
Social Support, Identity Affirmation, and Psychological Well-Being: A Developmental and Intersectional Comparison between Italian Cisgender and Non-Binary People with Bisexual Orientation

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
1.1. Minority Stress and Health in Bisexual People
1.2. Integrating Positive Psychology, Intersectionality, and Life Course Perspective into the Minority Stress Framework
1.2.1. Positive Psychology
1.2.2. Intersectionality
1.2.3. Life Course
1.3. The Current Study
2. Materials and Methods
2.1. Procedures
2.2. Participants
2.3. Measures
2.3.1. Sociodemographic Characteristics
2.3.2. Perceived Social Support
2.3.3. Identity Affirmation
2.3.4. Psychological Well-Being
2.4. Statistical Analyses
3. Results
3.1. Descriptive Statistics and Partial Correlations
3.2. Associations of Perceived Social Support, Identity Affirmation, and Psychological Well-Being with Gender Identity and Age Groups
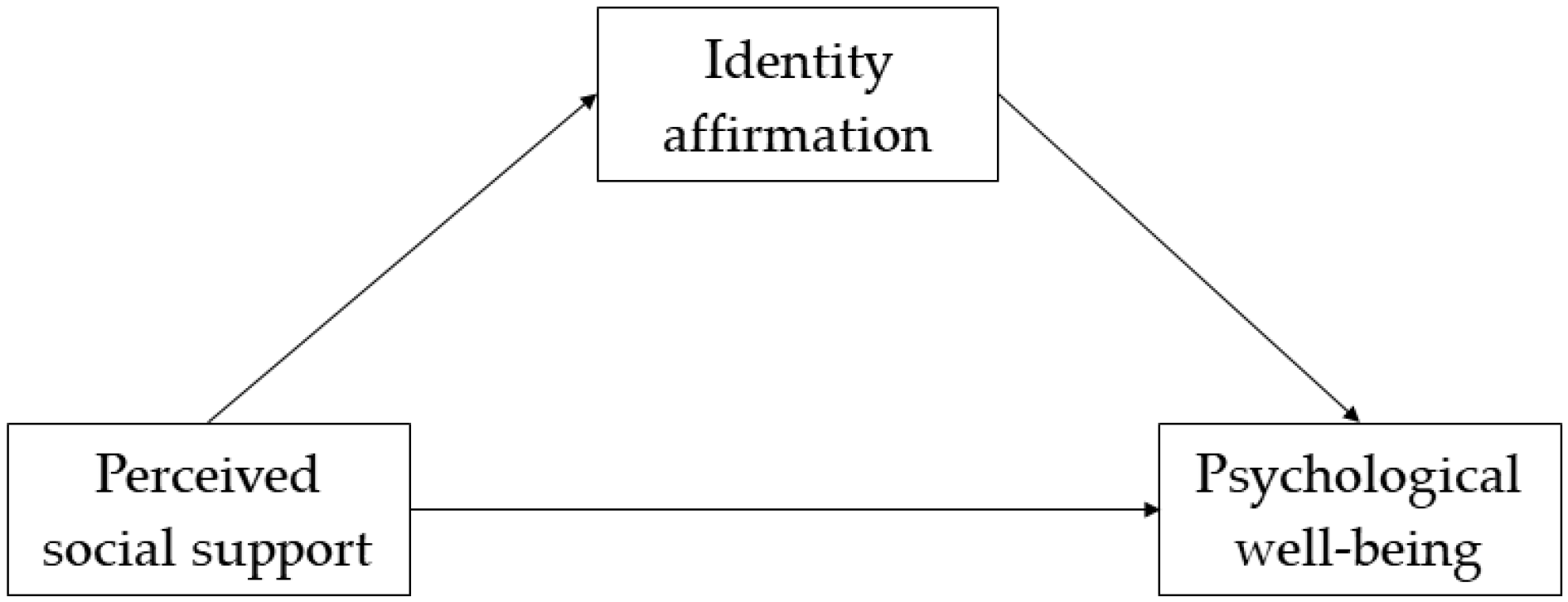
3.3. Multiple-Group Mediation Models
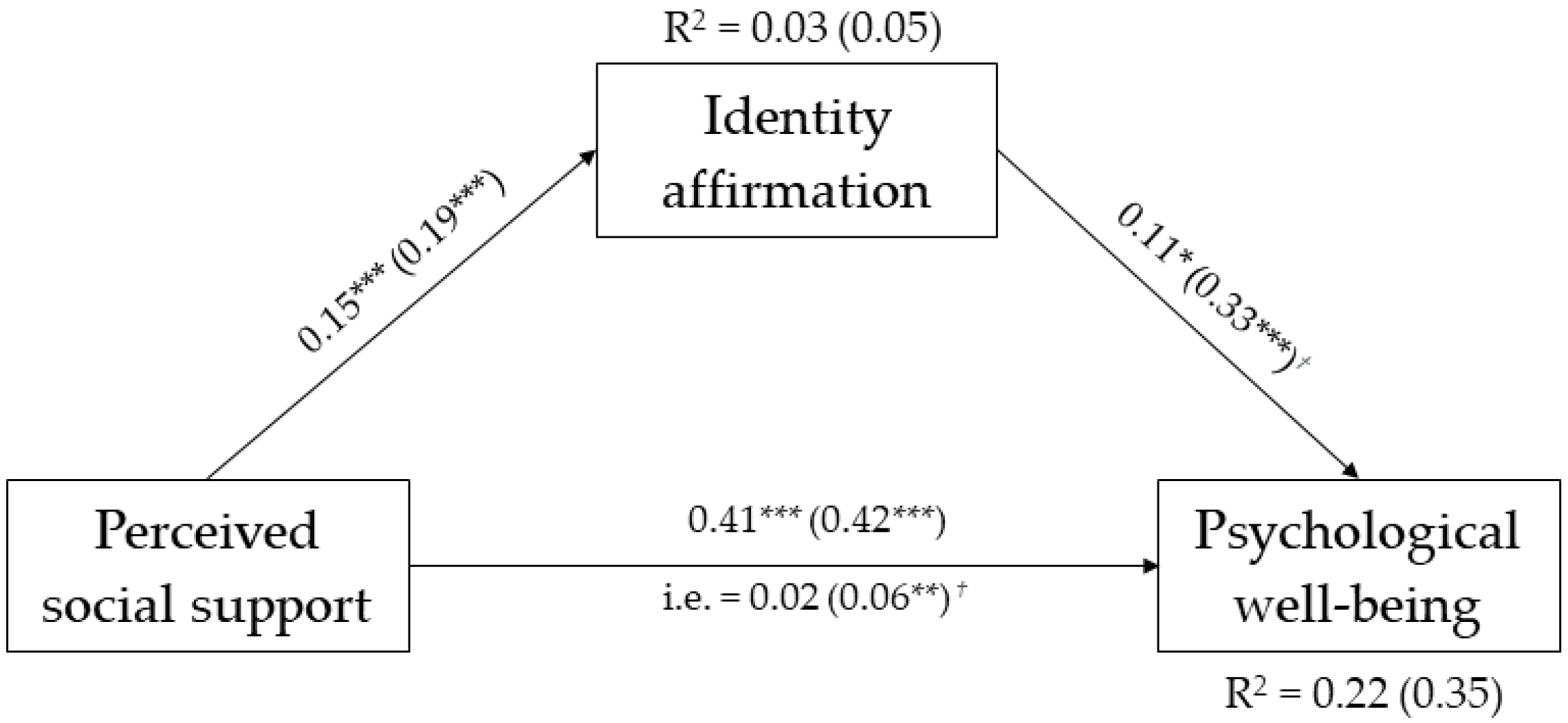
3.3.1. Gender Identity as Grouping Variable
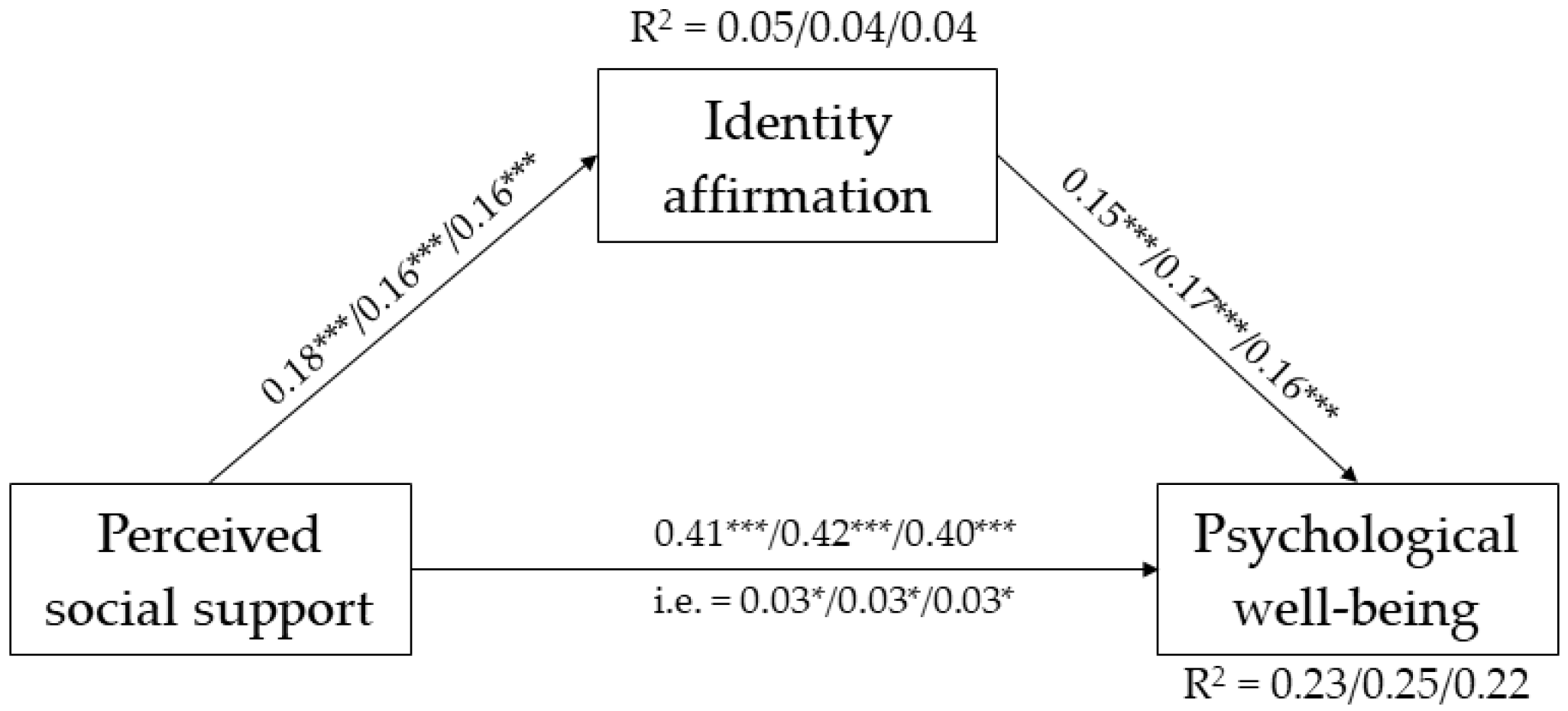
3.3.2. Age Groups as Grouping Variable
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Flanders, C.E.; Tarasoff, L.A.; Legge, M.M.; Robinson, M.; Gos, G. Positive identity experiences of young bisexual and other nonmonosexual people: A qualitative inquiry. J. Homosex. 2017, 64, 1014–1032. [Google Scholar] [CrossRef] [PubMed]
- LGBT + Pride 2021 Global Survey. Available online: https://www.ipsos.com/en/lgbt-pride-2021-global-survey-points-generation-gap-around-gender-identity-and-sexual-attraction (accessed on 9 February 2022).
- National Institute of Statistic. La Popolazione Omosessuale Nella Società Italiana. [Homosexual Population in Italian Society]. 2011. Available online: https://www.istat.it/it/files//2012/05/report-omofobia_6giugno.pdf (accessed on 5 January 2022).
- Feinstein, B.A.; Dyar, C. Bisexuality, minority stress, and health. Curr. Sex. Health Rep. 2017, 9, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.R.; Dodge, B.; Schick, V.; Herbenick, D.; Hubach, R.; Bowling, J.; Goncalves, G.; Krier, S.; Reece, M. From bias to bisexual health disparities: Attitudes toward bisexual men and women in the United States. LGBT Health 2014, 1, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef] [PubMed]
- Horne, S.G.; Puckett, J.A.; Apter, R.; Levitt, H.M. Positive Psychology and LGBTQ Populations. In Perspectives on the Intersection of Multiculturalism and Positive Psychology; Teramoto Pedrotti, J., Edwards, L.M., Eds.; Springer Science + Business Media: New York, NY, USA, 2014; pp. 189–202. [Google Scholar]
- Levitt, H.M.; Kehoe, K.A.; Hand, A.B. Beyond minority stress: Toward a multidimensional psychology of trans/nonbinary gender. Curr. Opin. Psychol. 2022, 49, 101515. [Google Scholar] [CrossRef]
- Tuck, E. Suspending damage: A letter to communities. Harv. Educ. Rev. 2009, 79, 409–427. [Google Scholar] [CrossRef]
- Bostwick, W.B.; Hughes, T.L.; Everett, B. Health behavior, status, and outcomes among a community-based sample of lesbian and bisexual women. LGBT Health 2015, 2, 121–126. [Google Scholar] [CrossRef]
- Puckett, J.A.; Surace, F.I.; Levitt, H.M.; Horne, S.G. Sexual orientation identity in relation to minority stress and mental health in sexual minority women. LGBT Health 2016, 3, 350–356. [Google Scholar] [CrossRef]
- Dyar, C.; Feinstein, B.A.; Stephens, J.; Zimmerman, A.; Newcomb, M.E.; Whitton, S.W. Nonmonosexual stress and dimensions of health: Within-group variation by sexual, gender, and racial/ethnic identities. Psychol. Sex. Orientat. Gend. Divers. 2020, 7, 12–25. [Google Scholar] [CrossRef]
- Katz-Wise, S.L.; Mereish, E.H.; Woulfe, J. Associations of bisexual-specific minority stress and health among cisgender and transgender adults with bisexual orientation. J. Sex. Res. 2017, 54, 899–910. [Google Scholar] [CrossRef]
- Rahman, M.; Li, D.H.; Moskowitz, D.A. Comparing the healthcare utilization and engagement in a sample of transgender and cisgender bisexual+ persons. Arch. Sex. Behav. 2019, 48, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Meyer, I.H.; Russell, S.T.; Hammack, P.L.; Frost, D.M.; Wilson, B. Minority stress, distress, and suicide attempts in three cohorts of sexual minority adults: A U.S. probability sample. PLoS ONE 2021, 16, e0246827. [Google Scholar] [CrossRef] [PubMed]
- Puckett, J.A.; Tornello, S.; Mustanski, B.; Newcomb, M.E. Gender variations, generational effects, and mental health of transgender people in relation to timing and status of gender identity milestones. Psychol. Sex. Orientat. Gend. Divers. 2022, 9, 165–178. [Google Scholar] [CrossRef] [PubMed]
- Scandurra, C.; Carbone, A.; Baiocco, R.; Mezzalira, S.; Maldonato, N.M.; Bochicchio, V. Gender identity milestones, minority stress and mental health in three generational cohorts of Italian binary and nonbinary transgender people. Int. J. Environ. Res. Public Health 2021, 18, 9057. [Google Scholar] [CrossRef] [PubMed]
- Bostwick, W.B.; Boyd, C.J.; Hughes, T.L.; McCabe, S.E. Dimensions of sexual orientation and the prevalence of mood and anxiety disorders in the United States. Am. J. Public Health 2010, 100, 468–475. [Google Scholar] [CrossRef]
- Katz-Wise, S.L.; Hyde, J.S. Victimization experiences of lesbian, gay, and bisexual individuals: A meta-analysis. J. Sex. Res. 2012, 49, 142–167. [Google Scholar] [CrossRef] [PubMed]
- Ross, L.E.; Salway, T.; Tarasoff, L.A.; MacKay, J.M.; Hawkins, B.W.; Fehr, C.P. Prevalence of depression and anxiety among bisexual people compared to gay, lesbian, and heterosexual individuals: A systematic review and meta-analysis. J. Sex. Res. 2018, 55, 435–456. [Google Scholar] [CrossRef]
- Taliaferro, L.A.; Gloppen, K.M.; Muehlenkamp, J.J.; Eisenberg, M.E. Depression and suicidality among bisexual youth: A nationally representative sample. J. LGBT Youth 2018, 15, 16–31. [Google Scholar] [CrossRef]
- Brewster, M.E.; Moradi, B. Perceived experiences of anti-bisexual prejudice: Instrument development and evaluation. J. Couns. Psychol. 2010, 57, 451–468. [Google Scholar] [CrossRef]
- de Lira, A.N.; de Morais, N.A. Resilience in lesbian, gay, and bisexual (LGB) populations: An integrative literature review. Sex. Res. Soc. Policy 2018, 15, 272–282. [Google Scholar] [CrossRef]
- Paul, R.; Smith, N.G.; Mohr, J.J.; Ross, L.E. Measuring dimensions of bisexual identity: Initial development of the Bisexual Identity Inventory. Psychol. Sex. Orientat. Gend. Divers. 2014, 1, 452–460. [Google Scholar] [CrossRef]
- Rostosky, S.S.; Riggle, E.D.B.; Pascale-Hague, D.; McCants, L.E. The positive aspects of a bisexual self-identifi cation. Psychol. Sex. 2010, 1, 131–144. [Google Scholar] [CrossRef]
- Pistella, J.; Salvati, M.; Ioverno, S.; Laghi, F.; Baiocco, R. Coming-out to family members and internalized sexual stigma in bisexual, lesbian and gay people. J. Child Fam. Stud. 2016, 25, 3694–3701. [Google Scholar] [CrossRef]
- Verrastro, V.; Fontanesi, L.; Petruccelli, I.; Santamaria, F.; Laghi, F.; Ioverno, S.; Baiocco, R. Binge drinking and internalized sexual stigma among Italian lesbian, gay and bisexual young adults. Nord. Stud. Alcohol. Drugs 2016, 33, 437–446. [Google Scholar] [CrossRef]
- Petrocchi, N.; Pistella, J.; Salvati, M.; Carone, N.; Laghi, F.; Baiocco, R. I embrace my LGB identity: Self-reassurance, social safeness, and the distinctive relevance of authenticity to well-being in Italian lesbians, gay men, and bisexual people. Sex. Res. Soc. Policy 2020, 17, 75–86. [Google Scholar] [CrossRef]
- Monaco, S. Being bisexual in contemporary Italy: Between stigma and desire of visibility. Int. J. Sociol. Soc. Policy 2021, 41, 673–688. [Google Scholar] [CrossRef]
- Scandurra, C.; Pennasilico, A.; Esposito, C.; Mezza, F.; Vitelli, R.; Bochicchio, V.; Maldonato, N.M.; Amodeo, A.L. Minority stress and mental health in Italian bisexual people. Soc. Sci. 2020, 9, 46. [Google Scholar] [CrossRef]
- Pistella, J.; Rosati, F.; Baiocco, R. Feeling safe and content: Relationship to internalized sexual stigma, self-awareness, and identity uncertainty in Italian lesbian and bisexual women. J. Lesbian Stud. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Rucco, D.; Anzani, A.; Scandurra, C.; Pennasilico, A.; Prunas, A. Structural stigma and bisexual + people: Effects of the rejection of the Zan Bill in Italy on minority stress and mental health. J. Bisex. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Meyer, I.H. Minority stress and positive psychology: Convergences and divergences to understanding LGBT health. Psychol. Sex. Orientat. Gend. Divers. 2014, 1, 348–349. [Google Scholar] [CrossRef]
- Vaughan, M.D.; Rodriguez, E.M. LGBT strengths: Incorporating positive psychology into theory, research, training, and practice. Psychol. Sex. Orientat. Gend. Divers. 2014, 1, 325–334. [Google Scholar] [CrossRef]
- Crenshaw, K. Demarginalizing the intersection of race and sex: A black feminist critique of antidiscrimination doctrine, feminist theory and antiracist politics. Univ. Chic. Leg. Forum 1989, 140, 139–167. [Google Scholar]
- Cole, E.R. Intersectionality and research in psychology. Am. Psychol. 2009, 64, 170–180. [Google Scholar] [CrossRef]
- Elder, G.H. The life course as developmental theory. Child Dev. 1998, 69, 1–12. [Google Scholar] [CrossRef]
- Seligman, M.E.P.; Csikszentmihalyi, M. Positive psychology: An introduction. Am. Psychol. 2000, 55, 5–14. [Google Scholar] [CrossRef]
- Duckworth, A.L.; Steen, T.A.; Seligman, M.E. Positive psychology in clinical practice. Annu. Rev. Clin. Psychol. 2005, 1, 629–651. [Google Scholar] [CrossRef]
- Bruce, D.; Harper, G.W.; Bauermeister, J.A. Minority stress, positive identity development, and depressive symptoms: Implications for resilience among sexual minority male youth. Psychol. Sex. Orientat. Gend. Divers. 2015, 2, 287–296. [Google Scholar] [CrossRef]
- Levitt, H.M.; Ippolito, M.R. Being transgender: Navigating minority stressors and developing authentic self-presentation. Psychol. Women Q. 2014, 38, 46–64. [Google Scholar] [CrossRef]
- Riggle, E.B.; Whitman, J.S.; Olson, A.; Rostosky, S.S.; Strong, S. The positive aspects of being a lesbian or gay man. Prof. Psychol. Res. Pract. 2008, 39, 210–217. [Google Scholar] [CrossRef]
- Brownfield, J.M.; Brown, C.; Jeevanba, S.B.; VanMattson, S.B. More than simply getting bi: An examination of coming out growth for bisexual individuals. Psychol. Sex. Orientat. Gend. Divers. 2018, 5, 220–232. [Google Scholar] [CrossRef]
- Dencker, J.C.; Joseph, A.J.; Martocchio, J. Towards a theoretical framework linking generational memories to workplace attitudes and behaviors. Hum. Resour. Manag. Rev. 2008, 18, 180–187. [Google Scholar] [CrossRef]
- Anderson, E.; Magrath, R.; Bullingham, R. Out in Sport: The Experiences of Openly Gay and Lesbian Athletes in Competitive Sport; Routledge: New York, NY, USA, 2016. [Google Scholar]
- McCormack, M.; Anderson, E. The influence of declining homophobia on men’s gender in the United States: An argument for the study of homohysteria. Sex. Roles 2014, 71, 109–120. [Google Scholar] [CrossRef]
- Rosati, F.; Pistella, J.; Nappa, M.R.; Baiocco, R. The coming-out process in family, social, and religious contexts among young, middle, and older Italian LGBQ+ adults. Front. Psychol. 2020, 11, 617217. [Google Scholar] [CrossRef] [PubMed]
- Dyar, C.; Sarno, E.L.; Newcomb, M.E.; Whitton, S.W. Longitudinal associations between minority stress, internalizing symptoms, and substance use among sexual and gender minority individuals assigned female at birth. J. Consult. Clin. Psychol. 2020, 88, 389–401. [Google Scholar] [CrossRef] [PubMed]
- Hatzenbuehler, M.L. How does sexual minority stigma “get under the skin”? A psychological mediation framework. Psychol. Bull. 2009, 135, 707–730. [Google Scholar] [CrossRef]
- Scandurra, C.; Bochicchio, V.; Amodeo, A.L.; Esposito, C.; Valerio, P.; Maldonato, N.M.; Bacchini, D.; Vitelli, R. Internalized transphobia, resilience, and mental health: Applying the Psychological Mediation Framework to Italian transgender individuals. Int. J. Environ. Res. Public Health 2018, 15, 508. [Google Scholar] [CrossRef]
- Schwartz, D.R.; Stratton, N.; Hart, T.A. Minority stress and mental and sexual health: Examining the psychological mediation framework among gay and bisexual men. Psychol. Sex. Orientat. Gend. Divers. 2016, 3, 313–324. [Google Scholar] [CrossRef]
- Schuler, M.S.; Stein, B.D.; Collins, R.L. Differences in substance use disparities across age groups in a national cross-sectional survey of lesbian, gay, and bisexual adults. LGBT Health 2019, 6, 68–76. [Google Scholar] [CrossRef]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1988, 52, 30–41. [Google Scholar] [CrossRef]
- Ryff, C.D. Happiness is everything, or is it? Explorations on the meaning of psychological well-being. J. Pers. Soc. Psychol. 1989, 57, 1069–1081. [Google Scholar] [CrossRef]
- Weston, R.; Gore, P.A. A brief guide to structural equation modeling. Couns. Psychol. 2006, 34, 719–751. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modelling, 3rd ed.; The Guilford Press: London, UK, 2011. [Google Scholar]
- Chew, D.; Tollit, M.A.; Poulakis, Z.; Zwickl, S.; Cheung, A.S.; Pang, K.C. Youths with a non-binary gender identity: A review of their sociodemographic and clinical profile. Lancet Child Adolesc. Health 2020, 4, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Kaltiala-Heino, R.; Lindberg, N. Gender identities in adolescent population: Methodological issues and prevalence across age groups. Eur. Psychiatry 2019, 55, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Scandurra, C.; Mezza, F.; Maldonato, N.M.; Bottone, M.; Bochicchio, V.; Valerio, P.; Vitelli, R. Health of non-binary and genderqueer people: A systematic review. Front. Psychol. 2019, 10, 1453. [Google Scholar] [CrossRef] [PubMed]
- Doyle, D.M.; Begeny, C.T.; Barreto, M.; Morton, T.A. Identity-related factors protect well-being against stigma for transgender and gender non-conforming people. Arch. Sex. Behav. 2021, 50, 3191–3200. [Google Scholar] [CrossRef] [PubMed]
- Garr-Schultz, A.; Gardner, W. “It’s just a phase”: Identity denial experiences, self-concept clarity, and emotional well-being in bisexual individuals. Self Identity 2021, 20, 528–544. [Google Scholar] [CrossRef]
- Wakslak, C.J.; Trope, Y. Cognitive consequences of affirming the self: The relationship between self-affirmation and object construal. J. Exp. Soc. Psychol. 2009, 45, 927–932. [Google Scholar] [CrossRef]
- Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in older adults. Annu. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef]
- Volkert, J.; Schulz, H.; Härter, M.; Wlodarczyk, O.; Andreas, S. The prevalence of mental disorders in older people in Western countries—A meta-analysis. Ageing Res. Rev. 2013, 12, 339–353. [Google Scholar] [CrossRef]
- Wolitzky-Taylor, K.B.; Castriotta, N.; Lenze, E.J.; Stanley, M.A.; Craske, M.G. Anxiety disorders in older adults: A comprehensive review. Depress. Anxiety 2010, 27, 190–211. [Google Scholar] [CrossRef]
- Bybee, J.A.; Sullivan, E.L.; Zielonka, E.; Moes, E. Are gay men in worse mental health than heterosexual men? The role of age, shame and guilt, and coming-out. J. Adult Dev. 2009, 16, 144–154. [Google Scholar] [CrossRef]
- Monin, J.K.; Mota, N.; Levy, B.; Pachankis, J.; Pietrzak, R.H. Older age associated with mental health resiliency in sexual minority US veterans. Am. J. Geriatr. Psychiatry 2017, 25, 81–90. [Google Scholar] [CrossRef] [PubMed]
- Dyar, C.; London, B. Longitudinal examination of a bisexual-specific minority stress process among bisexual cisgender women. Psychol. Women Q. 2018, 42, 342–360. [Google Scholar] [CrossRef]
- Wang, A.Y.; Feinstein, B.A. The perks of being bi+: Positive sexual orientation–related experiences among bisexual, pansexual, and queer male youth. Psychol. Sex. Orientat. Gend. Divers. 2022, 9, 58–70. [Google Scholar] [CrossRef] [PubMed]
- Rostosky, S.S.; Cardom, R.D.; Hammer, J.H.; Riggle, E.D.B. LGB positive identity and psychological well-being. Psychol. Sex. 2018, 5, 482–489. [Google Scholar] [CrossRef]
- Baiocco, R.; Scandurra, C.; Rosati, F.; Pistella, J.; Ioverno, S.; Bochicchio, V.; Wang, H.C.; Chang, T.S. Minority stress, resilience, and health in Italian and Taiwanese LGB+ people: A cross-cultural comparison. Curr. Psychol. 2021. Online ahead of print. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Total Sample (n = 483) | Cisgender (n = 354) | Non-Binary (n = 129) | ||
|---|---|---|---|---|
| n (%) | n (%) | n (%) | χ2 | |
| Age | ||||
| 18–25 years | 213 (44.1) | 150 (42.4) | 63 (48.8) | 1.63 |
| 26–34 years | 219 (45.3) | 165 (46.6) | 54 (41.9) | |
| 35–49 years | 51 (10.6) | 39 (11) | 12 (9.3) | |
| Sex assigned at birth | ||||
| Male | 81 (16.8) | 55 (15.5) | 26 (20.2) | 1.44 |
| Female | 402 (83.2) | 299 (84.5) | 103 (79.8) | |
| Ethnicity | ||||
| Caucasian | 476 (98.6) | 349 (98.6) | 127 (98.4) | 0.01 |
| Non-Caucasian | 7 (1.4) | 5 (1.4) | 2 (1.6) | |
| Education | ||||
| ≤High school | 201 (41.6) | 143 (40.4) | 58 (45) | 0.81 |
| ≥College | 282 (58.4) | 211 (59.6) | 71 (55) | |
| Stable partner | ||||
| No | 209 (43.3) | 152 (42.9) | 57 (44.2) | 0.06 |
| One or more | 274 (56.7) | 202 (57.1) | 72 (55.8) |
| 1 | 2 | 3 | M ± SD | Ranges | |
|---|---|---|---|---|---|
| 1. Perceived social support | — | 0.10 | 0.51 *** | 5.27 ± 1.13 | 1–7 |
| 2. Identity affirmation | 0.18 ** | — | 0.38 *** | 6.06 ± 1.05 | 1–7 |
| 3. Psychological well-being | 0.42 *** | 0.19 *** | — | 56.47 ± 9.39 | 14–84 |
| Gender Identity | ||||||
|---|---|---|---|---|---|---|
| Cisgender (n = 354) | Non-Binary (n = 129) | |||||
| M | SD | M | SD | F | η2 | |
| Perceived social support | 5.36 | 1.09 | 5.02 | 1.17 | 8.79 ** | 0.02 |
| Identity affirmation | 5.98 | 1.09 | 6.27 | 0.87 | 7.20 ** | 0.01 |
| Psychological well-being | 57.34 | 9.14 | 54.09 | 9.68 | 11.54 ** | 0.02 |
| Age Cohorts | ||||||||
|---|---|---|---|---|---|---|---|---|
| Young Adults (18–25 Years) (n = 213) | Early Adults (26–34 Years) (n = 219) | Middle Adults (35–49 Years) (n = 51) | ||||||
| M | SD | M | SD | M | SD | F | η2 | |
| Perceived social support | 5.21 | 1.14 | 5.33 | 1.10 | 5.26 | 1.19 | 0.55 | <0.01 |
| Identity affirmation | 6.17 | 0.99 | 5.95 | 1.07 | 6.07 | 1.12 | 2.46 | 0.01 |
| Psychological well-being | 54.96 a | 9.49 | 57.39 b | 8.71 | 58.88 b | 10.88 | 5.59 ** | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scandurra, C.; Esposito, C.; Fantacci, F.; Borrello, L.; Bochicchio, V.; Giunti, D.; Antonelli, P. Social Support, Identity Affirmation, and Psychological Well-Being: A Developmental and Intersectional Comparison between Italian Cisgender and Non-Binary People with Bisexual Orientation. Int. J. Environ. Res. Public Health 2023, 20, 3237. https://doi.org/10.3390/ijerph20043237
Scandurra C, Esposito C, Fantacci F, Borrello L, Bochicchio V, Giunti D, Antonelli P. Social Support, Identity Affirmation, and Psychological Well-Being: A Developmental and Intersectional Comparison between Italian Cisgender and Non-Binary People with Bisexual Orientation. International Journal of Environmental Research and Public Health. 2023; 20(4):3237. https://doi.org/10.3390/ijerph20043237
Chicago/Turabian StyleScandurra, Cristiano, Concetta Esposito, Francesco Fantacci, Lorenzo Borrello, Vincenzo Bochicchio, Daniel Giunti, and Paolo Antonelli. 2023. "Social Support, Identity Affirmation, and Psychological Well-Being: A Developmental and Intersectional Comparison between Italian Cisgender and Non-Binary People with Bisexual Orientation" International Journal of Environmental Research and Public Health 20, no. 4: 3237. https://doi.org/10.3390/ijerph20043237
APA StyleScandurra, C., Esposito, C., Fantacci, F., Borrello, L., Bochicchio, V., Giunti, D., & Antonelli, P. (2023). Social Support, Identity Affirmation, and Psychological Well-Being: A Developmental and Intersectional Comparison between Italian Cisgender and Non-Binary People with Bisexual Orientation. International Journal of Environmental Research and Public Health, 20(4), 3237. https://doi.org/10.3390/ijerph20043237