
Clinical Usefulness of a Short Version of the Internet Addiction Test to Screen for Probable Internet Addiction in Adolescents with Autism Spectrum Disorder

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Internet Addiction Test (IAT)
2.3. A Short Version of the Internet Addiction Test (s-IAT)
2.4. Clinical Diagnosis of IA
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Sociodemographic of the Subjects
3.2. Clinical Diagnosis of IA
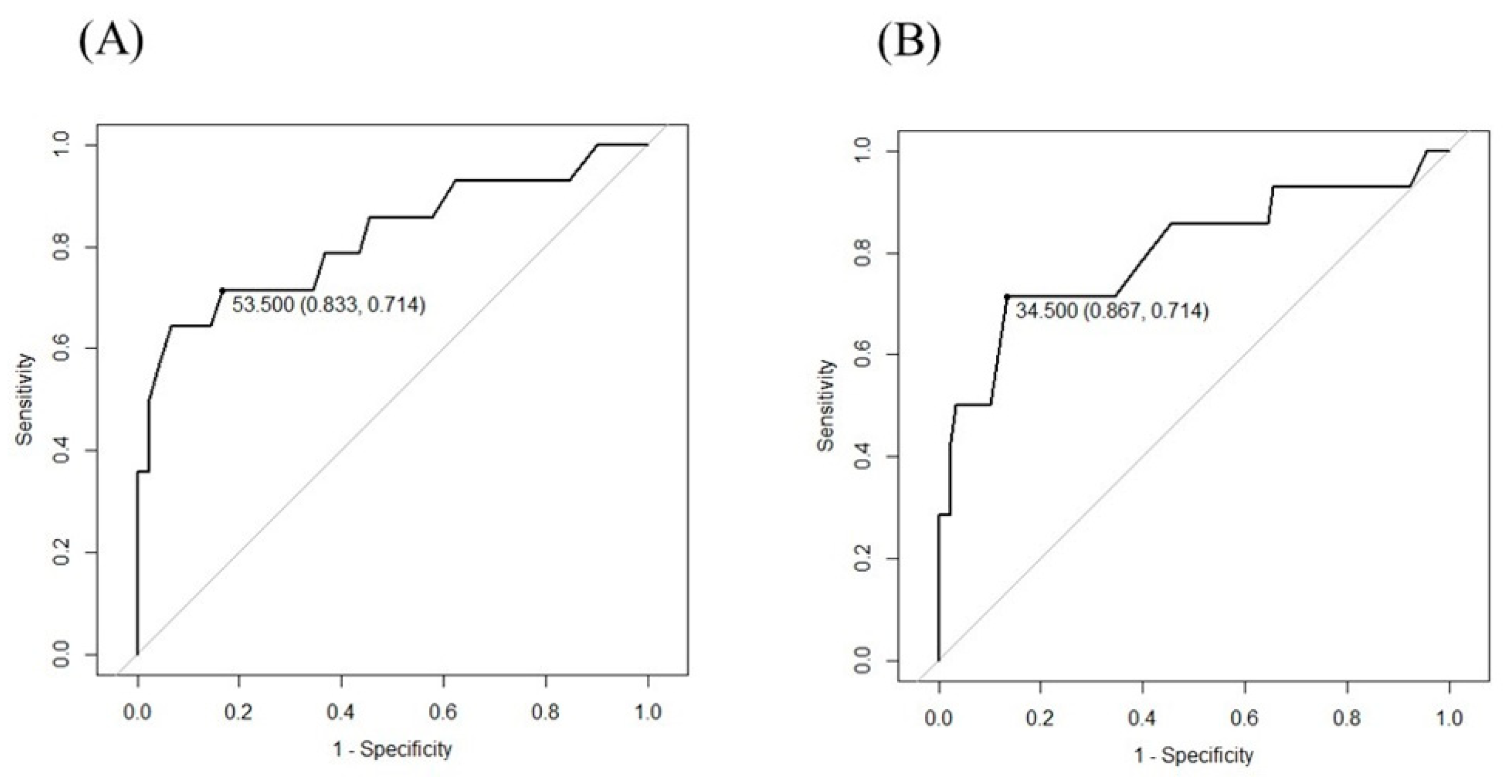
3.3. Cut-Off Points for IAT and s-IAT
3.4. Results of the IAT and s-IAT for Screening IA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aboujaoude, E. Problematic Internet use: An overview. World Psychiatry Off. J. World Psychiatr. Assoc. 2010, 9, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Marin, M.G.; Nunez, X.; de Almeida, R.M.M. Internet Addiction and Attention in Adolescents: A Systematic Review. Cyberpsychol. Behav. Soc. Netw. 2021, 24, 237–249. [Google Scholar] [CrossRef] [PubMed]
- Kawabe, K.; Horiuchi, F.; Miyama, T.; Jogamoto, T.; Aibara, K.; Ishii, E.; Ueno, S.I. Internet addiction and attention-deficit/hyperactivity disorder symptoms in adolescents with autism spectrum disorder. Res. Dev. Disabil. 2019, 89, 22–28. [Google Scholar] [CrossRef]
- So, R.; Makino, K.; Fujiwara, M.; Hirota, T.; Ohcho, K.; Ikeda, S.; Tsubouchi, S.; Inagaki, M. The Prevalence of Internet Addiction among a Japanese Adolescent Psychiatric Clinic Sample with Autism Spectrum Disorder and/or Attention-Deficit Hyperactivity Disorder: A Cross-Sectional Study. J. Autism. Dev. Disord. 2017, 47, 2217–2224. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.Q.; Yao, N.Q.; Zhou, X.; Liu, J.; Lv, Z.T. The association between attention deficit/hyperactivity disorder and internet addiction: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 260. [Google Scholar] [CrossRef]
- Gao, X.; Zhang, M.; Yang, Z.; Wen, M.; Huang, H.; Zheng, R.; Wang, W.; Wei, Y.; Cheng, J.; Han, S.; et al. Structural and Functional Brain Abnormalities in Internet Gaming Disorder and Attention-Deficit/Hyperactivity Disorder: A Comparative Meta-Analysis. Front. Psychiatry 2021, 12, 679437. [Google Scholar] [CrossRef]
- Ko, C.H.; Yen, J.Y.; Chen, C.S.; Yeh, Y.C.; Yen, C.F. Predictive values of psychiatric symptoms for internet addiction in adolescents: A 2-year prospective study. Arch. Pediatr. Adolesc. Med. 2009, 163, 937–943. [Google Scholar] [CrossRef]
- Tateno, M.; Matsuzaki, T.; Takano, A.; Higuchi, S. Increasing important roles of child and adolescent psychiatrists in the treatment of gaming disorder: Current status in Japan. Front. Psych. 2022, 13, 995665. [Google Scholar] [CrossRef]
- Dullur, P.; Krishnan, V.; Diaz, A.M. A systematic review on the intersection of attention-deficit hyperactivity disorder and gaming disorder. J. Psychiatr. Res. 2021, 133, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Murray, A.; Koronczai, B.; Király, O.; Griffiths, M.D.; Mannion, A.; Leader, G.; Demetrovics, Z. Autism, Problematic Internet Use and Gaming Disorder: A Systematic Review. Rev. J. Autism Dev. Disord. 2022, 9, 120–140. [Google Scholar] [CrossRef]
- Shane-Simpson, C.; Brooks, P.J.; Obeid, R.; Denton, E.; Gillespie-Lynch, K. Associations between compulsive internet use and the autism spectrum. Res. Autism Spectr. Disord. 2016, 23, 152–165. [Google Scholar] [CrossRef]
- Chen, Y.L.; Chen, S.H.; Gau, S.S. ADHD and autistic traits, family function, parenting style, and social adjustment for Internet addiction among children and adolescents in Taiwan: A longitudinal study. Res. Dev. Disabil. 2015, 39, 20–31. [Google Scholar] [CrossRef] [PubMed]
- Lombardo, M.V.; Chakrabarti, B.; Bullmore, E.T.; Sadek, S.A.; Pasco, G.; Wheelwright, S.J.; Suckling, J.; Consortium, M.A.; Baron-Cohen, S. Atypical neural self-representation in autism. Brain 2010, 133, 611–624. [Google Scholar] [CrossRef]
- Lai, M.C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- King, D.L.; Chamberlain, S.R.; Carragher, N.; Billieux, J.; Stein, D.; Mueller, K.; Potenza, M.N.; Rumpf, H.J.; Saunders, J.; Starcevic, V.; et al. Screening and assessment tools for gaming disorder: A comprehensive systematic review. Clin. Psychol. Rev. 2020, 77, 101831. [Google Scholar] [CrossRef]
- Meerkerk, G.J.; Van Den Eijnden, R.; Vermulst, A.A.; Garretsen, H.F.L. The Compulsive Internet Use Scale (CIUS): Some psychometric properties. Cyberpsychol. Behav. Soc. Netw. 2009, 12, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ko, C.H.; Yen, J.Y.; Chen, S.H.; Yang, M.J.; Lin, H.C.; Yen, C.F. Proposed diagnostic criteria and the screening and diagnosing tool of Internet addiction in college students. Compr. Psychiatry 2009, 50, 378–384. [Google Scholar] [CrossRef] [PubMed]
- Young, K.S. Internet addiction: The emergence of a new clinical disorder. Cyber. Psychol. Behav. 1998, 1, 237–244. [Google Scholar] [CrossRef]
- Young, K.S. Caught in the Net: How to Recognize the Signs of Internet Addiction—And a Winning Strategy for Recovery; Wiley: New York, NY, USA, 1998. [Google Scholar]
- Khazaal, Y.; Billieux, J.; Thorens, G.; Khan, R.; Louati, Y.; Scarlatti, E.; Theintz, F.; Lederrey, J.; Van Der Linden, M.; Zullino, D. French validation of the internet addiction test. Cyberpsychol. Behav. Impact Internet Multimed. Virtual Real. Behav. Soc. 2008, 11, 703–706. [Google Scholar] [CrossRef] [PubMed]
- Brand, M.; Laier, C.; Pawlikowski, M.; Schachtle, U.; Scholer, T.; Altstotter-Gleich, C. Watching pornographic pictures on the Internet: Role of sexual arousal ratings and psychological-psychiatric symptoms for using Internet sex sites excessively. Cyberpsychol. Behav. Soc. Netw. 2011, 14, 371–377. [Google Scholar] [CrossRef]
- Fernandez-Villa, T.; Molina, A.J.; Garcia-Martin, M.; Llorca, J.; Delgado-Rodriguez, M.; Martin, V. Validation and psychometric analysis of the Internet Addiction Test in Spanish among college students. BMC Public Health 2015, 15, 953. [Google Scholar] [CrossRef]
- Ferraro, G.; Caci, B.; D’Amico, A.; Di Blasi, M. Internet addiction disorder: An Italian study. Cyberpsychol. Behav. Impact Internet Multimed. Virtual Real. Behav. Soc. 2007, 10, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Siomos, K.E.; Dafouli, E.D.; Braimiotis, D.A.; Mouzas, O.D.; Angelopoulos, N.V. Internet addiction among Greek adolescent students. Cyberpsychol. Behav. Impact Internet Multimed. Virtual Real. Behav. Soc. 2008, 11, 653–657. [Google Scholar] [CrossRef]
- Kaya, F.; Delen, E.; Young, K.S. Psychometric properties of the Internet Addiction Test in Turkish. J. Behav. Addict. 2016, 5, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Cernja, I.; Vejmelka, L.; Rajter, M. Internet addiction test: Croatian preliminary study. BMC Psychiatry 2019, 19, 388. [Google Scholar] [CrossRef] [PubMed]
- Lam, L.T.; Peng, Z.W.; Mai, J.C.; Jing, J. Factors associated with Internet addiction among adolescents. Cyberpsychol. Behav. Impact Internet Multimed. Virtual Real. Behav. Soc. 2009, 12, 551–555. [Google Scholar] [CrossRef]
- Moon, S.J.; Hwang, J.S.; Kim, J.Y.; Shin, A.L.; Bae, S.M.; Kim, J.W. Psychometric Properties of the Internet Addiction Test: A Systematic Review and Meta-Analysis. Cyberpsychol. Behav. Soc. Netw. 2018, 21, 473–484. [Google Scholar] [CrossRef] [PubMed]
- Neelapaijit, A.; Pinyopornpanish, M.; Simcharoen, S.; Kuntawong, P.; Wongpakaran, N.; Wongpakaran, T. Psychometric properties of a Thai version internet addiction test. BMC Res. Notes 2018, 11, 69. [Google Scholar] [CrossRef]
- Siste, K.; Suwartono, C.; Nasrun, M.W.; Bardosono, S.; Sekartini, R.; Pandelaki, J.; Sarasvita, R.; Murtani, B.J.; Damayanti, R.; Wiguna, T. Validation study of the Indonesian internet addiction test among adolescents. PLoS ONE 2021, 16, e0245833. [Google Scholar] [CrossRef] [PubMed]
- Tateno, M.; Teo, A.R.; Shiraishi, M.; Tayama, M.; Kawanishi, C.; Kato, T.A. Prevalence rate of Internet addiction among Japanese college students: Two cross-sectional studies and reconsideration of cut-off points of Young’s Internet Addiction Test in Japan. Psychiatry Clin. Neurosci. 2018, 72, 723–730. [Google Scholar] [CrossRef]
- Lu, X.; Yeo, K.J.; Guo, F.; Zhao, Z.; Wu, O. Psychometric property and measurement invariance of internet addiction test: The effect of socio-demographic and internet use variables. BMC Public Health 2022, 22, 1548. [Google Scholar] [CrossRef] [PubMed]
- Pawlikowskia, M.; Altstötter-Gleichb, C.; Brandac, M. Validation and psychometric properties of a short version of Young’s Internet Addiction Test. Comput. Hum. Behav. 2013, 29, 1212–1223. [Google Scholar] [CrossRef]
- Tafur-Mendoza, A.A.; Acosta-Prado, J.C.; Zarate-Torres, R.A.; Ramirez-Ospina, D.E. Assessing the Psychometric Properties of the Internet Addiction Test in Peruvian University Students. Int. J. Environ. Res. Public Health 2020, 17, 5782. [Google Scholar] [CrossRef] [PubMed]
- APA. Diagnostic and Statistical Manual of Mental Disorders: DSM-5; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Tateno, M.; Teo, A.R.; Kato, T.A. Does LINE addiction exist? Potential concerns about Japan’s most popular form of social media on smartphones. Psychiatry Clin. Neurosci. 2018, 72, 540–541. [Google Scholar] [CrossRef]
- Dufour, M.; Brunelle, N.; Tremblay, J.; Leclerc, D.; Cousineau, M.M.; Khazaal, Y.; Legare, A.A.; Rousseau, M.; Berbiche, D. Gender Difference in Internet Use and Internet Problems among Quebec High School Students. Can. J. Psychiatry 2016, 61, 663–668. [Google Scholar] [CrossRef]
- Lai, C.M.; Mak, K.K.; Cheng, C.; Watanabe, H.; Nomachi, S.; Bahar, N.; Young, K.S.; Ko, H.C.; Kim, D.; Griffiths, M.D. Measurement Invariance of the Internet Addiction Test among Hong Kong, Japanese, and Malaysian Adolescents. Cyberpsychol. Behav. Soc. Netw. 2015, 18, 609–617. [Google Scholar] [CrossRef]
- Mak, K.K.; Lai, C.M.; Watanabe, H.; Kim, D.I.; Bahar, N.; Ramos, M.; Young, K.S.; Ho, R.C.; Aum, N.R.; Cheng, C. Epidemiology of internet behaviors and addiction among adolescents in six Asian countries. Cyberpsychol. Behav. Soc. Netw. 2014, 17, 720–728. [Google Scholar] [CrossRef]
- Wery, A.; Burnay, J.; Karila, L.; Billieux, J. The Short French Internet Addiction Test Adapted to Online Sexual Activities: Validation and Links With Online Sexual Preferences and Addiction Symptoms. J. Sex Res. 2016, 53, 701–710. [Google Scholar] [CrossRef]
- Wegmann, E.; Oberst, U.; Stodt, B.; Brand, M. Online-specific fear of missing out and Internet-use expectancies contribute to symptoms of Internet-communication disorder. Addict. Behav. Rep. 2017, 5, 33–42. [Google Scholar] [CrossRef]
- Wegmann, E.; Stodt, B.; Brand, M. Addictive use of social networking sites can be explained by the interaction of Internet use expectancies, Internet literacy, and psychopathological symptoms. J. Behav. Addict. 2015, 4, 155–162. [Google Scholar] [CrossRef]
- Muller, S.M.; Wegmann, E.; Garcia Arias, M.; Bernabeu Brotons, E.; Marchena Giraldez, C.; Brand, M. Deficits in executive functions but not in decision making under risk in individuals with problematic social-network use. Compr. Psychiatry 2021, 106, 152228. [Google Scholar] [CrossRef] [PubMed]
- Tran, B.X.; Mai, H.T.; Nguyen, L.H.; Nguyen, C.T.; Latkin, C.A.; Zhang, M.W.B.; Ho, R.C.M. Vietnamese validation of the short version of Internet Addiction Test. Addict. Behav. Rep. 2017, 6, 45–50. [Google Scholar] [CrossRef] [PubMed]
- WHO. International Classification of Diseases 11th Revision (ICD-11); World Health Organization (WHO): Geneva, Switzerland, 2019. [Google Scholar]
- Higuchi, S.; Osaki, Y.; Kinjo, A.; Mihara, S.; Maezono, M.; Kitayuguchi, T.; Matsuzaki, T.; Nakayama, H.; Rumpf, H.J.; Saunders, J.B. Development and validation of a nine-item short screening test for ICD-11 gaming disorder (GAMES test) and estimation of the prevalence in the general young population. J. Behav. Addict. 2021, 10, 263–280. [Google Scholar] [CrossRef] [PubMed]
- R_Core_Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Fay, M.P. Two-sided Exact Tests and Matching Confidence Intervals for Discrete Data. R J. 2010, 2, 53–58. [Google Scholar] [CrossRef]
- Robin, X.; Turck, N.; Hainard, A.; Tiberti, N.; Lisacek, F.; Sanchez, J.C.; Muller, M. pROC: An open-source package for R and S+ to analyze and compare ROC curves. BMC Bioinform. 2011, 12, 77. [Google Scholar] [CrossRef] [PubMed]
- Mihara, S.; Osaki, Y.; Kinjo, A.; Matsuzaki, T.; Nakayama, H.; Kitayuguchi, T.; Harada, T.; Higuchi, S. Validation of the Ten-Item Internet Gaming Disorder Test (IGDT-10) based on the clinical diagnosis of IGD in Japan. J. Behav. Addict. 2022, 11, 1024–1034. [Google Scholar] [CrossRef]


{kind=link}
| Overall | Non-Addicted | Addicted | p-Value | |
|---|---|---|---|---|
| n = 104 | n = 90 | n = 14 | (Welch’s t-Test or $ Fisher’s Exact Test) | |
| Age (Age range) Early/Late teens | 14.4 ± 2.4 (10–18) 57/47 | 14.4 ± 2.5 (10–18) 47/43 | 14.1 ± 1.9 (11–18) 10/4 | p = 0.5446 p = 0.2507 $ |
| Gender (M/F) | 80/24 | 71/19 | 9/5 | p = 0.3042 $ |
| IQ | 82.8 ± 14.0 | 82.8 ± 14.1 | 82.2 ± 14.0 | p = 0.8798 |
| IAT (20 items) | 43.7 ± 12.4 | 41.6 ± 11.0 | 56.8 ± 13.1 | p = 0.0012 |
| s-IAT (12 items) | 27.4 ± 7.9 | 26.2 ± 6.9 | 35.5 ± 9.0 | p = 0.0023 |
| Overall | Non-Addicted | Addicted | p-Value | |
|---|---|---|---|---|
| n = 104 | n = 90 | n = 14 | (Fisher’s Exact Test) | |
| s-IAT ≥ 35 | 22 | 12 | 10 | p = 0.07986 |
| IAT ≥ 50 | 35 | 25 | 10 | |
| IAT ≥ 70 | 2 | 0 | 2 |
| Sensitivity | Specificity | FPR | FNR | PPV | NPV | PLR | NLR | |
|---|---|---|---|---|---|---|---|---|
| s-IAT (CO35) | 0.714 | 0.867 | 0.133 | 0.286 | 0.455 | 0.951 | 5.357 | 0.330 |
| IAT (CO50) | 0.714 | 0.722 | 0.278 | 0.286 | 0.286 | 0.942 | 2.571 | 0.396 |
| IAT (CO70) | 0.143 | 1.00 | 0 | 0.857 | 1.00 | 0.882 | - | 0.857 |
| (A) s-IAT (CO35) and IAT (CO50) | ||||
| s-IAT ≥ 35 | s-IAT < 35 | Sum | p-Value (McNemar) | |
| IAT ≥ 50 | 21 | 14 | 35 | p = 0.00098 |
| IAT < 50 | 1 | 68 | 69 | |
| Sum | 22 | 82 | 104 | |
| (B) s-IAT (CO35) and IAT (CO70) | ||||
| s-IAT ≥ 35 | s-IAT < 35 | Sum | p-Value (McNemar) | |
| IAT ≥ 70 | 2 | 0 | 2 | p < 0.00001 |
| IAT < 70 | 20 | 82 | 102 | |
| Sum | 22 | 82 | 104 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tateno, M.; Horie, K.; Shirasaka, T.; Nanba, K.; Shiraishi, E.; Tateno, Y.; Kato, T.A. Clinical Usefulness of a Short Version of the Internet Addiction Test to Screen for Probable Internet Addiction in Adolescents with Autism Spectrum Disorder. Int. J. Environ. Res. Public Health 2023, 20, 4670. https://doi.org/10.3390/ijerph20054670
Tateno M, Horie K, Shirasaka T, Nanba K, Shiraishi E, Tateno Y, Kato TA. Clinical Usefulness of a Short Version of the Internet Addiction Test to Screen for Probable Internet Addiction in Adolescents with Autism Spectrum Disorder. International Journal of Environmental Research and Public Health. 2023; 20(5):4670. https://doi.org/10.3390/ijerph20054670
Chicago/Turabian StyleTateno, Masaru, Kazumasa Horie, Tomohiro Shirasaka, Kotaro Nanba, Eri Shiraishi, Yukie Tateno, and Takahiro A. Kato. 2023. "Clinical Usefulness of a Short Version of the Internet Addiction Test to Screen for Probable Internet Addiction in Adolescents with Autism Spectrum Disorder" International Journal of Environmental Research and Public Health 20, no. 5: 4670. https://doi.org/10.3390/ijerph20054670
APA StyleTateno, M., Horie, K., Shirasaka, T., Nanba, K., Shiraishi, E., Tateno, Y., & Kato, T. A. (2023). Clinical Usefulness of a Short Version of the Internet Addiction Test to Screen for Probable Internet Addiction in Adolescents with Autism Spectrum Disorder. International Journal of Environmental Research and Public Health, 20(5), 4670. https://doi.org/10.3390/ijerph20054670