
Prevalence, Patterns, and Clinical Severity of Long COVID among Chinese Medicine Telemedicine Service Users: Preliminary Results from a Cross-Sectional Study

 , , ,
, , ,
Abstract
1. Introduction
2. Methods
2.1. Setting and Participants
2.2. C19-YRS Assessment
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Respondents
3.2. Symptom and Functional Assessment
3.3. Subgroup Analysis
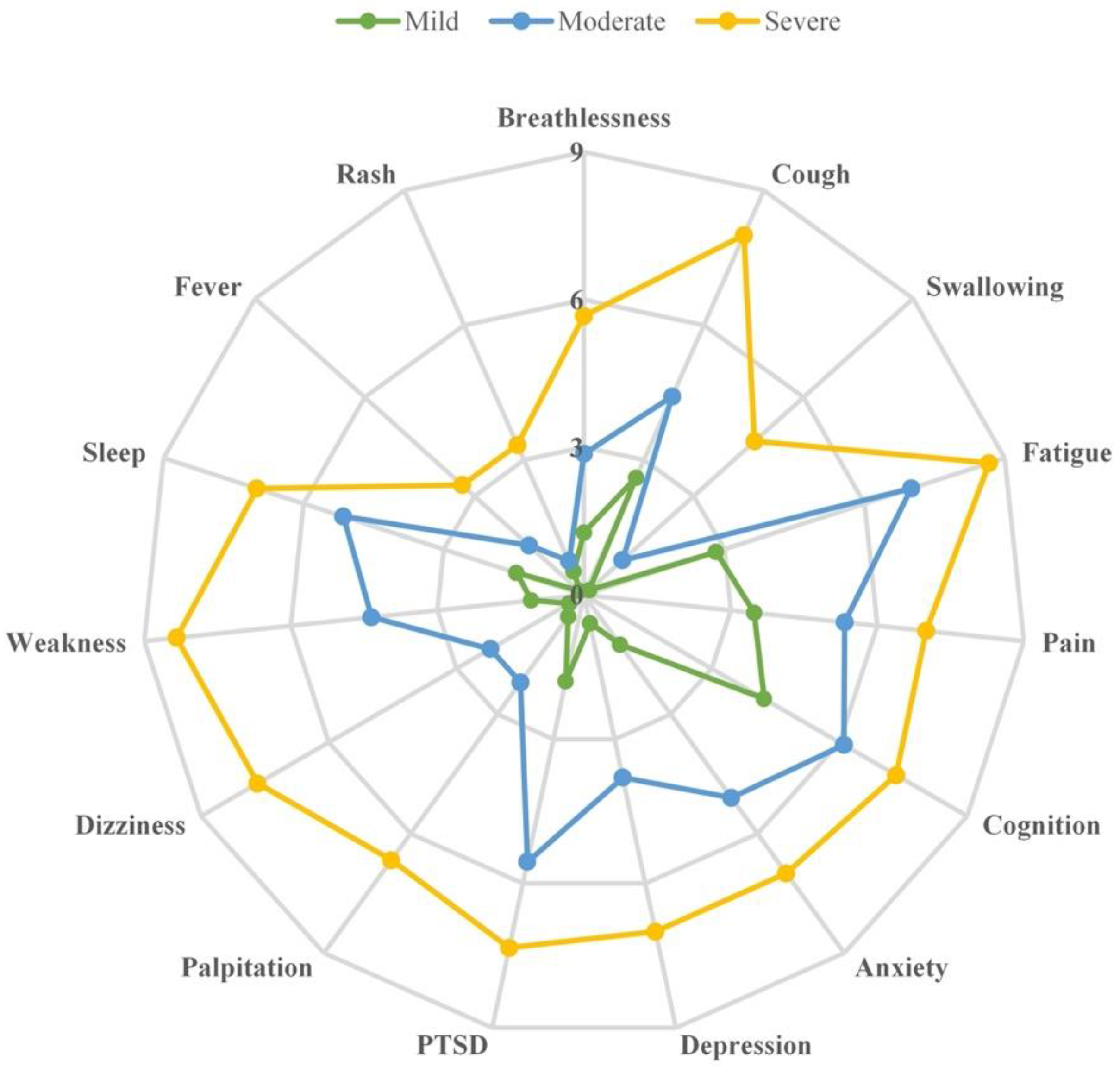
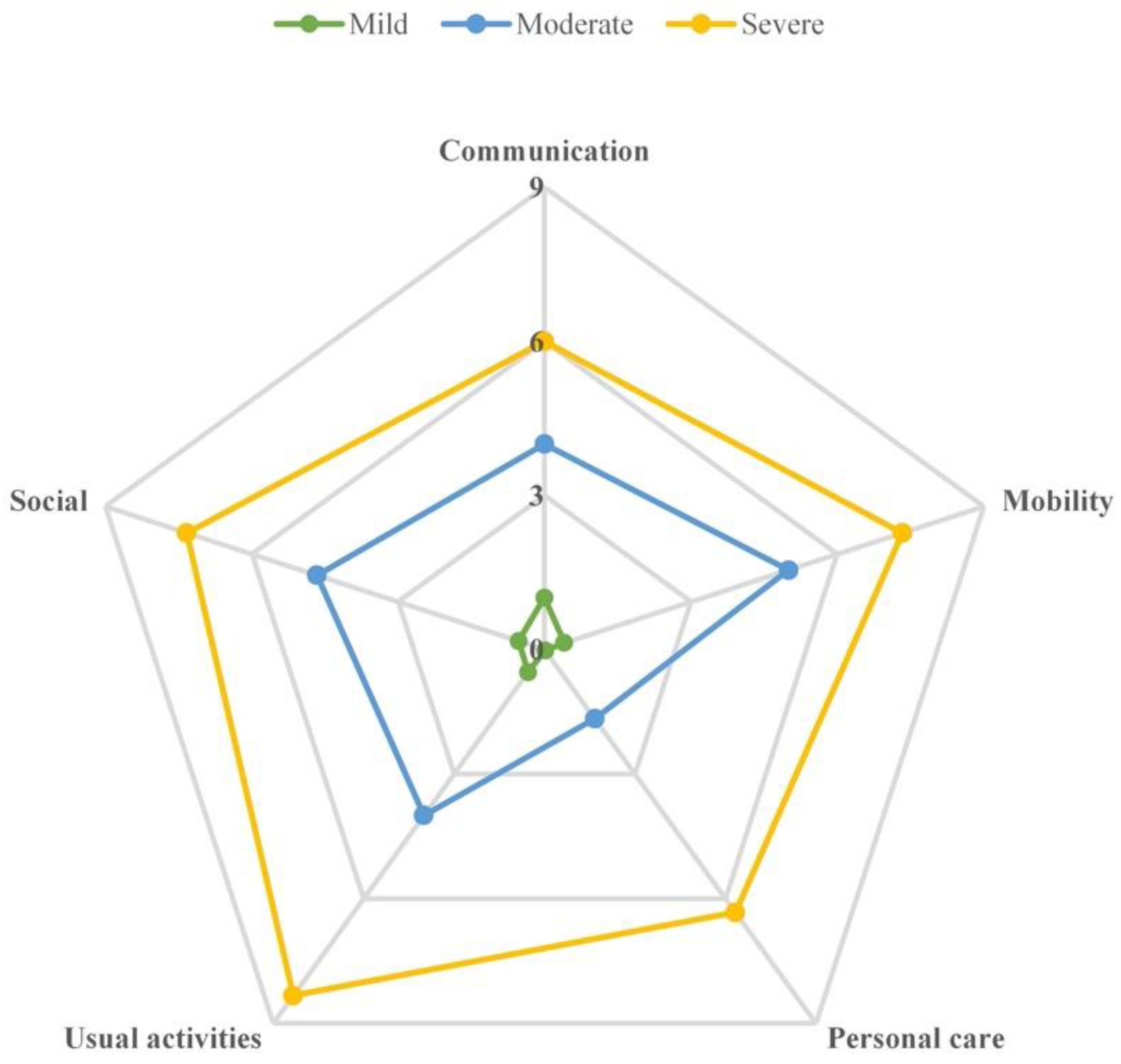
3.4. Symptom and Functional Distribution in Three Severity Categories
3.5. Correlation Analysis between Symptom Severity, Functional Impairments, and Overall Health
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Sivan, M.; Parkin, A.; Makower, S.; Greenwood, D.C. Post-COVID syndrome symptoms, functional disability, and clinical severity phenotypes in hospitalized and nonhospitalized individuals: A cross-sectional evaluation from a community COVID rehabilitation service. J. Med. Virol. 2022, 94, 1419–1427. [Google Scholar] [CrossRef]
- World Health Organization Home Page. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Post_COVID-19_condition-Clinical_case_definition-2021.1 (accessed on 1 September 2022).
- García, B.A.; Balado, Y.B.; López, A.P.; Lema, E.R.; Marchán-López, Á.; Álvarez, A.R.; País, M.J.G.; Sánchez, J.C.; Rey, R.R. Assessment of Post-COVID Symptoms Using the C19-YRS Tool in a Cohort of Patients from the First Pandemic Wave in Northwestern Spain. Telemed. e-Health, 2022; ahead of print. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute covid-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef]
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in Adults at 6 Months After COVID-19 Infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Kim, S.S.; Lindsell, C.J.; Rose, E.B.; Shapiro, N.I.; Files, D.C.; Gibbs, K.W.; Erickson, H.L.; Steingrub, J.S.; Smithline, H.A.; et al. Symptom Duration and Risk Factors for Delayed Return to Usual Health Among Outpatients with COVID-19 in a Multistate Health Care Systems Network—United States, March–June 2020. MMWR. Morb. Mortal. Wkly. Rep. 2020, 69, 993–998. [Google Scholar] [CrossRef]
- Cutler, D.M.; Summers, L.H. The COVID-19 Pandemic and the $16 Trillion Virus. JAMA J. Am. Med. Assoc. 2020, 324, 1495–1496. [Google Scholar] [CrossRef]
- Sivan, M.; University of Leeds; Halpin, S.; Gee, J.; Trust, A.N.F. Assessing long-term rehabilitation needs in COVID-19 survivors using a telephone screening tool (C19-YRS tool). Adv. Clin. Neurosci. Rehabil. 2020, 19, 14–17. [Google Scholar] [CrossRef]
- Sivan, M.; University of Leeds; Halpin, S.; Gees, J.; Makower, S.; Parkin, A.; Ross, D.; Horton, M.; O’Connor, R.; Hospitals, L.T.; et al. The self-report version and digital format of the COVID-19 Yorkshire Rehabilitation Scale (C19-YRS) for Long Covid or Post-COVID syndrome assessment and monitoring. Adv. Clin. Neurosci. Rehabil. 2021, 20. [Google Scholar] [CrossRef]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef]
- Kayaaslan, B.; Eser, F.; Kalem, A.K.; Kaya, G.; Kaplan, B.; Kacar, D.; Hasanoglu, I.; Coskun, B.; Guner, R. Post-COVID syndrome: A single-center questionnaire study on 1007 participants recovered from COVID-19. J. Med. Virol. 2021, 93, 6566–6574. [Google Scholar] [CrossRef]
- Hafeez, M.; Azhar, M.; Chudhary, H.; Nazar, W.; Rana, M. Innovation of audio-visual triage system in combating the spread of COVID-19 infection and its efficacy: A novel strategy. Pak. J. Intensiv. Care Med. 2021, 2021. [Google Scholar] [CrossRef]
- Sivan, M.; Taylor, S. NICE guideline on long covid. BMJ 2020, 371, m4938. [Google Scholar] [CrossRef]
- NHS England Home Page. Available online: https://www.england.nhs.uk/publication/national-commissioning-guidance-for-post-covid-services/ (accessed on 1 September 2022).
- The Chinese University of Hong Kong Chinese Specialty Clinic cum Clinical Teaching and Research Centre (CUHK CSCCTRC) Home Page. Available online: http://clinic.scm.cuhk.edu.hk/clinic/index.aspx (accessed on 30 September 2022).
- REDCap Home Page. Available online: www.project-redcap.org (accessed on 30 September 2022).
- Frontera, J.A.; Yang, D.; Medicherla, C.; Baskharoun, S.; Bauman, K.; Bell, L.; Bhagat, D.; Bondi, S.; Chervinsky, A.; Dygert, L.; et al. Trajectories of Neu-rologic Recovery 12 Months After Hospitalization for COVID-19: A Prospective Longitudinal Study. Neurol. 2022, 99, e33–e45. [Google Scholar] [CrossRef]
- Taquet, M.; Dercon, Q.; Harrison, P.J. Six-month sequelae of post-vaccination SARS-CoV-2 infection: A retrospective cohort study of 10,024 breakthrough infections. Brain Behav. Immun. 2022, 103, 154–162. [Google Scholar] [CrossRef]
- Tavares-Júnior, J.W.; de Souza, A.C.; Borges, J.W.; Oliveira, D.N.; Siqueira-Neto, J.I.; Sobreira-Neto, M.A.; Braga-Neto, P. COVID-19 associated cognitive impairment: A systematic review. Cortex 2022, 152, 77–97. [Google Scholar] [CrossRef]
- Subramanian, A.; Nirantharakumar, K.; Hughes, S.; Myles, P.; Williams, T.; Gokhale, K.M.; Taverner, T.; Chandan, J.S.; Brown, K.; Simms-Williams, N.; et al. Symptoms and risk factors for long COVID in non-hospitalized adults. Nat. Med. 2022, 28, 1706–1714. [Google Scholar] [CrossRef]
- Fernández-De-Las-Peñas, C.; Palacios-Ceña, D.; Gómez-Mayordomo, V.; Florencio, L.L.; Cuadrado, M.L.; Plaza-Manzano, G.; Navarro-Santana, M. Prevalence of post-COVID-19 symptoms in hospitalized and non-hospitalized COVID-19 survivors: A systematic review and meta-analysis. Eur. J. Intern. Med. 2021, 92, 55–70. [Google Scholar] [CrossRef]
- Lopez-Leon, S.; Wegman-Ostrosky, T.; Perelman, C.; Sepulveda, R.; Rebolledo, P.A.; Cuapio, A.; Villapol, S. More than 50 long-term effects of COVID-19: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Premraj, L.; Kannapadi, N.V.; Briggs, J.; Seal, S.M.; Battaglini, D.; Fanning, J.; Suen, J.; Robba, C.; Fraser, J.; Cho, S.-M. Mid and long-term neurological and neuropsychiatric manifestations of post-COVID-19 syndrome: A meta-analysis. J. Neurol. Sci. 2022, 434. [Google Scholar] [CrossRef]
- Klein, J.; Wood, J.; Jaycox, J.; Lu, P.; Dhodapkar, R.M.; Gehlhausen, J.R.; Tabachnikova, A.; Tabacof, L.; Malik, A.A.; Kamath, K.; et al. Distinguishing features of Long COVID identified through immune profiling. medRxiv 2022. [Google Scholar] [CrossRef]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; de Noordhout, C.M.; Jong, C.P.-D.; Cleemput, I.; Heede, K.V.D. Pathophysiology and mechanism of long COVID: A comprehensive review. Ann. Med. 2022, 54, 1473–1487. [Google Scholar] [CrossRef] [PubMed]
- Phetsouphanh, C.; Darley, D.R.; Wilson, D.B.; Howe, A.; Munier, C.M.L.; Patel, S.K.; Juno, J.A.; Burrell, L.M.; Kent, S.J.; Dore, G.J.; et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat Immunol 2022, 23, 210–216. [Google Scholar] [CrossRef]
- NICE National Institute for Health and Care Excellence Home Page. Available online: https://www.nice.org.uk/guidance/ng188 (accessed on 1 September 2022).
- Hospital Authority of the Government of the Hong Kong Special Administrative Region (HKSARG HA) Home Page. Available online: https://cmk.ha.org.hk/zh-cht/services/SpecialCMOPProg/SpecialCMOPProgEng (accessed on 30 September 2022).
- Chopra, V.; Flanders, S.A.; O’Malley, M.; Malani, A.N.; Prescott, H.C. Sixty-Day Outcomes Among Patients Hospitalized with COVID-19. Ann. Intern. Med. 2021, 174, 576–578. [Google Scholar] [CrossRef]
- Décary, S.; Dugas, M.; Stefan, T.; Langlois, L.; Skidmore, B.; Bhéreur, A.; LeBlanc, A.; Alberta Health Services; Hastings, S.; Manns, B.; et al. Care Models for Long COVID: A Rapid Systematic Review. medRxiv 2021. [Google Scholar] [CrossRef]
- Parkin, A.; Davison, J.; Tarrant, R.; Ross, D.; Halpin, S.; Simms, A.; Salman, R.; Sivan, M. A Multidisciplinary NHS COVID-19 Service to Manage Post-COVID-19 Syndrome in the Community. J. Prim. Care Community Heal. 2021, 12. [Google Scholar] [CrossRef]
- The Jockey Club School of Public Health and Primary Care at The Chinese University of Hong Kong (CUHK JCSPHPC) Home Page. Available online: www.jclongcovid.cuhk.edu.hk (accessed on 30 September 2022).
- Bai, F.; Tomasoni, D.; Falcinella, C.; Barbanotti, D.; Castoldi, R.; Mulè, G.; Augello, M.; Mondatore, D.; Allegrini, M.; Cona, A.; et al. Female gender is associated with long COVID syndrome: A pro-spective cohort study. Clin Microbiol Infect 2022, 28, 611.e9–611.e16. [Google Scholar] [CrossRef]
- Berger, Z.; Jesus, V.A.D.; Assoumou, S.A.; Greenhalgh, T. Long COVID and Health Inequities: The Role of Primary Care. Milbank Q. 2021, 99, 519–541. [Google Scholar] [CrossRef]
- The Government of the Hong Kong Special Administrative Region (HKSARG) Home Page. Available online: http://www.coronavirus.gov.hk/eng/vaccine-pass.html (accessed on 30 September 2022).
- Notarte, K.I.; Catahay, J.A.; Velasco, J.V.; Pastrana, A.; Ver, A.T.; Pangilinan, F.C.; Peligro, P.J.; Casimiro, M.; Guerrero, J.J.; Gellaco, M.M.L.; et al. Impact of COVID-19 vaccination on the risk of developing long-COVID and on existing long-COVID symptoms: A systematic review. EClinicalMedicine 2022. [Google Scholar] [CrossRef]
- Sivan, M.; Preston, N.; Parkin, A.; Makower, S.; Gee, J.; Ross, D.; Tarrant, R.; Davison, J.; Halpin, S.; O’Connor, R.J.; et al. The modified COVID-19 Yorkshire Rehabilitation Scale (C19-YRSm) patient-reported outcome measure for Long Covid or Post-COVID-19 syndrome. J. Med. Virol. 2022, 94, 4253–4264. [Google Scholar] [CrossRef]
- Baruch, Y.; Holtom, B.C. Survey response rate levels and trends in organizational research. Hum. Relat. 2008, 61, 1139–1160. [Google Scholar] [CrossRef]
- Ferorelli, D.; Celentano, F.E.; Benevento, M.; Dell’Erba, A.; Solarino, B. Destruction of telecommunications hinders access to healthcare: A crime against humanity? J. Telemed. Telecare 2023, 29, 72. [Google Scholar] [CrossRef]
- Demaerschalk, B.M.; Hollander, J.E.; Krupinski, E.; Scott, J.; Albert, D.; Bobokalonova, Z.; Bolster, M.; Chan, A.; Christopherson, L.; Coffey, J.D.; et al. Quality Frameworks for Virtual Care: Expert Panel Recommendations. Mayo Clin. Proc. Innov. Qual. Outcomes 2022, 7, 31–44. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | All Respondents (n = 135) |
|---|---|
| Age (yr) | 46.78 ± 14.05 |
| Gender (male) | 46 (34.07%) |
| BMI (kg/m2) | 23.06 ± 4.03 |
| Degree of education | |
| High school or below | 37 (27.41%) |
| Undergraduate or above | 85 (62.96%) |
| Not reported | 13 (9.63%) |
| Smoking a | 9 (6.67%) |
| Employment status | |
| Still employed/student | 91 (67.41%) |
| Still retired/homemaker/unemployed | 37 (27.41%) |
| Reduced hours | 3 (2.22%) |
| Stopped work | 1 (0.74%) |
| Not reported | 3 (2.22%) |
| Clinical characteristics | |
| Admission to hospital | 3 (2.22%) |
| Other medical | 48 (35.56%) |
| Number of chronic diseases | |
| 0 | 73 (54.07%) |
| 1 | 33 (24.44%) |
| 2 | 13 (9.63%) |
| 3 | 3 (2.22%) |
| Not reported | 13 (9.63%) |
| COVID-19 vaccine doses | |
| 0 | 3 (2.22%) |
| 1 | 12 (8.89%) |
| 2 | 66 (48.89%) |
| 3 | 41 (30.37%) |
| Not reported | 13 (9.63%) |
| Received influenza vaccination in the past 3 months | 10 (7.41%) |
| Symptoms/Functional Impairments | N | Prevalence a | Score b | ||||
|---|---|---|---|---|---|---|---|
| Current | Pre-COVID | Current | Pre-COVID | Z | p | ||
| Breathlessness | 135 | 108 (80.00%) | 93 (68.89%) | 1.60 ± 1.79 | 0.90 ± 1.23 | −6.907 | <0.001 |
| At rest | 135 | 42 (31.11%) | 21 (15.56%) | 1.05 ± 1.95 | 0.39 ± 1.15 | −5.203 | <0.001 |
| On dressing | 130 | 24 (18.46%) | 11 (8.46%) | 0.61 ± 1.61 | 0.28 ± 1.07 | −3.757 | <0.001 |
| On walking | 128 | 103 (80.47%) | 93 (72.66%) | 3.13 ± 2.47 | 2.09 ± 1.94 | −6.562 | <0.001 |
| Laryngeal/airway complications | 135 | 92 (68.15%) | - | 3.21 ± 2.41 | 0.72 ± 1.31 | −7.514 | <0.001 |
| Cough | 135 | 86 (63.70%) | - | - | - | - | - |
| Voice | 135 | 23 (17.04%) | - | - | - | - | - |
| Breathing murmur | 135 | 10 (7.41%) | - | - | - | - | - |
| The worst among them | |||||||
| cough | 89 | 81 (91.01%) | - | 3.19 ± 2.43 | 0.78 ± 1.35 | −7.155 | <0.001 |
| voice | 89 | 5 (5.62%) | - | 4.20 ± 2.59 | 0.20 ± 0.45 | −1.841 | 0.066 |
| breathing murmur | 89 | 3 (3.37%) | - | 2.33 ± 1.16 | 0.00 ± 0.00 | −1.633 | 0.102 |
| Swallowing | 135 | 19 (14.07%) | 9 (6.67%) | 0.38 ± 1.18 | 0.19 ± 0.83 | −3.482 | <0.001 |
| Nutrition | 135 | 15 (11.11%) | - | - | - | - | - |
| Fatigue | 135 | 103 (76.30%) | 89 (65.93%) | 3.57 ± 2.79 | 1.70 ± 1.71 | −8.254 | <0.001 |
| Incontinence | 134 | 6 (4.48%) | - | 5.33 ± 3.39 | 2.33 ± 1.51 | −2.041 | 0.041 |
| Fecal | 134 | 1 (0.75%) | - | - | - | - | - |
| Urinary | 134 | 6 (4.48%) | - | - | - | - | - |
| The worst among them | |||||||
| fecal | 6 | 0 (0.0%) | - | - | - | ||
| urinary | 6 | 6 (100.0%) | - | 5.33 ± 3.39 | 2.33 ± 1.51 | −2.041 | 0.041 |
| Pain | 134 | 34 (25.37%) | - | 4.18 ± 1.99 | 0.82 ± 1.40 | −4.961 | <0.001 |
| Chest pain | 134 | 12 (8.96%) | - | - | - | - | - |
| Joint pain | 134 | 11 (8.21%) | - | - | - | - | - |
| Muscle ache | 134 | 17 (12.69%) | - | - | - | - | - |
| Headache | 134 | 17 (12.69%) | - | - | - | - | - |
| Abdominal pain | 134 | 8 (5.97%) | - | - | - | - | - |
| Other pain | 134 | 8 (5.97%) | - | - | - | - | - |
| The worst in the past week | |||||||
| chest pain | 34 | 8 (23.53%) | - | 4.13 ± 1.46 | 0.50 ± 0.76 | −2.539 | 0.011 |
| joint pain | 34 | 4 (11.76%) | - | 6.00 ± 2.58 | 2.25 ± 2.22 | −1.890 | 0.059 |
| muscle ache | 34 | 7 (20.59%) | - | 4.71 ± 1.70 | 0.86 ± 1.57 | −2.226 | 0.026 |
| headache | 34 | 8 (23.53%) | - | 3.63 ± 2.13 | 1.00 ± 1.60 | −2.539 | 0.011 |
| abdominal pain | 34 | 3 (8.82%) | - | 4.00 ± 1.00 | 0.00 ± 0.00 | −1.604 | 0.109 |
| other pain | 34 | 4 (11.76%) | - | 2.75 ± 2.50 | 0.25 ± 0.50 | −1.604 | 0.109 |
| Cognition | 134 | 77 (57.46%) | - | 4.80 ± 2.15 | 1.77 ± 1.34 | −7.355 | <0.001 |
| Concentrating | 134 | 53 (39.55%) | - | - | - | - | - |
| Short-term memory | 134 | 72 (53.73%) | - | - | - | - | - |
| Event planning | 134 | 38 (28.36%) | - | - | - | - | - |
| The worst among them | |||||||
| concentrating | 77 | 20 (25.97%) | - | 4.15 ± 1.63 | 1.55 ± 1.15 | −3.759 | <0.001 |
| short-term memory | 77 | 53 (68.83%) | - | 4.96 ± 2.25 | 1.75 ± 1.31 | −6.177 | <0.001 |
| event planning | 77 | 4 (5.19%) | - | 6.00 ± 2.94 | 1.75 ± 1.26 | −1.633 | 0.102 |
| Anxiety | 133 | 67 (50.38%) | 55 (41.35%) | 1.96 ± 2.46 | 1.02 ± 1.58 | −6.075 | <0.001 |
| Depression | 133 | 47 (35.34%) | 41 (30.83%) | 1.22 ± 2.13 | 0.70 ± 1.43 | −4.669 | <0.001 |
| Thoughts about harming yourself | 133 | 2 (1.50%) | - | - | - | - | - |
| Post-traumatic stress disorder | |||||||
| Unwanted memories | 134 | 7 (5.22%) | - | - | - | - | - |
| Unpleasant dreams | 134 | 8 (5.97%) | - | - | - | - | - |
| Avoid thoughts | 134 | 18 (13.43%) | - | - | - | - | - |
| Pressure | 133 | 84 (63.16%) | 78 (58.65%) | 2.49 ± 2.52 | 1.74 ± 1.92 | −5.968 | <0.001 |
| Communication | 132 | 45 (34.09%) | 36 (27.27%) | 1.19 ± 1.97 | 0.56 ± 1.23 | −5.050 | <0.001 |
| Mobility | 132 | 27 (20.45%) | 14 (10.61%) | 0.67 ± 1.61 | 0.32 ± 1.09 | −4.250 | <0.001 |
| Personal care | 132 | 7 (5.30%) | 4 (3.03%) | 0.20 ± 1.05 | 0.14 ± 0.86 | −2.271 | 0.023 |
| Usual activities | 132 | 34 (25.76%) | 16 (12.12%) | 0.80 ± 1.76 | 0.28 ± 1.07 | −4.743 | <0.001 |
| Social | 132 | 30 (22.73%) | 15 (11.36%) | 0.78 ± 1.82 | 0.26 ± 0.98 | −4.408 | <0.001 |
| Palpitation | 132 | 40 (30.30%) | - | 0.94 ± 1.70 | - | - | - |
| Dizziness | 131 | 42 (32.06%) | - | 0.80 ± 1.59 | - | - | - |
| Weakness | 131 | 72 (54.96%) | - | 1.75 ± 2.18 | - | - | - |
| Sleep | 131 | 69 (52.67%) | - | 2.14 ± 2.77 | - | - | - |
| Fever | 131 | 19 (14.50%) | - | 0.40 ± 1.24 | - | - | - |
| Rash | 131 | 27 (20.61%) | - | 0.62 ± 1.47 | - | - | - |
| Overall health | 130 | - | - | 5.43 ± 2.33 | 6.78 ± 2.22 | −8.008 | <0.001 |
| Age | Gender | Education | Chronic Disease | COVID-19 Vaccine | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Z | p | Z | p | Z | p | Z | p | Z | p | |
| Breathlessness | −0.824 | 0.410 | −1.061 | 0.288 | −0.864 | 0.387 | −0.404 | 0.686 | −1.278 | 0.201 |
| Cough | −0.703 | 0.482 | −0.546 | 0.585 | −1.301 | 0.193 | −0.464 | 0.643 | −0.408 | 0.684 |
| Swallowing | −2.788 | 0.005b | −0.758 | 0.449 | −0.372 | 0.710 | −0.758 | 0.448 | −0.740 | 0.459 |
| Fatigue | −0.858 | 0.391 | −1.107 | 0.268 | −1.274 | 0.203 | −0.306 | 0.760 | −0.203 | 0.839 |
| Pain | −0.562 | 0.574 | −1.173 | 0.241 | −0.075 | 0.940 | −2.685 | 0.007a | −1.450 | 0.147 |
| Cognition | −0.515 | 0.606 | −0.360 | 0.719 | −0.125 | 0.901 | −1.992 | 0.046a | −0.656 | 0.512 |
| Anxiety | −0.674 | 0.500 | −1.258 | 0.208 | −0.405 | 0.686 | −0.650 | 0.516 | −1.907 | 0.056 |
| Depression | −2.195 | 0.028b | −1.332 | 0.183 | −0.153 | 0.879 | −0.397 | 0.691 | −1.117 | 0.264 |
| PTSD | −0.847 | 0.397 | −0.278 | 0.781 | −0.597 | 0.551 | −0.085 | 0.932 | −1.592 | 0.111 |
| Communication | −0.640 | 0.522 | −0.717 | 0.474 | −0.970 | 0.332 | −0.104 | 0.917 | −0.223 | 0.824 |
| Mobility | −1.544 | 0.123 | −0.519 | 0.604 | −0.986 | 0.324 | −1.435 | 0.151 | −1.994 | 0.046a |
| Personal care | −3.097 | 0.002b | −0.027 | 0.979 | −3.069 | 0.002a | −1.422 | 0.155 | −0.387 | 0.699 |
| Usual activities | −1.081 | 0.280 | −1.657 | 0.098 | −0.703 | 0.482 | −0.696 | 0.486 | −1.293 | 0.196 |
| Social | −2.276 | 0.023b | −2.098 | 0.036b | −0.804 | 0.422 | −1.784 | 0.074 | −0.735 | 0.463 |
| Overall health | −0.527 | 0.598 | −0.167 | 0.867 | −0.382 | 0.702 | −0.570 | 0.569 | −1.054 | 0.292 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, F.F.; Xu, S.; Kwong, T.M.H.; Li, A.S.-c.; Ha, E.H.; Hua, H.; Liong, C.; Leung, K.C.; Leung, T.H.; Lin, Z.; et al. Prevalence, Patterns, and Clinical Severity of Long COVID among Chinese Medicine Telemedicine Service Users: Preliminary Results from a Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 1827. https://doi.org/10.3390/ijerph20031827
Ho FF, Xu S, Kwong TMH, Li AS-c, Ha EH, Hua H, Liong C, Leung KC, Leung TH, Lin Z, et al. Prevalence, Patterns, and Clinical Severity of Long COVID among Chinese Medicine Telemedicine Service Users: Preliminary Results from a Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(3):1827. https://doi.org/10.3390/ijerph20031827
Chicago/Turabian StyleHo, Fai Fai, Shanshan Xu, Talos Ming Hong Kwong, Angus Siu-cheong Li, Eun Hae Ha, Heyu Hua, Ching Liong, Kwan Chi Leung, Ting Hung Leung, Zhixiu Lin, and et al. 2023. "Prevalence, Patterns, and Clinical Severity of Long COVID among Chinese Medicine Telemedicine Service Users: Preliminary Results from a Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 3: 1827. https://doi.org/10.3390/ijerph20031827
APA StyleHo, F. F., Xu, S., Kwong, T. M. H., Li, A. S.-c., Ha, E. H., Hua, H., Liong, C., Leung, K. C., Leung, T. H., Lin, Z., Wong, S. Y.-S., Pan, F., & Chung, V. C. H. (2023). Prevalence, Patterns, and Clinical Severity of Long COVID among Chinese Medicine Telemedicine Service Users: Preliminary Results from a Cross-Sectional Study. International Journal of Environmental Research and Public Health, 20(3), 1827. https://doi.org/10.3390/ijerph20031827