
A Climbing (Bouldering) Intervention to Increase the Psychological Well-Being of Adolescents in the Bekaa Valley in Lebanon-Study Protocol for a Controlled Trial

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
2.1. Overall Aims
2.2. Trial Outcomes and Hypothesis
2.2.1. Primary Outcome
2.2.2. Secondary Outcomes
2.2.3. Study Design and Setting
2.3. Eligibility Criteria
- Between the ages of 14 and 19;
- Informed consent for participation in the study from adolescents as well as legal guardians (adult relatives), particularly for data collection, pseudonymized data storage, and analysis;
- Availability and the ability to come to the climbing intervention and to participate in the data collection;
- Living in the area limited by Zahle (N), Deir Zenoun, Marj (S), and Qab Elias/Bouarej (W).
- Physical contraindications (pregnancy or other medical conditions that preclude climbing);
- BMI < 18.5 or >35.
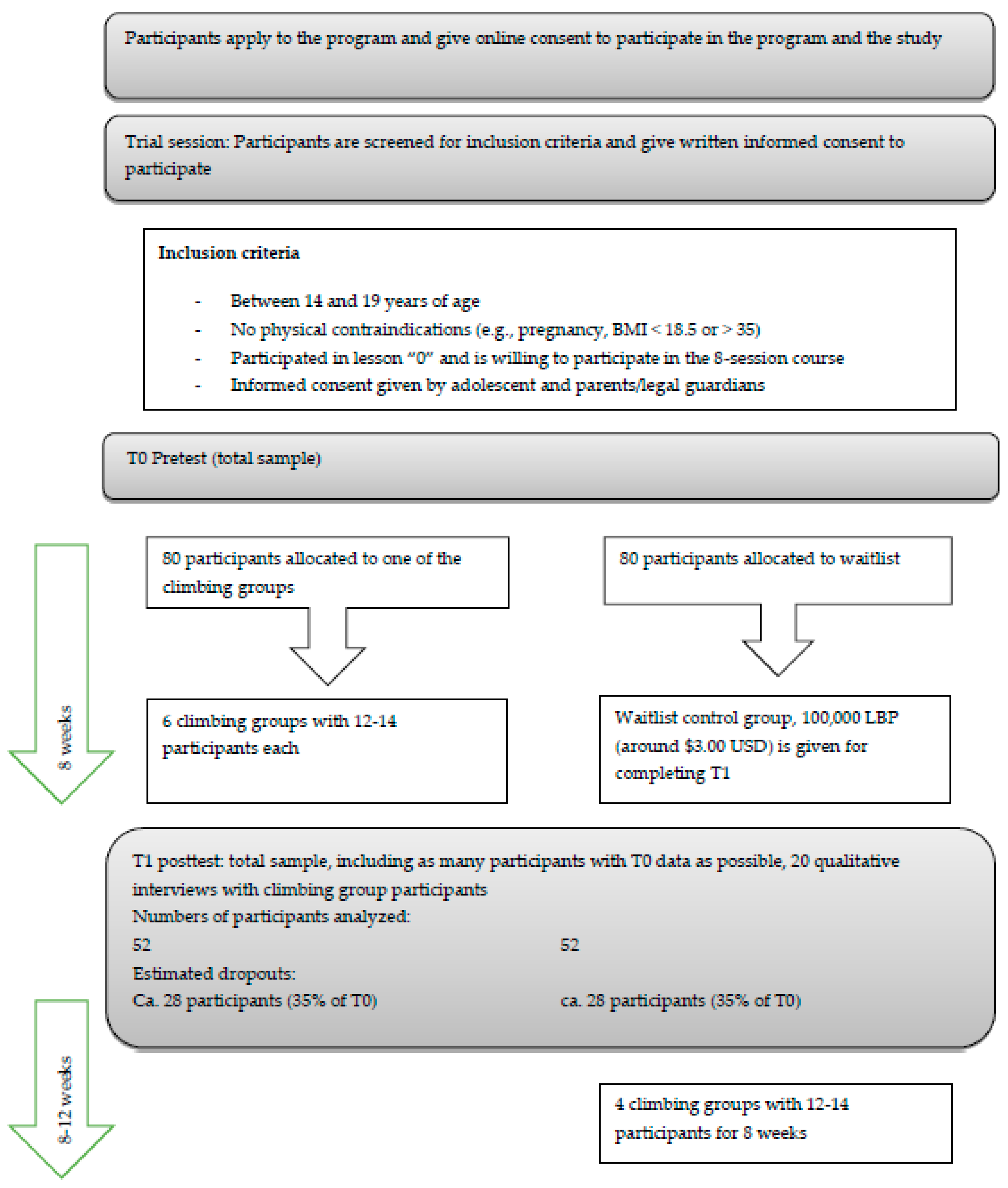
2.4. Screening and Enrollment
2.5. Intervention
2.6. Allocation to the IG and CG
2.7. Sample Size Estimation
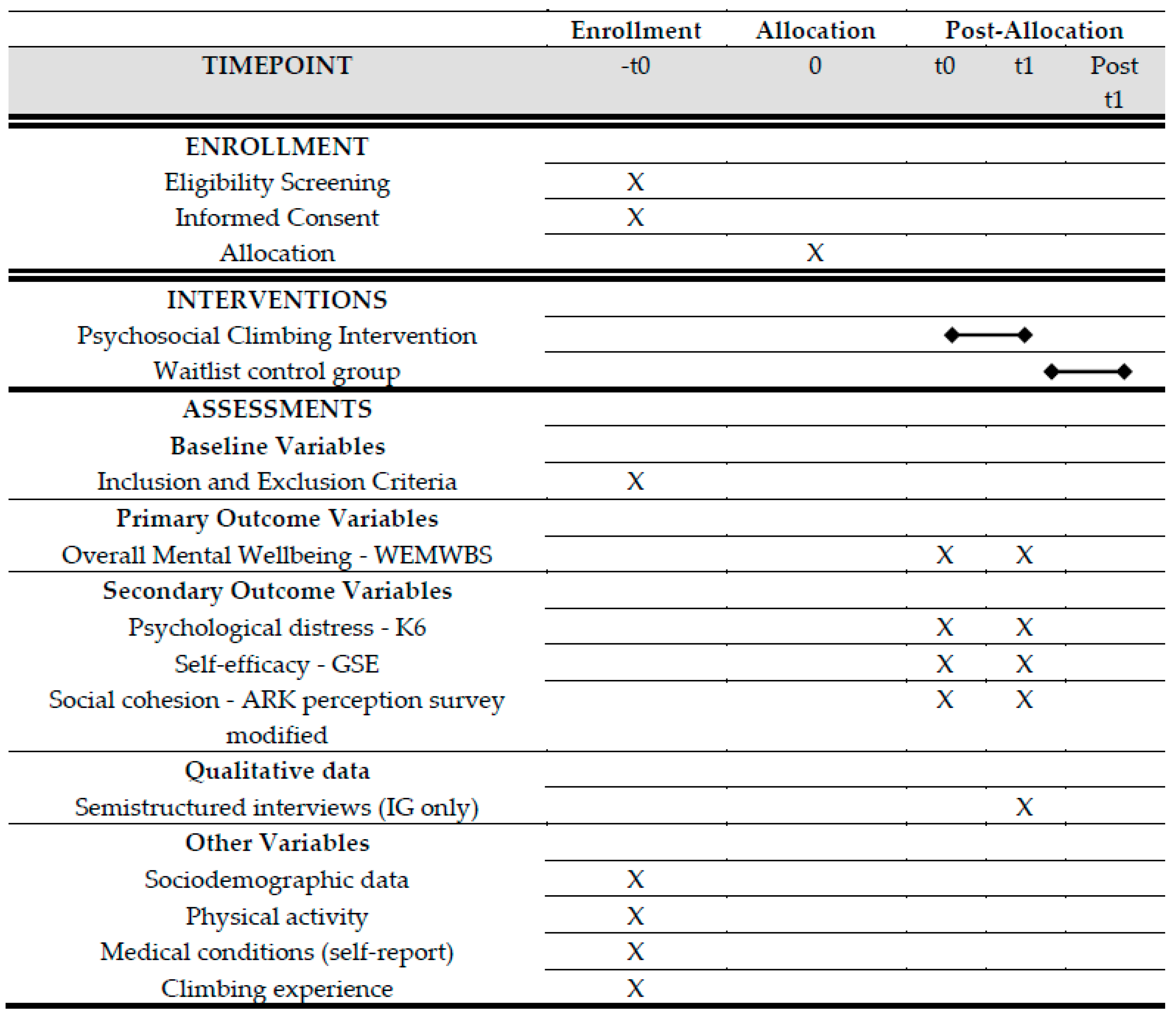
2.8. Data Collection
2.9. Measures
2.9.1. Primary Outcome Measure
2.9.2. Secondary Outcome Measure
- Sociodemographic data: sex, age, school enrollment, nationality, living conditions
- Physical activity
- Medical conditions
- Climbing experience
2.10. Data Quality Management
2.11. Data Analysis
2.11.1. Quantitative Data
2.11.2. Qualitative Data
2.12. Ethical Considerations
- Mild AEs in the IG: all sorts of bruises or scratches or other minor superficial injuries that are transient and do not require treatment;
- Moderate AEs: injuries that are transient but require medical treatment, such as ligament ruptures or sprains, broken bones in legs or arms;
- Severe adverse events (SAEs): severe head injuries, spinal cord injuries, death, suicide attempts.
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abouzeid, M.; Halwani, D.A.; Mokdad, A.H.; Habib, R.R. A Generation at Risk: The Impacts of Lebanon’s Escalating Humanitarian Crisis on Children. Front. Public Health 2021, 9, 704678. [Google Scholar] [CrossRef] [PubMed]
- Fouad, F.M.; Barkil-Oteo, A.; Diab, J.L. Mental health in Lebanon’s Triple-Fold crisis: The case of refugees and vulnerable groups in times of COVID-19. Front. Public Health 2021, 8, 1049. [Google Scholar] [CrossRef] [PubMed]
- United Nations Refugee Agency/ Libanon: Stark Belastetes Aufnahmeland. Available online: https://www.uno-fluechtlingshilfe.de/hilfe-weltweit/libanon/ (accessed on 15 February 2023).
- United Nations Children’ Fund (UNICEF). Lebanon, Children’s Future on the Line. Available online: https://www.unicef.org/lebanon/media/6541/file (accessed on 10 October 2022).
- ARK-UNDP Wave XIV Narrative Report. Available online: https://drive.google.com/file/d/1yADfaDM8_m1F5x5gidPXgAsI511ZPsEH/view (accessed on 27 October 2022).
- Doumit, R.; Kazandjian, C.; Militello, L.K. COPE for Adolescent Syrian Refugees in Lebanon: A Brief Cognitive-Behavioral Skill-Building Intervention to Improve Quality of Life and Promote Positive Mental Health. Clin. Nurs. Res. 2020, 29, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Firth, J.; Siddiqi, N.; Koyanagi, A.; Siskind, D.; Rosenbaum, S.; Galletly, C.; Allan, S.; Caneo, C.; Carney, R.; Carvalho, A.F. The Lancet Psychiatry Commission: A blueprint for protecting physical health in people with mental illness. Lancet Psychiatry 2019, 6, 675–712. [Google Scholar] [CrossRef]
- Thornicroft, G. Physical health disparities and mental illness: The scandal of premature mortality. Br. J. Psychiatry 2011, 199, 441–442. [Google Scholar] [CrossRef]
- Wells, R.; Némorin, S.; Steel, Z.; Guhathakurta, M.; Rosenbaum, S. Physical activity as a psychosocial intervention among Rohingya refugees in Bangladesh: A rapid ecological community assessment. Intervention 2019, 17, 140. [Google Scholar] [CrossRef]
- Think Tank Olympic Refuge, F. Realising the cross-cutting potential of sport in situations of forced displacement. BMJ Glob. Health 2022, 7, e008717. [Google Scholar] [CrossRef]
- Schuch, F.B.; Vancampfort, D.; Richards, J.; Rosenbaum, S.; Ward, P.B.; Stubbs, B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. J. Psychiatr Res. 2016, 77, 42–51. [Google Scholar] [CrossRef]
- Wegner, M.; Amatriain-Fernandez, S.; Kaulitzky, A.; Murillo-Rodriguez, E.; Machado, S.; Budde, H. Systematic Review of Meta-Analyses: Exercise Effects on Depression in Children and Adolescents. Front. Psychiatry 2020, 11, 81. [Google Scholar] [CrossRef]
- Bjorkman, F.; Ekblom, O. Physical Exercise as Treatment for PTSD: A Systematic Review and Meta-Analysis. Mil. Med. 2022, 187, e1103–e1113. [Google Scholar] [CrossRef]
- Ramos-Sanchez, C.P.; Schuch, F.B.; Seedat, S.; Louw, Q.A.; Stubbs, B.; Rosenbaum, S.; Firth, J.; van Winkel, R.; Vancampfort, D. The anxiolytic effects of exercise for people with anxiety and related disorders: An update of the available meta-analytic evidence. Psychiatry Res. 2021, 302, 114046. [Google Scholar] [CrossRef] [PubMed]
- Blanchet, C.; Mathieu, M.È.; St-Laurent, A.; Fecteau, S.; St-Amour, N.; Drapeau, V. A systematic review of physical activity interventions in individuals with binge eating disorders. Curr. Obes. Rep. 2018, 7, 76–88. [Google Scholar] [CrossRef] [PubMed]
- Moola, F.J.; Gairdner, S.E.; Amara, C.E. Exercise in the care of patients with anorexia nervosa: A systematic review of the literature. Ment. Health Phys. Act. 2013, 6, 59–68. [Google Scholar] [CrossRef]
- Wang, D.; Wang, Y.; Wang, Y.; Li, R.; Zhou, C. Impact of physical exercise on substance use disorders: A meta-analysis. PLoS ONE 2014, 9, e110728. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Stubbs, B.; Meyer, J.; Heissel, A.; Zech, P.; Vancampfort, D.; Rosenbaum, S.; Deenik, J.; Firth, J.; Ward, P.B.; et al. Physical activity protects from incident anxiety: A meta-analysis of prospective cohort studies. Depress Anxiety 2019, 36, 846–858. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; Ponce De Leon, A.; Dunn, A.L.; Deslandes, A.C.; et al. Physical Activity and Incident Depression: A Meta-Analysis of Prospective Cohort Studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, A.W.; Stuart, J.; Barber, B.L.; Abkhezr, P. Sport participation may protect socioeconomically disadvantaged youths with refugee backgrounds from experiencing behavioral and emotional difficulties. J. Adolesc. 2020, 85, 148–152. [Google Scholar] [CrossRef]
- Chaput, J.P.; Willumsen, J.; Bull, F.; Chou, R.; Ekelund, U.; Firth, J.; Jago, R.; Ortega, F.B.; Katzmarzyk, P.T. 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5–17 years: Summary of the evidence. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 141. [Google Scholar] [CrossRef]
- Biddle, S.J.; Asare, M. Physical activity and mental health in children and adolescents: A review of reviews. Br. J. Sports Med. 2011, 45, 886–895. [Google Scholar] [CrossRef]
- Ahmed, M.S.; Mahmuda, M.; Alam, A.M.M. Sports and physical activity in psychosocial interventions with adolescent groups of the Rohingya community in Bangladesh: Potential, limitations and critical factors for success. Intervention 2019, 17, 284. [Google Scholar] [CrossRef]
- Wang, K.; Yang, Y.; Zhang, T.; Ouyang, Y.; Liu, B.; Luo, J. The Relationship Between Physical Activity and Emotional Intelligence in College Students: The Mediating Role of Self-Efficacy. Front. Psychol. 2020, 11, 967. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, Y.; Wang, K.; Zhang, T.; Peng, L.; Song, G.; Luo, J. The Influence of Sports Participation on Body Image, Self-Efficacy, and Self-Esteem in College Students. Front. Psychol. 2019, 10, 3039. [Google Scholar] [CrossRef] [PubMed]
- Yip, C.; Sarma, S.; Wilk, P. The association between social cohesion and physical activity in canada: A multilevel analysis. SSM Popul. Health 2016, 2, 718–723. [Google Scholar] [CrossRef] [PubMed]
- Perales, F.; Pozo-Cruz, J.D.; Pozo-Cruz, B.D. Impact of physical activity on psychological distress: A prospective analysis of an Australian national sample. Am. J. Public Health 2014, 104, e91–e97. [Google Scholar] [CrossRef]
- Moon, I.; Frost, A.; Kim, M. The role of physical activity on psychological distress and health-related quality of life for people with comorbid mental illness and health conditions. Soc. Work. Ment. Health 2020, 18, 410–428. [Google Scholar] [CrossRef]
- Rosenbaum, S.; Ager, A.; Snider, L.; Warria, A.; Collison, H.; Hermosilla, S.; Vancampfort, D. Physical activity, mental health and psychosocial support. Forced. Migr. Rev. 2021, 66, 34–37. [Google Scholar]
- Momartin, S.; Coello, M.; Pittaway, E.; Downham, R.; Aroche, J. Capoeira Angola: An alternative intervention program for traumatized adolescent refugees from war-torn countries. Torture 2019, 29, 85. [Google Scholar]
- Marshall, J.; Kamuskay, S.; Samai, M.M.; Marah, I.; Tonkara, F.; Conteh, J.; Keita, S.; Jalloh, O.; Missalie, M.; Bangura, M. A Mixed Methods Exploration of Surf Therapy Piloted for Youth Well-Being in Post-Conflict Sierra Leone. Int. J. Environ. Res. Public Health 2021, 18, 6267. [Google Scholar] [CrossRef]
- Tuakli-Wosornu, Y.A.; Rowan, M.; Gittelsohn, J. Perceptions of physical activity, activity preferences and health among a group of adult women in urban Ghana: A pilot study. Ghana Med. J. 2014, 48, 3–13. [Google Scholar] [CrossRef]
- Belza, B.; Walwick, J.; Shiu-Thornton, S.; Schwartz, S.; Taylor, M.; LoGerfo, J. Older adult perspectives on physical activity and exercise: Voices from multiple cultures. Prev. Chronic. Dis. 2004, 1, A09. [Google Scholar]
- Henderson, K.A.; Ainsworth, B.E. A synthesis of perceptions about physical activity among older African American and American Indian women. Am. J. Public Health 2003, 93, 313–317. [Google Scholar] [CrossRef] [PubMed]
- D’Alonzo, K.T.; Fischetti, N. Cultural beliefs and attitudes of Black and Hispanic college-age women toward exercise. J. Transcult. Nurs. 2008, 19, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Horn, R.; Ewart-Biggs, R.; Hudson, F.; Berilgen, S.; Ironside, J.; Prodromou, A. The role of a trauma-sensitive football group in the recovery of survivors of torture. Torture 2019, 29, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Ley, C.; Rato Barrio, M.; Koch, A. “In the Sport I Am Here”: Therapeutic Processes and Health Effects of Sport and Exercise on PTSD. Qual. Health Res. 2018, 28, 491–507. [Google Scholar] [CrossRef] [PubMed]
- Reed, R.V.; Fazel, M.; Jones, L.; Panter-Brick, C.; Stein, A. Mental health of displaced and refugee children resettled in low-income and middle-income countries: Risk and protective factors. Lancet 2012, 379, 250–265. [Google Scholar] [CrossRef]
- Rosso, E.; McGrath, R. Promoting physical activity among children and youth in disadvantaged South Australian CALD communities through alternative community sport opportunities. Health Promot. J. Austr. 2016, 27, 105–110. [Google Scholar] [CrossRef]
- Luttenberger, K.; Karg-Hefner, N.; Berking, M.; Kind, L.; Weiss, M.; Kornhuber, J.; Dorscht, L. Bouldering psychotherapy is not inferior to cognitive behavioural therapy in the group treatment of depression: A randomized controlled trial. Br. J. Clin. Psychol. 2021, 61, 465–493. [Google Scholar] [CrossRef] [PubMed]
- Stelzer, E.-M.; Book, S.; Graessel, E.; Hofner, B.; Kornhuber, J.; Luttenberger, K. Bouldering psychotherapy reduces depressive symptoms even when general physical activity is controlled for: A randomized controlled trial. Heliyon 2018, 4, e00580. [Google Scholar] [CrossRef]
- Gassner, L.; Dabnichki, P.; Langer, A.; Pokan, R.; Zach, H.; Ludwig, M.; Santer, A. The Therapeutic Effects of Climbing: A Systematic Review and Meta-Analysis. PM R 2022. online ahead of print. [Google Scholar] [CrossRef]
- Kratzer, A.; Luttenberger, K.; Karg-Hefner, N.; Weiss, M.; Dorscht, L. Bouldering psychotherapy is effective in enhancing perceived self-efficacy in people with depression: Results from a multicenter randomized controlled trial. BMC Psychol. 2021, 9, 126. [Google Scholar] [CrossRef]
- Maheswaran, H.; Weich, S.; Powell, J.; Stewart-Brown, S. Evaluating the responsiveness of the Warwick Edinburgh Mental Well-Being Scale (WEMWBS): Group and individual level analysis. Health Qual. Life Outcomes 2012, 10, 156. [Google Scholar] [CrossRef]
- Mayring, P.; Gläser-Zikuda, M. Die Praxis der Qualitativen Inhaltsanalyse, 2nd ed.; Beltz: Weinheim, Germany, 2008. [Google Scholar]
- Schulz von Thun, F. Miteinander Reden 1. Störungen und Klärungen: Allgemeine Psychologie der Kommunikation, 48th ed.; Rowohlt Taschenbuch: Hamburg, Germany, 2010. [Google Scholar]
- Rosenberg, M. Nonviolent Communication: A Language of Life, 3rd ed.; PuddleDancer Press: Encinitas, CA, USA, 2015. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Easton, S.D.; Safadi, N.S.; Wang, Y.; Hasson, R.G., 3rd. The Kessler psychological distress scale: Translation and validation of an Arabic version. Health Qual. Life Outcomes 2017, 15, 215. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.J.; Sung, H.Y.; Max, W.; Shi, Y.; Ong, M. Validity study of the K6 scale as a measure of moderate mental distress based on mental health treatment need and utilization. Int. J. Methods Psychiatr. Res. 2012, 21, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Crandall, A.; Rahim, H.; Yount, K. Validation of the general self-efficacy scale among Qatari young women. East Mediterr. Health J. 2015, 21, 891–896. [Google Scholar] [CrossRef] [PubMed]
- Romppel, M.; Herrmann-Lingen, C.; Wachter, R.; Edelmann, F.; Dungen, H.D.; Pieske, B.; Grande, G. A short form of the General Self-Efficacy Scale (GSE-6): Development, psychometric properties and validity in an intercultural non-clinical sample and a sample of patients at risk for heart failure. Psychosoc. Med. 2013, 10, Doc01. [Google Scholar] [CrossRef]
- Holtrop, J.S.; Rabin, B.A.; Glasgow, R.E. Qualitative approaches to use of the RE-AIM framework: Rationale and methods. BMC Health Serv. Res. 2018, 18, 177. [Google Scholar] [CrossRef]
- Ali, M.W.; Siddiqui, O. Multiple imputation compared with some informative dropout procedures in the estimation and comparison of rates of change in longitudinal clinical trials with dropouts. J. Biopharm. Stat. 2000, 10, 165–181. [Google Scholar] [CrossRef]
- Mayring, P. Qualitative Inhaltsanalyse. In Handbuch Qualitative Forschung in der Psychologie; Mey, G., Mruck, K., Eds.; VVS Verlag für Sozialwissenschaften Wiesbaden: Wiesbaden, Germany, 2010; pp. 601–613. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Mansour, Z.; Said, R.; Dbaibo, H.; Mrad, P.; Torossian, L.; Rady, A.; Dufouil, C. Non-communicable diseases in Lebanon: Results from World Health Organization STEPS survey 2017. Public. Health 2020, 187, 120–126. [Google Scholar] [CrossRef]
- Maalouf, F.T.; Alrojolah, L.; Akoury-Dirani, L.; Barakat, M.; Brent, D.; Elbejjani, M.; Shamseddeen, W.; Ghandour, L.A. Psychopathology in Children and Adolescents in Lebanon Study (PALS): A national household survey. Soc. Psychiatry Psychiatr. Epidemiol. 2022, 57, 761–774. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Data Category | Information |
|---|---|
| ISRCTN13005983 |
| 29 March 2022 |
| - |
| Mammut Sports Group |
| Universitätsklinikum Erlangen, Germany |
| Antonine University, Hadat Baabda, Lebanon |
| see Point 8 |
| PD Dr. Katharina Luttenberger, katharina.luttenberger@uk-erlangen.de |
| Effectiveness of a climbing (bouldering) intervention on psychological wellbeing for adolescents in the Bekaa Valley, Lebanon: (How) does it work? |
| Mixed method study on a climbing (bouldering) intervention to increase the psychological well-being of adolescents in the Bekaa Valley in Lebanon, waitlist-controlled trial. |
| Lebanon |
| Psychological wellbeing of adolescent in Bekaa, Lebanon, refugees and host community |
| Study arm 1: Intervention group receiving the psychosocial bouldering intervention |
| Study arm 2: waitlist control group receiving the intervention after posttest. | |
| Ages eligible for study: adults; Sexes eligible for study: both |
| Inclusion criteria: 1. Aged between 14 and 19 years 2. Written informed consent of parents or young adult 3. Ability to reach the climbing intervention | |
| Exclusion criteria: 1. physical contradictions to climbing | |
| Controlled intervention study |
| April 2022 |
| 160 |
| complete |
| Overall mental wellbeing is measured with the WEMWBS (Warwick-Edinburgh Mental Well-Being Scale) at baseline and after the intervention (8 weeks) |
| Distress severity, general self-efficacy, social cohesion |
| Session | Module Themes | Cross-Cutting Themes |
|---|---|---|
| 1 | Trust & respect | Shared leadership Emotional education Mindfulness |
| 2 | ||
| 3 | Cooperation & teamwork | |
| 4 | ||
| 5 | Communication & conflict resolution | |
| 6 | ||
| 7 | Problem-solving & decision-making | |
| 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luttenberger, K.; Najem, C.; Rosenbaum, S.; Sifri, C.; Kind, L.; Baggenstos, B. A Climbing (Bouldering) Intervention to Increase the Psychological Well-Being of Adolescents in the Bekaa Valley in Lebanon-Study Protocol for a Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 4289. https://doi.org/10.3390/ijerph20054289
Luttenberger K, Najem C, Rosenbaum S, Sifri C, Kind L, Baggenstos B. A Climbing (Bouldering) Intervention to Increase the Psychological Well-Being of Adolescents in the Bekaa Valley in Lebanon-Study Protocol for a Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(5):4289. https://doi.org/10.3390/ijerph20054289
Chicago/Turabian StyleLuttenberger, Katharina, Charbel Najem, Simon Rosenbaum, Charles Sifri, Leona Kind, and Beat Baggenstos. 2023. "A Climbing (Bouldering) Intervention to Increase the Psychological Well-Being of Adolescents in the Bekaa Valley in Lebanon-Study Protocol for a Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 5: 4289. https://doi.org/10.3390/ijerph20054289
APA StyleLuttenberger, K., Najem, C., Rosenbaum, S., Sifri, C., Kind, L., & Baggenstos, B. (2023). A Climbing (Bouldering) Intervention to Increase the Psychological Well-Being of Adolescents in the Bekaa Valley in Lebanon-Study Protocol for a Controlled Trial. International Journal of Environmental Research and Public Health, 20(5), 4289. https://doi.org/10.3390/ijerph20054289