
A Serial Mediation Model of Insecure Attachment and Psychological Distress: The Role of Dispositional Shame and Shame-Coping Styles

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Preliminary Analyses
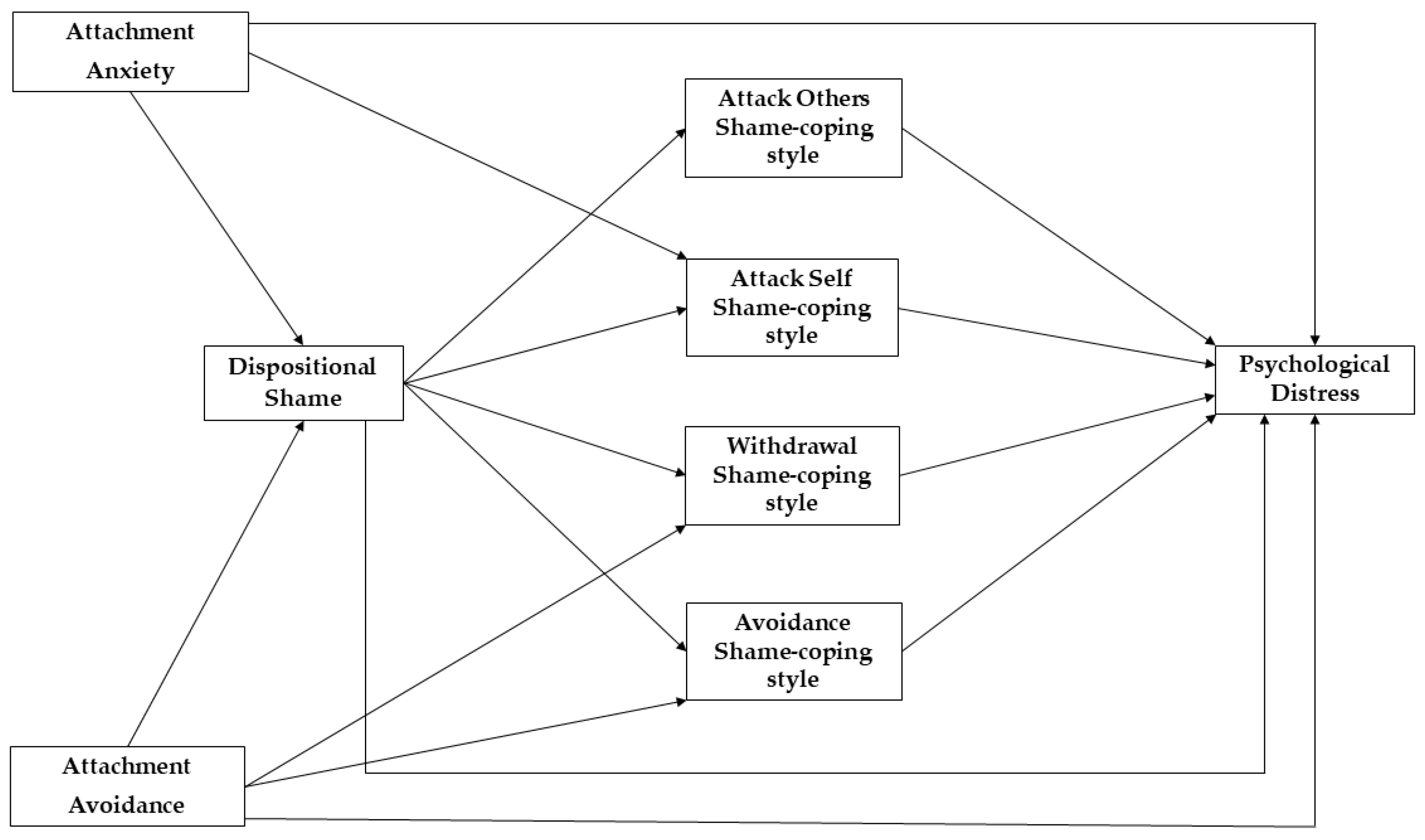
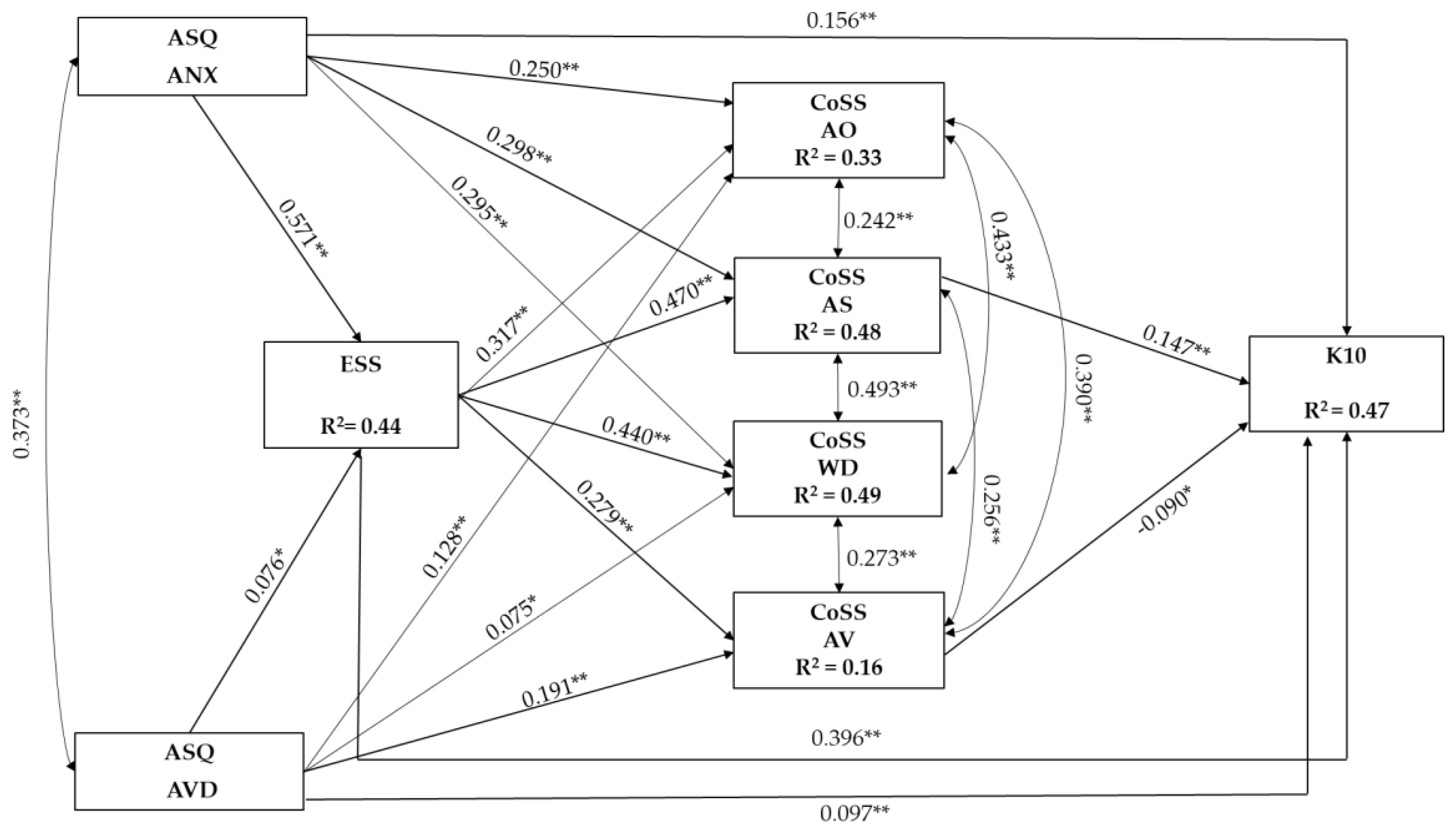
3.3. Serial Mediation Model
3.4. Multi-Group Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lopez, F.G.; Brennan, K.A. Dynamic processes underlying adult attachment organization: Toward an attachment theoretical perspective on the healthy and effective self. J. Couns. Psychol. 2000, 47, 283–300. [Google Scholar] [CrossRef]
- Mallinckrodt, B. Attachment, social competencies, social support, and interpersonal process in psychotherapy. Psychother. Res. 2000, 10, 239–266. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R. Attachment in Adulthood: Structure, Dynamics, and Change, 2nd ed.; The Guilford Press: New York, NY, USA, 2016; p. 578. [Google Scholar]
- Pascuzzo, K.; Cyr, C.; Moss, E. Longitudinal association between adolescent attachment, adult romantic attachment, and emotion regulation strategies. Attach. Hum. Dev. 2013, 15, 83–103. [Google Scholar] [CrossRef] [PubMed]
- Tasca, G.A.; Brugnera, A.; Baldwin, D.; Carlucci, S.; Compare, A.; Balfour, L.; Proulx, G.; Gick, M.; Lafontaine, M.F. Reliability and validity of the Experiences in Close Relationships Scale-12: Attachment dimensions in a clinical sample with eating disorders. Int. J. Eat. Disord. 2018, 51, 18–27. [Google Scholar] [CrossRef]
- Simpson, J.A.; Rholes, W.S. Adult attachment orientations and well-being during the transition to parenthood. Curr. Opin. Psychol. 2019, 25, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Mikulincer, M.; Shaver, P.R. An attachment perspective on psychopathology. World Psychiatry 2012, 11, 11–15. [Google Scholar] [CrossRef]
- Jinyao, Y.; Xiongzhao, Z.; Auerbach, R.P.; Gardiner, C.K.; Lin, C.; Yuping, W.; Shuqiao, Y. Insecure attachment as a predictor of depressive and anxious symptomology. Depress. Anxiety 2012, 29, 789–796. [Google Scholar] [CrossRef]
- Marganska, A.; Gallagher, M.; Miranda, R. Adult attachment, emotion dysregulation, and symptoms of depression and generalized anxiety disorder. Am. J. Orthopsychiatry 2013, 83, 131–141. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Shaffer, P.A.; Young, S.K.; Zakalik, R.A. Adult Attachment, Shame, Depression, and Loneliness: The Mediation Role of Basic Psychological Needs Satisfaction. J. Couns. Psychol. 2005, 52, 591–601. [Google Scholar] [CrossRef]
- De Paoli, T.; Fuller-Tyszkiewicz, M.; Halliwell, E.; Puccio, F.; Krug, I. Social Rank and Rejection Sensitivity as Mediators of the Relationship between Insecure Attachment and Disordered Eating. Eur. Eat. Disord. Rev. 2017, 25, 469–478. [Google Scholar] [CrossRef]
- Bayrak, R.; Güler, M.; Şahin, N.H. The Mediating Role of Self-Concept and Coping Strategies on the Relationship between Attachment Styles and Perceived Stress. Eur. J. Psychol. 2018, 14, 897–913. [Google Scholar] [CrossRef] [PubMed]
- Bowlby, J. A Secure Base: Clinical Applications of Attachment Theory; Routledge: London, UK, 1988. [Google Scholar]
- Marshall, W.L.; Marshall, L.E.; Serran, G.A.; O’Brien, M.D. Self-esteem, shame, cognitive distortions and empathy in sexual offenders: Their integration and treatment implications. Psychol. Crime Law 2009, 15, 217–234. [Google Scholar] [CrossRef]
- Elison, J.; Lennon, R.; Pulos, S. Investigating the compass of shame: The development of the Compass of Shame Scale. Soc. Behav. Personal. Int. J. 2006, 34, 221–238. [Google Scholar] [CrossRef]
- Elison, J.; Pulos, S.; Lennon, R. Shame-Focused Coping: An Empirical Study of the Compass of Shame. Soc. Behav. Personal. Int. J. 2006, 34, 161–168. [Google Scholar] [CrossRef]
- Vagos, P.; Ribeiro da Silva, D.; Brazão, N.; Rijo, D.; Elison, J. Psychometric Properties of the Compass of Shame Scale: Testing for Measurement Invariance Across Community Boys and Boys in Foster Care and Juvenile Detentions Facilities. Child Youth Care Forum 2019, 48, 93–110. [Google Scholar] [CrossRef]
- Passanisi, A.; Gervasi, A.M.; Madonia, C.; Guzzo, G.; Greco, D. Attachment, Self-Esteem and Shame in Emerging Adulthood. Procedia Soc. Behav. Sci. 2015, 191, 342–346. [Google Scholar] [CrossRef]
- Matos, M.; Pinto-Gouveia, J. Shame as a traumatic memory. Clin. Psychol. Psychother. 2010, 17, 299–312. [Google Scholar] [CrossRef] [PubMed]
- Matos, M.; Pinto-Gouveia, J.; Costa, V. Understanding the importance of attachment in shame traumatic memory relation to depression: The impact of emotion regulation processes. Clin. Psychol. Psychother. 2013, 20, 149–165. [Google Scholar] [CrossRef]
- Andrews, B.; Qian, M.; Valentine, J.D. Predicting depressive symptoms with a new measure of shame: The Experience of Shame Scale. Br. J. Clin. Psychol. 2002, 41 Pt 1, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Tangney, J.P.; Dearing, R.L. Shame and Guilt; Guilford Press: New York, NY, USA, 2002; p. xvi, 272. [Google Scholar]
- Leeming, D.; Boyle, M. Shame as a social phenomenon: A critical analysis of the concept of dispositional shame. Psychol. Psychother. 2004, 77, 375–396. [Google Scholar] [CrossRef]
- Gilbert, P. The relationship of shame, social anxiety and depression: The role of the evaluation of social rank. Clin. Psychol. Psychother. 2000, 7, 174–189. [Google Scholar] [CrossRef]
- Cibich, M.; Woodyatt, L.; Wenzel, M. Moving beyond “shame is bad”: How a functional emotion can become problematic. Soc. Personal. Psychol. Compass 2016, 10, 471–483. [Google Scholar] [CrossRef]
- Gilbert, P. Evolution, Social Roles, and the Differences in Shame and Guilt. Soc. Res. 2003, 70, 1205–1230. [Google Scholar] [CrossRef]
- Muris, P.; Meesters, C. Small or Big in the Eyes of the Other: On the Developmental Psychopathology of Self-Conscious Emotions as Shame, Guilt, and Pride. Clin. Child Fam. Psychol. Rev. 2014, 17, 19–40. [Google Scholar] [CrossRef] [PubMed]
- Velotti, P.; Garofalo, C.; Bottazzi, F.; Caretti, V. Faces of Shame: Implications for Self-Esteem, Emotion Regulation, Aggression, and Well-Being. J. Psychol. 2017, 151, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Elison, J.; Garofalo, C.; Velotti, P. Shame and aggression: Theoretical considerations. Aggress. Violent Behav. 2014, 19, 447–453. [Google Scholar] [CrossRef]
- Kim, S.; Thibodeau, R.; Jorgensen, R.S. Shame, guilt, and depressive symptoms: A meta-analytic review. Psychol. Bull. 2011, 137, 68–96. [Google Scholar] [CrossRef]
- Bilevicius, E.; Neufeld, D.C.; Single, A.; Foot, M.; Ellery, M.; Keough, M.T.; Johnson, E.A. Vulnerable narcissism and addiction: The mediating role of shame. Addict. Behav. 2019, 92, 115–121. [Google Scholar] [CrossRef]
- Schoenleber, M.; Berenbaum, H. Shame aversion and shame-proneness in Cluster C personality disorders. J. Abnorm. Psychol. 2010, 119, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Nathanson, D.L. Shame and Pride: Affect, Sex, and the Birth of the Self; WW Norton & Company: New York, NY, USA, 1994. [Google Scholar]
- Garofalo, C.; Velotti, P. Shame coping and psychopathy: A replication and extension in a sample of male incarcerated offenders. J. Crim. Justice 2021, 76, 101845. [Google Scholar] [CrossRef]
- Campbell, J.S.; Elison, J. Shame coping styles and psychopathic personality traits. J. Pers. Assess. 2005, 84, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Schore, A.N. Early Shame Experiences and Infant Brain Development. In Shame: Interpersonal Behavior, Psychopathology, and Culture; Oxford University Press: New York, NY, USA, 1998; pp. 57–77. [Google Scholar]
- Hewitt, P.L.; Flett, G.L.; Mikail, S.F. Perfectionism: A Relational Approach to Conceptualization, Assessment, and Treatment; The Guilford Press: New York, NY, USA, 2017; p. xv, 336. [Google Scholar]
- DeVille, D.C.; Ellmo, F.I.; Horton, W.A.; Erchull, M.J. The Role of Romantic Attachment in Women’s Experiences of Body Surveillance and Body Shame. Gend. Issues 2015, 32, 111–120. [Google Scholar] [CrossRef]
- Cheche Hoover, R.; Jackson, J.B. Insecure Attachment, Emotion Dysregulation, and Psychological Aggression in Couples. J. Interpers. Violence 2021, 36, NP10908–NP10936. [Google Scholar] [CrossRef]
- Hazan, C.; Shaver, P.R. Attachment as an organizational framework for research on close relationships. Psychol. Inq. 1994, 5, 1–22. [Google Scholar] [CrossRef]
- Ferguson, T.J.; Eyre, H.L.; Ashbaker, M. Unwanted Identities: A Key Variable in Shame–Anger Links and Gender Differences in Shame. Sex Roles 2000, 42, 133–157. [Google Scholar] [CrossRef]
- Paulo, M.; Vagos, P.; Ribeiro Da Silva, D.; Rijo, D. The role of shame and shame coping strategies on internalizing/externalizing symptoms: Differences across gender in adolescents. Eur. J. Dev. Psychol. 2020, 17, 578–597. [Google Scholar] [CrossRef]
- Szentágotai-Tătar, A.; Miu, A.C. Individual Differences in Emotion Regulation, Childhood Trauma and Proneness to Shame and Guilt in Adolescence. PLoS ONE 2016, 11, e0167299. [Google Scholar] [CrossRef]
- Feeney, J.A.; Noller, P.; Hanrahan, M. Assessing adult attachment. In Attachment in Adults: Clinical and Developmental Perspectives; Guilford Press: New York, NY, USA, 1994; pp. 128–152. [Google Scholar]
- Fossati, A.; Feeney, J.A.; Donati, D.; Donini, M.; Novella, L.; Bagnato, M.; Acquarini, E.; Maffei, C. On the Dimensionality of the Attachment Style Questionnaire in Italian Clinical and Nonclinical Participants. J. Soc. Pers. Relatsh. 2003, 20, 55–79. [Google Scholar] [CrossRef]
- Caretti, V.; Craparo, G.; Schimmenti, A. Il ruolo della disregolazione affettiva, della dissociazione e della vergogna nei disturbi del comportamento alimentare. In Addiction. Aspetti Biologici e di Ricerca; Raffaello Cortina Editore: Milano, Italy, 2010; pp. 135–165. [Google Scholar]
- Behling, O.; Law, K.S. Translating Questionnaires and Other Research Instruments; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2000. [Google Scholar]
- Carrà, G.; Sciarini, P.; Segagni-Lusignani, G.; Clerici, M.; Montomoli, C.; Kessler, R.C. Do they actually work across borders? Evaluation of two measures of psychological distress as screening instruments in a non Anglo-Saxon country. Eur. Psychiatry 2011, 26, 122–127. [Google Scholar] [CrossRef]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.L.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 7th ed.; Pearson Education: Boston, MA, USA, 2019. [Google Scholar]
- Mansfield, E.R.; Helms, B.P. Detecting Multicollinearity. Am. Stat. 1982, 36, 158–160. [Google Scholar]
- Frigon, J.-Y.; Laurencelle, L. Analysis of Covariance: A Proposed Algorithm. Educ. Psychol. Meas. 1993, 53, 1–18. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Byrne, B.M. Structural Equation Modeling with EQS: Basic Concepts, Applications, and Programming, 2nd ed.; Routledge: New York, NY, USA, 2006. [Google Scholar]
- Cheung, G.W.; Rensvold, R.B. Evaluating Goodness-of-Fit Indexes for Testing Measurement Invariance. Struct. Equ. Model. A Multidiscip. J. 2002, 9, 233–255. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Gilbert, P.; Irons, C. Shame, self-criticism, and self-compassion in adolescence. In Adolescent Emotional Development and the Emergence of Depressive Disorders; Sheeber, L.B., Allen, N.B., Eds.; Cambridge University Press: Cambridge, UK, 2008; pp. 195–214. [Google Scholar]
- Fossum, M.A.; Mason, M.J. Facing Shame: Families in Recovery; WW Norton & Company: New York, NY, USA, 1989. [Google Scholar]
- Sedighimornani, N.; Rimes, K.; Verplanken, B. Factors contributing to the experience of shame and shame management: Adverse childhood experiences, peer acceptance, and attachment styles. J. Soc. Psychol. 2021, 161, 129–145. [Google Scholar] [CrossRef] [PubMed]
- Gross, C.A.; Hansen, N.E. Clarifying the experience of shame: The role of attachment style, gender, and investment in relatedness. Personal. Individ. Differ. 2000, 28, 897–907. [Google Scholar] [CrossRef]
- Read, D.L.; Clark, G.I.; Rock, A.J.; Coventry, W.L. Adult attachment and social anxiety: The mediating role of emotion regulation strategies. PLoS ONE 2018, 13, e0207514. [Google Scholar] [CrossRef]
- Corcoran, M.; McNulty, M. Examining the role of attachment in the relationship between childhood adversity, psychological distress and subjective well-being. Child Abuse Negl. 2018, 76, 297–309. [Google Scholar] [CrossRef]
- Remondi, C.; Compare, A.; Tasca, G.A.; Greco, A.; Pievani, L.; Poletti, B.; Brugnera, A. Insecure Attachment and Technology Addiction Among Young Adults: The Mediating Role of Impulsivity, Alexithymia, and General Psychological Distress. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 761–767. [Google Scholar] [CrossRef]
- Gilbert, P.; Woodyatt, L. An Evolutionary Approach to Shame-Based Self-Criticism, Self-Forgiveness, and Compassion. In Handbook of the Psychology of Self-Forgiveness; Woodyatt, L., Worthington, J.E.L., Wenzel, M., Griffin, B.J., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 29–41. [Google Scholar]
- Martin, F.; Scheel, C.; Legenbauer, T. Shame Coping Strategies Amplify Certain Psychopathologies. Psychopathology 2021, 54, 305–314. [Google Scholar] [CrossRef]
- Dorahy, M.J.; Corry, M.; Shannon, M.; Webb, K.; McDermott, B.; Ryan, M.; Dyer, K.F. Complex trauma and intimate relationships: The impact of shame, guilt and dissociation. J. Affect. Disord. 2013, 147, 72–79. [Google Scholar] [CrossRef]
- Dyer, K.F.; Dorahy, M.J.; Corry, M.; Black, R.; Matheson, L.; Coles, H.; Curran, D.; Seager, L.; Middleton, W. Comparing shame in clinical and nonclinical populations: Preliminary findings. Psychol. Trauma 2017, 9, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Kealy, D.; Treeby, M.S.; Rice, S.M.; Spidel, A. Shame and guilt as mediators between dispositional optimism and symptom severity among mental health outpatients. Psychol. Health Med. 2022, 27, 1245–1254. [Google Scholar] [CrossRef] [PubMed]
- Capinha, M.; Rijo, D.; Matos, M.; Pereira, M. The Compass of Shame Scale: Dimensionality and Gender Measurement Invariance in a Portuguese Sample. J. Pers. Assess. 2021, 103, 807–817. [Google Scholar] [CrossRef]
- Leeming, D.; Boyle, M. Managing shame: An interpersonal perspective. Br. J. Soc. Psychol. 2013, 52, 140–160. [Google Scholar] [CrossRef]
- Van Vliet, K.J. Shame and resilience in adulthood: A grounded theory study. J. Couns. Psychol. 2008, 55, 233–245. [Google Scholar] [CrossRef]
- Black, R.S.; Curran, D.; Dyer, K.F. The impact of shame on the therapeutic alliance and intimate relationships. J. Clin. Psychol. 2013, 69, 646–654. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | Mean (SD) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Gender | - | |||||||||||
| 2. Age | 32.17 (13.48) | −0.100 ** | - | |||||||||
| 3. Education | 0.139 ** | −0.198 ** | - | |||||||||
| 4. Job status | 0.192 ** | −0.165 ** | 0.033 | - | ||||||||
| 5. ASQ ANX | 47.51 (12.18) | 0.135 ** | −0.197 ** | 0.056 | 0.068 ** | - | ||||||
| 6. ASQ AVD | 51.24 (10.74) | −0.058 | −0.008 | −0.054 | 0.004 | 0.368 ** | - | |||||
| 7. ESS | 45.86 (14.02) | 0.198 ** | −0.302 ** | 0.119 ** | 0.065 ** | 0.636 ** | 0.288 ** | - | ||||
| 8. CoSS AO | 11.47 (7.34) | 0.133 ** | −0.135 ** | 0.092 ** | 0.014 | 0.499 ** | 0.311 ** | 0.513 ** | - | |||
| 9. CoSS AS | 19.14 (10.23) | 0.210 ** | −0.248 ** | 0.130 ** | 0.104 ** | 0.595 ** | 0.238 ** | 0.658 ** | 0.530 ** | - | ||
| 10. CoSS WD | 15.45 (9.53) | 0.232 ** | −0.187 ** | 0.085 ** | 0.078 * | 0.602 ** | 0.310 ** | 0.649 ** | 0.651 ** | 0.736 ** | - | |
| 11. CoSS AV | 16.78 (7.16) | 0.053 | −0.201 ** | 0.034 | 0.050 | 0.273 ** | 0.281 ** | 0.351 ** | 0.509 ** | 0.413 ** | 0.436 ** | - |
| 12. K10 | 21.51 (7.43) | 0.140 ** | −0.159 ** | 0.065 * | 0.073 * | 0.555 ** | 0.304 ** | 0.641 ** | 0.404 ** | 0.545 ** | 0.529 ** | 0.217 ** |
| Effects | β | SE | 95% CI |
|---|---|---|---|
| Attachment anxiety | |||
| Total indirect effect | 0.336 ** | 0.025 | [0.289, 0.379] |
| Specific indirect effects | |||
| ASQ ANX→ESS→K10 | 0.226 ** | 0.023 | [0.182, 0.263] |
| ASQ ANX→CoSS AO→K10 | 0.004 | 0.008 | [−0.011, 0.019] |
| ASQ ANX→CoSS AS→K10 | 0.044 * | 0.013 | [0.020, 0.066] |
| ASQ ANX→CoSS WD→K10 | 0.020 | 0.012 | [−0.004, 0.040] |
| ASQ ANX→CoSS AV→K10 | −0.002 | 0.004 | [−0.011, 0.003] |
| Serial indirect effects | |||
| ASQ ANX→ESS→CoSS AO→K10 | 0.003 | 0.006 | [−0.008, 0.013] |
| ASQ ANX→ESS→CoSS AS→K10 | 0.039 ** | 0.011 | [0.019, 0.058] |
| ASQ ANX→ESS→CoSS WD→K10 | 0.017 | 0.011 | [−0.003, 0.035] |
| ASQ ANX→ESS→CoSS AV→K10 | −0.014 * | 0.005 | [−0.025, −0.007] |
| Attachment avoidance | |||
| Total indirect effect | 0.025 | 0.014 | [−0.003, 0.053] |
| Specific indirect effects | |||
| ASQ AVD→ESS→K10 | 0.030 * | 0.011 | [0.011, 0.052] |
| ASQ AVD→CoSS AO→K10 | 0.002 | 0.004 | [−0.006, 0.011] |
| ASQ AVD→CoSS AS→K10 | −0.001 | 0.004 | [−0.009, 0.006] |
| ASQ AVD→CoSS WD→K10 | 0.005 | 0.004 | [0.000, 0.015] |
| ASQ AVD→CoSS AV→K10 | −0.017 * | 0.006 | [−0.031, −0.007] |
| Serial indirect effects | |||
| ASQ AVD→ESS→CoSS AO→K10 | 0.000 | 0.001 | [−0.001, 0.002] |
| ASQ AVD→ESS→CoSS AS→K10 | 0.005 * | 0.002 | [0.002, 0.011] |
| ASQ AVD→ESS→CoSS WD→K10 | 0.002 | 0.002 | [0.000, 0.007] |
| ASQ AVD→ESS→CoSS AV→K10 | −0.002 * | 0.001 | [−0.004, −0.001] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Remondi, C.; Casu, G.; Pozzi, C.; Greco, F.; Gremigni, P.; Brugnera, A. A Serial Mediation Model of Insecure Attachment and Psychological Distress: The Role of Dispositional Shame and Shame-Coping Styles. Int. J. Environ. Res. Public Health 2023, 20, 3193. https://doi.org/10.3390/ijerph20043193
Remondi C, Casu G, Pozzi C, Greco F, Gremigni P, Brugnera A. A Serial Mediation Model of Insecure Attachment and Psychological Distress: The Role of Dispositional Shame and Shame-Coping Styles. International Journal of Environmental Research and Public Health. 2023; 20(4):3193. https://doi.org/10.3390/ijerph20043193
Chicago/Turabian StyleRemondi, Chiara, Giulia Casu, Camilla Pozzi, Francesco Greco, Paola Gremigni, and Agostino Brugnera. 2023. "A Serial Mediation Model of Insecure Attachment and Psychological Distress: The Role of Dispositional Shame and Shame-Coping Styles" International Journal of Environmental Research and Public Health 20, no. 4: 3193. https://doi.org/10.3390/ijerph20043193
APA StyleRemondi, C., Casu, G., Pozzi, C., Greco, F., Gremigni, P., & Brugnera, A. (2023). A Serial Mediation Model of Insecure Attachment and Psychological Distress: The Role of Dispositional Shame and Shame-Coping Styles. International Journal of Environmental Research and Public Health, 20(4), 3193. https://doi.org/10.3390/ijerph20043193