

Dental Malocclusion in Mixed Dentition Children and Its Relation to Podal System and Gait Parameters


 , and
, and
Abstract
:1. Introduction
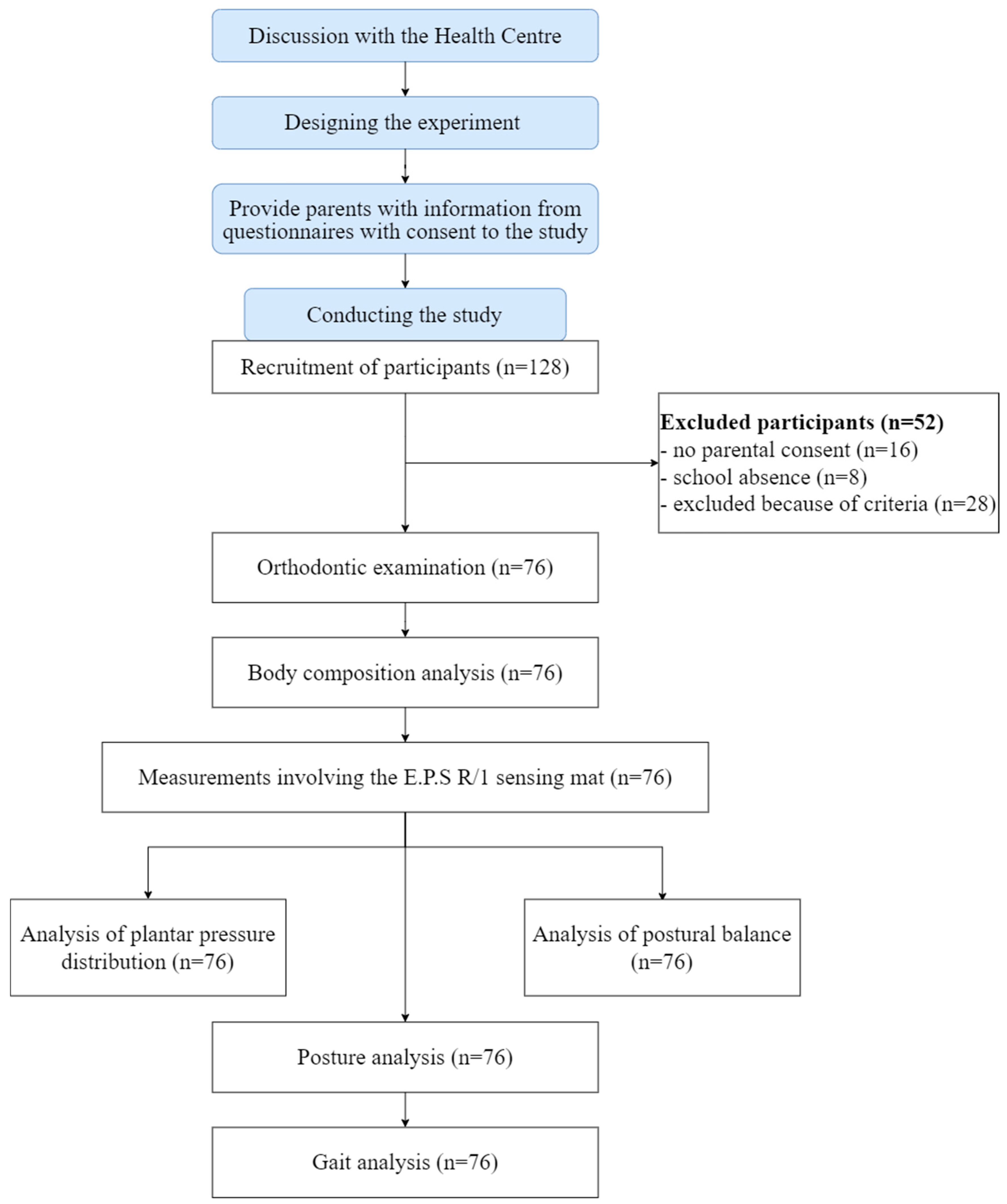
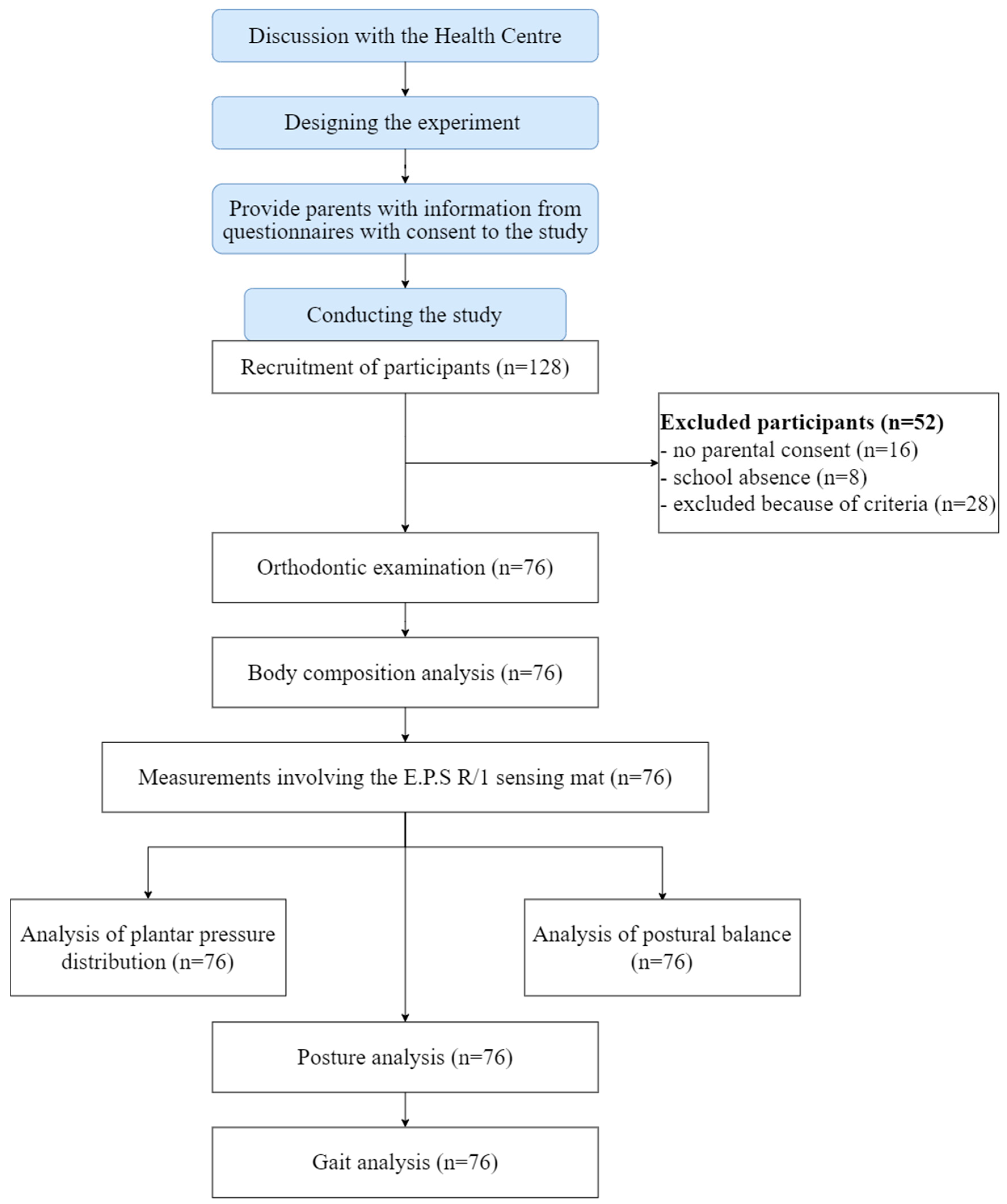
2. Materials and Methods
- Class I—normal molar occlusion; the mesiobuccal cusp of the maxillary first molar aligns with the mesiobuccal groove of the mandibular first molar. The mesial incline of the maxillary canine occludes with the distal incline of the mandibular canine. The distal incline of the maxillary canine occludes with the mesial incline of the mandibular first premolar.
- Class II—distoocclusion; the mesiobuccal groove of the mandibular first molar is DISTALLY (posteriorly) positioned when in occlusion with the mesiobuccal cusp of the maxillary first molar. The mesial incline of the maxillary canine occludes ANTERIORLY with the distal incline of the mandibular canine. The distal surface of the mandibular canine is POSTERIOR to the mesial surface of the maxillary canine by at least the width of a premolar.
- Class III—mesiooclusion; the mesiobuccal cusp of the maxillary first permanent molar occludes DISTALLY (posteriorly) to the mesiobuccal groove of the mandibular first molar. Distal surface of the mandibular canines is mesial to the mesial surface of the maxillary canines by at least the width of a premolar. Mandibular incisors are in complete crossbite. Moreover, the following malocclusion features were observed: cross bites, lingual occlusion, and deep and open bites. The study data were collected by direct observation of the oral cavity [22].
2.1. Instruments
2.2. Procedure
2.3. Measurement Protocol
2.4. Statistical Analysis
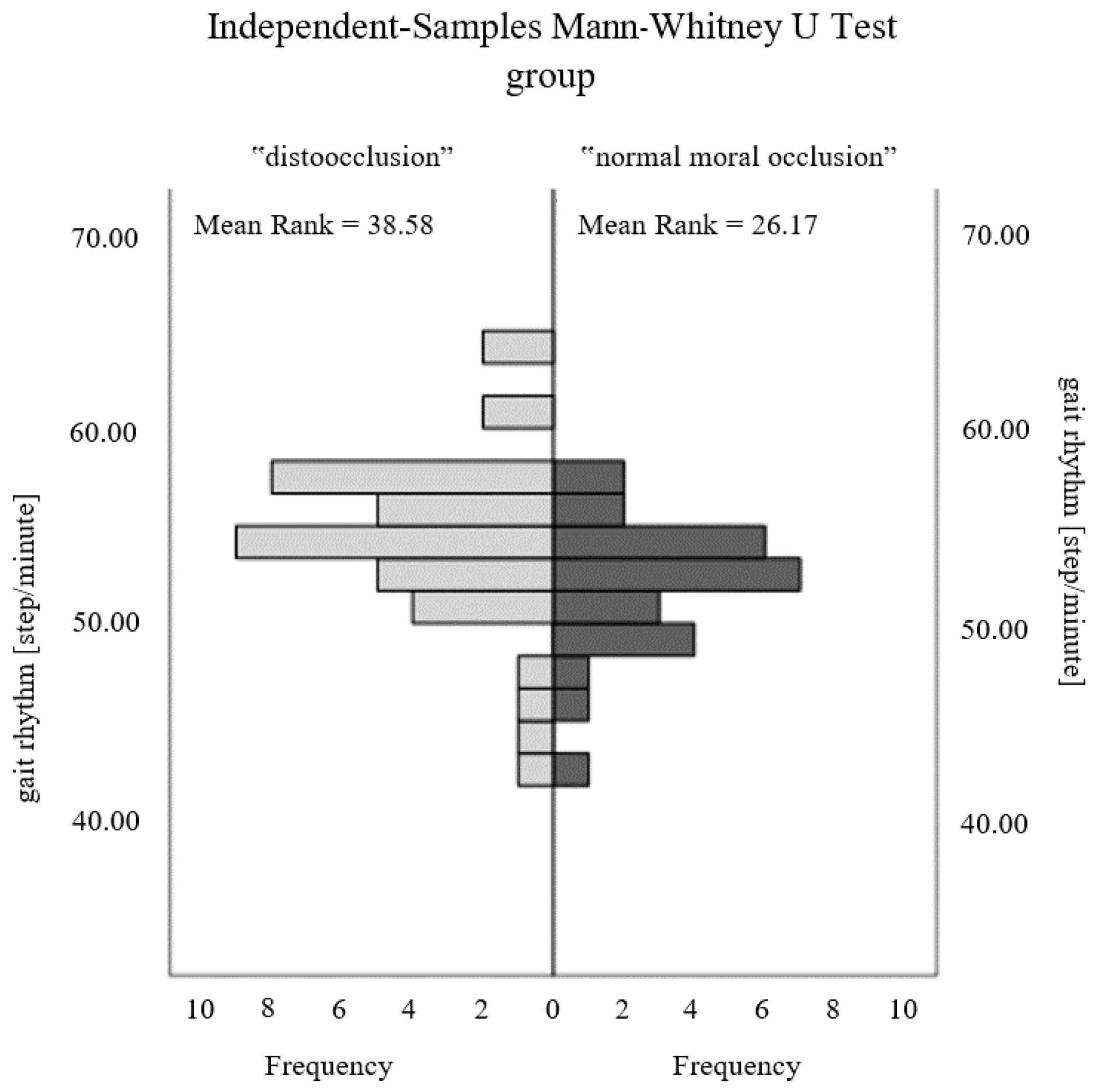
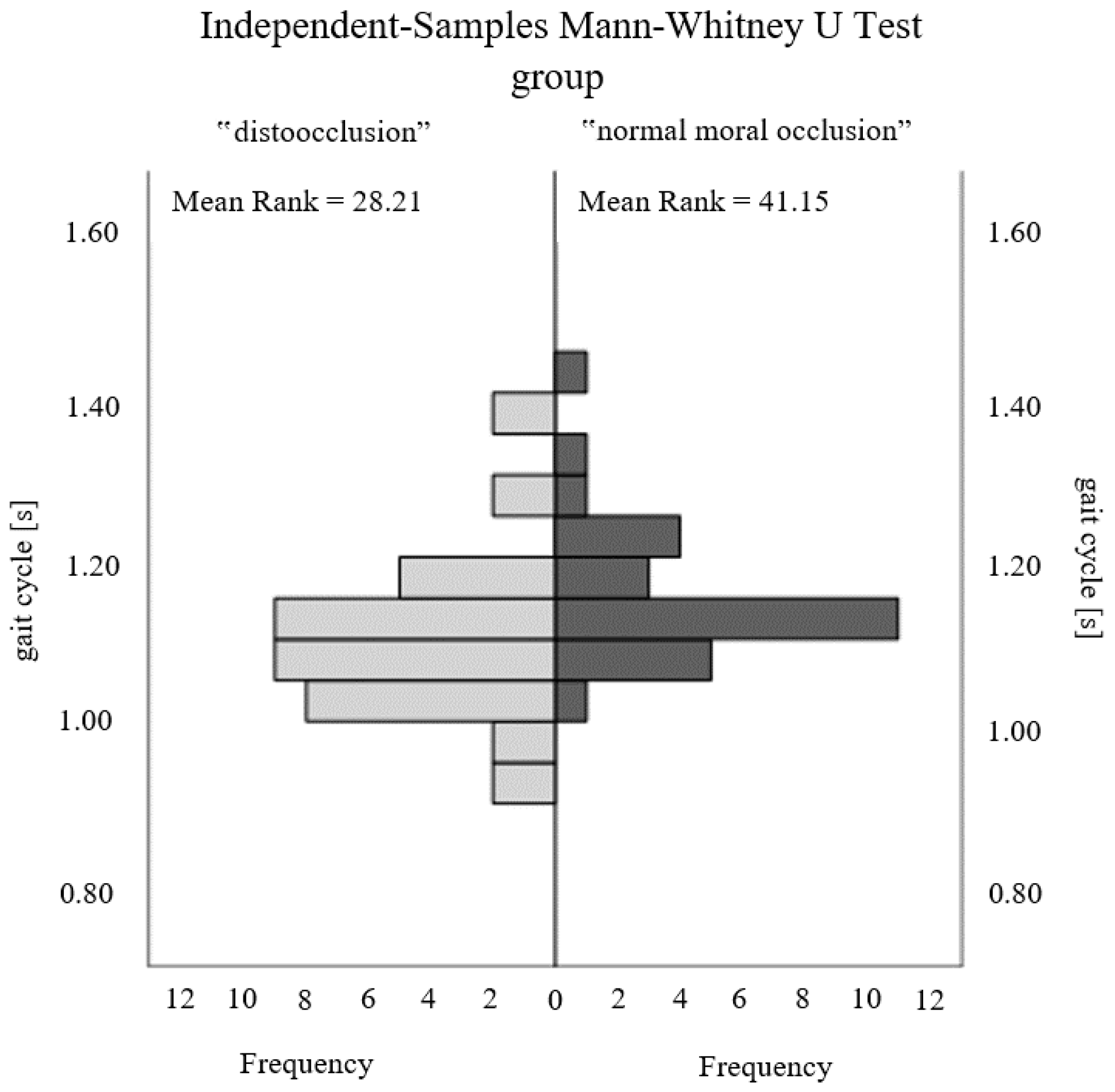
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rocabado, M.; Johnston, B.; Blakney, M.G. Physical therapy and dentistry: An overview. J. Craniomandibular. Pract. 1982, 1, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Stancker, T.G.; Silva, A.C.O.; Neto, H.P.; Rodrigues, C.D.A. Malocclusion influence on balance and posture: A systematic review. Man. Ther. Posturol. Rehabil. J. 2015, 1–6. [Google Scholar] [CrossRef]
- Michelotti, A.; Buonocore, G.; Manzo, P.; Pellegrino, G.; Farella, M. Dental occlusion and posture: An overview. Prog. Orthod 2011, 12, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Álvarez Solano, C.; González Camacho, L.A.; Castaño Duque, S.P.; Cortés Velosa, T.; Vanoy Martin, J.A.; Chambrone, L. To evaluate whether there is a relationship between occlusion and body posture as delineated by a stabilometric platform: A systematic review. Cranio 2020, 1–12. [Google Scholar] [CrossRef]
- Pacella, E.; Dari, M.; Giovannoni, D.; Mezio, M.; Caterini, L.; Costantini, A.; Carreri, C. The relationship between occlusion and posture: A systematic review. Webmedcentral Orthod. 2017, 8, WMC005374. [Google Scholar]
- Ben-Bassat, Y.; Yitschaky, M.; Kaplan, L.; Brin, I. Occlusal patterns in patients with idiopathic scoliosis. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 629–633. [Google Scholar] [CrossRef] [PubMed]
- Segatto, E.; Lippold, C.; Végh, A. Craniofacial features of children with spinal deformities. BMC Musculoskelet. Disord 2008, 9, 169. [Google Scholar] [CrossRef] [PubMed]
- Harila, V.; Valkama, M.; Sato, K.; Tolleson, S.; Hanis, S.; Kau Ch, H.; Pirttiniemi, P. Occlusal asymmetries in children with congenital hip dislocation. Eur. J. Orthod 2012, 34, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Nowak, M. Wady zgryzu a zaburzenia stabilności posturalnej i wybranych parametrów chodu u dorosłych. Doctoral Dissertation, Wydział Rehabilitacji Ruchowej, Akademia Wychowania Fizycznego im. Bronisława Czecha w Krakowie, Kraków, Poland, 2022. [Google Scholar]
- Levinkind, M. Consideration of whole body posture in relation to dental development and treatment of malocclusion in children. BDA J. 2008, 1–6. [Google Scholar]
- Perinetti, G.; Contardo, L.; Silvestrini-Biavati, A.; Perdoni, L.; Castaldo, I.A. Dental Malocclusion and Body Posture in Young Subjects: A Multiple Regression Study. Clinics 2010, 65, 689–695. [Google Scholar] [CrossRef]
- Labajo-Manzanares, M.T.; Marchena-Rodríguez, A.; Moreno-Morales, N.; Ramírez-Parga, E.; Luque-Suárez, A.; Gijon-Nogueron, G. Relationship between foot posture and dental malocclusions in children aged 6 to 9 years. A cross-sectional study. Medicine 2018, 97, 17. [Google Scholar] [CrossRef]
- Perinetti, G. Dental occlusion and body posture: No detectable correlation. Gait. Posture 2006, 24, 165–168. [Google Scholar] [CrossRef] [PubMed]
- Sambataro, S.; Bocchieri, S.; Cervino, G.; La Bruna, R.; Cicciù, A.; Innorta, M.; Torrisi, B.; Cicciù, M. Correlations between Malocclusion and Postural Anomalies in Children with Mixed Dentition. J. Funct. Morphol. Kinesiol. 2019, 4, 45. [Google Scholar] [CrossRef] [PubMed]
- Paya-Argoud, M.; Tardieu, C.; Cheynet, F.; Raskin, A.; Borel, L. Impact of orthognathic surgery on the body posture. Gait. Posture 2019, 67, 25–30. [Google Scholar] [CrossRef]
- Pérez-Belloso, A.J.; Coheña-Jiménez, M.; Cabrera-Domínguez, M.E.; Galan-González, A.F.; Domínguez-Reyes, A.; Pabón-Carrasco, M. Influence of Dental Malocclusion on Body Posture and Foot Posture in Children: A Cross-Sectional Study. Healthcare 2020, 8, 485. [Google Scholar] [CrossRef]
- Tardieu, C.; Dumitrescu, M.; Giraudeau, A.; Blanc, J.C.; Cheynet, F.; Borel, L. Dental occlusion and postural control in adults. Neurosci. Lett. 2009, 450, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Odzimek, M.; Maj-Gnat, K. Disorders of the statics of the body and the temporomandibular joint. J. Educ. Health Sport 2021, 11, 369–380. [Google Scholar] [CrossRef]
- de Souza Silva, H.C.; da Silva, D.F.; Foggato, A.A.; Coléte, J.Z.; Jassi, F.J.; Toledo Neto, J.L. Analysis of the interrelationship between tmd and posture using rdc, electromyography and postural assessment. Braz. J. Dev. 2021, 7, 20169–20179. [Google Scholar] [CrossRef]
- Julià-Sánchez, S.; Álvarez-Herms, J.; Cirer-Sastre, R.; Corbi, F.; Burtscher, M. The Influence of Dental Occlusion on Dynamic Balance and Muscular Tone. Front. Physiol. 2019, 10, 1626. [Google Scholar] [CrossRef]
- Bricot, B. Posturologia, 2nd ed.; Icone: Sao Paulo, Brazil, 2001; pp. 151–162. [Google Scholar]
- Karłowska, I. Klasyfikacja Angle’a. In Zarys Współczesnej Ortodoncji. Podręcznik dla Studentów i Lekarzy Dentystów; Karłowska, I., Ed.; Warszawa, 4; PZWL Wydawnictwo Lekarskie: Warszawa, Poland, 2022; pp. 159–162. [Google Scholar]
- Lombardo, G.; Vena, F.; Negr, P.; Pagano, S.; Barilotti, C.; Paglia, L.; Colombo, S.; Orso, M.; Cianetti, S. Worldwide prevalance of malocclusion in the different stages of dentition: A systematic review and meta-analysis. Eur. J. Paediatr. Dent. 2020, 21, 115–122. [Google Scholar] [CrossRef]
- Hegazy, F.; Aboelnasr, E.; Abuzaid, M.; Kim, I.J.; Salem, Y. Comparing validity and diagnostic accuracy of clarke’s angle and foot posture index-6 to determine flexible flatfoot in adolescents: A cross-sectional investigation. J. Multidiscip. Healthc. 2021, 14, 2705–2717. [Google Scholar] [CrossRef]
- Laskowska, M.; Olczak-Kowalczyk, D.; Zadurska, M.; Czubak, J.; Czubak-Wrzosek, M.; Walerzak, M.; Tyrakowski, M. Evaluation of a relationship between malocclusion and idiopathic scoliosis in children and adolescents. J. Child Orthop. 2019, 13, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Domínguez, M.E.; Domínguez-Reyes, A.; Pabón-Carrasco, M.; Pérez-Belloso, A.J.; Coheña-Jiménez, M.; Galán-González, A.F. Dental Malocclusion and its relation to the podal system. Front. Pediatr. 2021, 9, 654229. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, M.; Hayakawa, I.; Hirano, S.; Watanabe, I. Changes in gait stability induced by alteration of mandibular position. J. Med. Dent. Sci. 2001, 48, 131–136. [Google Scholar] [CrossRef]
- Bardellini, E.; Gulino, M.G.; Fontana, S.; Amadori, F.; Febbrari, M.; Majorana, A. Can the Treatment of Dental Malocclusions Affect the Posture in Children? J. Clin. Pediatr. Dent. 2022, 46, 241–248. [Google Scholar] [CrossRef]
- Jaszczur-Nowicki, J.; Bukowska, J.M.; Kruczkowski, D.; Pieniążek, M.; Mańko, G.; Spieszny, M. Distribution of feet pressure on ground and maintaining body balance among 8–10-year-old children with and without external load application. Acta Bioeng. Biomech. 2020, 22, 22. [Google Scholar] [CrossRef]
- Bukowska, J.M.; Jekiełek, M.; Kruczkowski, D.; Ambroży, T.; Rydzik, Ł.; Spieszny, M.; Jaszczur-Nowicki, J. Podiatric and stabilographic examinations of the effects of school bag carrying in children aged 11 to 15 years. Appl. Sci. 2021, 11, 9357. [Google Scholar] [CrossRef]
- Bukowska, J.; Jekiełek, M.; Kruczkowski, D.; Ambroży, T.; Jaszczur-Nowicki, J. Biomechanical Aspects of the Foot Arch, Body Balance and Body Weight Composition of Boys Training Football. Int. J. Environ. Res. Public Health 2021, 18, 5017. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Parameters | Rhythm [Steps/min] | Duration of Gait Cycle [s] | Support Duration [% Gait Cycle] | Swing Duration [% Gait Cycle] | Double Support Time [% Gait Cycle] | Single Support Time [% Gait Cycle] | Left Step Length [(%] | Right Step Length [%] | Left Step Duration [%] | Right Step Duration [%] | Left Support Duration [% Gait Cycle] | Right Support Duration [% Gait Cycle] | Left Swing Duration [% Gait Cycle] | Right Swing Duration [% Gait Cycle] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | 53.50 | 1.12 | 60.80 | 37.20 | 11.75 | 37.20 | 50.45 | 49.55 | 50.05 | 50.05 | 60.80 | 60.90 | 37.85 | 37.15 |
| Q1 | 50.53 | 1.07 | 59.53 | 36.05 | 10.70 | 36.05 | 48.05 | 48.00 | 49.20 | 49.20 | 59.10 | 59.63 | 36.33 | 35.43 |
| Q3 | 55.98 | 1.19 | 61.95 | 38.40 | 12.78 | 38.40 | 52.00 | 51.95 | 50.80 | 50.88 | 61.70 | 62.18 | 39.08 | 38.35 |
| Parameters | Podology | Stabilographic | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Left Foot Load [%] | Right Foot Load [%] | Left Foot | Right Foot | The Total Surface Area of the Body’s Center of Gravity [mm2] | |||||
| Forefoot [%] | Metatarsus [%] | Heel [%] | Forefoot [%] | Metatarsus [%] | Heel [%] | ||||
| M | 53.65 | 46.90 | 42.95 | 8.95 | 45.30 | 46.40 | 8.30 | 38.95 | 111.74 |
| Q1 | 48.38 | 41.93 | 35.35 | 0.38 | 37.25 | 34.80 | 2.00 | 32.50 | 34.61 |
| Q3 | 58.25 | 52.08 | 50.38 | 20.70 | 51.88 | 57.55 | 20.10 | 53.70 | 190.61 |
| Parameter | Z | p |
|---|---|---|
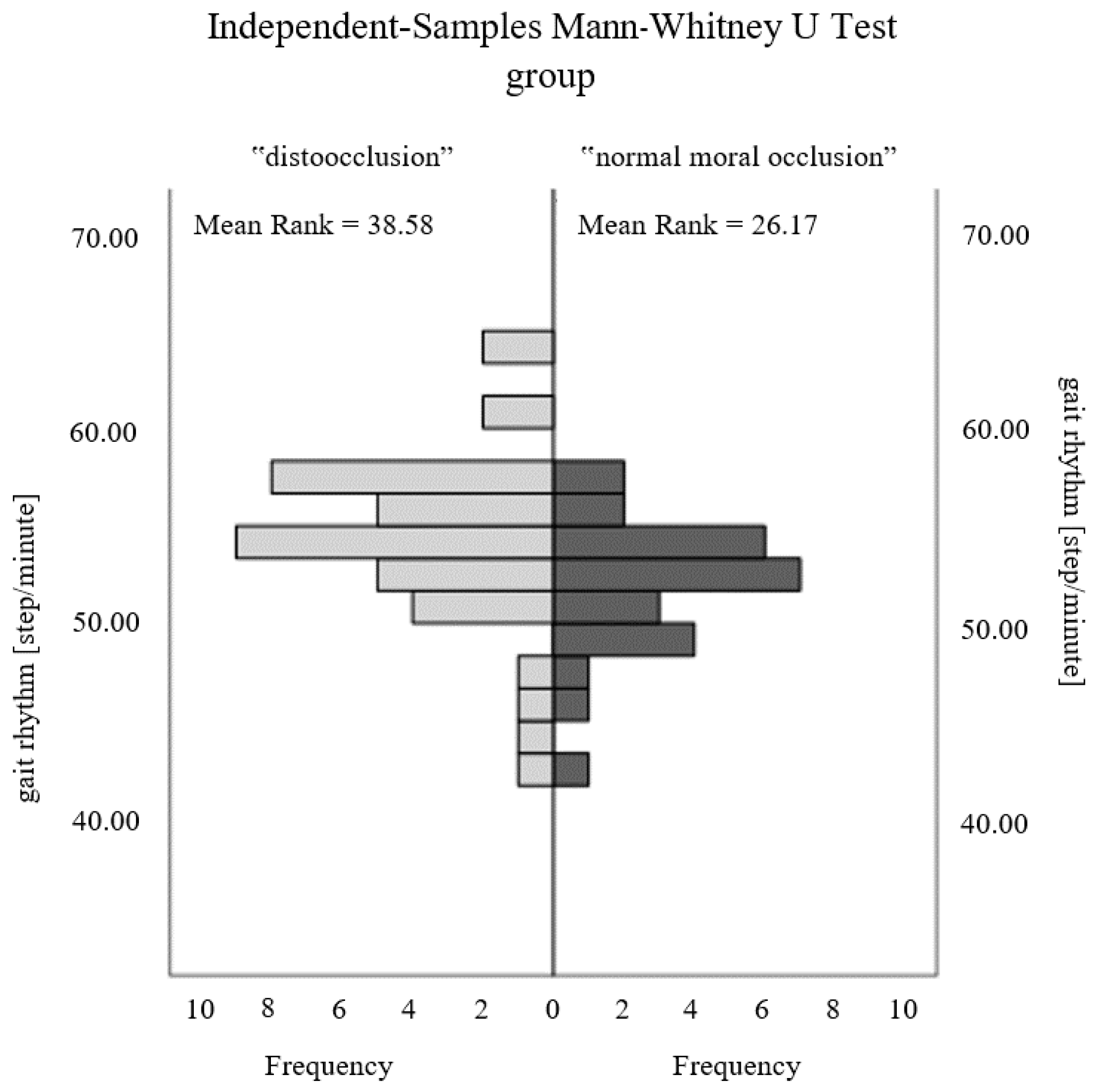
| Rhythm [steps/min] | 2.576 | 0.010 * |
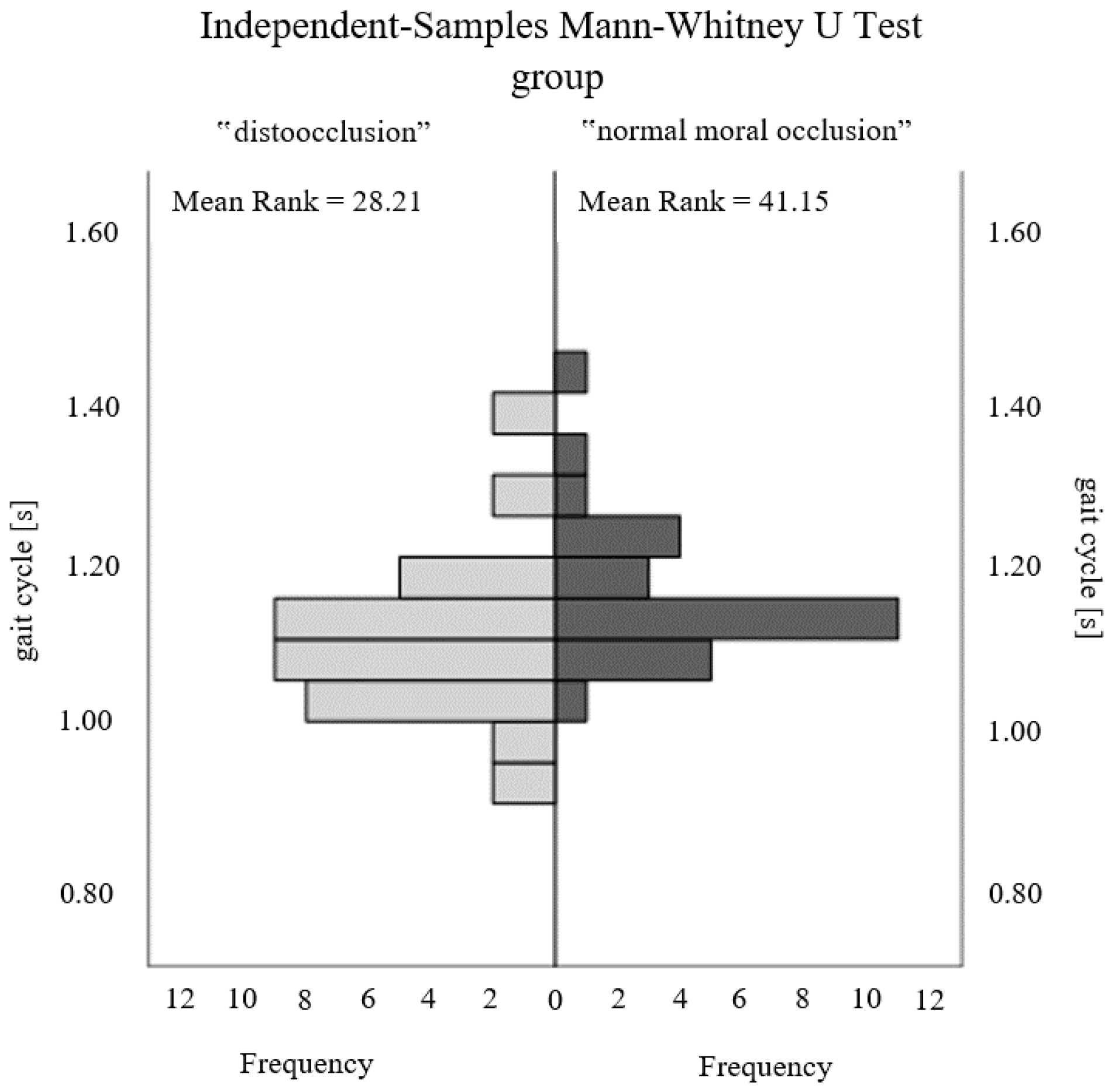
| Duration of gait cycle [s] | −2.687 | 0.007 * |
| Support duration [% gait cycle] | 0.685 | 0.494 |
| Swing duration [% gait cycle] | −1.435 | 0.151 |
| Double support time [% gait cycle] | 1.285 | 0.199 |
| Single support time [% gait cycle] | −1.532 | 0.125 |
| Left step length [%] | 1.487 | 0.137 |
| Right step length [%] | −1.467 | 0.142 |
| Left step duration: [%] | 1.806 | 0.071 |
| Right step duration: [%] | −2.217 | 0.027 * |
| Left support duration [% gait cycle] | 1.226 | 0.220 |
| Right support duration [% gait cycle] | 0.078 | 0.938 |
| Left swing duration [% gait cycle] | −1.311 | 0.190 |
| Right swing duration [% gait cycle] | −1.239 | 0.215 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Różańska-Perlińska, D.; Jaszczur-Nowicki, J.; Kruczkowski, D.; Bukowska, J.M. Dental Malocclusion in Mixed Dentition Children and Its Relation to Podal System and Gait Parameters. Int. J. Environ. Res. Public Health 2023, 20, 2716. https://doi.org/10.3390/ijerph20032716
Różańska-Perlińska D, Jaszczur-Nowicki J, Kruczkowski D, Bukowska JM. Dental Malocclusion in Mixed Dentition Children and Its Relation to Podal System and Gait Parameters. International Journal of Environmental Research and Public Health. 2023; 20(3):2716. https://doi.org/10.3390/ijerph20032716
Chicago/Turabian StyleRóżańska-Perlińska, Dorota, Jarosław Jaszczur-Nowicki, Dariusz Kruczkowski, and Joanna Magdalena Bukowska. 2023. "Dental Malocclusion in Mixed Dentition Children and Its Relation to Podal System and Gait Parameters" International Journal of Environmental Research and Public Health 20, no. 3: 2716. https://doi.org/10.3390/ijerph20032716
APA StyleRóżańska-Perlińska, D., Jaszczur-Nowicki, J., Kruczkowski, D., & Bukowska, J. M. (2023). Dental Malocclusion in Mixed Dentition Children and Its Relation to Podal System and Gait Parameters. International Journal of Environmental Research and Public Health, 20(3), 2716. https://doi.org/10.3390/ijerph20032716