
Association of Lung Fibrotic Changes and Cardiological Dysfunction with Comorbidities in Long COVID-19 Cohort

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
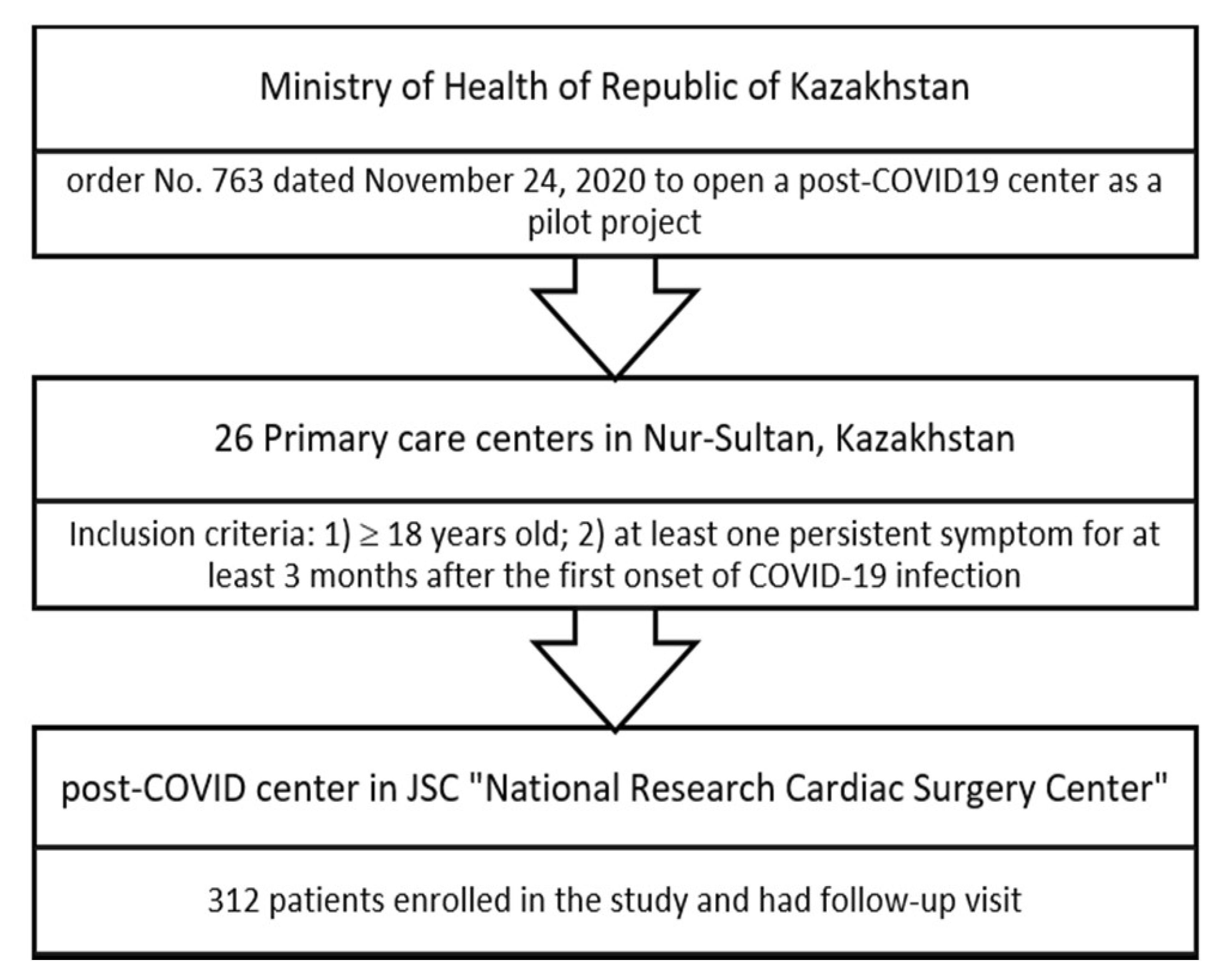
2.1. Study Design and Participants
2.2. Clinical Assessment
2.3. Statistical Analysis
3. Results
3.1. Cohort Description
3.2. Clinical Manifestations at the Follow-Up
3.3. Lung Function Screening
3.4. Cardiac Screening
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Furukawa, N.W.; Brooks, J.T.; Sobel, J. Evidence supporting transmission of severe acute respiratory syndrome coronavirus 2 while pre-symptomatic or asymptomatic. Emerg. Infect. Dis. 2020, 26, e201595. [Google Scholar] [CrossRef] [PubMed]
- Rivett, L.; Sridhar, S.; Sparkes, D.; Routledge, M.; Jones, N.; Forrest, S.; Young, J.; Pereira-Dias, J.; Hamilton, W.; Ferris, M.; et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. eLife 2020, 9, e58728. [Google Scholar] [CrossRef] [PubMed]
- Buitrago-Garcia, D.; Egli-Gany, D.; Counotte, M.; Hossmann, S.; Imeri, H.; Ipekci, A.; Salanti, G.; Low, N. Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: A living systematic review and meta-analysis. PLoS Med. 2020, 17, e1003346. [Google Scholar] [CrossRef] [PubMed]
- Clerkin, K.J.; Fried, J.A.; Raikhelkar, J.; Sayer, G.; Griffin, J.M.; Masoumi, A.; Jain, S.S.; Burkhoff, D.; Kumaraiah, D.; Rabbani, L.; et al. COVID-19 and cardiovascular disease. Circulation 2020, 141, 1648–1655. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Laukkanen, J.A. Cardiovascular complications in COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, e139–e141. [Google Scholar] [CrossRef] [PubMed]
- Polverino, F.; Stern, D.A.; Ruocco, G.; Balestro, E.; Bassetti, M.; Candelli, M.; Cirillo, B.; Contoli, M.; Corsico, A.; D’Amico, F.; et al. Comorbidities, cardiovascular therapies, and COVID-19 mortality: A nationwide, Italian observational study (ItaliCO). Front. Cardiovasc. Med. 2020, 7, 585866. [Google Scholar] [CrossRef]
- Hiroi, Y.; Ohtsu, H.; Uemura, Y.; Hayakawa, K.; Asai, Y.; Kutsuna, S.; Terada, M.; Sugiura, W.; Ohmagari, N. Cardiovascular complications of hospitalized patients with coronavirus disease 2019 in a Japanese registry in 2020. Circ. J. 2022, 86, 464–471. [Google Scholar] [CrossRef]
- Leth, S.; Gunst, J.D.; Mathiasen, V.; Hansen, K.; Søgaard, O.; Østergaard, L.; Jensen-Fangel, S.; Storgaard, M.; Agergaard, J. Persistent symptoms in patients recovering from COVID-19 in Denmark. Open Forum Infect. Dis. 2021, 8, ofab042. [Google Scholar] [CrossRef]
- Renda, G.; Ricci, F.; Spinoni, E.G.; Grisafi, L.; D’ardes, D.; Mennuni, M.; Tana, C.; Rognoni, A.; Bellan, M.; Sainaghi, P.P.; et al. Predictors of mortality and cardiovascular outcome at 6 months after hospitalization for COVID-19. J. Clin. Med. 2022, 11, 729. [Google Scholar] [CrossRef]
- Sigfrid, L.; Drake, T.M.; Pauley, E.; Jesudason, E.C.; Olliaro, P.; Lim, W.S.; Gillesen, A.; Berry, C.; Lowe, D.J.; McPeake, J. Long Covid in adults discharged from UK Hospitals after Covid-19: A prospective, multicentre cohort study using the ISARIC WHO clinical characterisation protocol. Lancet Reg. Health Eur. 2021, 8, 100186. [Google Scholar] [CrossRef]
- Buonsenso, D.; Munblit, D.; Pazukhina, E.; Ricchiuto, A.; Sinatti, D.; Zona, M.; De Matteis, A.; D’Ilario, F.; Gentili, C.; Lanni, R.; et al. Post-COVID condition in adults and children living in the same household in Italy: A prospective cohort study using the ISARIC global follow-up protocol. Front. Pediatr. 2022, 10, 834875. [Google Scholar] [CrossRef] [PubMed]
- Haunhorst, S.; Bloch, W.; Wagner, H.; Ellert, C.; Krueger, K.; Vilser, D.C.; Finke, K.; Reuken, P.; Pletz, M.W.; Stallmach, A.; et al. Long COVID: A narrative review of the clinical aftermaths of COVID-19 with a focus on a putative pathophysiology and aspects of physical activity. Oxford Open Immunol. 2022, 3, iqac006. [Google Scholar] [CrossRef]
- Tang, Y.; Liu, J.; Zhang, D.; Xu, Z.; Ji, J.; Wen, C. Cytokine storm in COVID-19: The current evidence and treatment strategies. Front. Immunol. 2020, 11, 1708. [Google Scholar] [CrossRef]
- Young, S.J. Long-COVID or post-COVID-19 syndrome: Putative pathophysiology, risk factors and treatments. Infect. Dis. 2021, 53, 737–754. [Google Scholar] [CrossRef]
- Michelen, M.; Manoharan, L.; Elkheir, N.; Cheng, V.; Dagens, A.; Hastie, C.; O’Hara, M.; Suett, J.; Dahmash, D.; Bugaeva, P.; et al. Characterising Long COVID: A living systematic review. BMJ Glob. Health 2021, 6, e005427. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-Acute COVID-19 Syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Hajjaji, N.; Lepoutre, K.; Lakhdar, S.; Bécourt, S.; Bellier, C.; Kaczmarek, E.; Broyelle, A.; Giscard, S.; Lartigau, E. 16 Months follow up of patients’ behavior and mild COVID-19 patterns in a large cohort of cancer patients during the pandemic. Front. Oncol. 2022, 12, 901426. [Google Scholar] [CrossRef] [PubMed]
- Carfi, A.; Bernabei, R.; Landi, F.; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent symptoms in patients after acute COVID-19. JAMA 2020, 324, 603–605. [Google Scholar] [CrossRef]
- Michelen, M.; Cheng, V.; Manoharan, L.; Elkheir, N.; Dagens, D.; Hastie, C.; O’Hara, M.; Suett, J.C.; Dahmash, D.; Bugaeva, P.; et al. What are the long-term symptoms and complications of COVID-19: A protocol for a living systematic review. F1000 Res. 2020, 9, 1455. [Google Scholar] [CrossRef]
- Cares-Marambio, K.; Montenegro-Jimenez, Y.; Torres-Castro, R.; Vera-Uribe, R.; Torralba, R.; Alsina-Restoy, X.; Vasconcello-Castillo, L.; Vilaró, J. Prevalence of potential respiratory symptoms in survivors of hospital admission after coronavirus disease 2019 (COVID-19): A systematic review and meta-analysis. Chron. Respir. Dis. 2021, 18, 14799731211002240. [Google Scholar] [CrossRef]
- Shah, W.; Hillman, T.; Playford, E.D.; Hishmech, L. Managing the long-term effects of Covid-19: Summary of NICE, SIGN, and RCGP rapid guideline. BMJ 2021, 372, n136. [Google Scholar] [CrossRef] [PubMed]
- Davido, B.; Seang, S.; Tubiana, R.; de Truchis, P. Post–COVID-19 chronic symptoms: A postinfectious entity? Clin. Microbiol. Infect. 2020, 26, 1448–1449. [Google Scholar] [CrossRef] [PubMed]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Post-discharge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2020, 93, 1013–1022. [Google Scholar] [CrossRef]
- Singh, A.K.; Singh, R. Hyperglycemia without diabetes and new-onset diabetes are both associated with poorer outcomes in COVID-19. Diabetes Res. Clin. Pract. 2020, 167, 108382. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Arora, A.; Sharma, P.; Anikhindi, S.; Bansal, N.; Singla, V.; Khare, S.; Srivastava, A. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Pranata, R.; Lim, M.A.; Huang, I.; Raharjo, S.B.; Lukito, A.A. Hypertension is associated with increased mortality and severity of disease in COVID-19 pneumonia: A systematic review, meta-analysis and meta-regression. J. Renin-Angiotensin Aldosterone Syst. 2020, 21, 1470320320926899. [Google Scholar] [CrossRef]
- de Almeida-Pititto, B.; Dualib, P.M.; Zajdenverg, L.; Dantas, J.R.; De Souza, F.D.; Rodacki, M.; Bertoluci, M.C.; Brazilian Diabetes Society Study Group (SBD). Severity and mortality of COVID 19 in patients with diabetes, hypertension and cardiovascular disease: A meta-analysis. Diabetol. Metab. Syndr. 2020, 12, 75. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; Hu, B.; Zhang, Y.; Wang, H.; Zhou, X.; Hu, W.; Cheng, Y.; Yan, J.; Ping, H.; Zhou, Q. Suspected myocardial injury in patients with COVID-19: Evidence from front-line clinical observation in Wuhan, China. Int. J. Cardiol. 2020, 311, 116–121. [Google Scholar] [CrossRef]
- Han, H.; Xie, L.; Liu, R.; Yang, J.; Liu, F.; Wu, K.; Chen, L.; Hou, W.; Feng, Y.; Zhu, C. Analysis of heart injury laboratory parameters in 273 COVID-19 patients in one hospital in Wuhan, China. J. Med. Virol. 2020, 92, 819–823. [Google Scholar] [CrossRef]
- Fortini, A.; Torrigiani, A.; Sbaragli, S.; LoForte, A.; Crociani, A.; Cecchini, P.; Bruni, G.I.; Faraone, A. COVID-19: Persistence of symptoms and lung alterations after 3-6 months from hospital discharge. Infection 2021, 49, 1007–1015. [Google Scholar] [CrossRef]
- Fumagalli, A.; Misuraca, C.; Bianchi, A.; Borsa, N.; Limonta, S.; Maggiolini, S.; Bonardi, D.R.; Corsonello, A.; Di Rosa, M.; Soraci, L.; et al. Long-term changes in pulmonary function among patients surviving to COVID-19 pneumonia. Infection 2022, 50, 1019–1022. [Google Scholar] [CrossRef] [PubMed]
- Wu, Q.; Zhong, L.; Li, H.; Guo, J.; Li, Y.; Hou, X.; Yang, F.; Xie, Y.; Li, L.; Xing, Z. A follow-up study of lung function and chest computed tomography at 6 months after discharge in patients with coronavirus disease 2019. Can. Respir. J. 2021, 2021, 6692409. [Google Scholar] [CrossRef] [PubMed]
- Navarro, A.O.; Cervantes-Bojalil, J.; Quevedo, O.D.J.C.; Martínez, A.A.; Hernández-Jiménez, C.A.; Álvarez, E.P.; Gil, A.G.; Amaro, A.L.P.; Lastra, O.L.V.; Luis, B.A.L. Decreased quality of life and spirometric alterations even after mild-moderate COVID-19. Respir. Med. 2021, 181, 106391. [Google Scholar] [CrossRef]
- Wang, J.Y.; Chang, S.Y.; Huang, Y.W.; Chang, S.C. Serology-positive but minimally symptomatic COVID-19 may still cause lung injury and lung function impairment. Int. J. Tuberc. Lung Dis. 2020, 24, 568–569. [Google Scholar] [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-reactive protein at sites of inflammation and infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef]
- Cavalcante-Silva, L.H.; Carvalho, D.C.; de Almeida Lima, É.; Galvao, J.G.; da Silva, J.S.; de Sales-Neto, J.M.; Rodrigues-Mascarenhas, S. Neutrophils and COVID-19: The road so far. Inter. Immunopharmacol. 2021, 90, 107233. [Google Scholar] [CrossRef]
- Caro-Codón, J.; Rey, J.R.; Buño, A.; Iniesta, A.M.; Rosillo, S.O.; Castrejon-Castrejon, S.; Rodriguez-Sotelo, L.; Martinez, L.A.; Marco, I.; Merino, C.; et al. Characterization of NT-proBNP in a large cohort of COVID-19 patients. Eur. J. Heart Fail. 2021, 23, 456–464. [Google Scholar] [CrossRef]
- Critchley, J.A.; Carey, I.M.; Harris, T.; DeWilde, S.; Hosking, F.J.; Cook, D.G. Glycemic control and risk of infections among people with type 1 or type 2 diabetes in a large primary care cohort study. Diabetes Care 2018, 4, 2127–2135. [Google Scholar] [CrossRef] [PubMed]
- Alahmad, B.; Al-Shammari, A.A.; Bennakhi, A.; Al-Mulla, F.; Ali, H. Fasting blood glucose and COVID-19 severity: Nonlinearity matters. Diabetes Care 2020, 43, 3113–3116. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef] [PubMed]
- Nasserie, T.; Hittle, M.; Goodman, S.N. Assessment of the frequency and variety of persistent symptoms among patients with COVID-19: A systematic review. JAMA Netw. Open 2021, 4, e2111417. [Google Scholar] [CrossRef]
- Nehme, M.; Braillard, O.; Alcoba, G.; Perone, S.A.; Courvoisier, D.; Chappuis, F.; Guessous, I. COVID-19 symptoms: Longitudinal evolution and persistence in outpatient settings. Ann. Intern. Med. 2021, 174, 723–725. [Google Scholar] [CrossRef]
- Holmes, G.P.; Kaplan, J.E.; Gantz, N.M.; Komaroff, A.L.; Schonberger, L.B.; Straus, S.E.; Jones, J.F.; Dubois, R.E.; Cunningham-Rundles, C.; Pahwa, S.; et al. Chronic fatigue syndrome: A working case definition. Ann. Intern. Med. 1988, 108, 387–389. [Google Scholar] [CrossRef] [PubMed]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, U.; Cameron, B.; Vernon, S.D.; Reeves, W.C.; Lloyd, A. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: Prospective cohort study. BMJ 2006, 333, 575. [Google Scholar] [CrossRef] [PubMed]
- Lerner, A.M.; Robinson, D.A.; Yang, L.; Williams, C.F.; Newman, L.M.; Breen, J.J.; Eisinger, R.W.; Schneider, J.S.; Adimora, A.A.; Erbelding, E.J. Toward understanding COVID-19 recovery: National Institutes of Health workshop on postacute COVID-19. Ann. Intern. Med. 2021, 174, 999–1003. [Google Scholar] [CrossRef] [PubMed]
- Naik, P.K.; Moore, B.B. Viral infection and aging as cofactors for the development of pulmonary fibrosis. Expert Rev. Respir. Med. 2010, 4, 759–771. [Google Scholar] [CrossRef]
- Abelmann, W.H. Virus and the heart. Circulation 1971, 44, 950–956. [Google Scholar] [CrossRef] [PubMed]
- Lechowicz, K.; Drozdzal, S.; Machaj, F.; Rosik, J.; Szostak, B.; Zegan-Barańska, M.; Biernawska, J.; Dabrowski, W.; Rotter, I.; Kotfis, K. COVID-19: The potential treatment of pulmonary fibrosis associated with SARS-CoV-2 infection. J. Clin. Med. 2020, 9, 1917. [Google Scholar] [CrossRef]
- Ali, R.M.M.; Ghonimy, M.B.I. Post-COVID-19 pneumonia lung fibrosis: A worrisome sequelae in surviving patients. Egypt. J. Radiol. Nucl. Med. 2021, 52, 101. [Google Scholar] [CrossRef]
- Bose, R.; McCarthy, J. Direct SARS-CoV-2 infection of the heart potentiates the cardiovascular sequelae of COVID-19. Drug Discov. Today 2020, 25, 1559–1560. [Google Scholar] [CrossRef]
- Nalysnyk, L.; Hernandez-Medina, M.; Krishnarajah, G. Glycaemic variability and complications in patients with diabetes mellitus: Evidence from a systematic review of the literature. Diabetes Obes. Metab. 2010, 12, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Kearney, P.M.; Whelton, M.; Reynolds, K.; Muntner, P.; Whelton, P.K.; He, J. Global burden of hypertension: Analysis of worldwide data. Lancet 2005, 365, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Forouzanfar, M.H.; Liu, P.; Roth, G.A.; Ng, M.; Biryukov, S.; Marczak, L.; Alexander, L.; Estep, K.; Abate, K.H.; Akinyemiju, T.F.; et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mm Hg, 1990–2015. JAMA 2017, 317, 165–182. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Shi, L.; Wang, Y.; Xiao, W.; Duan, G.; Yang, H. The association of hypertension with the severity and mortality of COVID-19 patients: Evidence based on adjusted effect estimates. J. Infect. 2020, 81, e44–e47. [Google Scholar] [CrossRef]
- Madhur, M.S.; Elijovich, F.; Alexander, M.R.; Pitzer, A.; Ishimwe, J.; Van Beusecum, J.P.; Patrick, D.M.; Smart, C.D.; Kleyman, T.R.; Kingery, J.; et al. Hypertension. Do inflammation and immunity hold the key to solving this epidemic? Circ. Res. 2021, 128, 908–933. [Google Scholar] [CrossRef]
- Gao, C.; Cai, Y.; Zhang, K.; Zhou, L.; Zhang, Y.; Zhang, X.; Li, Q.; Li, W.; Yang, S.; Zhao, X.; et al. Association of hypertension and antihypertensive treatment with COVID-19 mortality: A retrospective observational study. Eur. Heart J. 2020, 41, 2058–2066. [Google Scholar] [CrossRef] [PubMed]
- Sisti, N.; Valente, S.; Mandoli, G.E.; Santoro, C.; Sciaccaluga, C.; Franchi, F.; Cameli, P.; Mondillo, S.; Cameli, M. COVID-19 in patients with heart failure: The new and the old epidemic. Postgrad. Med. J. 2021, 97, 175–179. [Google Scholar] [CrossRef]
- Kell, D.B.; Pretorius, E. Serum ferritin is an important inflammatory disease marker, as it is mainly a leakage product from damaged cells. Metallomics 2014, 6, 748–773. [Google Scholar] [CrossRef]
- Davalos, D.; Akassoglou, K. Fibrinogen as a key regulator of inflammation in disease. Semin. Immunopathol. 2012, 34, 43–62. [Google Scholar] [CrossRef]
- Vilar, R.; Fish, R.J.; Casini, A.; Neerman-Arbez, M. Fibrin (ogen) in human disease: Both friend and foe. Haematologica 2020, 105, 284–296. [Google Scholar] [CrossRef] [PubMed]
- Len, P.; Iskakova, G.; Sautbayeva, Z.; Kussanova, A.; Taeukelova, A.T.; Sugralimova, M.M.; Dautbayeva, A.S.; Abdieva, M.M.; Ponomarev, E.D.; Tikhonov, A.; et al. Meta-analysis and systematic review of coagulation disbalances in COVID-19: 41 studies and 17,601 patients. Front. Cardiovasc. Med. 2022, 9, 794092. [Google Scholar] [CrossRef] [PubMed]
- Long, W.; Yang, J.; Li, Z.; Li, J.; Chen, S.; Chen, D.; Wang, S.; Li, Q.; Hu, D.; Huang, J.; et al. Abnormal fibrinogen level as a prognostic Indicator in coronavirus disease patients: A retrospective cohort study. Front. Med. 2021, 8, 687220. [Google Scholar] [CrossRef] [PubMed]
- Tartari, C.J.; Milani, G.; Salvetti, F.; Marchetti, M.; Russo, L.; Vignoli, A.; Vitali, M.; Schieppati, F.; Ravasio, G.; Castellani, L.; et al. Post-Covid-19 hemostatic characteristics of convalescent patients: The Bergamo Experience. Blood 2021, 138, 1054. [Google Scholar] [CrossRef]
- Medranda, G.A.; Fazlalizadeh, H.; Case, B.C.; Yerasi, C.; Zhang, C.; Rapaport, H.; Shea, C.; Weintraub, W.S.; Waksman, R. Implications of left ventricular function on short-term outcomes in COVID-19 patients with myocardial injury. Cardiovasc. Revasc. Med. 2021, 29, 45–49. [Google Scholar] [CrossRef]
- Zhou, M.; Wong, C.; Un, K.; Lau, Y.; Lee, J.; Tam, F.; Lau, Y.-M.; Lai, W.-H.; Tam, A.R.; Lam, Y.-Y.; et al. Cardiovascular sequalae in uncomplicated COVID-19 survivors. PLoS ONE 2021, 16, e0246732. [Google Scholar] [CrossRef]
- Satterfield, B.A.; Bhatt, D.L.; Gersh, B.J. Cardiac involvement in the long-term applications of COVID-19. Nat. Rev. Cardiol. 2022, 19, 332–341. [Google Scholar] [CrossRef]
- Tudoran, C.; Tudoran, M.; Cut, T.G.; Lazureanu, V.E.; Oancea, C.; Marinescu, A.R.; Pescariu, R.A.; Pop, G.N.; Bende, F. Evolution of echocardiographic abnormalities identified in previously healthy individuals recovering from COVID-19. J. Pers. Med. 2022, 12, 46. [Google Scholar] [CrossRef]
- Mohammad, M.; Emin, M.; Bhutta, A.; Gul, E.H.; Voorhees, E.; Afzal, M.R. Cardiac arrhythmias associated with COVID-19 infection: State of the art review. Expert Rev. Cardiovasc. Ther. 2021, 19, 881–889. [Google Scholar] [CrossRef]
- Suthahar, N.; Meijers, W.C.; Silljé, H.H.; de Boer, R.A. From inflammation to fibrosis—Molecular and cellular mechanisms of myocardial tissue remodelling and perspectives on differential treatment opportunities. Curr. Heart Fail. Rep. 2017, 14, 235–250. [Google Scholar] [CrossRef]
- Raafs, A.G.; Verdonschot, J.A.; Henkens, M.T.; Adriaans, B.P.; Wang, P.; Derks, K.; Hamid, M.A.A.; Knackstedt, C.; Empel, V.P.; Díez, J.; et al. The combination of carboxy-terminal propeptide of procollagen type I blood levels and late gadolinium enhancement at cardiac magnetic resonance provides additional prognostic information in idiopathic dilated cardiomyopathy—A multilevel assessment of myocardial fibrosis in dilated cardiomyopathy. Eur. J. Heart Fail. 2021, 23, 933–944. [Google Scholar] [CrossRef] [PubMed]
- de Boer, R.A.; De Keulenaer, G.; Bauersachs, J.; Brutsaert, D.; Cleland, J.G.; Diez, J.; Du, X.; Ford, P.; Heinzel, F.R.; Lipson, K.E.; et al. Towards better definition, quantification and treatment of fibrosis in heart failure. A scientific roadmap by the Committee of Translational Research of the Heart Failure Association (HFA) of the European Society of Cardiology. Eur. J. Heart Fail. 2019, 21, 272–285. [Google Scholar] [CrossRef] [PubMed]
- Sandler, M. Is the lung a ‘target organ’ in diabetes mellitus? Arch. Intern. Med. 1990, 150, 1385–1388. [Google Scholar] [CrossRef] [PubMed]
- Hsia, C.C.; Raskin, P. The diabetic lung: Relevance of alveolar microangiopathy for the use of inhaled insulin. Am. J. Med. 2005, 118, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Xue, Q.; Miao, L.; Cai, L. Pulmonary fibrosis: A possible diabetic complication. Diabetes/Metab. Res. Rev. 2011, 27, 311–317. [Google Scholar] [CrossRef]
- Yang, J.K.; Feng, Y.; Yuan, M.Y.; Yuan, S.Y.; Fu, H.J.; Wu, B.Y.; Sun, G.Z.; Yang, G.R.; Zhang, X.L.; Wang, L.; et al. Plasma glucose levels and diabetes are independent predictors for mortality and morbidity in patients with SARS. Diabet. Med. 2006, 23, 623–628. [Google Scholar] [CrossRef]
- Alraddadi, B.; Watson, J.T.; Almarashi, A.; Abedi, G.R.; Turkistani, A.; Sadran, M.; Housa, A.; AlMazroa, M.A.; Alraihan, N.; Banjar, A.; et al. Risk factors for primary Middle East respiratory syndrome coronavirus illness in humans, Saudi Arabia, 2014. Emerg. Infect. Dis. 2016, 22, 49–55. [Google Scholar] [CrossRef]
- Shim, H.; Hanm, X.; Jiangm, N.; Caom, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Huang, A.T.; Garcia-Carreras, B.; Hitchings, M.D.; Yang, B.; Katzelnick, L.C.; Rattigan, S.M.; Borgert, B.A.; Moreno, C.A.; Solomon, B.D.; Trimmer-Smith, L.; et al. A systematic review of antibody mediated immunity to coronaviruses: Kinetics, correlates of protection, and association with severity. Nat. Commun. 2020, 11, 4704. [Google Scholar] [CrossRef] [PubMed]
- Mallon, P.W.; Tinago, W.; Leon, A.G.; McCann, K.; Kenny, G.; McGettrick, P.; Green, S.; Inzitari, R.; Cottere, A.G.; Feeney, E.R.; et al. Dynamic change and clinical relevance of postinfectious SARS-CoV-2 antibody responses. Open Forum Infect. Dis. 2021, 8, ofab122. [Google Scholar] [CrossRef]
- Štěpánek, L.; Janošíková, M.; Štěpánek, L.; Nakládalová, M.; Boriková, A. The kinetics and predictors of anti-SARS-CoV-2 antibodies up to 8 months after symptomatic COVID-19: A Czech cross-sectional study. J. Med. Virol. 2022, 94, 3731–3738. [Google Scholar] [CrossRef] [PubMed]
- Bichara, C.D.; Amoras, E.S.; Vaz, G.L.; Bichara, C.N.; Amaral, I.P.; Vallinoto, A.C. Persistence of Anti-SARS-CoV-2 IgM antibody up to 8 Months post-COVID-19. Case Rep. Clin. Med. 2021, 10, 227–231. [Google Scholar] [CrossRef]
- Hills, S.L.; Van Keulen, A.; Feser, J.; Panella, A.; Letson, G.W.; Staples, J.E.; Marfin, A.A.; Brault, A.C. Persistence of IgM antibodies after vaccination with live attenuated Japanese encephalitis vaccine. Amer. J. Trop. Med. Hyg. 2021, 104, 576–579. [Google Scholar] [CrossRef]
- Kao, H.W.; Ashcavai, M.; Redeker, A.G. The persistence of hepatitis A IgM antibody after acute clinical hepatitis A. Hepatology 1984, 4, 933–936. [Google Scholar] [CrossRef]
- Chien, Y.-W.; Liu, Z.-H.; Tseng, F.-C.; Ho, T.-C.; Guo, H.-R.; Ko, N.-Y.; Ko, W.-C.; Perng, G.C. Prolonged persistence of IgM against dengue virus detected by commonly used commercial assays. BMC Infect. Dis. 2018, 18, 156. [Google Scholar] [CrossRef] [PubMed]
- Griffin, I.; Martin, S.W.; Fischer, M.; Chambers, T.V.; Kosoy, O.L.; Goldberg, C.; Falise, A.; Villamil, V.; Ponomareva, O.; Gillis, L.D.; et al. Zika virus IgM 25 months after symptom onset, Miami-Dade county, Florida, USA. Emerg. Infect. Dis. 2019, 25, 2264–2265. [Google Scholar] [CrossRef]
- Gibney, K.B.; Edupuganti, S.; Panella, A.J.; Kosoy, O.I.; Delorey, M.J.; Lanciotti, R.S.; Mulligan, M.J.; Fischer, M.; Staples, J.E. Detection of anti-yellow fever virus immunoglobulin M antibodies at 3–4 years following yellow fever vaccination. Am. J. Trop. Med. Hyg. 2012, 87, 1112–1115. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, H.; Signs, K.; Somsel, P.; Downes, F.P.; Clark, P.A.; Massey, J.P. Persistence of West Nile Virus (WNV) IgM antibodies in cerebrospinal fluid from patients with CNS disease. J. Clin. Virol. 2004, 31, 289–291. [Google Scholar] [CrossRef]
- Roehrig, J.T.; Nash, D.; Maldin, B.; Labowitz, A.; Martin, D.A.; Lanciotti, R.S.; Campbell, G.L. Persistence of virus-reactive serum immunoglobulin M antibody in confirmed West Nile virus encephalitis cases. Emerg. Infect. Dis. 2003, 9, 376–379. [Google Scholar] [CrossRef]
- Papa, A.; Xanthopoulou, K.; Gewehr, S.; Mourelatos, S. Detection of West Nile virus lineage 2 in mosquitoes during a human outbreak in Greece. Clin. Microbiol. Infect. 2011, 17, 1176–1180. [Google Scholar] [CrossRef]
- Murray, K.O.; Garcia, M.N.; Yan, C.; Gorchakov, R. Persistence of detectable immunoglobulin M antibodies up to 8 years after infection with West Nile virus. Amer. J. Trop. Med. Hyg. 2013, 89, 996–1000. [Google Scholar] [CrossRef] [PubMed]
- Kreye, J.; Reincke, S.M.; Prüss, H. Do cross-reactive antibodies cause neuropathology in COVID-19? Nat. Rev. Immunol. 2020, 20, 645–646. [Google Scholar] [CrossRef] [PubMed]
- Vojdani, A.; Monro, J.; Lanzisera, F.; Sadeghi, H. Serological cross-reactivity between viruses and their contribution to autoimmunity. Autoimmun. Rev. 2021, 20, 102840. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 312) | Female (n = 211) | Male (n = 101) p-Value | |
|---|---|---|---|
| Age †, years | 54 (42.5;60) | 54 (44;60) | 55 (40;61) ns |
| BMI †, kg/m2 | 26.9 (23.4;31.1) | 26.9 (23.1;31.6) | 26.7 (24;30.4) ns |
| Obesity class | |||
| Overweight | |||
| (BMI 25.0–29.9) | 90 (28.9) | 57 (27.0) | 33 (32.7) ns |
| Obese | |||
| (BMI 30.0) | 103 (33.0) | 73 (34.6) | 30 (29.7) ns |
| CFS ≥ 4 | 243 (77.9) | 173 (82.0) | 70 (69.31) 0.013 |
| Hypertension | 158 (50.6) | 112 (53.1) | 61 (60.4) ns |
| GI disorders | 74 (23.7) | 49 (23.2) | 25 (24.7) ns |
| Neurological disorders | 43 (13.8) | 31 (14.7) | 12 (11.9) ns |
| Type 2 Diabetes | 40 (12.8) | 27 (12.8) | 12 (12.9) ns |
| CAD | 30 (9.62) | 15 (7.10) | 15 (14.9) 0.039 |
| Endocrine disorders | 17 (5.45) | 16 (7.58) | 1 (0.99) 0.015 |
| Heart Failure | 14 (4.49) | 8 (3.79) | 6 (5.94) ns |
| UTI disorders | 14 (4.49) | 7 (3.32) | 7 (6.93) ns |
| Rhythm disturbances | 6 (1.92) | 3 (1.42) | 3 (1.42) ns |
| Asthma | 7 (2.24) | 6 (2.84) | 1 (0.99) ns |
| COPD | 2 (0.64) | 1 (0.47) | 1 (0.99) ns |
| Total (n = 312) | Female (n = 211) | Male (n = 101) | p-Value | |
|---|---|---|---|---|
| Fatigue | 220 (70.5) | 143 (67.8) | 77 (76.2) | ns |
| Tiredness | 180 (57.7) | 118 (55.9) | 62 (61.5) | ns |
| Sleep disturbances | 168 (53.9) | 116 (55.0) | 52 (51.5) | ns |
| Muscle pain | 109 (34.9) | 78 (37.0) | 31 (30.7) | ns |
| Memory dysfunction | 108 (34.6) | 81 (38.4) | 27 (26.7) | 0.04 |
| Dizziness | 107 (34.3) | 80 (37.9) | 27 (26.7) | 0.05 |
| Headache | 79 (25.3) | 59 (28.0) | 20 (19.8) | ns |
| BP instability | 62 (19.9) | 38 (18.0) | 24 (23.8) | ns |
| Palpitation | 47 (15.1) | 34 (16.1) | 13 (12.9) | ns |
| Dyspnea on exertion | 45 (14.4) | 31 (14.7) | 14 (13.9) | ns |
| Joint pain | 39 (12.5) | 30 (14.2) | 9 (8.9) | ns |
| Increased sweating | 39 (12.5) | 29 (13.7) | 10 (9.9) | ns |
| Anxiety | 28 (8.97) | 26 (12.32) | 2 (1.98) | 0.003 |
| Hair loss | 27 (8.65) | 19 (9.00) | 8 (7.92) | ns |
| Dyspnea on rest | 18 (5.77) | 11 (5.21) | 7 (6.93) | ns |
| Decreased vision | 18 (5.77) | 12 (5.69) | 6 (5.94) | ns |
| GI symptoms | 16 (5.13) | 12 (5.69) | 4 (3.96) | ns |
| Chest pain in rest | 12 (3.85) | 11 (5.21) | 1 (0.99) | ns |
| Daytime sleeping | 11 (3.53) | 6 (2.84) | 5 (4.95) | ns |
| Cough with sputum | 9 (2.88) | 7 (3.32) | 2 (1.98) | ns |
| Mood change | 8 (2.56) | 5 (2.37) | 3 (2.97) | ns |
| Chest pain on exertion | 7 (2.24) | 5 (2.37) | 2 (1.98) | ns |
| Dry cough | 7 (2.24) | 7 (3.32) | 0 | ns |
| Numbness in extremity | 7 (2.24) | 5 (2.37) | 2 (1.98) | ns |
| Decreased hearing | 6 (1.92) | 6 (2.84) | 0 | ns |
| Tremor in extremity | 5 (1.60) | 3 (1.42) | 2 (1.98) | ns |
| Impaired sense of smell | 5 (1.60) | 3 (1.42) | 2 (1.98) | ns |
| Increased weight | 4 (1.28) | 3 (1.42) | 1 (0.99) | ns |
| Decreased concentration | 3 (0.96) | 2 (0.95) | 1 (0.99) | ns |
| Wheezing | 2 (0.67) | 1 (0.47) | 1 (0.99) | ns |
| Nervousness | 2 (0.64) | 2 (0.95) | 0 | ns |
| Presyncope | 2 (0.64) | 2 (0.95) | 0 | ns |
| Syncope | 2 (0.64) | 2 (0.95) | 0 | ns |
| Impaired sense of taste | 2 (0.64) | 1 (0.47) | 1 (0.99) | ns |
| Fever | 2 (0.64) | 1 (0.47) | 1 (0.99) | ns |
| Edema of extremities | 2 (0.64) | 2 (0.95) | 0 | ns |
| Serum Cardiac Biomarker | Total | |
|---|---|---|
| NT-proBNP > 125 pg/mL | 37 (11.9) | |
| Electrocardiography | ||
| Sinus bradycardia < 60 bpm | 26 (8.33) | |
| Sinus bradycardia < 50 bpm | 4 (1.28) | |
| Total | Newly detected | |
| Echocardiography | ||
| Left ventricular ejection fraction †, % | 61 ± 4.55 | |
| Left ventricular ejection fraction <50% | 5 (1.60) | |
| Left ventricular hypertrophy | 50 (15.5) | 7 (2.24) |
| Diastolic dysfunction of left ventricle | 122 (39.1) | 2 (0.64) |
| Dilation of right atrium | 2 (0.64) | 1 (0.32) |
| Dilation of left atrium | 12 (3.85) | 0 |
| Holter electrocardiography | ||
| Atrial fibrillation | 5 (1.60) | 4 (1.28) |
| AV block II degree | 4 (0.32) | 3 (0.96) |
| Sinoatrial block | 1 (0.32) | 1 (0.32) |
| RBBB | 1 (0.32) | 1 (0.32) |
| 24 hr BPM | ||
| Mean SBP ≥140 mmHg | 71 (22.8) | 19 (6.10) |
| Mean DBP ≥90 mm Hg | 49 (15.7) | 19 (6.10) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tauekelova, A.T.; Kalila, Z.; Bakhtiyar, A.; Sautbayeva, Z.; Len, P.; Sailybayeva, A.; Khamitov, S.; Kadroldinova, N.; Barteneva, N.S.; Bekbossynova, M.S. Association of Lung Fibrotic Changes and Cardiological Dysfunction with Comorbidities in Long COVID-19 Cohort. Int. J. Environ. Res. Public Health 2023, 20, 2567. https://doi.org/10.3390/ijerph20032567
Tauekelova AT, Kalila Z, Bakhtiyar A, Sautbayeva Z, Len P, Sailybayeva A, Khamitov S, Kadroldinova N, Barteneva NS, Bekbossynova MS. Association of Lung Fibrotic Changes and Cardiological Dysfunction with Comorbidities in Long COVID-19 Cohort. International Journal of Environmental Research and Public Health. 2023; 20(3):2567. https://doi.org/10.3390/ijerph20032567
Chicago/Turabian StyleTauekelova, Ainur T., Zhanar Kalila, Akerke Bakhtiyar, Zarina Sautbayeva, Polina Len, Aliya Sailybayeva, Sadyk Khamitov, Nazira Kadroldinova, Natasha S. Barteneva, and Makhabbat S. Bekbossynova. 2023. "Association of Lung Fibrotic Changes and Cardiological Dysfunction with Comorbidities in Long COVID-19 Cohort" International Journal of Environmental Research and Public Health 20, no. 3: 2567. https://doi.org/10.3390/ijerph20032567
APA StyleTauekelova, A. T., Kalila, Z., Bakhtiyar, A., Sautbayeva, Z., Len, P., Sailybayeva, A., Khamitov, S., Kadroldinova, N., Barteneva, N. S., & Bekbossynova, M. S. (2023). Association of Lung Fibrotic Changes and Cardiological Dysfunction with Comorbidities in Long COVID-19 Cohort. International Journal of Environmental Research and Public Health, 20(3), 2567. https://doi.org/10.3390/ijerph20032567