

Pain and Psychological Readiness to Return to Sport in Elite Volleyball Players: A Cross-Sectional Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Procedure and Instruments
2.3. Statistical Analysis
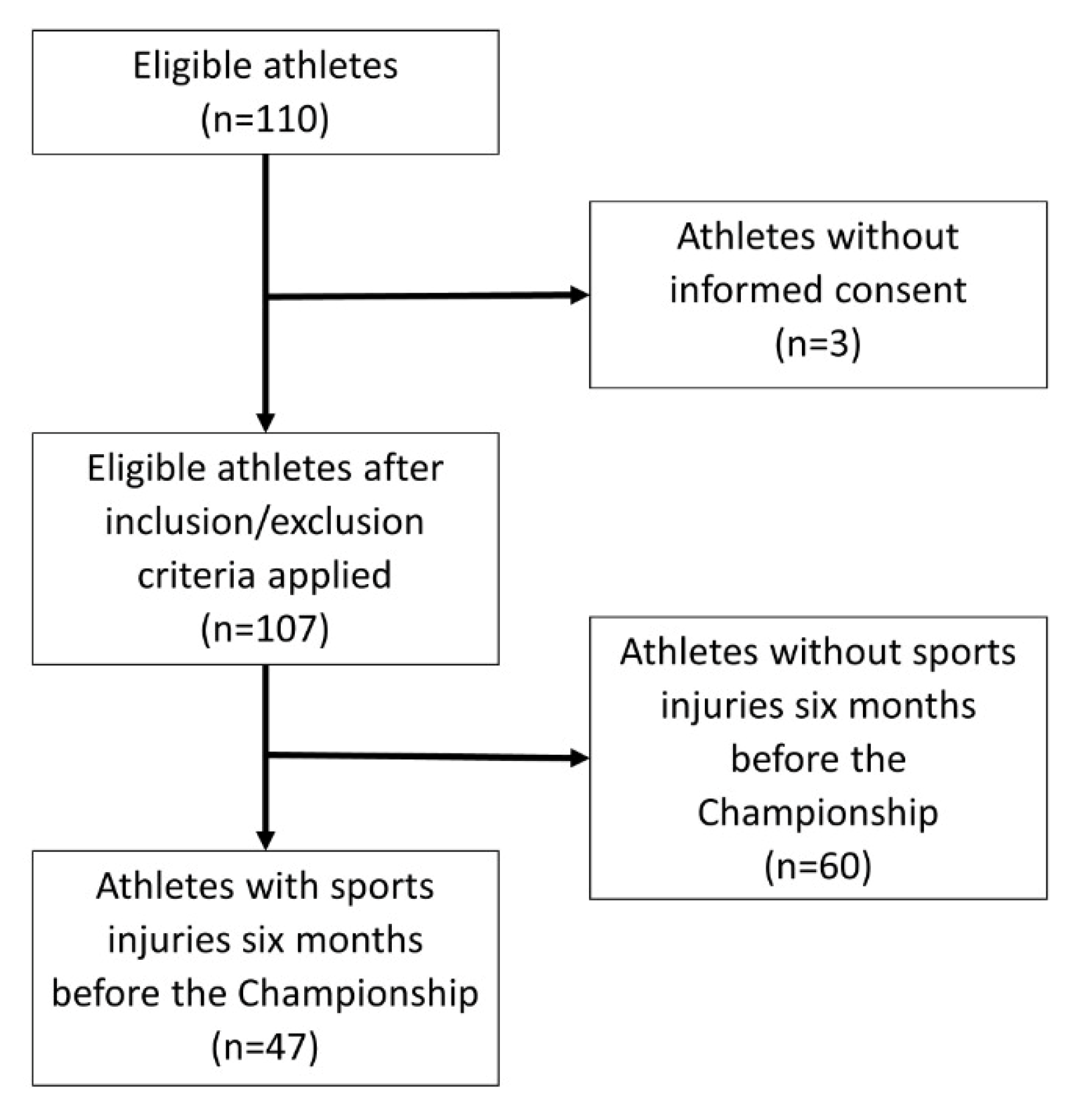
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kilic, O.; Maas, M.; Verhagen, E.; Zwerver, J.; Gouttebarge, V. Incidence, aetiology and prevention of musculoskeletal injuries in volleyball: A systematic review of the literature. Eur. J. Sport Sci. 2017, 17, 765–793. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Bahr, I.A. Incidence of acute volleyball injuries: A prospective cohort study of injury mechanisms and risk factors. Scand. J. Med. Sci. Sports 2007, 7, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Alonso, J.-M.; Jacobsson, J.; Timpka, T.; Ronsen, O.; Kajenienne, A.; Dahlström, Ö.; Spreco, A.; Edouard, P. Preparticipation injury complaint is a risk factor for injury: A prospective study of the Moscow 2013 IAAF Championships. Br. J. Sports Med. 2015, 49, 1118–1124. [Google Scholar] [CrossRef]
- Mountjoy, M.; Junge, A.; Benjamen, S.; Boyd, K.; Diop, M.; Gerrard, D.; van den Hoogenband, C.-R.; Marks, S.; Martinez-Ruiz, E.; Miller, J.; et al. Competing with injuries: Injuries prior to and during the 15th FINA World Championships 2013 (aquatics). Br. J. Sports Med. 2015, 49, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Raja, S.N.; Carr, D.B.; Cohen, M.; Finnerup, N.B.; Flor, H.; Gibson, S.; Keefe, F.J.; Mogil, J.S.; Ringkamp, M.; Sluka, K.A.; et al. The revised International Association for the Study of Pain definition of pain: Concepts, challenges, and compromises. Pain 2020, 161, 1976–1982. [Google Scholar] [CrossRef] [PubMed]
- Hasselström, J.; Liu-Palmgren, J.; Rasjö-Wrååk, G. Prevalence of pain in general practice. Eur. J. Pain 2002, 6, 375–385. [Google Scholar] [CrossRef] [PubMed]
- Bascour-Sandoval, C.; Salgado-Salgado, S.; Gómez-Milán, E.; Fernández-Gómez, J.; Michael, G.A.; Gálvez-García, G. Pain and Distraction According to Sensory Modalities: Current Findings and Future Directions. Pain Pract. 2019, 19, 686–702. [Google Scholar] [CrossRef]
- Bascour-Sandoval, C.; Belmar-Arriagada, H.; Albayay, J.; Lacoste-Abarzua, C.; Bielefeldt-Astudillo, D.; Gajardo-Burgos, R.; Vidal-Torres, M.; Gálvez-García, G. The Effect of Sleep Quality on Pain in Chilean Individuals with Musculoskeletal Disorders. Int. J. Environ. Res. Public Health 2021, 18, 11370. [Google Scholar] [CrossRef]
- Jonasson, P.; Halldin, K.; Karlsson, J.; Thoreson, O.; Hvannberg, J.; Swärd, L.; Baranto, A. Prevalence of joint-related pain in the extremities and spine in five groups of top athletes. Knee Surg. Sport Traumatol. Arthrosc. 2011, 19, 1540–1546. [Google Scholar] [CrossRef]
- Diehl, K.; Mayer, J.; Thiel, A.; Zipfel, S.; Schneider, S. “Playing hurt”: Der Umgang jugendlicher Leistungssportler mit Gelenkschmerzen. Der Schmerz 2019, 33, 49–56. [Google Scholar] [CrossRef]
- Schneider, S.; Sauer, J.; Berrsche, G.; Schmitt, H. No Pain, No Gain? Prevalence, Location, Context, and Coping Strategies with Regard to Pain Among Young German Elite Basketball Players. J. Hum. Kinet. 2019, 69, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Yokoe, T.; Tajima, T.; Yamaguchi, N.; Nagasawa, M.; Ota, T.; Morita, Y.; Chosa, E. Orthopaedic medical examination for young amateur athletes: A repeated cross-sectional study from 2014 to 2018. BMJ Open 2021, 11, e042188. [Google Scholar] [CrossRef] [PubMed]
- Gajardo-Burgos, R.; Monrroy-Uarac, M.; Barría-Pailaquilén, R.M.; Norambuena-Noches, Y.; van Rensburg, D.C.J.; Bascour-Sandoval, C.; Besomi, M. Frequency of Injury and Illness in the Final 4 Weeks before a Trail Running Competition. Int. J. Environ. Res. Public Health 2021, 18, 5431. [Google Scholar] [CrossRef] [PubMed]
- Bolling, C.; Delfino Barboza, S.; van Mechelen, W.; Pasman, H.R. How elite athletes, coaches, and physiotherapists perceive a sports injury. Transl. Sport Med. 2018, 2, 17–23. [Google Scholar] [CrossRef]
- Ardern, C.L.; Glasgow, P.; Schneiders, A.; Witvrouw, E.; Clarsen, B.; Cools, A.; Gojanovic, B.; Griffin, S.; Khan, K.M.; Moksnes, H.; et al. 2016 Consensus statement on return to sport from the First World Congress in Sports Physical Therapy, Bern. Br. J. Sports Med. 2016, 50, 853–864. [Google Scholar] [CrossRef]
- Ardern, C.L.; Taylor, N.F.; Feller, J.A.; Webster, K.E. A systematic review of the psychological factors associated with returning to sport following injury. Br. J. Sports Med. 2013, 47, 1120–1126. [Google Scholar] [CrossRef] [PubMed]
- Van der Horst, N.; Backx, F.; Goedhart, E.A.; Huisstede, B.M. Return to play after hamstring injuries in football (soccer): A worldwide Delphi procedure regarding definition, medical criteria and decision-making. Br. J. Sports Med. 2017, 51, 1583–1591. [Google Scholar] [CrossRef]
- Podlog, L.; Banham, S.M.; Wadey, R.; Hannon, J.C. Psychological Readiness to Return to Competitive Sport Following Injury: A Qualitative Study. Sport Psychol. 2015, 29, 1–14. [Google Scholar] [CrossRef]
- Burland, J.P.; Toonstra, J.L.; Howard, J.S. Psychosocial Barriers After Anterior Cruciate Ligament Reconstruction: A Clinical Review of Factors Influencing Postoperative Success. Sport. Health A Multidiscip. Approach 2019, 11, 528–534. [Google Scholar] [CrossRef]
- Clement, D.; Arvinen-Barrow, M.; Fetty, T. Psychosocial Responses During Different Phases of Sport-Injury Rehabilitation: A Qualitative Study. J. Athl. Train. 2015, 50, 95–104. [Google Scholar] [CrossRef]
- Hart, H.F.; Culvenor, A.G.; Guermazi, A.; Crossley, K.M. Worse knee confidence, fear of movement, psychological readiness to return-to-sport and pain are associated with worse function after ACL reconstruction. Phys. Ther. Sport 2020, 41, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Maclachlan, L.R.; Collins, N.J.; Matthews, M.L.G.; Hodges, P.W.; Vicenzino, B. The psychological features of patellofemoral pain: A systematic review. Br. J. Sports Med. 2017, 51, 732–742. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.; Putukian, M.; Aerni, G.; Diamond, A.; Hong, G.; Ingram, Y.; Reardon, C.L.; Wolanin, A. Mental health issues and psychological factors in athletes: Detection, management, effect on performance and prevention: American Medical Society for Sports Medicine Position Statement—Executive Summary. Br. J. Sports Med. 2020, 54, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Hays, K.; Thomas, O.; Maynard, I.; Bawden, M. The role of confidence in world-class sport performance. J. Sports Sci. 2009, 27, 1185–1199. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Alonso, J.M.; Junge, A.; Renström, P.; Engebretsen, L.; Mountjoy, M.; Dvorak, J. Sports Injuries Surveillance During the 2007 IAAF World Athletics Championships. Clin. J. Sport Med. 2009, 19, 26–32. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63 (Suppl. S1), S240–S252. [Google Scholar] [CrossRef]
- Glazer, D.D. Development and Preliminary Validation of the Injury-Psychological Readiness to Return to Sport (I-PRRS) Scale. J. Athl. Train. 2009, 44, 185–189. [Google Scholar] [CrossRef]
- Sala-Barat, E.; Alvarez-Diaz, P.; Montes-Hidalgo, J.; Steinbacher, G.; Alentorn-Geli, E.; Rius, M.; Grossi, S.; Barastegui, D.; Cugat-Bertomeu, R.; Tomás-Sábado, J. The Spanish Version of the Injury-Psychological Readiness to Return to Sport Scale. In Football Medicine Meets the Universe of Sport, Proceedings of the XXVIII Isokinetic Medical Group Conference, London, UK, 27–29 April 2019; Calzetti Mariucci: Torgiano, Italy, 2019. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: New York, NY, USA, 2013; ISBN 978-1-13474-270-7. [Google Scholar]
- Sala-Barat, E.; Álvarez-Díaz, P.; Alentorn-Geli, E.; Webster, K.E.; Cugat, R.; Tomás-Sabado, J. Translation, cross-cultural adaptation, validation, and measurement properties of the Spanish version of the anterior cruciate ligament-return to sport after injury (ACL-RSI-Sp) scale. Knee Surg. Sport. Traumatol. Arthrosc. 2020, 28, 833–839. [Google Scholar] [CrossRef]
- Fischerauer, S.F.; Talaei-Khoei, M.; Bexkens, R.; Ring, D.C.; Oh, L.S.; Vranceanu, A.-M. What Is the Relationship of Fear Avoidance to Physical Function and Pain Intensity in Injured Athletes? Clin. Orthop. Relat. Res. 2018, 476, 754–763. [Google Scholar] [CrossRef]
- Bascour-Sandoval, C.; Albayay, J.; Martínez-Molina, A.; Opazo-Sepúlveda, A.; Lacoste-Abarzúa, C.; Bielefeldt-Astudillo, D.; Gajardo-Burgos, R.; Galvéz-García, G. Psychometric Properties of the PCS and the PCS-4 in Individuals with Musculoskeletal Pain. Psicothema 2022, 34, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Buckthorpe, M.; Frizziero, A.; Roi, G.S. Update on functional recovery process for the injured athlete: Return to sport continuum redefined. Br. J. Sports Med. 2019, 53, 265–267. [Google Scholar] [CrossRef] [PubMed]
- Serrien, B.; Ooijen, J.; Goossens, M.; Baeyens, J.-P. A Motion Analysis in the Volleyball Spike—Part 2: Coordination and Performance Variability. Int. J. Hum. Mov. Sport. Sci. 2016, 4, 83–90. [Google Scholar] [CrossRef]
- Mayer, S.W.; Queen, R.M.; Taylor, D.; Moorman, C.T.; Toth, A.P.; Garrett, W.E.; Butler, R.J. Functional Testing Differences in Anterior Cruciate Ligament Reconstruction Patients Released Versus Not Released to Return to Sport. Am. J. Sports Med. 2015, 43, 1648–1655. [Google Scholar] [CrossRef]
- Webster, K.E.; Nagelli, C.V.; Hewett, T.E.; Feller, J.A. Factors Associated With Psychological Readiness to Return to Sport After Anterior Cruciate Ligament Reconstruction Surgery. Am. J. Sports Med. 2018, 46, 1545–1550. [Google Scholar] [CrossRef] [PubMed]
- Morrey, M.A.; Stuart, M.J.; Smith, A.M.; Wiese-Bjornstal, D.M. A Longitudinal Examination of Athletes’ Emotional and Cognitive Responses to Anterior Cruciate Ligament Injury. Clin. J. Sport Med. 1999, 9, 63–69. [Google Scholar] [CrossRef]
- Levy, A.R.; Nicholls, A.R.; Polman, R.C.J. Pre-competitive confidence, coping, and subjective performance in sport. Scand. J. Med. Sci. Sports 2011, 21, 721–729. [Google Scholar] [CrossRef]
- De Sire, A.; Marotta, N.; Lippi, L.; Scaturro, D.; Farì, G.; Liccardi, A.; Moggio, L.; Letizia Mauro, G.; Ammendolia, A.; Invernizzi, M. Pharmacological Treatment for Acute Traumatic Musculoskeletal Pain in Athletes. Medicina 2021, 57, 1208. [Google Scholar] [CrossRef]
- Bascour-Sandoval, C.; Norambuena-Noches, Y.; Monrroy-Uarac, M.; Flández-Valderrama, J.; Gálvez-García, G.; Gajardo-Burgos, R. Association between sleep quality and pain in young amateur athletes. Rev. Bras. Med. Esporte 2021, 27, 165–169. [Google Scholar] [CrossRef]
- Conti, C.; di Fronso, S.; Pivetti, M.; Robazza, C.; Podlog, L.; Bertollo, M. Well-Come Back! Professional Basketball Players Perceptions of Psychosocial and Behavioral Factors Influencing a Return to Pre-Injury Levels. Front. Psychol. 2019, 10, 222. [Google Scholar] [CrossRef]
- Carson, F.; Polman, R. Experiences of professional rugby union players returning to competition following anterior cruciate ligament reconstruction. Phys. Ther. Sport 2012, 13, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Dekker, J.; de Groot, V.; Ter Steeg, A.M.; Vloothuis, J.; Holla, J.; Collette, E.; Satink, T.; Post, L.; Doodeman, S.; Littooij, E. Setting meaningful goals in rehabilitation: Rationale and practical tool. Clin. Rehabil. 2020, 34, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Roberts, G.C.; Kristiansen, E. Goal Setting to Enhance Motivation in Sport. In Advances in Motivation in Sport and Exercise; Human Kinetics: Champaign, IL, USA, 2012. [Google Scholar]


{kind=link}
| M ± SD | n (%) | |
|---|---|---|
| Age (years) | 23.70 ± 3.54 | |
| Height (cm) | 192.11 ± 8.48 | |
| Body mass (kg) | 87.70 ± 9.83 | |
| BMI | 23.76 ± 2.18 | |
| Game position | ||
| Setter | 7 (14.89) | |
| Middle blocker | 13 (27.66) | |
| Outside spiker | 9 (19.15) | |
| Spiker | 14 (29.79) | |
| Libero | 4 (8.51) | |
| Dominant hand | ||
| Right | 44 (93.62) | |
| Left | 3 (6.38) | |
| Dominant leg | ||
| Right | 39 (82.98) | |
| Left | 8 (17.02) |
| Item | Md (IQR) |
|---|---|
| 100 (90–100) |
| 90 (60–100) |
| 100 (99–100) |
| 90 (50–100) |
| 85 (60–100) |
| 100 (80–100) |
| I-PRRS total | 54 (46–58) |
| Items | rs (95% CI) | p-Value |
|---|---|---|
| −0.02 (−0.33–0.29) | 0.898 |
| −0.02 (−0.50–0.08) | 0.162 |
| −0.37 (−0.061–−0.12) | 0.003 * |
| −0.24 (−0.53–0.04) | 0.093 |
| −0.54 (−0.78–−0.29) | <0.001 ** |
| 0.01 (−0.31–0.34) | 0.947 |
| I-PRRS total | −0.36 (−0.64–−0.08) | 0.011 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gajardo-Burgos, R.; Valdebenito-Tejos, C.; Gálvez-García, G.; Bascour-Sandoval, C. Pain and Psychological Readiness to Return to Sport in Elite Volleyball Players: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 2492. https://doi.org/10.3390/ijerph20032492
Gajardo-Burgos R, Valdebenito-Tejos C, Gálvez-García G, Bascour-Sandoval C. Pain and Psychological Readiness to Return to Sport in Elite Volleyball Players: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(3):2492. https://doi.org/10.3390/ijerph20032492
Chicago/Turabian StyleGajardo-Burgos, Rubén, Camila Valdebenito-Tejos, Germán Gálvez-García, and Claudio Bascour-Sandoval. 2023. "Pain and Psychological Readiness to Return to Sport in Elite Volleyball Players: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 3: 2492. https://doi.org/10.3390/ijerph20032492
APA StyleGajardo-Burgos, R., Valdebenito-Tejos, C., Gálvez-García, G., & Bascour-Sandoval, C. (2023). Pain and Psychological Readiness to Return to Sport in Elite Volleyball Players: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 20(3), 2492. https://doi.org/10.3390/ijerph20032492