


Knowledge of and Testing Rate for Hepatitis C Infection among the General Public of Saudi Arabia: A Cross-Sectional Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Respondents
3.2. Knowledge of HCV Infection among Respondents
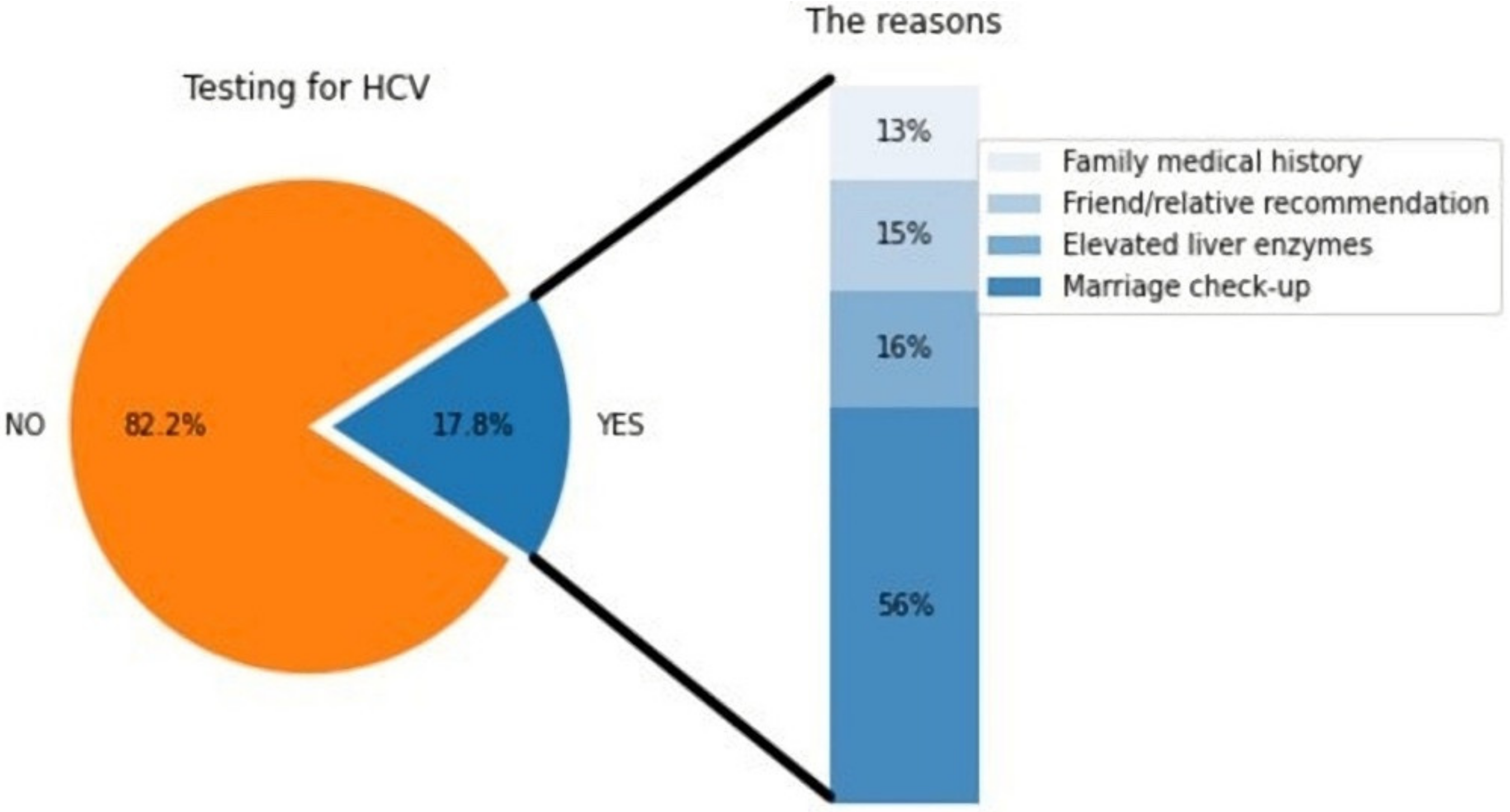
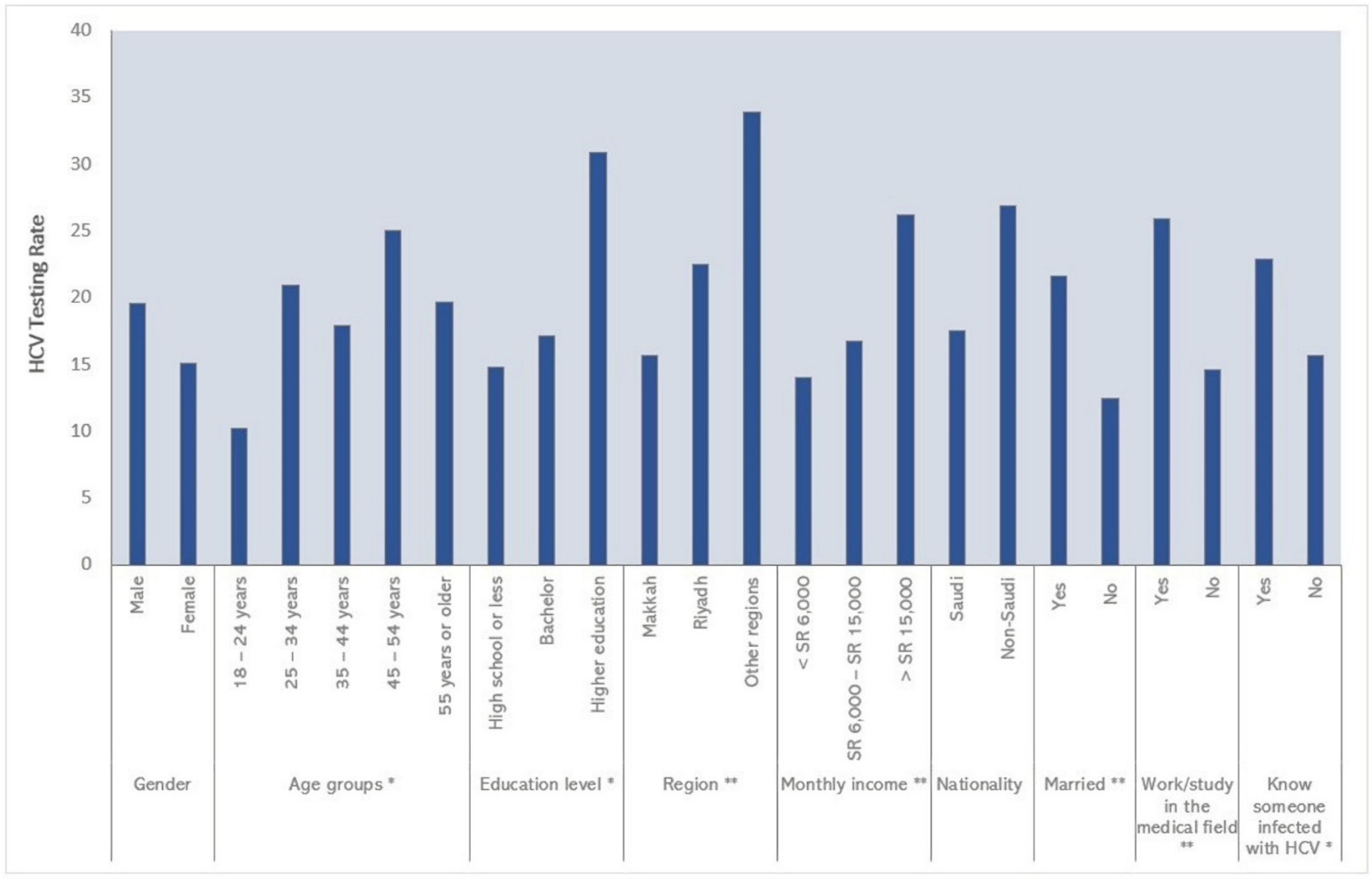
3.3. Testing for HCV among Respondents
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Hepatitis C. 24 June 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-c (accessed on 27 July 2022).
- Moosavy, S.H.; Dvoodian, P.; Nazarnezhad, M.A.; Nejatizaheh, A.; Ephtekhar, E.; Mahboobi, H. Epidemiology, transmission, diagnosis, and outcome of Hepatitis C virus infection. Electron. Physician 2017, 9, 5646–5656. [Google Scholar] [CrossRef] [PubMed]
- Grattagliano, I.; Rossi, A.; Marconi, E.; Lapi, F.; Cricelli, C. Determinants of HCV-related complications in Italian primary care patients. Liver Int. 2021, 41, 2857–2865. [Google Scholar] [CrossRef] [PubMed]
- Tada, T.; Toyoda, H.; Yasuda, S.; Miyake, N.; Kumada, T.; Kurisu, A.; Ohisa, M.; Akita, T.; Tanaka, J. Natural history of liver-related disease in patients with chronic hepatitis C virus infection: An analysis using a Markov chain model. J. Med. Virol. 2019, 91, 1837–1844. [Google Scholar] [CrossRef] [PubMed]
- Madani, T.A. Hepatitis C virus infections reported in Saudi Arabia over 11 years of surveillance. Ann. Saudi Med. 2007, 27, 191–194. [Google Scholar] [CrossRef] [PubMed]
- Bawazir, A.; AlGusheri, F.; Jradi, H.; AlBalwi, M.; Abdel-Gader, A.-G. Hepatitis C virus genotypes in Saudi Arabia: A future prediction and laboratory profile. Virol. J. 2017, 14, 208. [Google Scholar] [CrossRef] [PubMed]
- Abdo, A.A.; Sanai, F.M.; Al-Faleh, F.Z. Epidemiology of viral hepatitis in Saudi Arabia: Are we off the hook? Saudi J. Gastroenterol. 2012, 18, 349–357. [Google Scholar] [CrossRef] [PubMed]
- AASLD/IDSA. HCV Guidance: Recommendations for Testing, Managing, and Treating Hepatitis C. Clin. Liver Dis. 2018, 12, 117. [Google Scholar] [CrossRef]
- Geddawy, A.; Ibrahim, Y.F.; Elbahie, N.M.; Ibrahim, M.A. Direct acting anti-hepatitis C virus drugs: Clinical pharmacology and future direction. J. Transl. Intern. Med. 2017, 5, 8–17. [Google Scholar] [CrossRef] [PubMed]
- Bezemer, G.; Van Gool, A.R.; Verheij-Hart, E.; Hansen, B.E.; Lurie, Y.; Esteban, J.I.; Lagging, M.; Negro, F.; Zeuzem, S.; Ferrari, C.; et al. Long-term effects of treatment and response in patients with chronic hepatitis C on quality of life. An international, multicenter, randomized, controlled study. BMC Gastroenterol. 2012, 12, 11. [Google Scholar] [CrossRef] [PubMed]
- Hebo, H.J.; Gemeda, D.; Abdusemed, K.A. Hepatitis B and C Viral Infection: Prevalence, Knowledge, Attitude, Practice, and Occupational Exposure among Healthcare Workers of Jimma University Medical Center, Southwest Ethiopia. Sci. World J. 2019, 2019, 9482607. [Google Scholar] [CrossRef] [PubMed]
- Sultan, N.Y.; YacoobMayet, A.; Alaqeel, S.A.; Al-Omar, H.A. Assessing the level of knowledge and available sources of information about hepatitis C infection among HCV-infected Egyptians. BMC Public Health 2018, 18, 747. [Google Scholar] [CrossRef] [PubMed]
- Rashrash, M.E.; Maneno, M.K.; Wutoh, A.K.; Ettienne, E.B.; Daftary, M.N. An evaluation of hepatitis C knowledge and correlations with health belief model constructs among African American “baby boomers”. J. Infect. Public Health 2015, 9, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Mtengezo, J.; Lee, H.; Ngoma, J.; Kim, S.; Aronowitz, T.; DeMarco, R.; Shi, L. Knowledge and attitudes toward HIV, hepatitis B virus, and hepatitis C virus infection among health-care workers in Malawi. Asia-Pacific J. Oncol. Nurs. 2016, 3, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Ashri, N. Hepatitis B and C knowledge among Saudi dental patients. Saudi Med. J. 2008, 29, 1785–1790. [Google Scholar] [PubMed]
- Al-Raddadi, R.M.; Dashash, N.A.; Alghamdi, H.A.; Al-Raddadi, Z.M.; Mph, H.S.A.; Alsahafi, A.J.; Algarni, A.M.; Alghamdi, M.M.; Hakim, R.F.; Al-Zalabani, A.H.; et al. Hepatitis C virus infection in Jeddah city, Saudi Arabia: Seroprevalence and knowledge. J. Med. Virol. 2017, 90, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health Saudi Arabia. MOH Calls for Hepatitis C Screening Initiative. MOH Portal. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/news-2018-04-26-010.aspx (accessed on 25 September 2022).
- Pourhoseingholi, M.A.; Vahedi, M.; Rahimzadeh, M. Sample size calculation in medical studies. Gastroenterol. Hepatol. Bed Bench 2013, 6, 14–17. [Google Scholar] [PubMed]
- Ministry of Health Saudi Arabia. (MOH): National Program to Eradicate HCV and Achieve the Global Objective. MOH Portal. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/news-2018-04-09-001.aspx (accessed on 25 September 2022).
- Alotaibi, B.S.; Althobaiti, M.A.; Hazazi, A.Y.; Hazazi, S.Y.; Nassir, R.A.; Alhaddad, M.S.; Abdelwahab, S.F. Exploration of Knowledge, Attitude, and Practice Among Residents of Saudi Arabia Toward Hepatitis Viruses. Inq. J. Health Care Organ. Provis. Financ. 2021, 58, 00469580211059965. [Google Scholar] [CrossRef] [PubMed]
- Alhedyan, F.S.; Alqhtani, N.; Alharbi, A.R.; Alasimi, K.S.; Alomran, A.I.; Aldibas, A.O.; Alotibi, A.M. Knowledge and Attitude of Dental Students and Interns in Saudi Arabia (Riyadh Region) among Hepatitis C Virus Infection. J. Pharm. Res. Int. 2021, 33, 13–26. [Google Scholar] [CrossRef]
- Saudi Women, The Partner of Success. General Authority of Statistics in Saudi Arabia. 2020. Available online: https://www.stats.gov.sa/sites/default/files/woman_international_day_2020.pdf (accessed on 30 September 2022).
- Altraif, I. Can hepatitis C virus be eliminated by 2030? Saudi Arabia as an example. Saudi Med. J. 2018, 39, 842–845. [Google Scholar] [CrossRef] [PubMed]
- Alharbi, I.M.; Aljarallah, B.M. Premarital hepatitis screening. Saudi Med. J. 2018, 39, 1179–1185. [Google Scholar] [CrossRef] [PubMed]
- Eliminate Hepatitis: WHO. Available online: https://www.who.int/news/item/27-07-2017-eliminate-hepatitis-who (accessed on 17 September 2022).



{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Gender | |
| Male | 424 (61.54) |
| Female | 265 (38.46) |
| Age, mean ± SD | 34.1 ± 11.9 |
| Age groups | |
| 18–24 years | 186 (27) |
| 25–34 years | 163 (23.66) |
| 35–44 years | 156 (22.64) |
| 45–54 years | 108 (15.67) |
| 55 years or older | 76 (11.03) |
| Education level | |
| High school or less | 176 (25.54) |
| Bachelor | 445 (64.59) |
| Higher education | 68 (9.87) |
| Region | |
| Makkah | 562 (81.57) |
| Riyadh | 71 (10.3) |
| Other regions | 56 (8.13) |
| Marital status | |
| Single | 271 (39.33) |
| Married | 402 (58.35) |
| Divorced | 14 (2.03) |
| Widowed | 2 (0.29) |
| Monthly income | |
| <SR 6000 | 285 (41.36) |
| SR 6000–SR 15,000 | 240 (34.83) |
| >SR 15,000 | 164 (23.80) |
| Nationality (Saudi) | 663 (96.23) |
| Work/study in the medical field (Yes) | 197 (28.60) |
| Know someone infected with HCV (yes) | 210 (30.50) |
| Ever heard of HCV infection (Yes) | 604 (88) |
| Self-reported HCV infection diagnosis (Yes) | 9 (1.31) |
| Item No. | Item | Responses | ||
|---|---|---|---|---|
| Yes | No | Don’t Know | ||
| 1 | A person with hepatitis C can live for | 277 * | 179 | 233 |
| years without symptoms or health problems | (40.2%) | (25.9%) | (33.8%) | |
| 2 | Hepatitis C can cause other diseases | 447 * | 36 | 206 |
| such as liver cirrhosis and liver cancer | (64.8%) | (5.2%) | (29.9%) | |
| 3 | Hepatitis C can be transmitted through | 482 * | 56 | 151 |
| blood transfusion from an infected person | (69.9%) | (8.1%) | (21.9%) | |
| 4 | This disease can be passed on via sex | 262 * | 209 | 218 |
| with an infected person | (38%) | (30.3%) | (31.6%) | |
| 5 | This disease can be spread through | 361 * | 115 | 213 |
| cupping or piercing | (52.4%) | (16.7%) | (30.9%) | |
| 6 | This disease can be transmitted by using personal hygiene products from an infected person, such as toothbrushes and razors | 394 * (57.1%) | 132 (19.2%) | 163 (23.7%) |
| 7 | It is possible to transmit the disease through a casual contact with an infected person such as shaking hands | 32 (4.6%) | 514 * (74.6%) | 143 (20.7%) |
| 8 | It is possible to transmit the disease through an infected mother to her child during childbirth | 240 * (34.8%) | 163 (23.6%) | 286 (41.5%) |
| 9 | There is a vaccine for hepatitis C | 333 | 135 * | 221 |
| (48.3%) | (19.6%) | (32.1%) | ||
| 10 | Hepatitis C can be completely cured | 326 * | 103 | 260 |
| with medications | (47.3%) | (14.9%) | (37.7%) | |
| Characteristics | HCV Knowledge Levels | ||
|---|---|---|---|
| Low Knowledge (Score ≤ Median), n (%) | High Knowledge (Score > Median), n (%) | p | |
| Overall | 370 (53.7) | 319 (46.3) | - |
| Gender | 0.021 | ||
| Male | 213 (50.2) | 211 (49.8) | |
| Female | 157 (59.3) | 108 (40.7) | |
| Age groups | 0.886 | ||
| 18–24 years | 95 (51.1) | 91 (48.9) | |
| 25–34 years | 86 (52.8) | 77 (47.2) | |
| 35–44 years | 88 (56.4) | 68 (43.5) | |
| 45–54 years | 59 (54.6) | 49 (45.4) | |
| 55 years or older | 42 (55.3) | 34 (44.7) | |
| Education level | <0.001 | ||
| High school or less | 118 (67.1) | 58 (32.9) | |
| Bachelor | 223 (50.1) | 222 (49.9) | |
| Higher education | 29 (42.7) | 39 (57.3) | |
| Region | 0.148 | ||
| Makkah | 311 (55.3) | 251 (44.7) | |
| Riyadh | 35 (49.3) | 36 (50.7) | |
| Other regions | 24 (42.9) | 32 (57.1) | |
| Marital status | 0.019 | ||
| Married | 231 (57.5) | 171 (42.5) | |
| Single\Divorced\Widowed | 139 (48.4) | 148 (51.6) | |
| Monthly income | 0.014 | ||
| <SR 6000 | 169 (59.3) | 116 (40.7) | |
| SR 6000–SR 15,000 | 127 (52.9) | 113 (47.1) | |
| >SR 15,000 | 74 (45.1) | 90 (54.9) | |
| Nationality | 0.987 | ||
| Saudi | 356 (53.7) | 307 (46.3) | |
| Non-Saudi | 14 (53.9) | 12 (46.1) | |
| Work/study in the medical field | <0.001 | ||
| Yes | 56 (28.4) | 141 (71.6) | |
| No | 314 (63.8) | 178 (36.2) | |
| Know someone infected with HCV | <0.001 | ||
| Yes | 85 (40.5) | 125 (59.5) | |
| No | 285 (59.5) | 194 (40.5) | |
| Tested for HCV | <0.001 | ||
| Yes | 42 (34.2) | 81 (65.8) | |
| No | 328 (57.9) | 238 (42.1) | |
| Characteristics | Unadjusted OR [95% CI] | p | Adjusted OR [95% CI] | p |
|---|---|---|---|---|
| Gender | ||||
| Male | Ref. | Ref. | ||
| Female | 1.44 [1.06–1.96] | 0.021 | 1.01 [0.69–1.46] | 0.942 |
| Age groups | ||||
| 18–24 years | Ref. | Ref. | ||
| 25–34 years | 1.07 [0.70–1.63] | 0.726 | 1.19 [0.69–2.05] | 0.239 |
| 35–44 years | 1.24 [0.81–1.90] | 0.518 | 0.79 [0.38–1.66] | 0.331 |
| 45–54 years | 1.15 [0.72–1.85] | 0.887 | 0.81 [0.34–1.89] | 0.704 |
| 55 years or older | 1.18 [0.69–2.02] | 0.801 | 0.93 [0.38–2.34] | 0.49 |
| Education level | ||||
| Higher education | Ref. | Ref. | ||
| Bachelor | 1.35 [0.81–2.26] | 0.246 | 1.21 [0.67–2.18] | 0.586 |
| High school or less | 2.74 [1.54–4.85] | <0.001 | 1.82 [0.95–3.46] | 0.03 |
| Region | ||||
| Riyadh and other regions | Ref. | Ref. | ||
| Makkah | 1.43 [0.97–2.10] | 0.071 | 1.13 [0.72–1.75] | 0.6 |
| Marital status | ||||
| Single\Divorced\Widowed | Ref. | Ref. | ||
| Married | 1.44 [1.06–1.95] | 0.019 | 1.66 [0.94–2.92] | 0.08 |
| Monthly income | ||||
| >SR 15,000 | Ref. | Ref. | ||
| SR 6000–SR 15,000 | 1.37 [0.92–2.04] | 0.870 | 1.36 [0.85–2.17] | 0.598 |
| <SR 6000 | 1.77 [1.20–2.61] | 0.008 | 2.27 [1.29–4.01] | 0.005 |
| Nationality | ||||
| Saudi | Ref. | Ref. | ||
| Non-Saudi | 1.01 [0.46–2.21] | 0.987 | 0.94 [0.37–2.34] | 0.893 |
| Work/study in the medical field | ||||
| Yes | Ref. | Ref. | ||
| No | 4.44 [3.09–6.36] | <0.001 | 4.28 [2.80–6.53] | <0.001 |
| Know someone infected with HCV | ||||
| Yes | Ref. | Ref. | ||
| No | 2.16 [1.55–3.01] | <0.001 | 2.26 [1.56–3.26] | <0.001 |
| Tested for HCV | ||||
| Yes | Ref. | Ref. | ||
| No | 2.66 [1.77–3.99] | <0.001 | 2.19 [1.39–3.44] | 0.001 |
| Characteristics | Unadjusted OR [95% CI] | p | Adjusted OR [95% CI] | p |
|---|---|---|---|---|
| Gender | ||||
| Male | Ref. | Ref. | ||
| Female | 0.73 [0.48–1.10] | 0.136 | 1.05 [0.65–1.70] | 0.829 |
| Age groups | ||||
| 18–24 years | Ref. | Ref. | ||
| 25–34 years | 2.32 [1.26–4.24] | 0.344 | 1.82 [0.89–3.72] | 0.244 |
| 35–44 years | 1.92 [1.03–3.59] | 0.941 | 1.24 [0.47–3.22] | 0.553 |
| 45–54 years | 2.93 [1.54–5.57] | 0.043 | 1.75 [0.64–4.75] | 0.405 |
| 55 years or older | 2.16 [1.03–4.52] | 0.676 | 1.46 [0.49–4.34] | 0.93 |
| Education level | ||||
| Higher education | Ref. | Ref. | ||
| Bachelor | 0.46 [0.26–0.81] | 0.153 | 0.67 [0.35–1.28] | 0.757 |
| High school or less | 0.39 [0.20–0.75] | 0.029 | 0.53 [0.25–1.09] | 0.117 |
| Region | ||||
| Riyadh and other regions | Ref. | Ref. | ||
| Makkah | 0.49 [0.31–0.77] | 0.002 | 0.59 [0.36–0.97] | 0.038 |
| Marital status | ||||
| Single\Divorced\Widowed | Ref. | Ref. | ||
| Married | 1.93 [1.26–2.93] | 0.002 | 2.45 [1.20–4.96] | 0.013 |
| Monthly income | ||||
| >SR 15,000 | Ref. | Ref. | ||
| SR 6000–SR 15,000 | 0.56 [0.35–0.92] | 0.381 | 0.74 [0.42–1.28] | 0.216 |
| <SR 6000 | 0.45 [0.28–0.74] | 0.02 | 0.96 [0.49–1.90] | 0.698 |
| Nationality | ||||
| Saudi | Ref. | Ref. | ||
| Non-Saudi | 1.74 [0.71–4.22] | 0.223 | 1.59 [0.58–4.38] | 0.366 |
| Work/study in the medical field | ||||
| No | Ref. | Ref. | ||
| Yes | 2.04 [1.36–3.05] | 0.001 | 2.19 [1.31–3.69] | 0.003 |
| Know someone infected with HCV | ||||
| No | Ref. | Ref. | ||
| Yes | 1.59 [1.06–2.39] | 0.024 | 1.09 [0.70–1.71] | 0.682 |
| HCV knowledge level | ||||
| High | Ref. | Ref. | ||
| Low | 0.38 [0.25–0.56] | <0.001 | 0.47 [0.29–0.74] | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzahrani, M.S.; Ayn Aldeen, A.; Almalki, R.S.; Algethami, M.B.; Altowairqi, N.F.; Alzahrani, A.; Almalki, A.S.; Alzhrani, R.M.; Algarni, M.A. Knowledge of and Testing Rate for Hepatitis C Infection among the General Public of Saudi Arabia: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2023, 20, 2080. https://doi.org/10.3390/ijerph20032080
Alzahrani MS, Ayn Aldeen A, Almalki RS, Algethami MB, Altowairqi NF, Alzahrani A, Almalki AS, Alzhrani RM, Algarni MA. Knowledge of and Testing Rate for Hepatitis C Infection among the General Public of Saudi Arabia: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2023; 20(3):2080. https://doi.org/10.3390/ijerph20032080
Chicago/Turabian StyleAlzahrani, Mohammad S., Abdullah Ayn Aldeen, Rayan S. Almalki, Mohammed B. Algethami, Nawaf F. Altowairqi, Ammar Alzahrani, Ahmed S. Almalki, Rami M. Alzhrani, and Majed A. Algarni. 2023. "Knowledge of and Testing Rate for Hepatitis C Infection among the General Public of Saudi Arabia: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 20, no. 3: 2080. https://doi.org/10.3390/ijerph20032080
APA StyleAlzahrani, M. S., Ayn Aldeen, A., Almalki, R. S., Algethami, M. B., Altowairqi, N. F., Alzahrani, A., Almalki, A. S., Alzhrani, R. M., & Algarni, M. A. (2023). Knowledge of and Testing Rate for Hepatitis C Infection among the General Public of Saudi Arabia: A Cross-Sectional Study. International Journal of Environmental Research and Public Health, 20(3), 2080. https://doi.org/10.3390/ijerph20032080