google Scholar]
- Bureau of Finance & Economic Development Amhara National Regional State. Population Affairss Bureau of Finance & Economic Development (BoFED), Amhara National Regional State. 2016. Available online: http://www.amharabofed.gov.et/about_bofed.html (accessed on 8 April 2019).
- World Health Organization. International Classification of Diseases for Oncology, 3rd ed.; World Health Organization: Geneva, Switzerland, 2001. [Google Scholar]
- Bureau of Finance and Economic Development Amhara Region. The Projected Population Data of 2017 to 2019 for Amhara Regional National State; Bureau of Finance and Economic Development Amhara Region: Bahir Dar, Ethiopia, 2019. [Google Scholar]
- Fotheringham, A.S.; Brunsdon, C.; Charlton, M. Geographically Weighted Regression: The Analysis of Spatially Varying Relationships; John Wiley & Sons: Hoboken, NJ, USA, 2003. [Google Scholar]
- Timotewos, G.; Solomon, A.; Mathewos, A.; Addissie, A.; Bogale, S.; Wondemagegnehu, T.; Aynalem, A.; Ayalnesh, B.; Dagnechew, H.; Bireda, W.; et al. First data from a population based cancer registry in Ethiopia. Cancer Epidemiol. 2018, 53, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Cook, M.B.; Dawsey, S.M.; Freedman, N.D.; Inskip, P.D.; Wichner, S.M.; Quraishi, S.M.; Devesa, S.S.; McGlynn, K.A. Sex disparities in cancer incidence by period and age. Cancer Epidemiol. Biomark. Prev. 2009, 18, 1174–1182. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Shi, O.; Cai, N.; Jiang, Y.; Zhang, K.; Zhu, Z.; Yuan, H. Disparities in Cancer Incidence among Chinese Population versus Migrants to Developed Regions: A Population-Based Comparative Study. Cancer Epidemiol. Biomark. Prev. 2019, 28, 890–899. [Google Scholar] [CrossRef]
- Jiang, X.; Cai, S.; Hu, Y.; Ye, D.; Li, Q.; Chen, K.; Jin, M. Sex disparities in cancer incidence in Jiashan County, China, 1995-2014. Cancer Epidemiol. 2017, 50, 46–52. [Google Scholar] [CrossRef]
- Stewart, B.; Wild, C.P. World Cancer Report 2014; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Kamper-Jørgensen, M.; Rostgaard, K.; Glaser, S.L.; Zahm, S.H.; Cozen, W.; Smedby, K.E.; Sanjosé, S.; Chang, E.T.; Zheng, T.; La Vecchia, C.; et al. Cigarette smoking and risk of Hodgkin lymphoma and its subtypes: A pooled analysis from the International Lymphoma Epidemiology Consortium (InterLymph). Ann. Oncol. 2013, 24, 2245–2255. [Google Scholar] [CrossRef]
- Taborelli, M.; Montella, M.; Libra, M.; Tedeschi, R.; Crispo, A.; Grimaldi, M.; Dal Maso, L.; Serraino, D.; Polesel, J. The dose-response relationship between tobacco smoking and the risk of lymphomas: A case-control study. BMC Cancer 2017, 17, 421. [Google Scholar] [CrossRef]
- Hu, L.; Luo, D.; Zhou, T.; Tao, Y.; Feng, J.; Mei, S. The association between non-Hodgkin lymphoma and organophosphate pesticides exposure: A meta-analysis. Environ. Pollut. (Barking Essex 1987) 2017, 231, 319–328. [Google Scholar] [CrossRef]
- Luo, D.; Zhou, T.; Tao, Y.; Feng, Y.; Shen, X.; Mei, S. Exposure to organochlorine pesticides and non-Hodgkin lymphoma: A meta-analysis of observational studies. Sci. Rep. 2016, 6, 25768. [Google Scholar] [CrossRef] [PubMed]
- Fitzmaurice, C.; Allen, C.; Barber, R.M.; Barregard, L.; Bhutta, Z.A.; Brenner, H.; Dicker, D.J.; Chimed-Orchir, O.; Dandona, R.; Dandona, L. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: A systematic analysis for the global burden of disease study. JAMA Oncol. 2017, 3, 524–548. [Google Scholar] [PubMed]
- Torre, L.A.; Islami, F.; Siegel, R.L.; Ward, E.M.; Jemal, A. Global cancer in women: Burden and trends. Cancer Epidemiol. Biomark. Prev. 2017, 26, 444–457. [Google Scholar] [CrossRef] [PubMed]
- Hadi, M.A. Breast cancer in developing countries: The shrinking age gap. Breast J. 2019, 25, 795–797. [Google Scholar] [CrossRef] [PubMed]
- Denny, L.; de Sanjose, S.; Mutebi, M.; Anderson, B.O.; Kim, J.; Jeronimo, J.; Herrero, R.; Yeates, K.; Ginsburg, O.; Sankaranarayanan, R. Interventions to close the divide for women with breast and cervical cancer between low-income and middle-income countries and high-income countries. Lancet 2017, 389, 861–870. [Google Scholar] [CrossRef]
- Obel, J.; Souares, Y.; Hoy, D.; Baravilala, W.; Garland, S.M.; Kjaer, S.K.; Roth, A. A systematic review of cervical cancer incidence and mortality in the Pacific Region. Asian Pac. J. Cancer Prev. 2014, 15, 9433–9437. [Google Scholar] [CrossRef]
- Shrestha, A.D.; Neupane, D.; Vedsted, P.; Kallestrup, P. Cervical Cancer Prevalence, Incidence and Mortality in Low and Middle Income Countries: A Systematic Review. Asian Pac. J. Cancer Prev. 2018, 19, 319–324. [Google Scholar] [CrossRef]
- Seckl, M.J.; Sebire, N.J.; Berkowitz, R.S. Gestational trophoblastic disease. Lancet 2010, 376, 717–729. [Google Scholar] [CrossRef]
- Rick, T.; Habtamu, B.; Tigeneh, W.; Abreha, A.; Norden, Y.v.; Grover, S.; Assefa, M.; Incrocci, L. Patterns of Care of Cancers and Radiotherapy in Ethiopia. J. Glob. Oncol. 2019, 5, 1–8. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
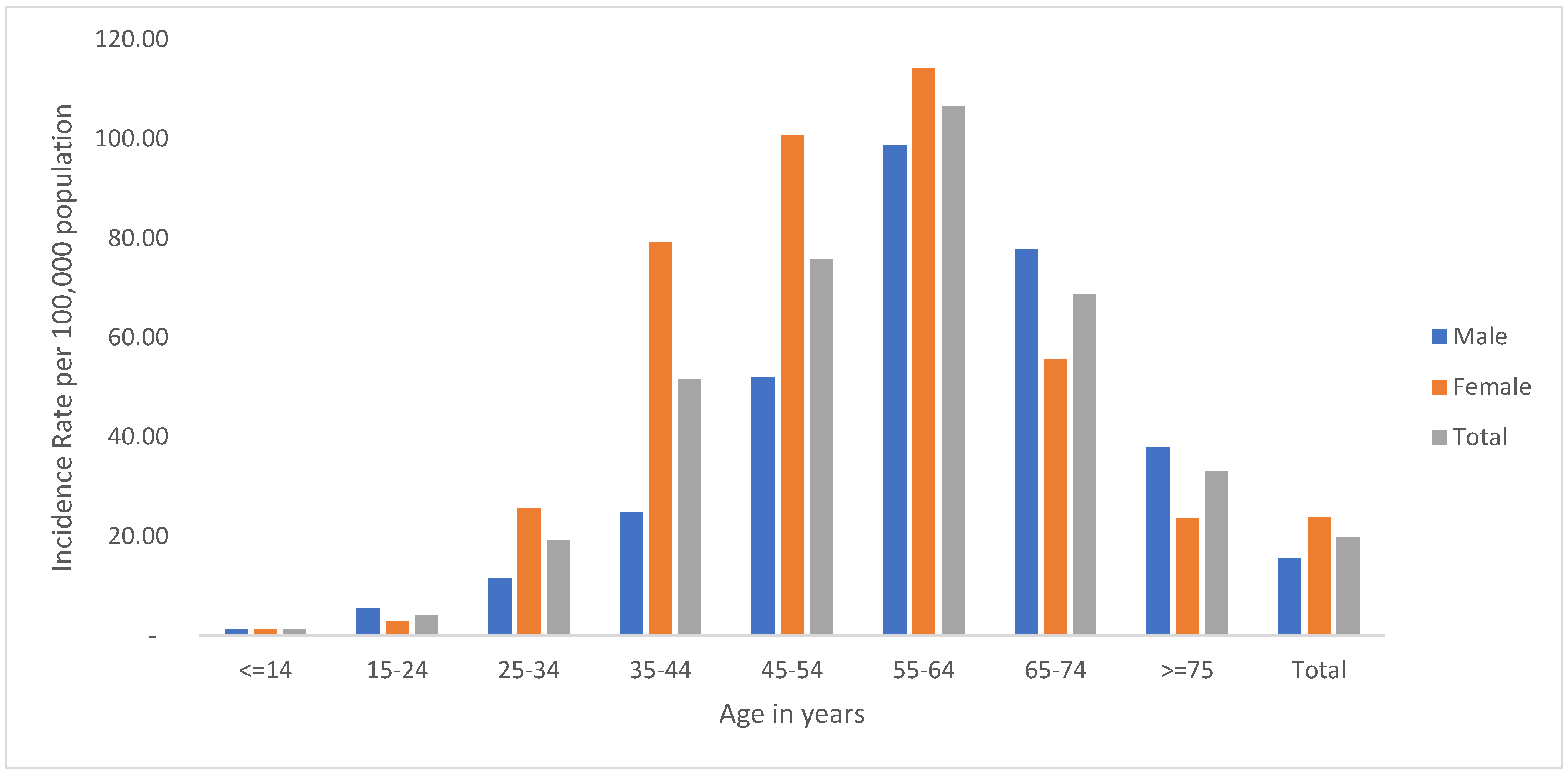
| Age | Frequency | Proportion (95%CI) | Total n (Proportion with 95%CI) | ||
|---|---|---|---|---|---|
| Female | Male | Female | Male | ||
| ≤14 | 22 | 25 | 1.9 (1.3–2.9) | 3.4 (2.3–4.9) | 47 (2.5, 1.9–3.3) |
| 15–24 | 36 | 58 | 3.1 (2.3–4.3) | 7.8 (6.1–9.9) | 94 (5.0, 4.1–6.1) |
| 25–34 | 178 | 72 | 15.5 (13.5–17.7) | 9.7 (7.8–12.1) | 250 (13.2, 11.8–14.8) |
| 35–44 | 344 | 114 | 30.0 (27.4–32.7) | 15.4 (13.0–18.2) | 458 (24.3, 22.4–26.2) |
| 45–54 | 293 | 158 | 25.5 (23.1–28.1) | 21.3 (18.5–24.4) | 451 (23.9, 22.0–25.9) |
| 55–64 | 219 | 190 | 19.1 (16.9–21.5) | 25.6 (22.6–28.9) | 409 (21.7, 19.9–23.7) |
| 65–74 | 46 | 97 | 4.0 (3.0–5.3) | 13.1 (10.8–15.7) | 143 (7.6, 6.5–8.9) |
| ≥75 | 10 | 27 | 0.9 (0.5–1.6) | 3.6 (2.5–5.3) | 37 (2.0, 1.4–2.7) |
| Total | 1148 | 741 | 60.8 (58.5–63.0) | 39.2 (37.0–41.5) | 1889 (100) |
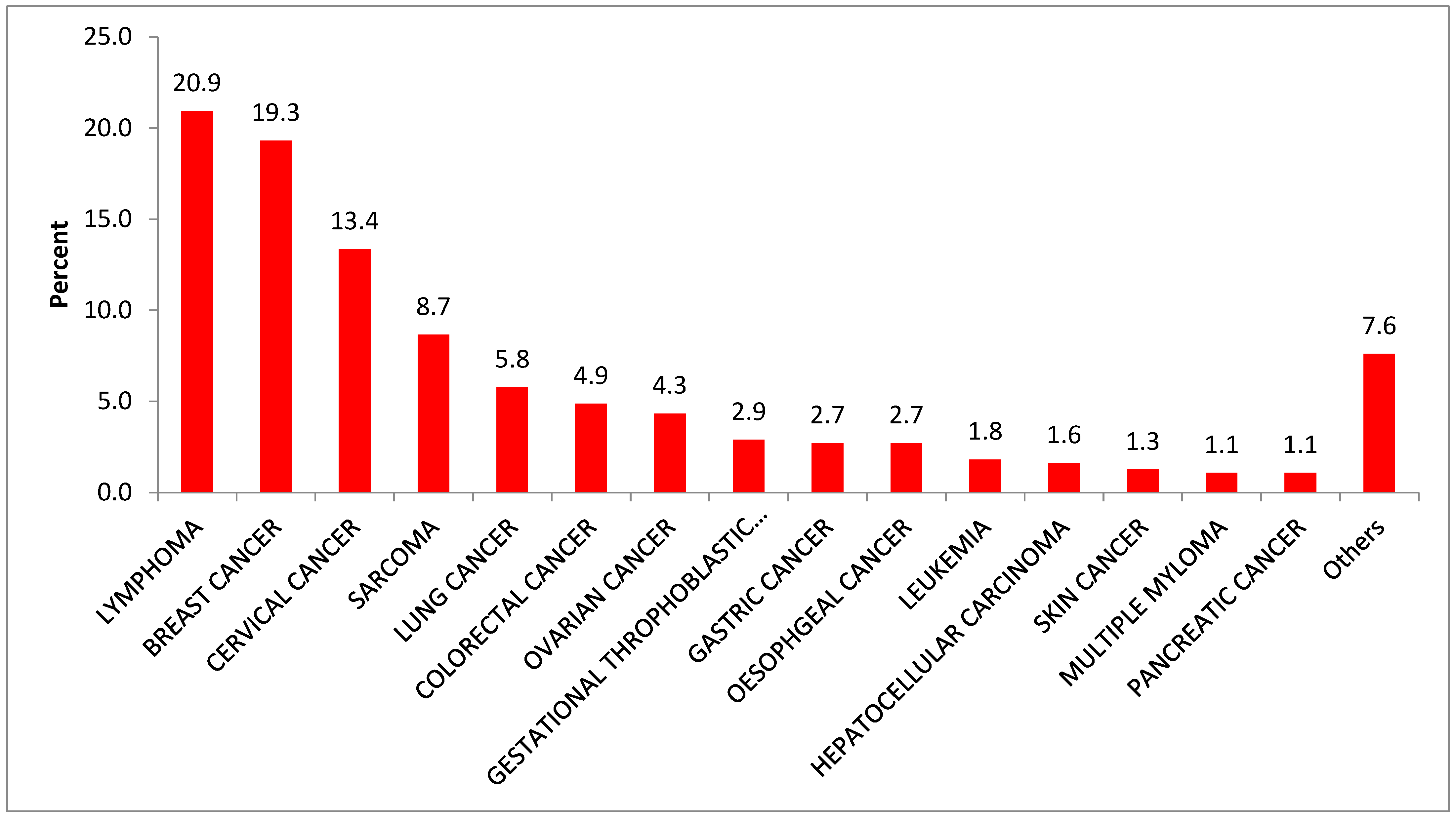
| Female | Male | |||||
|---|---|---|---|---|---|---|
| Cancer Type | No | % | Cancer Type | No | % | |
| 1. | BREAST | 326 | 28.4 | LYMPHOMA | 218 | 29.4 |
| 2. | CERVICAL | 242 | 21.1 | SARCOMA | 77 | 10.4 |
| 3. | LYMPHOMA | 78 | 6.8 | LUNG | 66 | 8.9 |
| 4. | OVARIAN | 72 | 6.3 | COLORECTAL | 61 | 8.23 |
| 5. | SARCOMA | 61 | 5.3 | LEUKEMIA | 59 | 8.0 |
| 6. | COLORECTAL | 60 | 5.2 | HEPATOCELLULAR CARCINOMA | 46 | 6.2 |
| 7. | GESTATIONAL THROPHOBLASTIC NEUPLASM | 57 | 5.0 | BREAST | 41 | 5.5 |
| 8. | LUNG | 47 | 4.1 | OESOPHGEAL | 26 | 3.5 |
| 9. | GASTRIC | 33 | 2.9 | OROPHARYNGEAL | 21 | 2.8 |
| 10. | ESOPHGEAL | 33 | 2.9 | GASTRIC | 19 | 2.6 |
| 11. | HEPATOCELLULAR CARCINOMA | 29 | 2.5 | TESTICULAR | 14 | 1.9 |
| 12. | HEAD AND NECK | 19 | 1.7 | PANCREATIC | 12 | 1.6 |
| 13. | LEUKEMIA | 10 | 0.9 | HEAD AND NECK | 11 | 1.5 |
| 14. | PANCREATIC | 10 | 0.9 | SKIN | 11 | 1.5 |
| 15. | VULVAR | 7 | 0.6 | WILLM’S TUMOR | 8 | 1.08 |
| 16. | OROPHARYNGEAL | 7 | 0.6 | NASOPHARENGEAL | 7 | 0.94 |
| 17. | ANAL | 6 | 0.5 | MULTIPLE MYLOMA | 6 | 0.81 |
| 18. | CHRONIC MYELOID LEUKAEMIA | 6 | 0.6 | CANCER OF UNKNOWN PRIMARY SITE | 4 | 0.5 |
| 19. | CANCER OF UNKNOWN PRIMARY SITE | 6 | 0.5 | SMALL BOWEL | 4 | 0.5 |
| 20. | SMALL BOWEL | 6 | 0.5 | PROSTATE | 4 | 0.5 |
| 21. | MULTIPLE MYLOMA | 5 | 0.4 | ANAL | 3 | 0.4 |
| 22. | NASOPHARENGEAL | 4 | 0.4 | NEUROBLASTOMA | 3 | 0.4 |
| 23. | WILMS’ TUMOR | 4 | 0.4 | ACUTE LYMPHOCYTIC LEUKEMIA | 2 | 0.27 |
| 24. | TERATOMA | 4 | 0.4 | BRAIN TUMOR | 2 | 0.27 |
| 25. | KAPOSIS SARCOMA | 3 | 0.3 | CHRONIC MYELOID LEUKAEMIA | 2 | 0.27 |
| 26. | SKIN | 3 | 0.3 | CHOLANGOCARCINOMA | 2 | 0.27 |
| 27. | BLADDER | 2 | 0.2 | LIPOSARCOMA | 2 | 0.27 |
| 28. | CHOLANGOCARCINOMA | 2 | 0.2 | TERATOMA | 2 | 0.27 |
| 29. | OTHER CANCER | 6 | 1 | OTHER CANCER | 7 | 1.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azage, M.; Zewudie, S.; Goedert, M.H.; Hagos, E.G. Epidemiological Characteristics of Cancer Patients Attending at Felege Hiwot Referral Hospital, Northwest Ethiopia. Int. J. Environ. Res. Public Health 2023, 20, 5218. https://doi.org/10.3390/ijerph20065218
Azage M, Zewudie S, Goedert MH, Hagos EG. Epidemiological Characteristics of Cancer Patients Attending at Felege Hiwot Referral Hospital, Northwest Ethiopia. International Journal of Environmental Research and Public Health. 2023; 20(6):5218. https://doi.org/10.3390/ijerph20065218
Chicago/Turabian StyleAzage, Muluken, Serkalem Zewudie, Martha H. Goedert, and Engda G. Hagos. 2023. "Epidemiological Characteristics of Cancer Patients Attending at Felege Hiwot Referral Hospital, Northwest Ethiopia" International Journal of Environmental Research and Public Health 20, no. 6: 5218. https://doi.org/10.3390/ijerph20065218
APA StyleAzage, M., Zewudie, S., Goedert, M. H., & Hagos, E. G. (2023). Epidemiological Characteristics of Cancer Patients Attending at Felege Hiwot Referral Hospital, Northwest Ethiopia. International Journal of Environmental Research and Public Health, 20(6), 5218. https://doi.org/10.3390/ijerph20065218