


Caring for Those Who Take Care of Others: Developing Systemic and Sustainable Mental Health Support for the Diverse Healthcare Workforce in the United Kingdom

 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Discussion
3. Conclusions
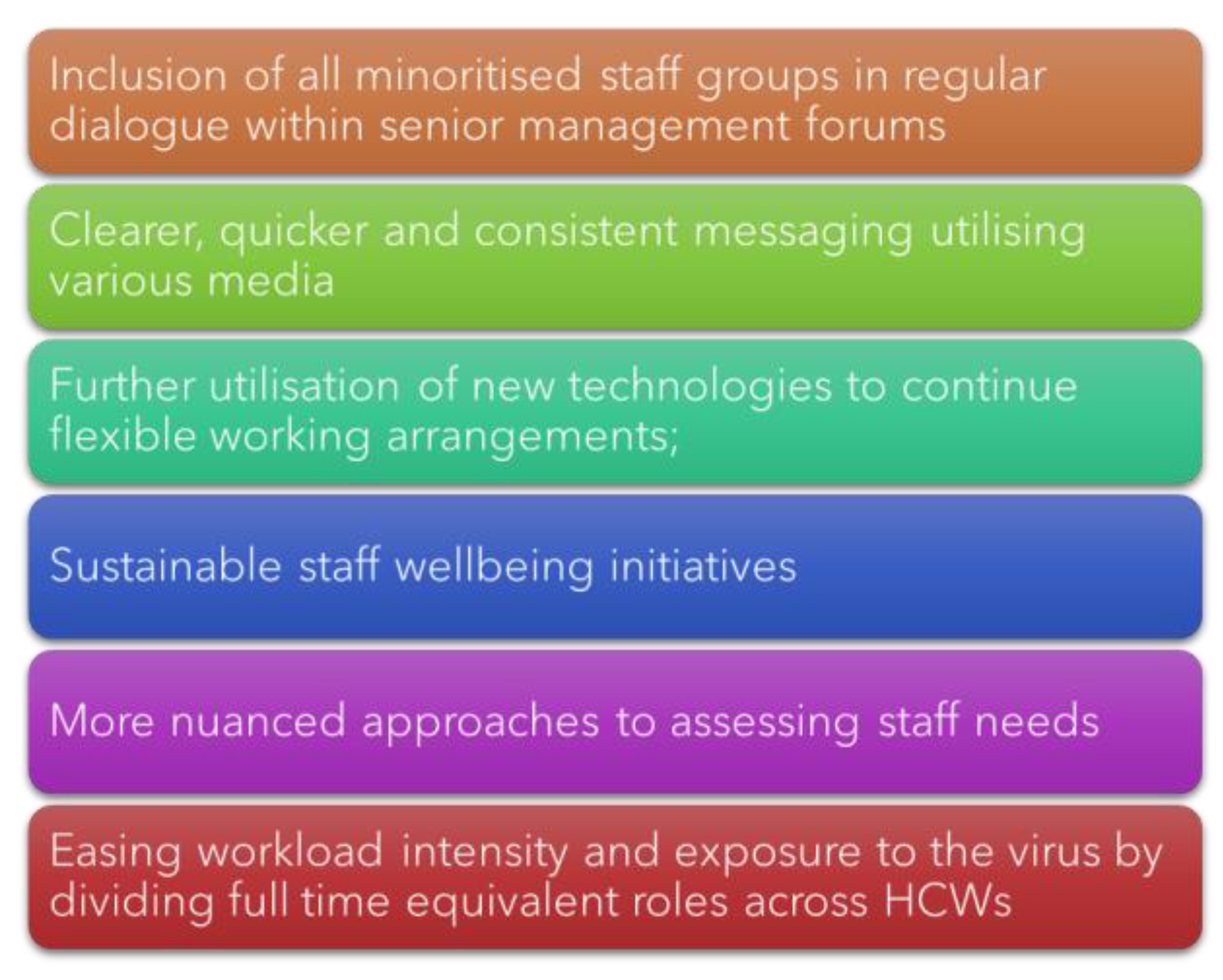
- Inclusion of all minoritised and underserved staff groups in key decision-making policies and dialogues at all levels within the policy eco-system.
- Increase government-led research and funding targeted at improving the communication channels and dissemination of information related to policy and guideline changes to HCWs during pandemics and other dynamic national emergencies to reduce the burden of stress and anxiety associated with poor and confusing communications.
- Continue to invest in new technologies to help enable HCWs more flexible working arrangements to facilitate and improve the mental wellbeing of staff with families and encourage the regular taking of paid breaks.
- Ensure that all NHS staff have equal and equitable access to free, flexible, and high-quality mental health services regardless of their speciality, geographical area, and/or shift time. Simultaneously also equip leaders and line-managers to support staff with wellbeing and mental health needs through trainings and resource dissemination.
- Nuanced approaches to assessing staff needs taking into consideration their intersecting social identities and positions (e.g., a female nurse who is also a single mother) are needed to tailor effective mental health interventions and initiatives.
- Maximise investments into a sustainable recruitment campaign to improve and ease workload intensities across all departments to improve the health system’s resilience and response during a future pandemic, combined with reduced post-pandemic financial costs associated with backlogged and delayed elective surgeries.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
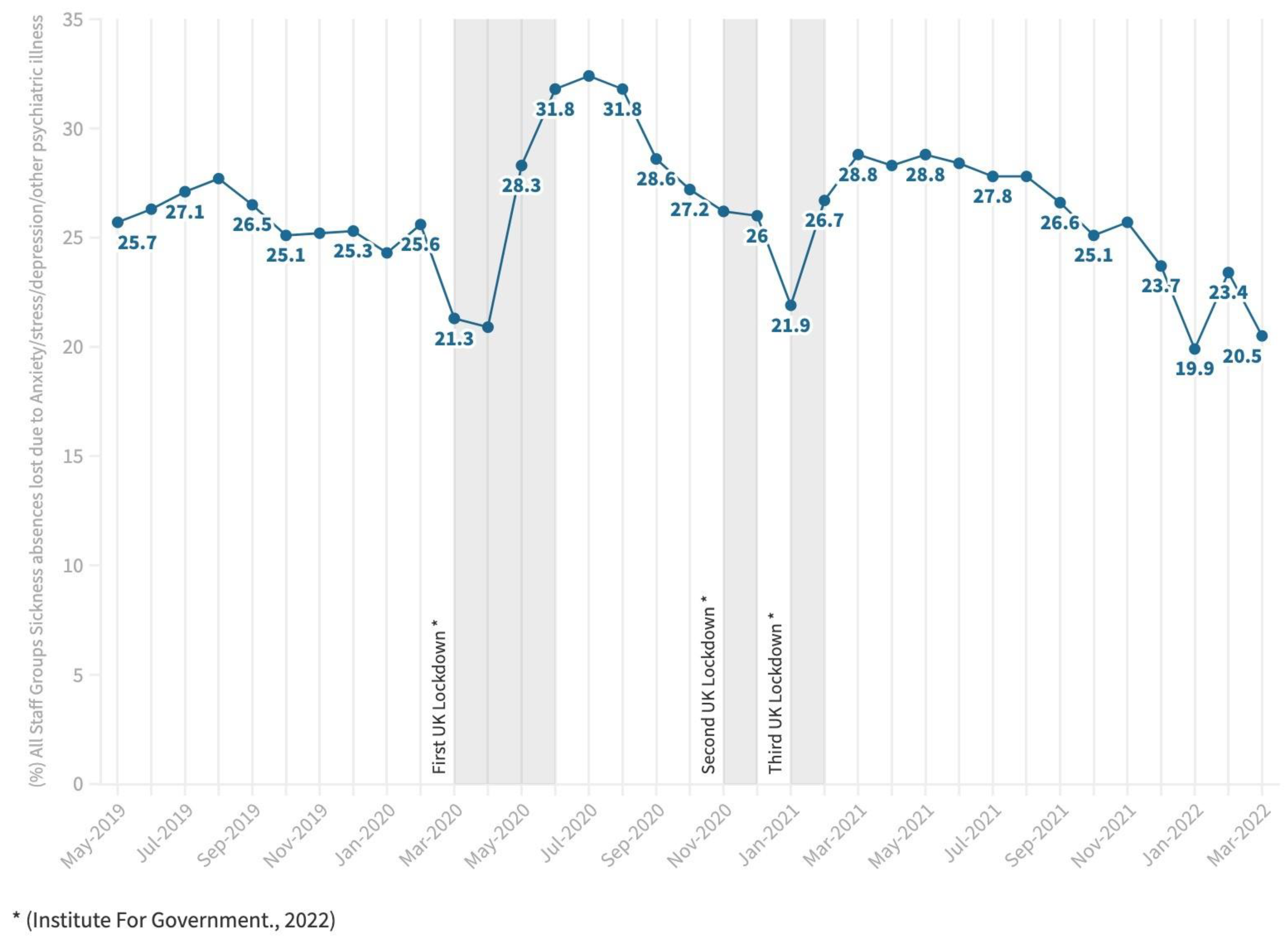
- NHS Digital. NHS Sickness Absence Rates, January 2022 to March 2022, and Annual Summary 2009 to 2022, January 2022. 2023; pp. 1–16. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/nhs-sickness-absence-rates/nhs-sickness-absence-rates-january-2022-to-march-2022-and-annual-summary-2009-to-2020-provisional-statistics# (accessed on 17 October 2022).
- Evans, N. Commons health committee cites workload and “not feeling valued” for high vacancy rates in nursing. Nurs. Manag. 2018, 24, 8–9. [Google Scholar] [CrossRef]
- Lamb, D.; Gnanapragasam, S.; Greenberg, N.; Bhundia, R.; Carr, E.; Hotopf, M.; Razavi, R.; Raine, R.; Cross, S.; Dewar, A.; et al. Psychosocial Impact of the COVID-19 Pandemic on 4378 UK Healthcare Workers and Ancillary Staff: Initial Baseline Data from a Cohort Study Collected during the First Wave of the Pandemic. medRvix 2021. [Google Scholar] [CrossRef] [PubMed]
- Troglio da Silva, F.C.; Neto, M.L.R. Psychiatric disorders in health professionals during the COVID-19 pandemic: A systematic review with meta-analysis. J. Psychiatr. Res. 2021, 140, 474–487. [Google Scholar] [CrossRef] [PubMed]
- Awan, S.; Dowan, M.N.; Aamir, A.; Allahuddin, Z.; Irfan, M.; Carano, A.; Vellante, F.; Ventriglio, A.; Fornaro, M.; Valchera, A.; et al. Suicide in Healthcare Workers: Determinants, Challenges, and the Impact of COVID-19. Front. Psychiatry 2022, 12, 792925. [Google Scholar] [CrossRef] [PubMed]
- IFG. Timeline of UK Government Coronavirus Lockdowns and Measures, March 2020 to December 2021. 2021. Available online: https://www.instituteforgovernment.org.uk/data-visualisation/timeline-coronavirus-lockdowns (accessed on 10 October 2022).
- Scott, H.R.; Stevelink, S.A.M.; Gafoor, R.; Lamb, D.; Carr, E.; Bakolis, I.; Bhundia, R.; Docherty, M.J.; Dorrington, S.; Gnanapragasam, S.; et al. Prevalence of post-traumatic stress disorder and common mental disorders in health-care workers in England during the COVID-19 pandemic: A two-phase cross-sectional study. Lancet Psychiatry 2023, 10, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Joseph, B.; Joseph, M. The health of the healthcare workers. Indian J. Occup. Environ. Med. 2016, 20, 71–72. [Google Scholar] [CrossRef] [PubMed]
- Pollitt, A.; Pow, R. Supporting the Mental Health of NHS Staff as Part of Post-Pandemic Recovery. 2022. Available online: www.nhscheck.org (accessed on 25 January 2023).
- Allan, H.T.; Larsen, J.A.; Bryan, K.; Smith, P.A. The social reproduction of institutional racism: Internationally recruited nurses’ experiences of the British health services. Divers. Health Soc. Care 2004, 1, 117–125. [Google Scholar]
- Brathwaite, B. Black, Asian and minority ethnic female nurses: Colonialism, power and racism. Br. J. Nurs. 2018, 27, 254–258. [Google Scholar] [CrossRef]
- Kline, R.; Naqvi, H.; Razaq, S.A.; Wilhelm, R. NHS Workforce Race Equality Standard 2016 Data Analysis Report for NHS Trusts; NHS: London, UK, 2017. [Google Scholar]
- Takeuchi, D.; Dearing, T.; Bartholomew, M.; McRoy, R. Equality and Equity: Expanding Opportunities to Remedy Disadvantage. J. Am. Soc. Aging 2018, 42, 13–19. [Google Scholar]
- UK Government. Build Back Better: Our Plan for Health and Social Care. 2022. Available online: https://www.gov.uk/government/publications/build-back-better-our-plan-for-health-and-social-care/build-back-better-our-plan-for-health-and-social-care (accessed on 10 October 2022).
- NHS. NHS Staff Survey Results. 2019. Available online: https://www.nhsstaffsurveys.com/results/ (accessed on 10 October 2022).
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 19, 1967–1978. [Google Scholar] [CrossRef]
- West, M.; Coia, D.D. Caring for Doctors Caring for Patients. 2019. Available online: www.gmc-uk.org (accessed on 17 October 2022).
- Patel, R.S.; Bachu, R.; Adikey, A.; Malik, M.; Shah, M. Factors related to physician burnout and its consequences: A review. Behav. Sci. 2018, 8, 98. [Google Scholar] [CrossRef] [PubMed]
- Çölkesen, F. The Effects of COVID-19 Pandemic on the Mental Health of Healthcare Workers and Recommendations for the Prevention of Loss of Work Efficiency. Erciyes Med. J. 2021, 43, 560–565. [Google Scholar] [CrossRef]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare staff wellbeing, burnout, and patient safety: A systematic review. PLoS ONE 2016, 11, 1–12. [Google Scholar] [CrossRef]
- UK Government. COVID-19 Response: Living with COVID. 2022. Available online: https://www.gov.uk/government/publications/covid-19-response-living-with-covid-19/covid-19-response-living-with-covid-19 (accessed on 10 October 2022).
- Qureshi, I.; Gogoi, M.; Al-Oraibi, A.; Wobi, F.; Chaloner, J.; Gray, L.; Guyatt, A.L.; Hassan, O.; Nellums, L.B.; Pareek, M.; et al. Mental Health During COVID-19: A Qualitative Study With Ethnically Diverse Healthcare Workers in the United Kingdom. Eur. J. Psychotraumatol. 2022, 13, 2105577. [Google Scholar] [CrossRef]
- Ford, M. BME Nurses Feel Targeted to Work on COVID-19 Wards. Nursing Times. 2020. Available online: https://www.nursingtimes.net/news/coronavirus/exclusive-bme-nurses-feel-targeted-to-work-on-covid-19-wards-17-04-2020/ (accessed on 10 October 2022).
- Qureshi, I.; Gogoi, M.; Wobi, F.; Chaloner, J.; Al-Oraibi, A.; Hassan, O.; Pan, D.; Nellums, L.B.; Pareek, M. Healthcare Workers From Diverse Ethnicities and Their Perceptions of Risk and Experiences of Risk Management During the COVID-19 Pandemic: Qualitative Insights From the United Kingdom-REACH Study. Front. Med. 2022, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- UK Government. The Government Response to the Health and Social Care Committee Report on Workforce Burnout and Resilience in the NHS and Social Care. 2022. Available online: https://www.gov.uk/government/publications/workforce-burnout-and-resilience-in-the-nhs-and-social-care/the-government-response-to-the-health-and-social-care-committee-report-on-workforce-burnout-and-resilience-in-the-nhs-and-social-care (accessed on 25 January 2023).
- UK Government. The National Resilience Strategy A Call for Evidence. 2021. Available online: http://www.nationalarchives.gov.uk/doc/open-government-licence/ (accessed on 10 October 2022).
- UK Government. BAME Communities Advisory Group Report and Recommendations. 2020. Available online: https://www.gov.uk/government/publications/social-care-sector-covid-19-support-taskforce-report-on-first-phase-of-covid-19-pandemic/bame-communities-advisory-group-report-and-recommendations#part-1-report-and-recommendations (accessed on 17 October 2022).
- Ashe, S.D. SHF Race Report; 40 Years of Tackling Racial Inequality in Britain. 2021. Available online: https://www.stuarthallfoundation.org/projects/shf-race-report/ (accessed on 17 October 2022).
- Hwang, J.H.; Jung, H.S. The effects of work characteristics related to work–life imbalance on presenteeism among female workers in the health and social work sectors: Mediation analysis of psychological and physical health problems. Int. J. Environ. Res. Public Health 2021, 18, 6218. [Google Scholar] [CrossRef] [PubMed]
- MHF. Wave 13 Summary: 9 to 15 November 2021. Mental Health Foundation. Coronavirus: Mental Health in the Pandemic Study. 2021. Available online: https://www.mentalhealth.org.uk/our-work/research/coronavirus-mental-health-pandemic-study/wave-13-summary (accessed on 10 October 2022).

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qureshi, I.; Chaloner, J.; Gogoi, M.; Al-Oraibi, A.; Wobi, F.; Reilly, H.; Medisauskaite, A.; Martin, C.A.; Irizar, P.; Papineni, P.; et al. Caring for Those Who Take Care of Others: Developing Systemic and Sustainable Mental Health Support for the Diverse Healthcare Workforce in the United Kingdom. Int. J. Environ. Res. Public Health 2023, 20, 3242. https://doi.org/10.3390/ijerph20043242
Qureshi I, Chaloner J, Gogoi M, Al-Oraibi A, Wobi F, Reilly H, Medisauskaite A, Martin CA, Irizar P, Papineni P, et al. Caring for Those Who Take Care of Others: Developing Systemic and Sustainable Mental Health Support for the Diverse Healthcare Workforce in the United Kingdom. International Journal of Environmental Research and Public Health. 2023; 20(4):3242. https://doi.org/10.3390/ijerph20043242
Chicago/Turabian StyleQureshi, Irtiza, Jonathan Chaloner, Mayuri Gogoi, Amani Al-Oraibi, Fatimah Wobi, Holly Reilly, Asta Medisauskaite, Christopher A. Martin, Patricia Irizar, Padmasayee Papineni, and et al. 2023. "Caring for Those Who Take Care of Others: Developing Systemic and Sustainable Mental Health Support for the Diverse Healthcare Workforce in the United Kingdom" International Journal of Environmental Research and Public Health 20, no. 4: 3242. https://doi.org/10.3390/ijerph20043242
APA StyleQureshi, I., Chaloner, J., Gogoi, M., Al-Oraibi, A., Wobi, F., Reilly, H., Medisauskaite, A., Martin, C. A., Irizar, P., Papineni, P., Lagrata, S., Agbonmwandolor, J., Pareek, M., & Nellums, L. (2023). Caring for Those Who Take Care of Others: Developing Systemic and Sustainable Mental Health Support for the Diverse Healthcare Workforce in the United Kingdom. International Journal of Environmental Research and Public Health, 20(4), 3242. https://doi.org/10.3390/ijerph20043242