
24-Hour Movement Behaviours (Physical Activity, Sedentary Behaviour and Sleep) Association with Glycaemic Control and Psychosocial Outcomes in Adolescents with Type 1 Diabetes: A Systematic Review of Quantitative and Qualitative Studies

 , ,
, ,  , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Scientific Rigor
2.2. Inclusion Criteria
2.3. Population/Sample
2.4. Intervention/Exposure and Phenomenon of Interest
2.5. Comparisons and Design
2.6. Outcomes and Evaluation
2.7. Study and Research Type
2.8. Search Strategy
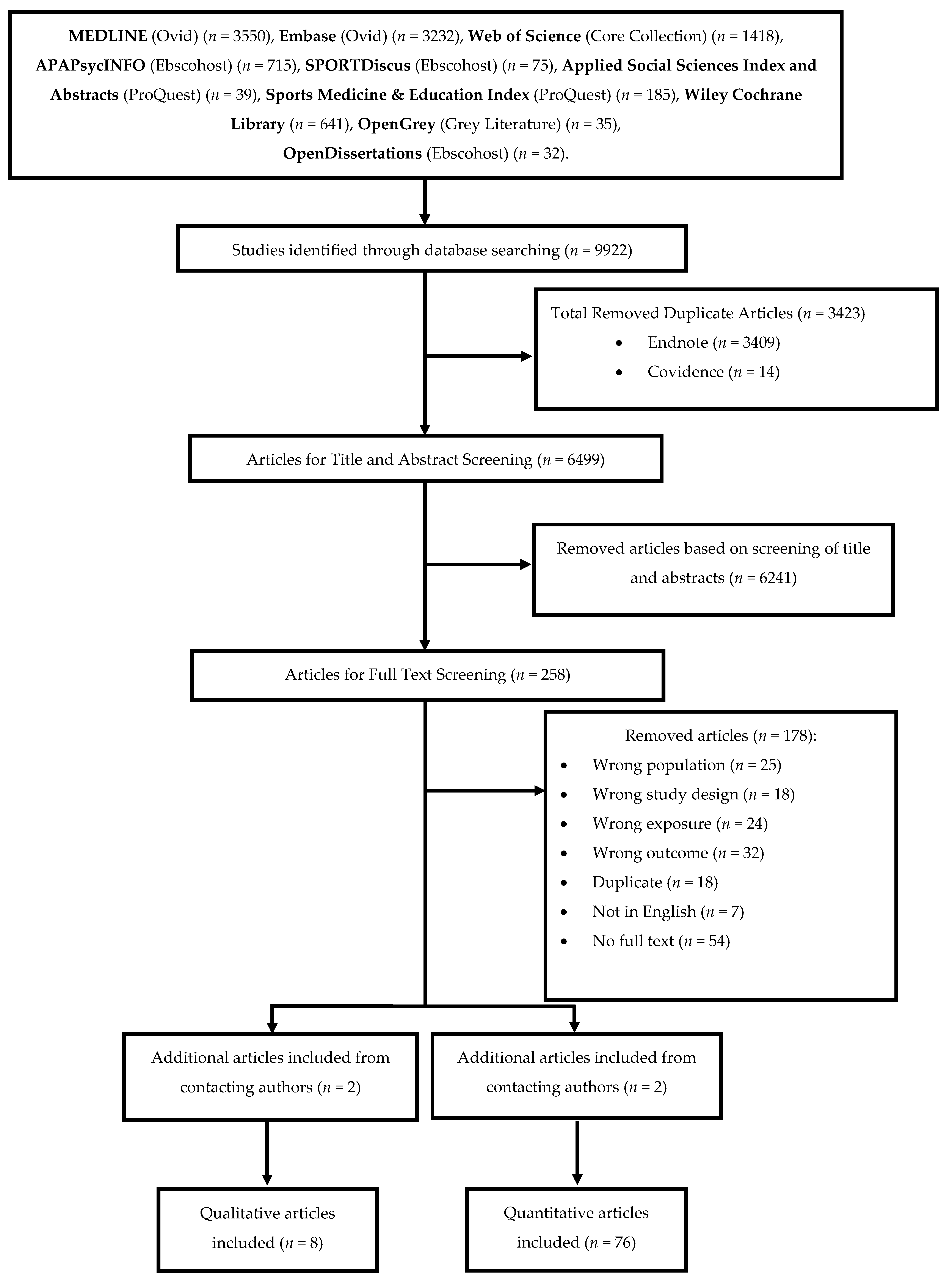
2.9. Screening Process
2.10. Data Extraction
2.11. Quality Assessment
2.12. Data Synthesis
2.12.1. Narrative Synthesis of Quantitative Studies
2.12.2. Narrative Synthesis of Qualitative Studies
2.12.3. Meta-Analysis Synthesis
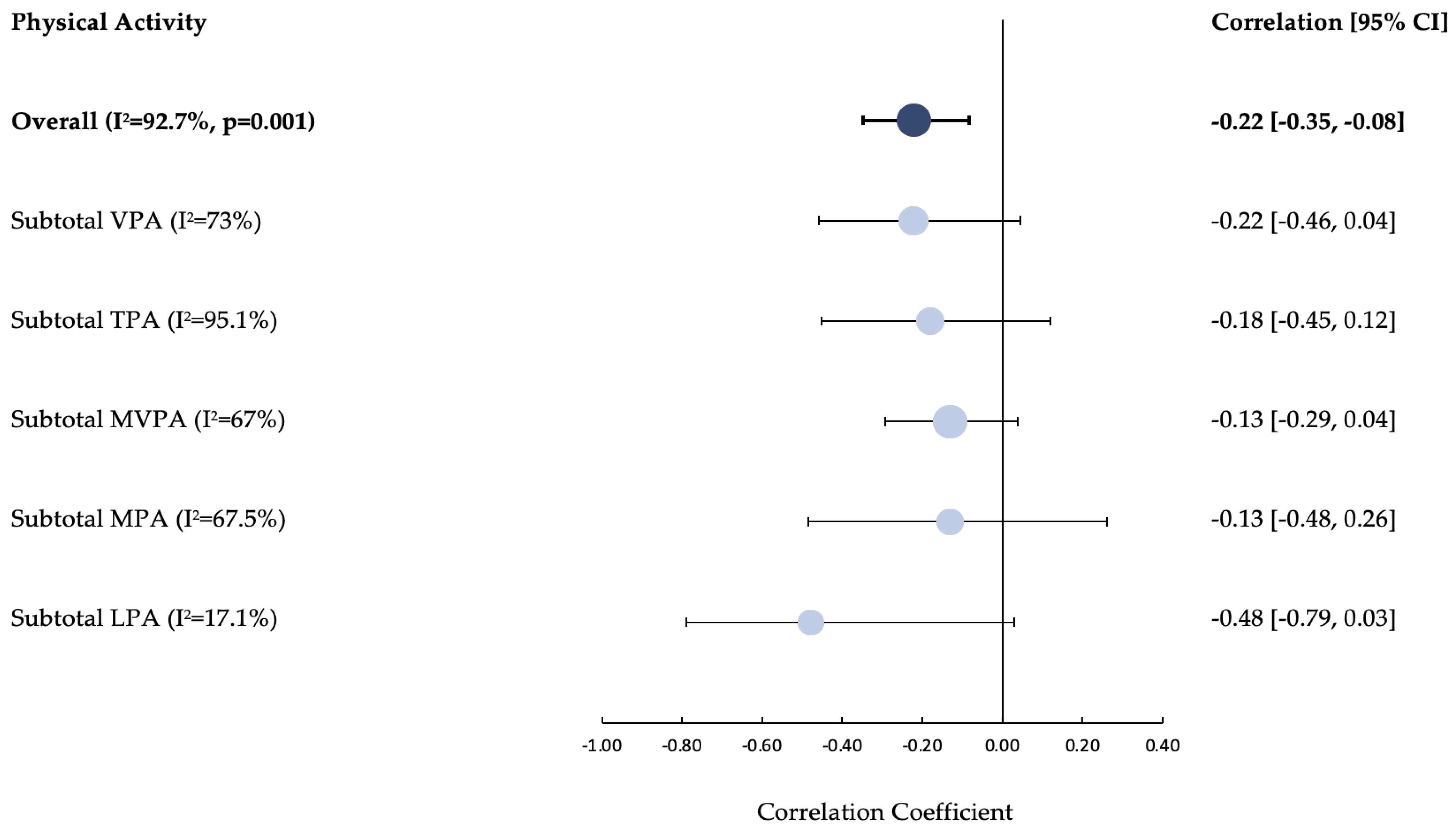
- PA and HbA1c (Subgroups = Light-PA (LPA), Moderate-PA (MPA), Vigorous-PA (VPA), Moderate-Vigorous-PA (MVPA) and Total-PA (TPA)).
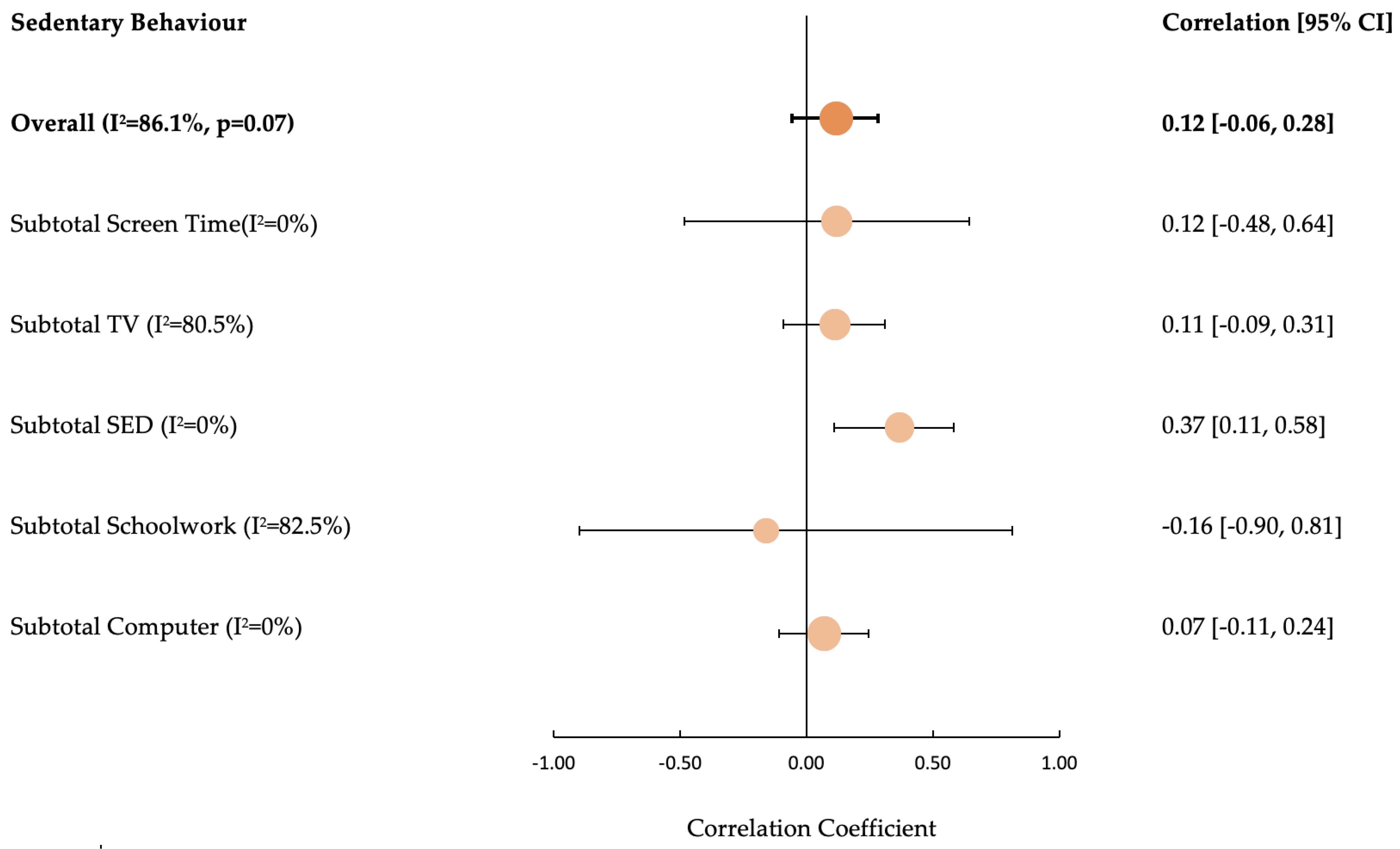
- SB and HbA1c (Subgroups = Computer, TV, Total Screen Time, Schoolwork and Total Sedentary Time).
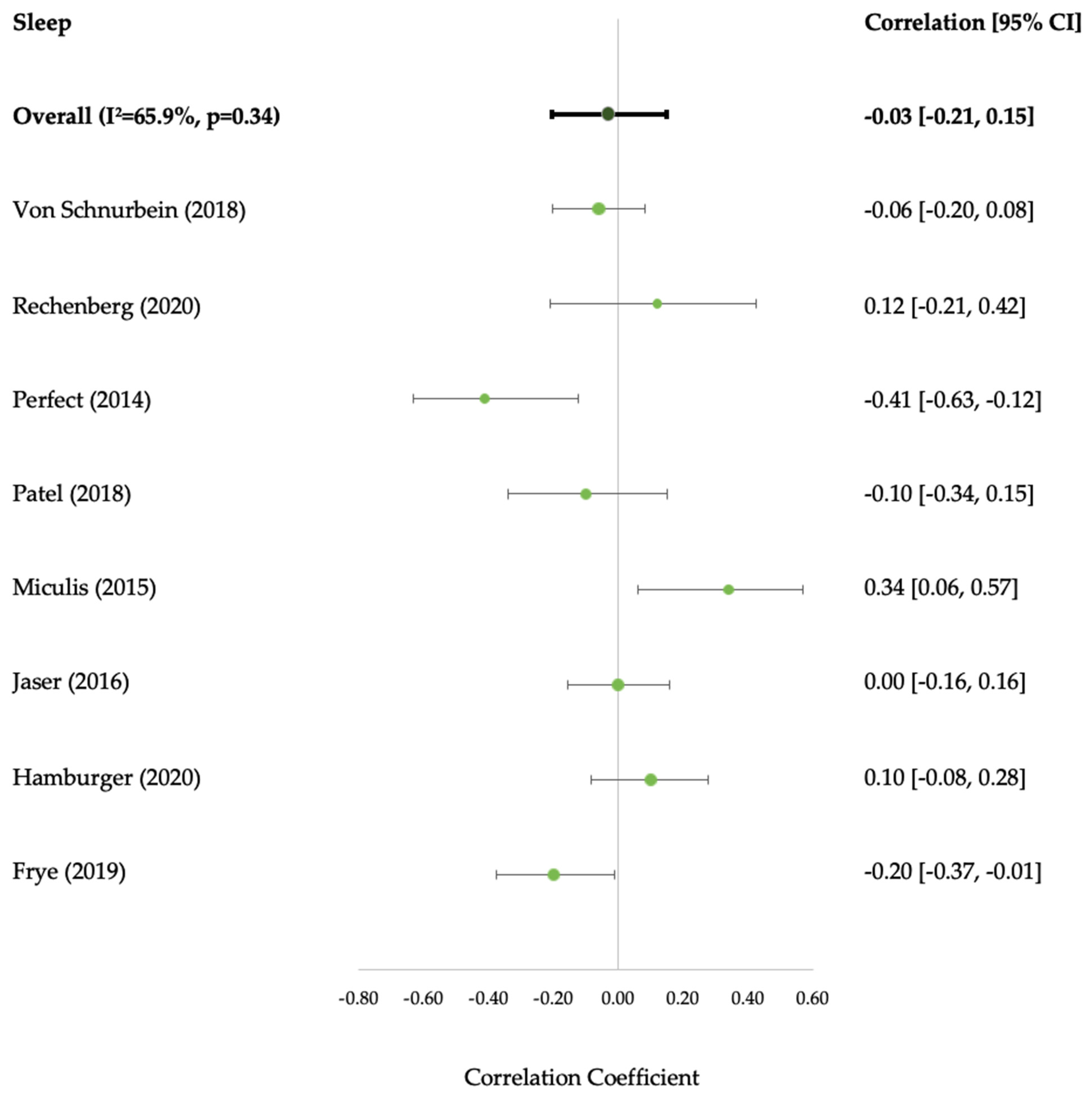
- Sleep and HbA1c (Duration dimension only due to study heterogeneity).
3. Results
3.1. Characteristics of Identified Studies
3.2. Movement Behaviour Composition
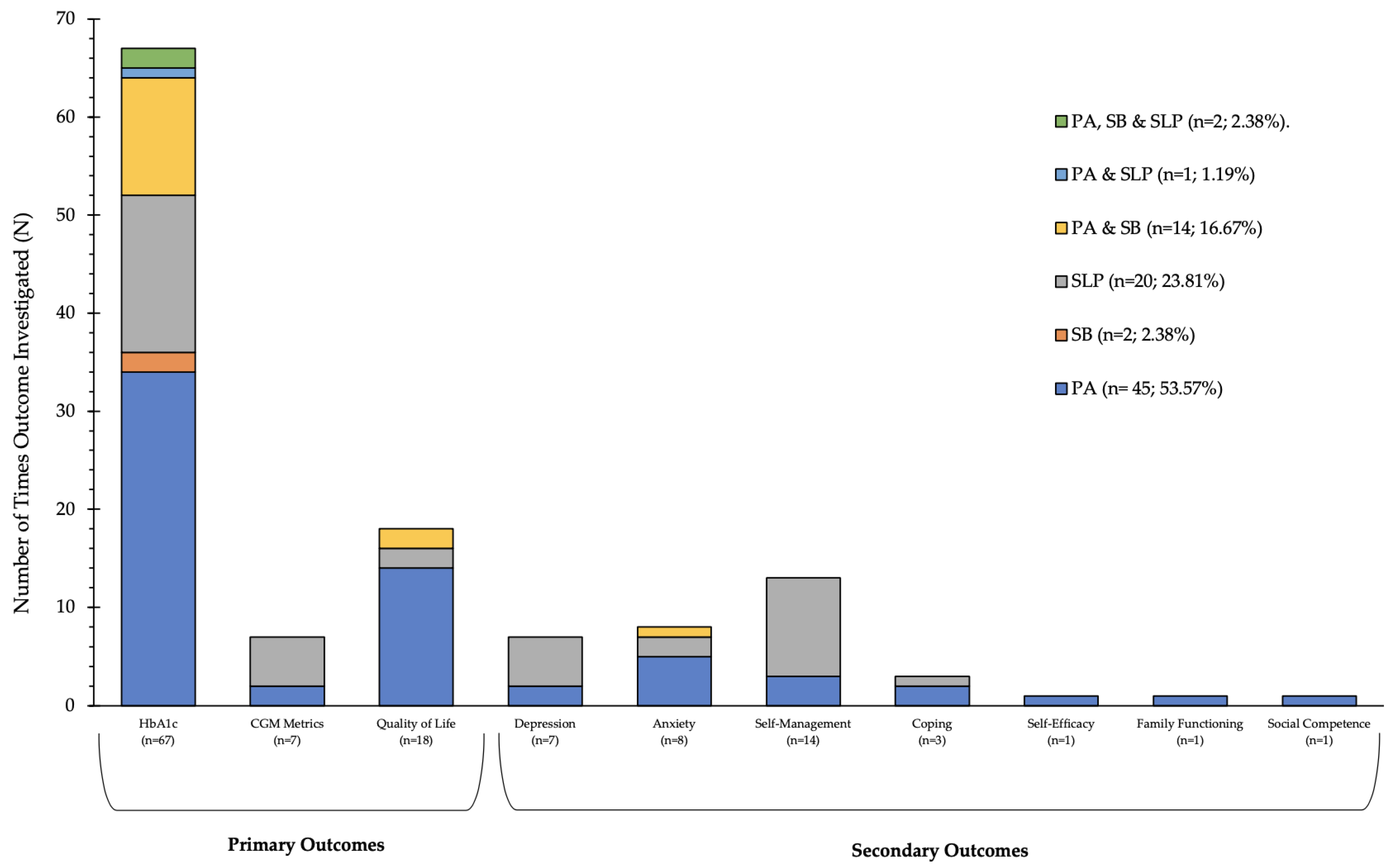
3.3. Included Articles Primary and Secondary Outcome Composition
3.4. Physical Activity
3.5. Sedentary Behaviour
3.6. Sleep
3.7. Qualitative Studies
‘‘It helps to sort of control. I don’t really know why but I felt that um, if I’m doing more exercise um I can normally keep my levels at a more consistent rate”.[Adolescent, p4] [104]
“What we’ve learned is that physical activity keeps the spikes and the lows more moderate so you don’t fluctuate as much… the physical activity just makes that more stable”[Caregiver, p4] [108]
“I feel quite satisfied”, “cheerful”, “I like walking because it really relaxes me”[Adolescents, p7] [107]
“When you’re doing exercise you know you’re helping your body as well as yourself”[Adolescent, p5] [104]
“a way of getting out his anger”[Caregiver, p6] [109]
“because it’s funner with other people, like you can keep motivated, but you can also have a laugh while you’re doing it…’,[Adolescent, p153] [106]
“Usually [TEEN] sleeps fine, unless his blood sugar’s high. Then he’s up every couple hours”.[Caregiver p123] [102]
“I panic a lot because one night my blood sugar dropped in the middle of the night and I ended up like having a seizure”.[Adolescent, p550] [103]
“My mother sets an alarm for 2:30 in the morning and she comes and checks me so she doesn’t want me to have to get up in the middle of the night”.[Adolescent, p550] [103]
“I’m not my usual self. I don’t like do things, I just kinda sit”.[Adolescent, p546] [102]
“the lack of sleep would probably cause [her teen] to not be able to keep track of his blood sugars or test when he needs—it probably causes him to be a little lazy about it”[Caregiver, p546] [102]
4. Discussions
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Atkinson, M.A.; Eisenbarth, G.S.; Michels, A.W. Type 1 Diabetes. Lancet 2014, 383, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Craig, M.E.; Jefferies, C.; Dabelea, D.; Balde, N.; Seth, A.; Donaghue, K.C. Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr. Diabetes 2014, 15, 4–17. [Google Scholar] [CrossRef] [PubMed]
- Tuomilehto, J.; Ogle, G.D.; Lund-Blix, N.A.; Stene, L.C. Update on Worldwide Trends in Occurrence of Childhood Type 1 Diabetes in 2020. Pediatr. Endocrinol. Rev. 2020, 17, 198–209. [Google Scholar]
- Cameron, F.J.; Garvey, K.; Hood, K.K.; Acerini, C.L.; Codner, E. Ispad Clinical Practice Consensus Guidelines 2018: Diabetes in Adolescence. Pediatr. Diabetes 2018, 19, 250–261. [Google Scholar] [CrossRef] [PubMed]
- Miller, K.M.; Foster, N.C.; Beck, R.W.; Bergenstal, R.M.; DuBose, S.N.; DiMeglio, L.A.; Maahs, D.M.; Tamborlane, W.V.; T1D Exchange Clinic Network. Current State of Type 1 Diabetes Treatment in the U.S.: Updated Data from the T1d Exchange Clinic Registry. Diabetes Care 2015, 38, 971–978. [Google Scholar] [CrossRef] [PubMed]
- Hislop, A.L.; Fegan, P.G.; Schlaeppi, M.J.; Duck, M.; Yeap, B.B. Prevalence and associations of psychological distress in young adults with Type 1 diabetes. Diabet. Med. 2008, 25, 91–96. [Google Scholar] [CrossRef]
- Cameron, F.J.; Northam, E.A.; Ambler, G.R.; Daneman, D. Routine Psychological Screening in Youth with Type 1 Diabetes and Their Parents: A Notion Whose Time Has Come? Diabetes Care 2007, 30, 2716–2724. [Google Scholar] [CrossRef]
- Adolfsson, P.; Riddell, M.C.; Taplin, C.E.; Davis, E.A.; Fournier, P.A.; Annan, F.; Scaramuzza, A.E.; Hasnani, D.; Hofer, S.E. ISPAD Clinical Practice Consensus Guidelines 2018: Exercise in children and adolescents with diabetes. Pediatr. Diabetes 2018, 19, 205–226. [Google Scholar] [CrossRef]
- Pedišić, Z.; Dumuid, D.; Olds, T.S. Integrating Sleep, Sedentary Behaviour and Physical Activity Research in the Emerging Field of Time-Use Epidemiology:Definitions, Concepts, Statistical Methods, Theoretical Framework, and Future Directions. Kinesiology 2017, 49, 252–269. [Google Scholar]
- Rollo, S.; Antsygina, O.; Tremblay, M.S. The Whole Day Matters: Understanding 24-Hour Movement Guideline Adherence and Relationships with Health Indicators across the Lifespan. J. Sport Health Sci. 2020, 9, 493–510. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Cooke, A.; Smith, D.; Booth, A. Beyond Pico: The Spider Tool for Qualitative Evidence Synthesis. Qual. Health Res. 2012, 22, 1435–1443. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the Pico Framework to Improve Searching Pubmed for Clinical Questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Buysse, D.J. Sleep Health: Can We Define It? Does It Matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Battelino, T.; Danne, R.M.T.; Bergenstal, S.A.; Amiel, R.; Beck, T.; Biester, E.; Bosi, B.A.; Buckingham, W.T.; Cefalu, K.L.; Close, C.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations from the International Consensus on Time in Range. Diabetes Care 2019, 42, 1593–1603. [Google Scholar] [CrossRef]
- Danne, T.; Nimri, T.R.; Battelino, R.M.; Bergenstal, K.L.; Close, J.H.; DeVries, S.; Garg, L.; Heinemann, I.; Hirsch, S.A.; Amiel, R.; et al. International Consensus on Use of Continuous Glucose Monitoring. Diabetes Care 2017, 40, 1631–1640. [Google Scholar] [CrossRef]
- Whittemore, R.; Jaser, S.; Guo, J.; Grey, M. A conceptual model of childhood adaptation to type 1 diabetes. Nurs. Outlook 2010, 58, 242–251. [Google Scholar] [CrossRef] [PubMed]
- American Psychological Association. APA Dictionary of Psychology. Available online: https://dictionary.apa.org (accessed on 3 January 2021).
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-Duplication of Database Search Results for Systematic Reviews in Endnote. J. Med. Libr. Assoc. 2016, 104, 240. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater Reliability: The Kappa Statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme (CASP). CASP Checklists; Critical Appraisal Skills Programme (CASP): Oxford, UK, 2022. [Google Scholar]
- Strengthening the Reporting of Observational Studies in Epidemiology (STROBE). Strobe Checklist; Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Bern, Switzerland, 2022. [Google Scholar]
- Suurmond, R.; van Rhee, H.; Hak, T. Introduction, Comparison, and Validation of Meta-Essentials: A Free and Simple Tool for Meta-Analysis. Res. Synth. Methods 2017, 8, 537–553. [Google Scholar] [CrossRef] [PubMed]
- Peterson, R.A.; Brown, S.P. On the Use of Beta Coefficients in Meta-Analysis. J. Appl. Psychol. 2005, 90, 175–181. [Google Scholar] [CrossRef]
- Higgins, J.; Green, S.; Ben Van Den, A. Cochrane Handbook for Systematic Reviews of Interventions; Cochrane Collaborations: London, UK, 2011. [Google Scholar]
- Abdelmaksoud, A.A.; Salah, N.Y.; Ali, Z.M.; Rashed, H.R.; Abido, A.Y. Disturbed Sleep Quality and Architecture in Adolescents with Type 1 Diabetes Mellitus: Relation to Glycemic Control, Vascular Complications and Insulin Sensitivity. Diabetes Res. Clin. Pract. 2021, 174, 108774. [Google Scholar] [CrossRef] [PubMed]
- Al-Agha, A.; Ocheltree, A.; Hakeem, A. Metabolic Control in Children and Adolescents with Insulin-Dependent Diabetes Mellitus at King Abdul-Aziz University Hospital. J. Clin. Res. Pediatr. Endocrinol. 2011, 3, 202–207. [Google Scholar]
- Aman, J.; Skinner, T.C.; de Beaufort, C.E.; Swift, P.G.; Aanstoot, H.J.; Cameron, F.; Diabetes Hvidoere Study Group on Childhood. Associations between Physical Activity, Sedentary Behavior, and Glycemic Control in a Large Cohort of Adolescents with Type 1 Diabetes: The Hvidoere Study Group on Childhood Diabetes. Pediatr. Diabetes 2009, 10, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.J.; Laffel, L.M.; Domenger, C.; Danne, T.; Phillip, M.; Mazza, C.; Hanas, R.; Waldron, S.; Beck, R.W.; Calvi-Gries, F.; et al. Factors Associated with Diabetes-Specific Health-Related Quality of Life in Youth With Type 1 Diabetes: The Global TEENs Study. Diabetes Care 2017, 40, 1002–1009. [Google Scholar] [CrossRef]
- Ash, G.I.; Joiner, K.L.; Savoye, M.; Baker, J.S.; Gerosa, J.; Kleck, E.; Patel, N.S.; Sadler, L.S.; Stults-Kolehmainen, M.; Weinzimer, S.A.; et al. Feasibility and safety of a group physical activity program for youth with type 1 diabetes. Pediatr. Diabetes 2019, 20, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Beraki, Å.; Magnuson, A.; Särnblad, S.; Åman, J.; Samuelsson, U. Increase in physical activity is associated with lower HbA1c levels in children and adolescents with type 1 diabetes: Results from a cross-sectional study based on the Swedish pediatric diabetes quality registry (SWEDIABKIDS). Diabetes Res. Clin. Pract. 2014, 105, 119–125. [Google Scholar] [CrossRef]
- Bernardini, A.L.; Vanelli, M.; Chiari, G.; Iovane, B.; Gelmetti, C.; Vitale, R.; Errico, M.K. Adherence to physical activity in young people with type 1 diabetes. Acta Biomed. 2004, 75, 153–157. [Google Scholar]
- Bishop, F.K.; Wadwa, R.P.; Snell-Bergeon, J.; Nguyen, N.; Maahs, D.M. Changes in Diet and Physical Activity in Adolescents with and without Type 1 Diabetes over Time. Int. J. Pediatr. Endocrinol. 2014, 2014, 17. [Google Scholar] [CrossRef]
- Cuenca-Garcia, M.; Jago, R.; Shield, J.P.; Burren, C.P. How Does Physical Activity and Fitness Influence Glycaemic Control in Young People with Type 1 Diabetes? Diabet. Med. 2012, 29, e369–e376. [Google Scholar] [CrossRef]
- da Costa, L.M.F.C.; Vieira, S.E. Quality of Life of Adolescents with Type 1 Diabetes. Clinics 2015, 70, 173–179. [Google Scholar] [CrossRef] [PubMed]
- De Lima, V.A.; Mascarenhas, L.P.G.; Decimo, J.P.; De Souza, W.C.; Monteiro, A.L.S.; Lahart, I.; França, S.N.; Leite, N. Physical Activity Levels of Adolescents with Type 1 Diabetes Physical Activity in T1D. Pediatr. Exerc. Sci. 2017, 29, 213–219. [Google Scholar] [CrossRef]
- Edmunds, S.; Roche, D.; Stratton, G.; Wallymahmed, K.; Glenn, S.M. Physical activity and psychological well-being in children with Type 1 diabetes. Psychol. Health Med. 2007, 12, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Edmunds, S.; Roche, D.; Stratton, G. Levels and Patterns of Physical Activity in Children and Adolescents With Type 1 Diabetes and Associated Metabolic and Physiologic Health Outcomes. J. Phys. Act. Health 2010, 7, 68–77. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Fainardi, V.; Scarabello, C.; Cangelosi, A.; Fanciullo, L.; Mastrorilli, C.; Giannini, C.; Mohn, A.; Iafusco, D.; La Loggia, A.; Lombardo, F.; et al. Physical activity and sedentary lifestyle in children with type 1 diabetes: A multicentre Italian study. Acta Biomed. 2011, 82, 124–131. [Google Scholar]
- Faulkner, M.S.; Michaliszyn, S.F.; Hepworth, J.T. A personalized approach to exercise promotion in adolescents with type 1 diabetes. Pediatr. Diabetes 2009, 11, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, M.S.; Michaliszyn, S.; Hepworth, J.T.; Wheeler, M.D. Personalized Exercise for Adolescents with Diabetes or Obesity. Biol. Res. Nurs. 2014, 16, 46–54. [Google Scholar] [CrossRef]
- Frye, S.S.; Perfect, M.M.; Silva, G.E. Diabetes Management Mediates the Association between Sleep Duration and Glycemic Control in Youth with Type 1 Diabetes Mellitus. Sleep Med. 2019, 60, 132–138. [Google Scholar] [CrossRef]
- Galler, A.; Lindau, M.; Ernert, A.; Thalemann, R.; Raile, K. Associations between Media Consumption Habits, Physical Activity, Socioeconomic Status, and Glycemic Control in Children, Adolescents, and Young Adults with Type 1 Diabetes. Diabetes Care 2011, 34, 2356–2359. [Google Scholar] [CrossRef]
- Griggs, S.; Redeker, N.S.; Jeon, S.; Grey, M. Daily Variations in Sleep and Glucose in Adolescents with Type 1 Diabetes. Pediatr. Diabetes 2020, 21, 1493–1501. [Google Scholar] [CrossRef]
- Hamburger, E.R.; Goethals, E.R.; Choudhary, A.; Jaser, S.S. Sleep and depressive symptoms in adolescents with type 1 diabetes not meeting glycemic targets. Diabetes Res. Clin. Pract. 2020, 169, 108442. [Google Scholar] [CrossRef] [PubMed]
- Hanson, C.L.; De Guire, M.J.; Schinkel, A.M.; Kolterman, O.G.; Goodman, J.P.; Buckingham, B.A. Self-Care Behaviors in Insulin-Dependent Diabetes: Evaluative Tools and Their Associations with Glycemic Control. J. Pediatr. Psychol. 1996, 21, 467–482. [Google Scholar] [CrossRef] [PubMed]
- Hazen, R.A.; Fehr, K.K.; Fidler, A.; Cousino, M.K.; MacLeish, S.A.; Gubitosi-Klug, R. Sleep disruption in adolescents with Type 1 diabetes mellitus: Relationships with adherence and diabetes control. Diabetes Manag. 2015, 5, 257–265. [Google Scholar] [CrossRef]
- Herbst, A.; Bachran, R.; Kapellen, T.; Holl, R.W. Effects of Regular Physical Activity on Control of Glycemia in Pediatric Patients with Type 1 Diabetes Mellitus. Arch. Pediatr. Adolesc. Med. 2006, 160, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Herbst, A.; Kordonouri, O.; Schwab, K.O.; Schmidt, F.; Holl, R.W.; DPV Initiative of the German Working Group for Pediatric Diabetology Germany. Impact of Physical Activity on Cardiovascular Risk Factors in Children with Type 1 Diabetes: A Multicenter Study of 23,251 Patients. Diabetes Care 2007, 30, 2098–2100. [Google Scholar] [CrossRef] [PubMed]
- Jabbour, G. Vigorous Physical Activity Is Associated with Better Glycated Hemoglobin and Lower Fear of Hypoglycemia Scores in Youth with Type 1 Diabetes: A 2-Year Follow-Up Study. Front. Physiol. 2020, 11, 548417. [Google Scholar] [CrossRef]
- Jaser, S.S.; Ellis, D. Sleep in adolescents and young adults with type 1 diabetes: Associations with diabetes management and glycemic control. Health Psychol. Behav. Med. 2016, 4, 49–55. [Google Scholar] [CrossRef]
- Jaser, S.S.; Hamburger, E.R.; Bergner, E.M.; Williams, R.; Slaughter, J.C.; Simmons, J.H.; Malow, B.A. Sleep Coach Intervention for Teens with Type 1 Diabetes: Randomized Pilot Study. Pediatr. Diabetes 2020, 21, 473–478. [Google Scholar] [CrossRef]
- Johnson, S.B.; Freund, A.; Silverstein, J.; Hansen, C.A.; Malone, J. Adherence-health status relationships in childhood diabetes. Health Psychol. 1990, 9, 606–631. [Google Scholar] [CrossRef] [PubMed]
- Kahkoska, A.R.; Nguyen, C.T.; Jiang, X.; Adair, L.A.; Agarwal, S.; Aiello, A.E.; Burger, K.S.; Buse, J.B.; Dabelea, D.; Dolan, L.M.; et al. Characterizing the weight-glycemia phenotypes of type 1 diabetes in youth and young adulthood. BMJ Open Diabetes Res. Care 2020, 8, e000886. [Google Scholar] [CrossRef]
- Kalweit, K.L.; Briers, N.; Olorunju, S.A.S. The success of various management techniques used in South African children with type 1 diabetes mellitus. South Afr. Med. J. 2015, 105, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Kokkonen, J.; Taanla, A.; Kokkonen, E.-R. Diabetes in adolescence: The effect of family and psychologic factors on metabolic control. Nord. J. Psychiatry 1997, 51, 165–172. [Google Scholar] [CrossRef]
- Krzemińska, K.; Wieczorek, D.; Sitek, E.; Zaręba, W. Anxiety of physical activity and anxiety of hypoglycaemia in adolescents with diabetes mellitus type 1. Physiotherapy 2009, 17, 28–39. [Google Scholar] [CrossRef]
- Kummer, S.; Stahl-Pehe, K.A.; Castillo, C.; Bachle, C.; Graf, K.; Strassburger, B.; Salgin, E.; Mayatepek, G.; Giani, R.W.; Holl, T.; et al. Health Behaviour in Children and Adolescents with Type 1 Diabetes Compared to a Representative Reference Population. PLoS ONE 2014, 9, e112083. [Google Scholar] [CrossRef] [PubMed]
- Kyngäs, H. Compliance of adolescents with diabetes. J. Pediatr. Nurs. 2000, 15, 260–267. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Beech, B.; Crume, T.; Jr, R.B.D.; Dabelea, D.; Kaar, J.L.; Liese, A.D.; Mayer-Davis, E.J.; Pate, R.; Pettitt, D.J.; et al. Longitudinal association between television watching and computer use and risk markers in diabetes in the SEARCH for Diabetes in Youth Study. Pediatr. Diabetes 2014, 16, 382–391. [Google Scholar] [CrossRef]
- Lukács, A.; Mayer, K.; Juhász, E.; Varga, B.; Fodor, B.; Barkai, L. Reduced physical fitness in children and adolescents with type 1 diabetes. Pediatr. Diabetes 2012, 13, 432–437. [Google Scholar] [CrossRef]
- Lukács, A.; Mayer, K.; Török, A.; Kiss-Toth, E.; Barkai, L. Better cardiorespiratory fitness associated with favourable metabolic control and health-related quality of life in youths with type 1 diabetes mellitus. Acta Physiol. Hung. 2013, 100, 77–83. [Google Scholar] [CrossRef]
- Lukacs, A.; Sasvari, P.; Torok, A.; Barkai, L. Generic and Disease-Specific Quality of Life in Adolescents with Type 1 Diabetes: Comparison to Age-Matched Healthy Peers. J. Pediatr. Endocrinol. Metab. 2016, 29, 769–775. [Google Scholar] [CrossRef]
- Lukács, A.; Mayer, K.; Sasvári, P.; Barkai, L. Health-Related Quality of Life of Adolescents with Type 1 Diabetes in the Context of Resilience. Pediatr. Diabetes 2018, 19, 1481–1486. [Google Scholar] [CrossRef]
- Macaulay, G.C.; Galland, B.C.; Boucher, S.E.; Wiltshire, E.J.; Haszard, J.J.; Campbell, A.J.; Black, S.M.; Smith, C.; Elder, D.; Wheeler, B.J. Impact of Type 1 Diabetes Mellitus, Glucose Levels, and Glycemic Control on Sleep in Children and Adolescents: A Case-Control Study. Sleep 2020, 43, zsz226. [Google Scholar] [CrossRef] [PubMed]
- MacMillan, F.; Kirk, A.; Mutrie, N.; Robertson, K. Physical activity and sedentary behaviour in Scottish youth with type 1 diabetes. Pract. Diabetes 2014, 31, 228–233c. [Google Scholar] [CrossRef]
- Margeirsdottir, H.D.; Larsen, J.R.; Brunborg, C.; Sandvik, L.; Dahl-Jørgensen, K.; Diabetes Norwegian Study Group for Childhood. Strong Association between Time Watching Television and Blood Glucose Control in Children and Adolescents with Type 1 Diabetes. Diabetes Care 2007, 30, 1567–1570. [Google Scholar] [CrossRef][Green Version]
- Massin, M.M.; Lebrethon, M.-C.; Rocour, D.; Gérard, P.; Bourguignon, J.-P. Patterns of physical activity determined by heart rate monitoring among diabetic children. Arch. Dis. Child. 2005, 90, 1223–1226. [Google Scholar] [CrossRef] [PubMed]
- McDonough, R.J.; Clements, M.A.; DeLurgio, S.A.; Patton, S.R. Sleep Duration and Its Impact on Adherence in Adolescents with Type 1 Diabetes Mellitus. Pediatr. Diabetes 2017, 18, 262–270. [Google Scholar] [CrossRef]
- Michaliszyn, S.F.; Faulkner, M.S. Physical activity and sedentary behavior in adolescents with type 1 diabetes. Res. Nurs. Health 2010, 33, 441–449. [Google Scholar] [CrossRef]
- Miculis, C.P.; De Campos, W.; da Silva Boguszweski, M.C. Correlation between Glycemic Control and Physical Activity Level in Adolescents and Children with Type 1 Diabetes. J. Phys. Act. Health 2015, 12, 232–237. [Google Scholar] [CrossRef]
- Mitchell, F.; Wilkie, L.; Robertson, K.; Reilly, J.J.; Kirk, A. Feasibility and pilot study of an intervention to support active lifestyles in youth with type 1 diabetes: The ActivPals study. Pediatr. Diabetes 2018, 19, 443–449. [Google Scholar] [CrossRef]
- Mohammed, J.; Deda, L.; Clarson, C.L.; Stein, R.I.; Cuerden, M.S.; Mahmud, F.H. Assessment of Habitual Physical Activity in Adolescents with Type 1 Diabetes. Can. J. Diabetes 2014, 38, 250–255. [Google Scholar] [CrossRef]
- Mosso, C.; Halabi, V.; Ortiz, T.; Hodgson, M.I. Dietary intake, body composition, and physical activity among young patients with type 1 diabetes mellitus. J. Pediatr. Endocrinol. Metab. 2015, 28, 895–902. [Google Scholar] [CrossRef]
- Mozzillo, E.; Zito, E.; Maffeis, C.; De Nitto, E.; Maltoni, G.; Marigliano, M.; Zucchini, S.; Franzese, A.; Valerio, G. Unhealthy lifestyle habits and diabetes-specific health-related quality of life in youths with type 1 diabetes. Acta Diabetol. 2017, 54, 1073–1080. [Google Scholar] [CrossRef] [PubMed]
- Mutlu, E.B.R.U.; Mutlu, C.; Taskiran, H.; Özgen, İ. Relationship between Physical Activity Level and Depression, Anxiety, Quality of Life, Self-Esteem, and Hba1c in Adolescents with Type 1 Diabetes Mellitus. Turk. J. Physiother. Rehabil. Fiz. Rehabil. 2017, 28, 38–46. [Google Scholar]
- Naughton, M.J.; Yi-Frazier, J.P.; Morgan, T.M.; Seid, M.; Lawrence, J.M.; Klingensmith, G.J.; Waitzfelder, B.; Standiford, D.A.; Loots, B.; Search for Diabetes in Youth Study Group. Longitudinal Associations between Sex, Diabetes Self-Care, and Health-Related Quality of Life among Youth with Type 1 or Type 2 Diabetes Mellitus. J. Pediatr. 2014, 164, 1376–1383. [Google Scholar] [CrossRef]
- Neyman, A.; Woerner, S.; Russ, M.; Yarbrough, A.; DiMeglio, L.A. Strategies That Adolescents with Type 1 Diabetes Use in Relation to Exercise. Clin. Diabetes 2020, 38, 266–272. [Google Scholar] [CrossRef]
- Nguyen, T.; Obeid, J.; Walker, R.G.; Krause, M.P.; Hawke, T.J.; McAssey, K.; Vandermeulen, J.; Timmons, B.W. Fitness and physical activity in youth with type 1 diabetes mellitus in good or poor glycemic control. Pediatr. Diabetes 2015, 16, 48–57. [Google Scholar] [CrossRef] [PubMed]
- Øverby, N.C.; Margeirsdottir, H.D.; Brunborg, C.; Anderssen, S.A.; Andersen, L.F.; Dahl-Jørgensen, K. Norwegian Study Group for Childhood Diabetes. Physical activity and overweight in children and adolescents using intensified insulin treatment. Pediatr. Diabetes 2009, 10, 135–141. [Google Scholar] [CrossRef]
- Patel, N.J.; Savin, K.L.; Kahanda, S.N.; Malow, B.A.; Williams, L.A.; Lochbihler, G.; Jaser, S.S. Sleep habits in adolescents with type 1 diabetes: Variability in sleep duration linked with glycemic control. Pediatr. Diabetes 2018, 19, 1100–1106. [Google Scholar] [CrossRef]
- Perfect, M.M.; Patel, P.G.; Scott, R.E.; Wheeler, M.D.; Patel, C.; Griffin, K.J.; Sorensen, S.T.; Goodwin, J.L.; Quan, S.F. Sleep, Glucose, and Daytime Functioning in Youth with Type 1 Diabetes. Sleep 2012, 35, 81–88. [Google Scholar] [CrossRef]
- Perfect, M.M. The Relations of Sleep and Quality of Life to School Performance in Youth with Type 1 Diabetes. J. Appl. Sch. Psychol. 2014, 30, 7–28. [Google Scholar] [CrossRef]
- Rebesco, D.B.; Franca, S.N.; Lima, V.A.; Leite, N.; Smouter, L.; Souza, W.C.; Komatsu, W.R.; Mascarenhas, L.P.G. Different Amounts of Moderate to Vigorous Physical Activity and Change in Glycemic Variability in Adolescents with Type 1 Diabetes: Is There Dose-Response Relationship? Arch. Endocrinol. Metab. 2020, 64, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Rechenberg, K.; Griggs, S.; Jeon, S.; Redeker, N.; Yaggi, H.K.; Grey, M. Sleep and Glycemia in Youth with Type 1 Diabetes. J. Pediatr. Health Care 2020, 34, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.J.; Taplin, C.E.; Isom, S.; Divers, J.; Saydah, S.; Jensen, E.T.; Mayer-Davis, E.J.; Reid, L.A.; Liese, A.D.; Dolan, L.M.; et al. Association between fear of hypoglycemia and physical activity in youth with type 1 diabetes: The SEARCH for diabetes in youth study. Pediatr. Diabetes 2020, 21, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Roberts, A.J.; Yi-Frazier, J.P.; Carlin, K.; Taplin, C.E. Hypoglycaemia avoidance behaviour and exercise levels in active youth with type 1 diabetes. Endocrinol. Diabetes Metab. 2020, 3, e00153. [Google Scholar] [CrossRef] [PubMed]
- Roche, D.M.; Edmunds, S.; Cable, T.; Didi, M.; Stratton, G. Skin microvascular reactivity in children and adolescents with type 1 diabetes in relation to levels of physical activity and aerobic fitness. Pediatr. Exerc. Sci. 2008, 20, 426–438. [Google Scholar] [CrossRef] [PubMed]
- Salvatoni, A.; Cardani, R.; Biasoli, R.; Salmaso, M.; De Paoli, A.; Nespoli, L. Physical Activity and Diabetes. Acta Biomed. Atenei Parm. 2005, 76, 85–88. [Google Scholar]
- Särnblad, S.; Ekelund, U.; Åman, J. Physical activity and energy intake in adolescent girls with Type 1 diabetes. Diabet. Med. 2005, 22, 893–899. [Google Scholar] [CrossRef]
- Schiel, R.; Thomas, A.; Kaps, A.; Bieber, G. An Innovative Telemedical Support System to Measure Physical Activity in Children and Adolescents with Type 1 Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2011, 119, 565–568. [Google Scholar] [CrossRef]
- Schweiger, B.; Klingensmith, G.; Snell-Bergeon, J.K. Physical Activity in Adolescent Females with Type 1 Diabetes. Int. J. Pediatr. 2010, 2010, 328318. [Google Scholar] [CrossRef]
- Serrabulho, M.; Matos, M.; Raposo, J. The health and lifestyles of adolescents with type 1 diabetes in Portugal. Eur. Diabetes Nurs. 2015, 9, 12–16a. [Google Scholar] [CrossRef]
- Tercyak, K.P.; Beville, K.W.; Walker, L.R.; Prahlad, S.; Cogen, F.R.; Sobel, D.O.; Streisand, R. Health Attitudes, Beliefs, and Risk Behaviors among Adolescents and Young Adults with Type 1 Diabetes. Child. Health Care 2005, 34, 165–180. [Google Scholar] [CrossRef]
- Turner, S.L.; Queen, T.L.; Butner, J.; Wiebe, D.; Berg, C.A. Variations in Daily Sleep Quality and Type 1 Diabetes Management in Late Adolescents. J. Pediatr. Psychol. 2016, 41, 661–669. [Google Scholar] [CrossRef]
- Valerio, G.; Spagnuolo, M.I.; Lombardi, F.; Spadaro, R.; Siano, M.; Franzese, A. Physical activity and sports participation in children and adolescents with type 1 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 376–382. [Google Scholar] [CrossRef]
- Varni, J.W.; Limbers, C.A.; Bryant, W.P.; Wilson, D.P. The Pedsql Multidimensional Fatigue Scale in Type 1 Diabetes: Feasibility, Reliability, and Validity. Pediatr. Diabetes 2009, 10, 321–328. [Google Scholar] [CrossRef]
- von Schnurbein, J.; Boettcher, C.; Brandt, S.; Karges, B.; Dunstheimer, D.; Galler, A.; Denzer, C.; Denzer, F.; Vollbach, H.; Wabitsch, M.; et al. Sleep and glycemic control in adolescents with type 1 diabetes. Pediatr. Diabetes 2018, 19, 143–149. [Google Scholar] [CrossRef]
- Yeshayahu, Y.; Mahmud, F.H. Altered Sleep Patterns in Adolescents with Type 1 Diabetes: Implications for Insulin Regimen. Diabetes Care 2010, 33, e142. [Google Scholar] [CrossRef]
- Yetim, A.; Alikasifoglu, M.; Bas, F.; Eliacik, K.; Cig, G.; Erginoz, E.; Ercan, O.; Bundak, R. Glycemic Control and Health Be-haviors in Adolescents with Type 1 Diabetes. Turk. J. Pediatr. 2018, 60, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Adler, A.; Gavan, M.Y.; Tauman, R.; Phillip, M.; Shalitin, S. Do Children, Adolescents, and Young Adults with Type 1 Diabetes Have Increased Prevalence of Sleep Disorders? Pediatr. Diabetes 2017, 18, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Bergner, E.M.; Williams, R.; Hamburger, E.R.; Lyttle, M.; Davis, A.C.; Malow, B.; Simmons, J.H.; Lybarger, C.; Capin, R.; Jaser, S.S. Sleep in Teens with Type 1 Diabetes: Perspectives from Adolescents and Their Caregivers. Diabetes Educ. 2018, 44, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Rechenberg, K.; Grey, M.; Sadler, L. “Anxiety and Type 1 diabetes are like cousins”: The experience of anxiety symptoms in youth with Type 1 diabetes. Res. Nurs. Health 2018, 41, 544–554. [Google Scholar] [CrossRef]
- Ryninks, K.; Sutton, E.; Thomas, E.; Jago, R.; Shield, J.P.H.; Burren, C.P. Attitudes to Exercise and Diabetes in Young People with Type 1 Diabetes Mellitus: A Qualitative Analysis. PLoS ONE 2015, 10, e0137562. [Google Scholar] [CrossRef]
- Wennick, A.; Lundqvist, A.; Hallström, I.K. Everyday Experience of Families Three Years after Diagnosis of Type 1 Diabetes in Children: A research paper. J. Pediatr. Nurs. 2009, 24, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Wilkie, L.; Mitchell, F.; Robertson, K.; Kirk, A. Motivations for physical activity in youth with type 1 diabetes participating in the ActivPals project: A qualitative study. Pract. Diabetes 2017, 34, 151–155. [Google Scholar] [CrossRef][Green Version]
- Quirk, H.; Glazebrook, C.; Martin, R.; Blake, H. “We Don’t Worry about Diabetes That Much”: A Qualitative Study Exploring Perceptions of Physical Activity among Children with Type 1 Diabetes. Adv. Pediatr. Res. 2016, 3, 2. [Google Scholar]
- Blake, H.; da Silva, L.; Glazebrook, C. “They Don’t See It as Priority If the Kid’s Not Sporty”: Parents’ Perceptions of Clinic Communication around Physical Activity to Children with Type 1 Diabetes and Their Families. Adv. Pediatr. Res. 2018, 5, 1–14. [Google Scholar] [CrossRef]
- Quirk, H.; Blake, H.; Dee, B.; Glazebrook, C. “You Can’t Just Jump on a Bike and Go”: A Qualitative Study Exploring Parents’ Perceptions of Physical Activity in Children with Type 1 Diabetes. BMC Pediatr. 2014, 14, 313. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A.; Nirantharakumar, K.; Chimen, M.; Pang, T.T.; Hemming, K.; Andrews, R.; Narendran, P. Does Exercise Improve Glycaemic Control in Type 1 Diabetes? A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e58861. [Google Scholar] [CrossRef]
- MacMillan, F.; Kirk, A.; Mutrie, N.; Matthews, L.; Robertson, K.; Saunders, D.H. A Systematic Review of Physical Activity and Sedentary Behavior Intervention Studies in Youth with Type 1 Diabetes: Study Characteristics, Intervention Design, and Efficacy. Pediatr. Diabetes 2014, 15, 175–189. [Google Scholar] [CrossRef]
- Quirk, H.; Blake, H.; Tennyson, R.; Randell, T.L.; Glazebrook, C. Physical activity interventions in children and young people with Type 1 diabetes mellitus: A systematic review with meta-analysis. Diabet. Med. 2014, 31, 1163–1173. [Google Scholar] [CrossRef]
- Absil, H.; Baudet, L.; Robert, A.; Lysy, P.A. Benefits of physical activity in children and adolescents with type 1 diabetes: A systematic review. Diabetes Res. Clin. Pract. 2019, 156, 107810. [Google Scholar] [CrossRef]
- Rassart, J.; Oris, L.; Prikken, S.; Weets, I.; Moons, P.; Luyckx, K. Personality Functioning in Adolescents and Emerging Adults with Type 1 Diabetes. J. Adolesc. Health 2018, 63, 792–798. [Google Scholar] [CrossRef]
- Reutrakul, S.; Thakkinstian, A.; Anothaisintawee, T.; Chontong, S.; Borel, A.-L.; Perfect, M.M.; Janovsky, C.C.P.S.; Kessler, R.; Schultes, B.; Harsch, I.A. Sleep Characteristics in Type 1 Diabetes and Associations with Glycemic Control: Systematic Review and Meta-Analysis. Sleep Med. 2016, 23, 26–45. [Google Scholar] [CrossRef] [PubMed]
- Ji, X.; Wang, Y.; Saylor, J. Sleep and Type 1 Diabetes Mellitus Management among Children, Adolescents, and Emerging Young Adults: A Systematic Review. J. Pediatr. Nurs. 2021, 61, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Elmesmari, R.A.; Reilly, J.J.; Paton, J.Y. 24-Hour Movement Behaviors in Children with Chronic Disease and Their Healthy Peers: A Case-Control Study. Int. J. Environ. Res. Public Health 2022, 19, 2912. [Google Scholar] [CrossRef]
- Tremblay, M.S.; Carson, J.P.V.; Chaput, S.; Gorber, T.C.; Dinh, M.; Duggan, G.; Faulkner, C.E.; Gray, R.; Gruber, K.; Janson, I.; et al. Canadian 24-Hour Movement Guidelines for Children and Youth: An Integration of Physical Activity, Sedentary Behaviour, and Sleep. Appl. Physiol. Nutr. Metab. 2016, 41, S311–S327. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.-P.; Carson, V.; Gray, C.E.; Tremblay, M.S. Importance of All Movement Behaviors in a 24 Hour Period for Overall Health. Int. J. Environ. Res. Public Health 2014, 11, 12575–12581. [Google Scholar] [CrossRef] [PubMed]
- Perfect, M.M. Sleep-related disorders in patients with type 1 diabetes mellitus: Current insights. Nat. Sci. Sleep 2020, 12, 101–123. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| PICOS Statement (Quantitative) | SPIDER Statement (Qualitative) |
|---|---|
| Population: Adolescents (11–18 years) with researcher defined diagnosed type 1 diabetes | Sample: Adolescents (11–18 years) with researcher defined diagnosed type 1 diabetes and primary caregivers/parents of adolescents with researcher defined diagnosed type 1 diabetes |
| Intervention/Exposure: Individual or combined 24-hour movement behaviours | Phenomenon of Interest: At least one 24-hour movement behaviour theme |
| Comparisons: All control/comparison groups | Design: All qualitative methods |
| Outcomes: HbA1c, CGM metrics and QoL | Evaluation: Beliefs, experiences, attitudes, behaviours and interactions etc. |
| Study: Interventional/experimental and observational | Research Type: Qualitative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patience, M.; Janssen, X.; Kirk, A.; McCrory, S.; Russell, E.; Hodgson, W.; Crawford, M. 24-Hour Movement Behaviours (Physical Activity, Sedentary Behaviour and Sleep) Association with Glycaemic Control and Psychosocial Outcomes in Adolescents with Type 1 Diabetes: A Systematic Review of Quantitative and Qualitative Studies. Int. J. Environ. Res. Public Health 2023, 20, 4363. https://doi.org/10.3390/ijerph20054363
Patience M, Janssen X, Kirk A, McCrory S, Russell E, Hodgson W, Crawford M. 24-Hour Movement Behaviours (Physical Activity, Sedentary Behaviour and Sleep) Association with Glycaemic Control and Psychosocial Outcomes in Adolescents with Type 1 Diabetes: A Systematic Review of Quantitative and Qualitative Studies. International Journal of Environmental Research and Public Health. 2023; 20(5):4363. https://doi.org/10.3390/ijerph20054363
Chicago/Turabian StylePatience, Mhairi, Xanne Janssen, Alison Kirk, Stephanie McCrory, Eilidh Russell, William Hodgson, and Megan Crawford. 2023. "24-Hour Movement Behaviours (Physical Activity, Sedentary Behaviour and Sleep) Association with Glycaemic Control and Psychosocial Outcomes in Adolescents with Type 1 Diabetes: A Systematic Review of Quantitative and Qualitative Studies" International Journal of Environmental Research and Public Health 20, no. 5: 4363. https://doi.org/10.3390/ijerph20054363
APA StylePatience, M., Janssen, X., Kirk, A., McCrory, S., Russell, E., Hodgson, W., & Crawford, M. (2023). 24-Hour Movement Behaviours (Physical Activity, Sedentary Behaviour and Sleep) Association with Glycaemic Control and Psychosocial Outcomes in Adolescents with Type 1 Diabetes: A Systematic Review of Quantitative and Qualitative Studies. International Journal of Environmental Research and Public Health, 20(5), 4363. https://doi.org/10.3390/ijerph20054363