
Critical Success Factors for Successful Implementation of Healthcare 4.0: A Literature Review and Future Research Agenda




Abstract
1. Introduction
- RQ1:
- What are the critical success factors for the successful implementation of H 4.0?
- RQ2:
- How should research on H 4.0 proceed given our findings?
2. Literature Review
2.1. Smartness
2.2. Interconnectedness
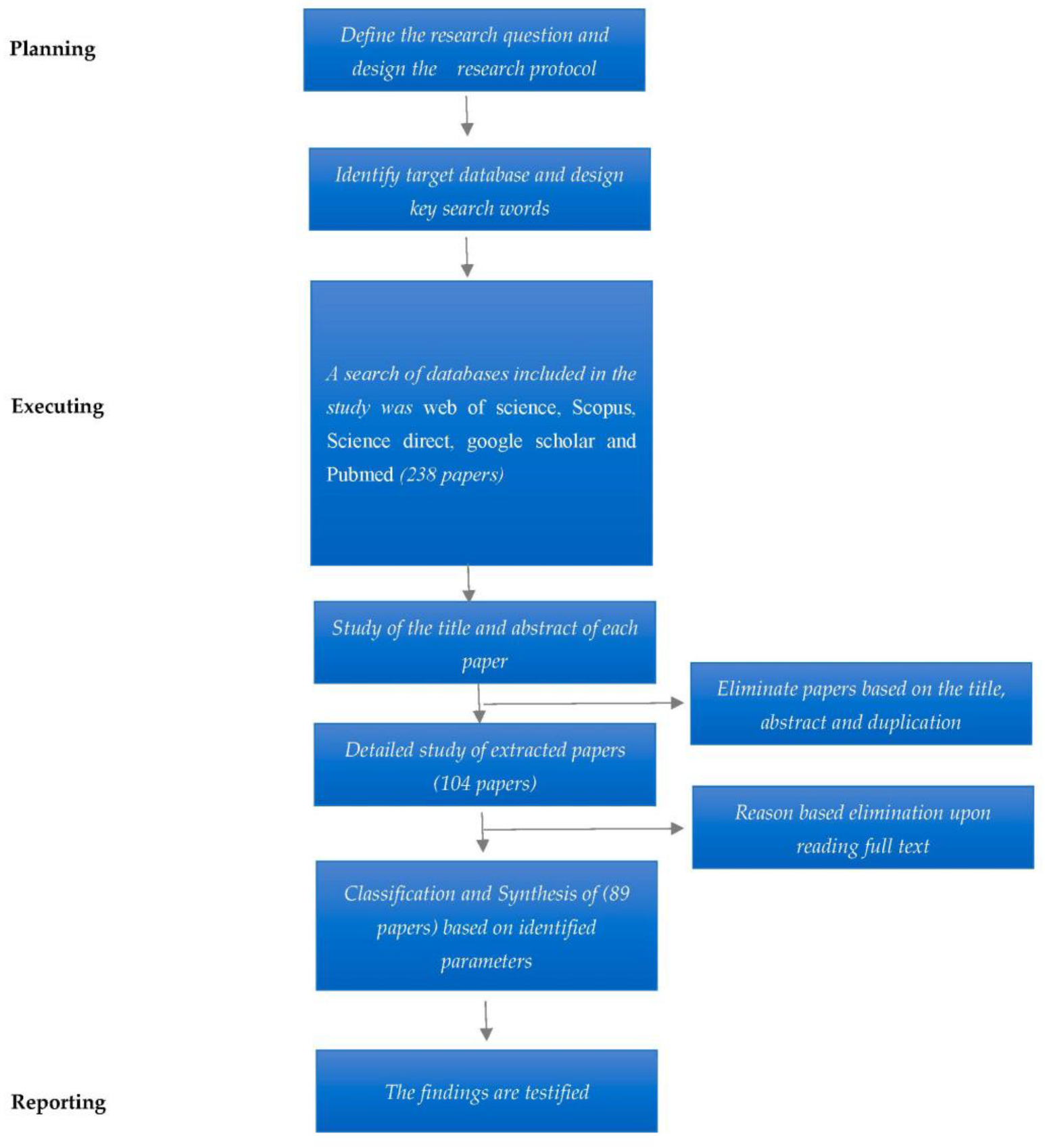
3. Research Method
3.1. Data Sources
3.2. Screening
3.3. Data Analysis
4. Results
4.1. Descriptive Analysis
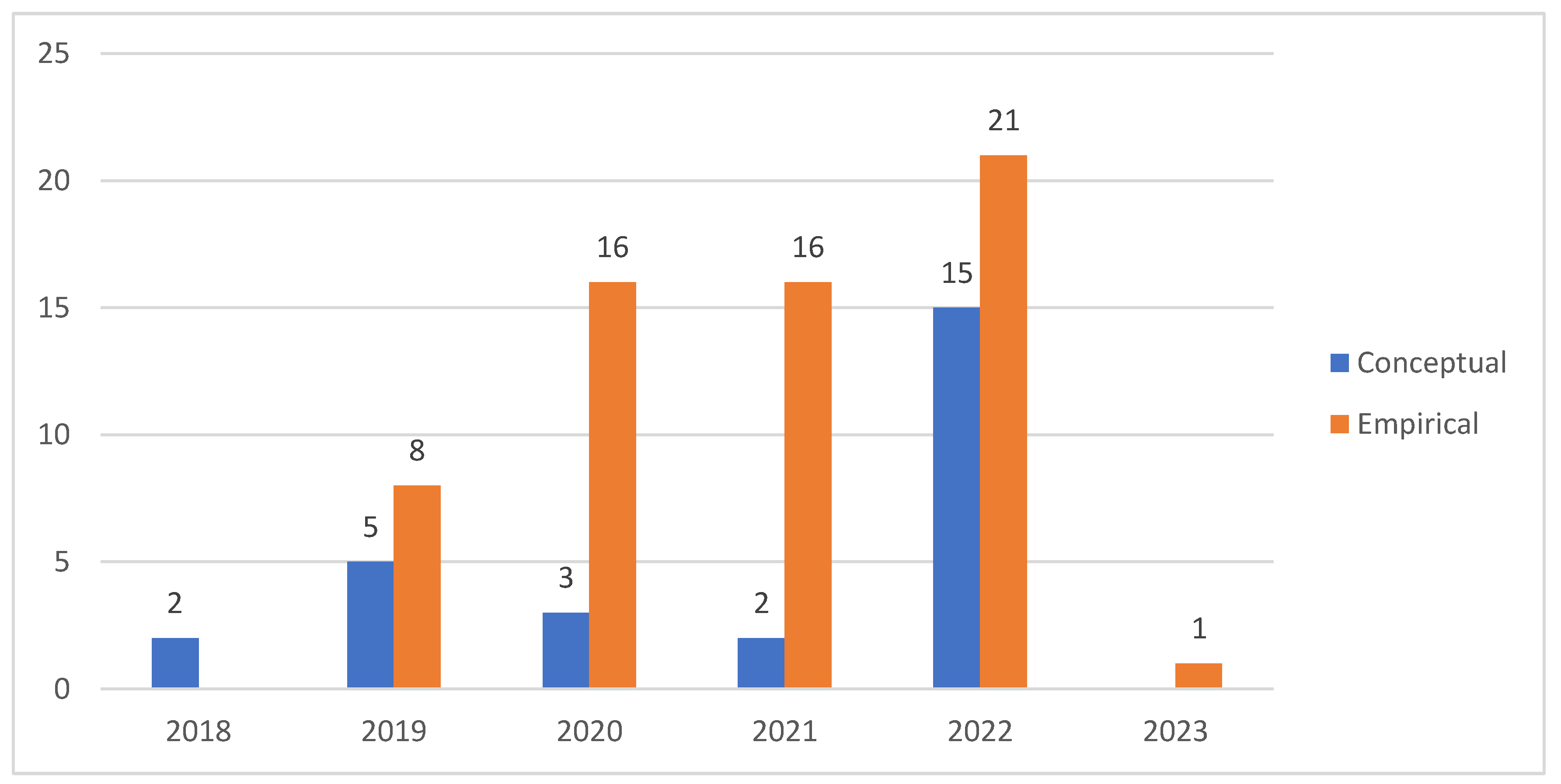
4.1.1. Timeline Distribution
4.1.2. Number of Authors
4.1.3. Productive and Influential Authors
4.1.4. Influential Authors
4.1.5. Top Source Journal
4.1.6. Countries
4.1.7. Keyword Analysis
4.1.8. Type of Study
4.2. Thematic Analysis of Articles
4.2.1. Digital Integration and Interconnectedness of the Healthcare Ecosystem
4.2.2. Human-Centric Automation of Healthcare Providers
4.2.3. Improve Patient-Centricity and the Patient Experience
4.2.4. Use Big Data and Analytics
4.2.5. Managing Digital Healthcare Supply Chains
4.2.6. Strategies for Promoting H 4.0
4.2.7. Promote a Culture for H 4.0
4.2.8. Healthcare Leadership
4.2.9. Healthcare Employees’ Skills
4.2.10. Adoption of New Business Models
5. Discussion
5.1. Individual Impact of CSFs on Successful Implementaiton of H 4.0
5.2. Interdependnace of CSFs for Sucessful Implemenation of H 4.0
6. Scope for Future Research
- This study finds ten critical success factors for the successful implementation of H 4.0. None of the studies in the literature explicitly addressed all the factors for the successful implementation of H 4.0, indicating the need for studies that explicitly outline the factors that could impact the implementation of H 4.0.
- Another interesting area of future research could be qualitatively exploring the success factors in various healthcare subsectors. Studies may examine whether these factors may differ, for example, in biotechnology, pharmaceuticals, equipment, facilities, distribution, and managed healthcare.
- Studies should also quantitively rank the critical success factors so that the importance of these factors can be examined in various settings such as between developed and developing countries. In addition, understanding the relevance of these factors will help in developing a framework for the successful implementation of H 4.0.
- Human-centric automation design is gaining importance in healthcare systems. Healthcare systems are sociotechnical systems, and hence, to be successful, there is a need for a high level of compatibility between social and technical systems. Future studies should explore the relationship between human-centric automation and the success of H 4.0 implementation.
- H 4.0 success depends on its ability to improve the patient experience and patient-centricity [53,76]. Future studies should examine how H 4.0 technologies impact the various dimensions of the patient experience. There is also a need for longitudinal studies to understand the time-oriented changes patients experience with the use of digital technologies.
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Keyword String

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Part 1 | Part 2 | Part 3 |
|---|---|---|
| Industry 4.0 | Advantages | Health system |
| Or | Or | Or |
| Industrie 4.0 | Benefits | Hospitals |
| Or | Or | Or |
| The fourth industrial revolution | Pros | Health centre |
| Or | Or | Or |
| The 4th industrial revolution | Strength | Health |
| Or | Or | Or |
| Healthcare 4.0 | Strengths | Primary care |
| Or | Or | Or |
| Heath 4.0 | Positives | Secondary care |
| Or | Or | Or |
| Medical 4.0 | Gains | Tertiary care |
| Or | Or | Or |
| Cyber physical system | Pluses | Nursing home |
| Or | Or | Or |
| Medical Cyber physical system | Highlights | Clinic |
| Or | Or | Or |
| CPS | Positive effects | Hospice |
| Or | Or | |
| MCPS | Implementation | |
| Or | Or | |
| Internet of things | Successful implementation | |
| Or | Or | |
| Big data | Success factors | |
| Or | ||
| Digitization | ||
| Or | ||
| Digitization | ||
| Or | ||
| Digitilisation | ||
| Or | ||
| Digitisation |
References
- Abbate, S.; Centobelli, P.; Cerchione, R.; Oropallo, E.; Riccio, E. Blockchain Technology for Embracing Healthcare 4.0; IEEE Transactions on Engineering Management; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2022; pp. 1–12. [Google Scholar]
- Afferni, P.; Merone, M.; Soda, P. Hospital 4.0 and its innovation in methodologies and technologies. In Proceedings of the 2018 IEEE 31st International Symposium on Computer-Based Medical Systems (CBMS), Karlstad, Sweden, 18–21 June 2018; pp. 333–338. [Google Scholar]
- Al-Jaroodi, J.; Mohamed, N.; Abukhousa, E. Health 4.0: On the Way to Realizing the Healthcare of the Future. IEEE Access 2020, 8, 211189–211210. [Google Scholar] [CrossRef] [PubMed]
- Melo, J.A.G.D.M.E.C.E.; Araújo, N.M.F. Impact of the Fourth Industrial Revolution on the Health Sector: A Qualitative Study. Health Inform. Res. 2020, 26, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Atallah, L.; Lo, B.; Ali, R.; King, R.; Yang, G.-Z. Real-Time Activity Classification Using Ambient and Wearable Sensors. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 1031–1039. [Google Scholar] [CrossRef] [PubMed]
- Awad, A.; Trenfield, S.J.; Gaisford, S.; Basit, A.W. 3D printed medicines: A new branch of digital healthcare. Int. J. Pharm. 2018, 548, 586–596. [Google Scholar] [CrossRef]
- Jamkhaneh, H.B.; Tortorella, G.L.; Parkouhi, S.V.; Shahin, R. A comprehensive framework for classification and selection of H4.0 digital technologies affecting healthcare processes in the grey environment. TQM J. 2022, 34, 1914–1941. [Google Scholar] [CrossRef]
- Beaulieu, M.; Bentahar, O. Digitalization of the healthcare supply chain: A roadmap to generate benefits and effectively support healthcare delivery. Technol. Forecast. Soc. Chang. 2021, 167, 120717. [Google Scholar] [CrossRef]
- Brown, D.; Fleron, A.; Singhal, S.; Ungermann, C. The Gathering Storm: An Opportunity to Reorder the Healthcare Industry, McKinsey and Company. 2022. Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/the-gathering-storm-an-opportunity-to-reorder-the-healthcare-industry (accessed on 17 November 2022).
- Buchelt, B.; Frączkiewicz-Wronka, A.; Dobrowolska, M. The Organizational Aspect of Human Resource Management as a Determinant of the Potential of Polish Hospitals to Manage Medical Professionals in Healthcare 4.0. Sustainability 2020, 12, 5118. [Google Scholar] [CrossRef]
- Burke, L.A.; Hutchins, H. Training Transfer: An Integrative Literature Review; Development Review; Sage Publications: Los Angeles, CA, USA, 2007; Volume 6, pp. 263–296. [Google Scholar] [CrossRef]
- Cabells. Predatory Reports. 2018. Available online: https://www2.cabells.com/ (accessed on 30 January 2023).
- Carpenter, M. Use of Robotics in Surgery: Current Trends, Challenges, and the Future; Artificial Intelligence; Chapman and Hall/CRC: Boca Raton, FL, USA, 2021; pp. 195–202. [Google Scholar]
- Chen, B.; Baur, A.; Stepniak, M.; Wang, J. Finding the Future of Care Provision: The Role of Smart Hospitals; McKinsey & Company: Sydney, NSW, Australia, 2019; Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/finding-the-future-of-care-provision-the-role-of-smart-hospitals (accessed on 30 January 2023).
- Chen, C.; Loh, E.-W.; Kuo, K.N.; Tam, K.-W. The Times they Are a-Changin’—Healthcare 4.0 Is Coming! J. Med. Syst. 2019, 44, 40. [Google Scholar] [CrossRef]
- Chute, C.; French, T. Introducing care 4.0: An integrated care paradigm built on industry 4.0 capabilities. Int. J. Environ. Res. Public Health 2019, 16, 2247. [Google Scholar] [CrossRef]
- Ciasullo, M.V.; Orciuoli, F.; Douglas, A.; Palumbo, R. Putting Health 4.0 at the service of Society 5.0: Exploratory insights from a pilot study. Socio-Econ. Plan. Sci. 2021, 80, 101163. [Google Scholar] [CrossRef]
- Conn, V.S.; Isaramalai, S.-A.; Rath, S.; Jantarakupt, P.; Wadhawan, R.; Dash, Y. Beyond MEDLINE for literature searches. J. Nurs. Sch. 2003, 35, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Darwish, L.R.; Farag, M.M.; El-Wakad, M.T. Towards Reinforcing Healthcare 4.0: A Green Real-Time IIoT Scheduling and Nesting Architecture for COVID-19 Large-Scale 3D Printing Tasks; IEEE Access; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2020; Volume 8, pp. 213916–213927. [Google Scholar]
- Durach, C.F.; Kembro, J.; Wieland, A. A New Paradigm for Systematic Literature Reviews in Supply Chain Management. J. Supply Chain Manag. 2017, 53, 67–85. [Google Scholar] [CrossRef]
- Ferlie, E.; Montgomery, K.; Pedersen, A.R. The Oxford Handbook of Health Care Management; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Furstenau, L.B.; Zani, C.; Terra, S.X.; Sott, M.K.; Choo, K.-K.R.; Saurin, T.A. Resilience capabilities of healthcare supply chain and supportive digital technologies. Technol. Soc. 2022, 71, 102095. [Google Scholar] [CrossRef]
- Figueroa, C.A.; Harrison, R.; Chauhan, A.; Meyer, L. Priorities and challenges for health leadership and workforce management globally: A rapid review. BMC Health Serv. Res. 2019, 19, 239. [Google Scholar] [CrossRef] [PubMed]
- Gbouna, Z.V.; Pang, G.; Yang, G.; Hou, Z.; Lv, H.; Yu, Z.; Pang, Z. User-Interactive Robot Skin with Large-Area Scalability for Safer and Natural Human-Robot Collaboration in Future Telehealthcare. IEEE J. Biomed. Health Inform. 2021, 25, 4276–4288. [Google Scholar] [CrossRef]
- Gisby, S.; Micca, P.; Kheyn-Kheyfets, B.; Chang, C.; Wagh, M. New Business Models in Health Care: Building Platform-Enabled Ecosystems. 2021. Available online: https://www2.deloitte.com/content/dam/insights/articles/us165009_chs-health-care-ecosystem/DI_CHS-Health-care-ecosystem.pdf (accessed on 8 September 2022).
- Golinelli, D.; Boetto, E.; Carullo, G.; Nuzzolese, A.G.; Landini, M.P.; Fantini, M.P. Adoption of Digital Technologies in Health Care During the COVID-19 Pandemic: Systematic Review of Early Scientific Literature. J. Med. Internet Res. 2020, 22, e22280. [Google Scholar] [CrossRef]
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef]
- Galetsi, P.; Katsaliaki, K.; Kumar, S. Values, challenges and future directions of big data analytics in healthcare: A systematic review. Soc. Sci. Med. 2019, 241, 112533. [Google Scholar] [CrossRef]
- Fletcher, G.; Griffiths, M. Digital Transformation during a Lockdown. Int. J. Inf. Manag. 2020, 55, 102185. [Google Scholar] [CrossRef]
- Guk, K.; Han, G.; Lim, J.; Jeong, K.; Kang, T.; Lim, E.-K.; Jung, J. Evolution of Wearable Devices with Real-Time Disease Monitoring for Personalized Healthcare. Nanomaterials 2019, 9, 813. [Google Scholar] [CrossRef]
- Haidegger, T.; Speidel, S.; Stoyanov, D.; Satava, R.M. Robot-Assisted Minimally Invasive Surgery—Surgical Robotics in the Data Age. Proc. IEEE 2022, 110, 835–846. [Google Scholar] [CrossRef]
- Hasselgren, A.; Rensaa, J.-A.H.; Kralevska, K.; Gligoroski, D.; Faxvaag, A. Blockchain for Increased Trust in Virtual Health Care: Proof-of-Concept Study. J. Med. Internet Res. 2021, 23, e28496. [Google Scholar] [CrossRef] [PubMed]
- Hathaliya, J.J.; Tanwar, S.; Evans, R. Securing electronic healthcare records: A mobile-based biometric authentication approach. J. Inf. Secur. Appl. 2020, 53, 102528. [Google Scholar] [CrossRef]
- Hathaliya, J.J.; Tanwar, S.; Tyagi, S.; Kumar, N. Securing Electronics Healthcare Records in Healthcare 4.0: A Biometric-Based Approach; Computers and Electrical Engineering; Elsevier Ltd.: Amsterdam, The Netherlands, 2019; Volume 76, pp. 398–410. [Google Scholar]
- Inuwa, H.M.; Ravi Raja, A.; Kumar, A.; Singh, B.; Singh, S. Status of Industry 4.0 Applications in Healthcare 4.0 and Pharma 4.0; Materials Today: Proceedings; Elsevier Ltd.: Amsterdam, The Netherlands, 2022; Volume 62, pp. 3593–3598. [Google Scholar]
- Tranfield, D.; Denyer, D.; Smart, P. Towards a Methodology for Developing Evidence-Informed Management Knowledge by Means of Systematic Review. Br. J. Manag. 2003, 14, 207–222. [Google Scholar] [CrossRef]
- Jaleel, A.; Mahmood, T.; Hassan, M.A.; Bano, G.; Khurshid, S.K. Towards Medical Data Interoperability Through Collaboration of Healthcare Devices. IEEE Access 2020, 8, 132302–132319. [Google Scholar] [CrossRef]
- Jayaraman, P.P.; Forkan, A.R.M.; Morshed, A.; Haghighi, P.D.; Kang, Y.-B. Healthcare 4.0: A Review of Frontiers in Digital Health; Wiley Interdisciplinary Reviews: Data Mining and Knowledge Discovery; Wiley Online Library: New York, NY, USA, 2020; Volume 10, p. e1350. [Google Scholar]
- Jecker, N.S. Nothing to be ashamed of: Sex robots for older adults with disabilities. J. Med. Ethic. 2020, 47, 26–32. [Google Scholar] [CrossRef]
- Kang, B.H.; Park, K.; Hambsch, M.; Hong, S.; Kim, H.T.; Choi, D.H.; Lee, J.H.; Kim, S.; Kim, H.J. Skin-conformable photoplethysmogram sensors for energy-efficient always-on cardiovascular monitoring systems. Nano Energy 2021, 92, 106773. [Google Scholar] [CrossRef]
- Kishor, A.; Chakraborty, C. Artificial Intelligence and Internet of Things Based Healthcare 4.0 Monitoring System. Wirel. Pers. Commun. 2021, 127, 1615–1631. [Google Scholar] [CrossRef]
- Kitsios, F.; Kapetaneas, N. Digital Transformation in Healthcare 4.0: Critical Factors for Business Intelligence Systems. Information 2022, 13, 247. [Google Scholar] [CrossRef]
- Kolling, M.; Furstenau, L.; Sott, M.; Rabaioli, B.; Ulmi, P.; Bragazzi, N.; Tedesco, L. Data Mining in Healthcare: Applying Strategic Intelligence Techniques to Depict 25 Years of Research Development. Int. J. Environ. Res. Public Health 2021, 18, 3099. [Google Scholar] [CrossRef]
- Krishnamoorthy, S.; Dua, A.; Gupta, S. Role of emerging technologies in future IoT-driven Healthcare 4.0 technologies: A survey, current challenges and future directions. J. Ambient. Intell. Humaniz. Comput. 2021, 14, 361–407. [Google Scholar] [CrossRef]
- Kumar, A.; Krishnamurthi, R.; Nayyar, A.; Sharma, K.; Grover, V.; Hossain, E. A Novel Smart Healthcare Design, Simulation, and Implementation Using Healthcare 4.0 Processes; IEEE Access; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2020; Volume 8, pp. 118433–118471. [Google Scholar]
- Kumari, A.; Tanwar, S.; Tyagi, S.; Kumar, N. Fog Computing for Healthcare 4.0 Environment: Opportunities and Challenges; Computers and Electrical Engineering; Elsevier Ltd.: Amsterdam, The Netherlands, 2018; Volume 72, pp. 1–13. [Google Scholar]
- Li, J.; Carayon, P. Health Care 4.0: A Vision for Smart and Connected Health Care; IISE Transactions on Healthcare Systems Engineering; Taylor & Francis: Boca Raton, FL, USA, 2021; Volume 11, pp. 171–180. [Google Scholar]
- Liaw, C.-Y.; Guvendiren, M. Current and emerging applications of 3D printing in medicine. Biofabrication 2017, 9, 024102. [Google Scholar] [CrossRef] [PubMed]
- Loeza-Mejía, C.-I.; Sánchez-DelaCruz, E.; Pozos-Parra, P.; Landero-Hernández, L.-A. The Potential and Challenges of Health 4.0 to Face COVID-19 Pandemic: A Rapid Review; Health and Technology; Springer: New York, NY, USA, 2021; Volume 11, pp. 1321–1330. [Google Scholar]
- Lucas, H. Information and communications technology for future health systems in developing countries. Soc. Sci. Med. 2008, 66, 2122–2132. [Google Scholar] [CrossRef] [PubMed]
- Mannion, R.; Davies, H. Understanding organisational culture for healthcare quality improvement. BMJ 2018, 363, k4907. [Google Scholar] [CrossRef] [PubMed]
- Mavrogiorgou, A.; Kiourtis, A.; Perakis, K.; Miltiadou, D.; Pitsios, S.; Kyriazis, D. Analyzing data and data sources towards a unified approach for ensuring end-to-end data and data sources quality in healthcare 4.0. Comput. Methods Programs Biomed. 2019, 181, 104967. [Google Scholar] [CrossRef]
- Mavrogiorgou, A.; Kiourtis, A.; Touloupou, M.; Kapassa, E.; Kyriazis, D. Internet of Medical Things (IoMT): Acquiring and Transforming Data into HL7 FHIR through 5G Network Slicing. Emerg. Sci. J. 2019, 3, 64. [Google Scholar] [CrossRef]
- Mlakar, I.; Kampič, T.; Flis, V.; Kobilica, N.; Molan, M.; Smrke, U.; Plohl, N.; Bergauer, A. Study Protocol: A Survey Exploring Patients’ and Healthcare Professionals’ Expectations, Attitudes and Ethical Acceptability Regarding the Integration of Socially Assistive Humanoid Robots in Nursing. BMJ Open 2022, 12, e054310. [Google Scholar] [CrossRef]
- Nash, D.B. Health 3.0; Pharmacy and Therapeutics; MediMedia: Morrisville, PA, USA, 2008; Volume 33, p. 69. [Google Scholar]
- Okoli, C. A guide to conducting a systematic literature review of information systems research. Commun. Assoc. Inf. Syst. 2015, 37, 579–910. [Google Scholar] [CrossRef]
- Ong, T.L.; Ruppert, M.M.B.; Akbar, M.B.; Rashidi, P.; Ozrazgat-Baslanti, T.; Bihorac, A.M.; Suvajdzic, M. Improving the Intensive Care Patient Experience with Virtual Reality—A Feasibility Study. Crit. Care Explor. 2020, 2, e0122. [Google Scholar] [CrossRef]
- Pang, Z.; Yang, G.; Khedri, R.; Zhang, Y.-T. Introduction to the Special Section: Convergence of Automation Technology, Biomedical Engineering, and Health Informatics Toward the Healthcare 4.0; IEEE Reviews in Biomedical Engineering; IEEE: Piscataway, NJ, USA, 2018; Volume 11, pp. 249–259. [Google Scholar]
- Paul, S.; Riffat, M.; Yasir, A.; Mahim, M.N.; Sharnali, B.Y.; Naheen, I.T.; Rahman, A.; Kulkarni, A. Industry 4.0 applications for medical/healthcare services. J. Sens. Actuator Netw. 2021, 10, 43. [Google Scholar] [CrossRef]
- Phares, J.; Dobrzykowski, D.D.; Prohofsky, J. How policy is shaping the macro healthcare delivery supply chain: The emergence of a new tier of retail medical clinics. Bus. Horizons 2021, 64, 333–345. [Google Scholar] [CrossRef]
- Pillai, A.S.; Mathew, P.S. Impact of Virtual Reality in Healthcare: A Review; Virtual and Augmented Reality in Mental Health Treatment; IGI Global: Hershey, PA, USA, 2019; pp. 17–31. [Google Scholar]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews; A Product from the ESRC Methods Programme Version; Institute of Health Research Lancaster: Bailrigg, UK, 2006; Volume 1, p. b92. [Google Scholar]
- Pu, C.; Zerkle, H.; Wall, A.; Lim, S.; Choo, K.-K.R.; Ahmed, I. A Lightweight and Anonymous Authentication and Key Agreement Protocol for Wireless Body Area Networks. IEEE Internet Things J. 2022, 9, 21136–21146. [Google Scholar] [CrossRef]
- Qiu, H.; Qiu, M.; Liu, M.; Memmi, G. Secure Health Data Sharing for Medical Cyber-Physical Systems for the Healthcare 4.0. IEEE J. Biomed. Health Inform. 2020, 24, 2499–2505. [Google Scholar] [CrossRef] [PubMed]
- Robbins, D.A.; Curro, F.A.; Fox, C.H. Defining Patient-Centricity: Opportunities, Challenges, and Implications for Clinical Care and Research. Ther. Innov. Regul. Sci. 2013, 47, 349–355. [Google Scholar] [CrossRef]
- Rodrigues, V.F.; Righi, R.D.R.; da Costa, C.A.; Antunes, R.S. Smart Hospitals and IoT Sensors: Why Is QoS Essential Here? J. Sens. Actuator Netw. 2022, 11, 33. [Google Scholar] [CrossRef]
- Sakurai, E.; Kurashige, K.; Tsuruta, S.; Sakurai, Y.; Knauf, R.; Damiani, E.; Kutics, A.; Frati, F. Embodiment matters: Toward culture-specific robotized counselling. J. Reliab. Intell. Environ. 2020, 6, 129–139. [Google Scholar] [CrossRef]
- Schein, E.H. Organizational Culture and Leadership; John Wiley & Sons: New York, NY, USA, 2010; Volume 2. [Google Scholar]
- Sharma, D.; Singh Aujla, G.; Bajaj, R. Evolution from Ancient Medication to Human-Centered Healthcare 4.0: A Review on Health Care Recommender Systems. Int. J. Commun. Syst. 2019, 9, e4058. [Google Scholar] [CrossRef]
- Sinha, K.K.; Kohnke, E.J. Health Care Supply Chain Design: Toward Linking the Development and Delivery of Care Globally. Decis. Sci. 2009, 40, 197–212. [Google Scholar] [CrossRef]
- Smith, K.B.; Profetto-McGrath, J.; Cummings, G.G. Emotional intelligence and nursing: An integrative literature review. Int. J. Nurs. Stud. 2009, 46, 1624–1636. [Google Scholar] [CrossRef]
- Sony, M.; Antony, J.; McDermott, O. The Impact of Healthcare 4.0 on the Healthcare Service Quality: A Systematic Literature Review; Hospital Topics, Taylor & Francis: New York, NY, USA, 2022; pp. 1–17. [Google Scholar]
- Spatharou, A.; Hieronimus, S.; Jenkins, J. Transforming Healthcare with AI: The Impact on the Workforce and Organizations; McKinsey & Company: Sydney, NSW, Australia, 2020; Volume 10. [Google Scholar]
- Stephanie, V.; Khalil, I.; Atiquzzaman, M.; Yi, X. Trustworthy Privacy-Preserving Hierarchical Ensemble and Federated Learning in Healthcare 4.0 with Blockchain; IEEE Transactions on Industrial Informatics; IEEE Computer Society: Washington, DC, USA, 2022; pp. 1–10. [Google Scholar]
- Tanwar, S.; Kumari, A.; Vekaria, D.; Kumar, N.; Sharma, R. An AI-based disease detection and prevention scheme for COVID-19. Comput. Electr. Eng. 2022, 103, 108352. [Google Scholar] [CrossRef]
- Tanwar, S.; Parekh, K.; Evans, R. Blockchain-based electronic healthcare record system for healthcare 4.0 applications. J. Inf. Secur. Appl. 2019, 50, 102407. [Google Scholar] [CrossRef]
- Teng, F.; Ma, Z.; Chen, J.; Xiao, M.; Huang, L. Automatic Medical Code Assignment via Deep Learning Approach for Intelligent Healthcare. IEEE J. Biomed. Health Inform. 2020, 24, 2506–2515. [Google Scholar] [CrossRef] [PubMed]
- Tortorella, G.; Prashar, A.; Samson, D.; Kurnia, S.; Fogliatto, F.S.; Capurro, D.; Antony, J. Resilience development and digitalization of the healthcare supply chain: An exploratory study in emerging economies. Int. J. Logist. Manag. 2022, 34, 130–163. [Google Scholar] [CrossRef]
- Dima, A.; Bugheanu, A.-M.; Boghian, R.; Madsen, D. Mapping Knowledge Area Analysis in E-Learning Systems Based on Cloud Computing. Electronics 2022, 12, 62. [Google Scholar] [CrossRef]
- Tortorella, G.L.; Fogliatto, F.S.; Kurnia, S.; Thürer, M.; Capurro, D. Healthcare 4.0 digital applications: An empirical study on measures, bundles and patient-centered performance. Technol. Forecast. Soc. Chang. 2022, 181, 121780. [Google Scholar] [CrossRef]
- Tortorella, G.L.; Fogliatto, F.S.; Mac Cawley Vergara, A.; Vassolo, R.; Sawhney, R. Healthcare 4.0: Trends, Challenges and Research Directions; Production Planning & Control; Taylor & Francis: Boca Raton, FL, USA, 2020; Volume 31, pp. 1245–1260. [Google Scholar]
- Tortorella, G.L.; Saurin, T.A.; Fogliatto, F.S.; Rosa, V.M.; Tonetto, L.M.; Magrabi, F. Impacts of Healthcare 4.0 Digital Technologies on the Resilience of Hospitals. Technol. Forecast. Soc. Change 2021, 166, 120666. [Google Scholar] [CrossRef]
- Valtolina, S.; Barricelli, B.R.; Di Gaetano, S. Communicability of traditional interfaces VS chatbots in healthcare and smart home domains. Behav. Inf. Technol. 2019, 39, 108–132. [Google Scholar] [CrossRef]
- van Overbeeke, E.; Vanbinst, I.; Jimenez-Moreno, A.C.; Huys, I. Patient Centricity in Patient Preference Studies: The Patient Perspective. Front. Med. 2020, 7, 93. [Google Scholar] [CrossRef]
- Wahl, B.; Cossy-Gantner, A.; Germann, S.; Schwalbe, N.R. Artificial intelligence (AI) and global health: How can AI contribute to health in resource-poor settings? BMJ Glob. Health 2018, 3, e000798. [Google Scholar] [CrossRef]
- Wehde, M. Healthcare 4.0; IEEE Engineering Management Review; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2019; Volume 47, pp. 24–28. [Google Scholar]
- Whittemore, R. Combining Evidence in Nursing Research: Methods and Implications. Nurs. Res. 2005, 54, 56–62. [Google Scholar] [CrossRef]
- Yang, G.; Pang, Z.; Deen, M.J.; Dong, M.; Zhang, Y.-T.; Lovell, N.; Rahmani, A.M. Homecare Robotic Systems for Healthcare 4.0: Visions and Enabling Technologies. IEEE J. Biomed. Health Inform. 2020, 24, 2535–2549. [Google Scholar] [CrossRef] [PubMed]
- Selvakkumaran, S.; Ahlgren, E.O. Determining the factors of household energy transitions: A multi-domain study. Technol. Soc. 2018, 57, 54–75. [Google Scholar] [CrossRef]
- Yadav, N.R.; Jain, M.; Sharma, A.; Singh, S.; Jain, V.; Khanna, B.; Singh, A.; Chhibber, R. Fostering cognizance of organ donation: An education-based approach. J. Fam. Med. Prim. Care 2019, 8, 4021–4026. [Google Scholar] [CrossRef] [PubMed]









| Sr No | Author | Articles | Total Citations |
|---|---|---|---|
| 1 | Fogliatto F.S. | 12 | 157 |
| 2 | Kumar N. | 11 | 1038 |
| 3 | Tanwar S. | 11 | 1361 |
| 4 | Tortorella G.L. | 11 | 156 |
| 5 | Tyagi S. | 7 | 979 |
| 6 | Pang Z. | 5 | 127 |
| 7 | Vassolo R. | 5 | 100 |
| 8 | Yang G. | 5 | 127 |
| 9 | Narayanamurthy G. | 4 | 51 |
| 10 | Saurin T.A. | 4 | 53 |
| 11 | Tonetto L.M. | 4 | 53 |
| ID | Author | Documents | Total Citations | CPP |
|---|---|---|---|---|
| 1 | Parekh K. | 1 | 339 | 339 |
| 2 | Mistry I. | 1 | 273 | 273 |
| 3 | Evans R. | 2 | 363 | 181.5 |
| 4 | Tyagi S. | 7 | 979 | 139.86 |
| 5 | Kumari A. | 2 | 271 | 135.5 |
| 6 | Tanwar S. | 11 | 1361 | 123.73 |
| 7 | Kumar N. | 11 | 1038 | 94.36 |
| 8 | Liu M. | 1 | 90 | 90 |
| 9 | Memmi G. | 1 | 90 | 90 |
| 10 | Qiu H. | 1 | 90 | 90 |
| CPP = citations per publication | ||||
| ID | Source | Documents |
|---|---|---|
| 1 | IEEE J. Biomed. Health Inform. | 5 |
| 2 | IEEE Trans. Ind. Inform. | 5 |
| 3 | IEEE Access | 4 |
| 4 | Comput. Electr. Eng. | 3 |
| 5 | IEEE Internet Things J. | 3 |
| 6 | Int. J. Prod. Res. | 3 |
| 7 | Technol. Forecast. Soc. Change | 3 |
| 8 | IEEE Netw. | 2 |
| 9 | IEEE Trans. Eng. Manag. | 2 |
| 10 | IEEE Trans. Netw. Sci. Eng. | 2 |
| ID | Country | Documents | Citations |
|---|---|---|---|
| 1 | India | 34 | 1670 |
| 2 | Brazil | 19 | 246 |
| 3 | Australia | 16 | 124 |
| 4 | China | 12 | 202 |
| 5 | United Kingdom | 12 | 536 |
| 6 | United States | 11 | 315 |
| 7 | Argentina | 10 | 117 |
| 8 | Sweden | 7 | 162 |
| 9 | Canada | 5 | 139 |
| 10 | Chile | 5 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sony, M.; Antony, J.; Tortorella, G.L. Critical Success Factors for Successful Implementation of Healthcare 4.0: A Literature Review and Future Research Agenda. Int. J. Environ. Res. Public Health 2023, 20, 4669. https://doi.org/10.3390/ijerph20054669
Sony M, Antony J, Tortorella GL. Critical Success Factors for Successful Implementation of Healthcare 4.0: A Literature Review and Future Research Agenda. International Journal of Environmental Research and Public Health. 2023; 20(5):4669. https://doi.org/10.3390/ijerph20054669
Chicago/Turabian StyleSony, Michael, Jiju Antony, and Guilherme L. Tortorella. 2023. "Critical Success Factors for Successful Implementation of Healthcare 4.0: A Literature Review and Future Research Agenda" International Journal of Environmental Research and Public Health 20, no. 5: 4669. https://doi.org/10.3390/ijerph20054669
APA StyleSony, M., Antony, J., & Tortorella, G. L. (2023). Critical Success Factors for Successful Implementation of Healthcare 4.0: A Literature Review and Future Research Agenda. International Journal of Environmental Research and Public Health, 20(5), 4669. https://doi.org/10.3390/ijerph20054669