Abstract
Background: Blood flow restriction is characterized as a method used during exercise at low loads of around 20–40% of a repetition maximum, or at a low-moderate intensity of aerobic exercise, in which cuffs that occlude the proximal part of the extremities can partially reduce arterial flow and fully restrict the venous flow of the musculature in order to achieve the same benefits as high-load exercise. Objective: The main objective of this systematic literature review was to analyze the effects of BFR intervention on pain, functionality, and quality of life in subjects with neuromusculoskeletal pathologies. Methods: The search to carry out was performed in PubMed, Cochrane, EMBASE, PEDro, CINHAL, SPORTDiscus, Trip Medical Database, and Scopus: “kaatsu” OR “ischemic training” OR “blood flow restriction” OR “occlusion resistance training” OR “vascular occlusion” OR “vascular restriction”. Results: After identifying 486 papers and eliminating 175 of them due to duplication and 261 after reading the title and abstract, 50 papers were selected. Of all the selected articles, 28 were excluded for not presenting a score equal to or higher than 6 points on the PEDro scale and 8 for not analyzing the target outcome variables. Finally, 14 papers were selected for this systematic review. Conclusions: The data collected indicate that the blood flow restriction tool is a therapeutic alternative due to its effectiveness under different exercise modalities. The benefits found include decreases in pain thresholds and improvement in the functionality and quality of life of the neuro-musculoskeletal patient during the first six weeks. However, the results provided by this tool are still not clear for medium- and long-term interventions.
1. Introduction
Currently, there are different strategies to restrict blood flow before or during exercise seeking to improve performance such as remote ischemic preconditioning or blood flow restriction (BFR).The term remote ischemic preconditioning refers to a type of blood flow restriction focused on sport performance where the cuffs are inflated and deflated during sets [1]. Second, BFR could be considered as a training adjuvant that in recent years has been used during physical exercise at low intensities during strength training (around 20–40%) or at low or medium intensities during aerobic exercise with the intention of improving cardiopulmonary capacities. In [2], in which cuffs that occlude the proximal part of the extremities can partially reduce arterial flow and fully restrict venous flow of the musculature in order to achieve the same benefits as high-load exercise [2,3]. Several theories attempt to justify the results obtained from BFR intervention. One of these theories considers that the metabolic effects of induced hypoxia cause a higher amount of lactate [4], reactive oxygen free radicals, and nitrogen oxide [5], which lead to an increase in protein synthesis and the recruitment of muscle fibers as well as to a decrease in proteolysis [6]. On the other hand, the effects of BFR intervention may be due to neuromuscular and hormonal reactions, given that the cuff pressure, between 50 and 230 mm Hg, induces a greater muscle activation [7,8], and even a greater secretion of the growth hormone IGF-1 depending on the pressure applied by the cuff [9].
In rehabilitation, the working methodologies employed are heterogeneous in terms of the occlusion measurement used, arterial occlusion pressure or limb occlusion pressure, differences in the material used, cuff amplitude, amount of pressure applied, and the type of training [10,11].
Currently, it has been analyzed whether BFR intervention is capable of directly influencing other variables such as pain, functionality, and quality of life, obtaining favorable results that indicate that this technique can improve, above all, the intensity of pain and the ability to perform activities of daily living [12]. Although there are many systematic reviews that analyze the effect of BFR intervention [3,13,14,15,16,17,18,19,20,21], no systematic review has been found that analyzes the effect of BFR intervention on subjective and objective variables in the short-, medium-, and long-term in patients suffering from neuromusculoskeletal pathologies. Thus, to date, and to the best of our knowledge, no review has analyzed how BFR intervention can directly contribute to these variables in the rehabilitation area. The main objective of this systematic literature review was to analyze the effects of BFR intervention on pain, functionality, and quality of life in subjects with neuro-musculoskeletal pathologies.
2. Methods
A systematic review was carried out using the guidelines of the PRISMA checklist system.
2.1. Search Strategy
The search to carry out this systematic review was performed in different Health Sciences databases (PubMed, Cochrane, EMBASE, CINHAL, SPORTDiscus, Trip Medical Database, Scopus) using the terms: “kaatsu” OR “ischemic training” OR “blood flow restriction” OR “occlusion resistance training” OR “vascular occlusion” OR “vascular restriction”. The search included all the articles published up to 31 October 2022, which were subsequently evaluated [22].
2.2. Selection of Documents
This study included articles that were designed as a randomized clinical trial, whose objective was to evaluate therapeutic exercise in combination with blood flow restriction on subjects with neurological and musculoskeletal pathologies, and that were published up to 31 October 2022. For inclusion, the studies had to present at least one intervention or control group in which the BFR intervention was applied.
Studies not published in master theses, case reports, reviews, cross-sectional studies, and cohort studies were excluded. The PEDro scale considers that studies with a score of less than 6 points present a sufficient or poor methodological quality, thus they were excluded [23].
2.3. Selection Method
In parallel and blinded, two researchers conducted a search of the scientific literature in the different databases and selected the documents applying the inclusion and exclusion criteria set out above. After reviewing the articles in the different databases, all those that were duplicates were discarded. In the case of discrepancy, the paper selection was performed by a third blinded researcher. Once the articles were selected, their internal validity was assessed using the PEDro scale.
2.4. Methodological Quality
The methodological quality of the randomized clinical trials was assessed using the PEDro rating scale. This scale consists of 11 questions, of which 10 were scored by a dichotomous answer (Yes/No), which was awarded on the basis of meeting the requirements of the specified section. The unscored question was discarded due to influences of external validity and not internal or statistical validity of the trial [24].
2.5. Outcomes
The outcome variables involved in the analysis of the selected studies were pain, functionality, and quality of life. The pain variable should be understood from a more global perspective such as the biopsychosocial one apart from purely biological damage such as nociceptive or neuropathic pain [25].
Functionality is understood as the individual’s ability to move around in different types of environments with total safety and independence in order to be able to perform all of the tasks that are part of the person’s activities of daily living in any context [26]. On the other hand, quality of life is defined as the state of life perceived by the individual regarding the impact of their pathology and the treatment performed on their disability and daily functionality [27].
Likewise, a time continuity model was established for the analysis of the results of the study. In order to compare the results between the different studies, the results were standardized on a scale from 0 to 100.
Data were collected at the baseline, short- (0–6 weeks), medium- (6–12 w), and long-term (12–24 w), and the follow-up period as the post-treatment period.
3. Results
After identifying 486 papers in the different databases, and eliminating 175 of them due to duplication and 261 after reading the title and abstract, 50 papers were selected. Of all the selected articles, 28 were excluded for not presenting a score equal to or higher than 6 points on the PEDro scale and 8 for not analyzing the target outcome variables. Finally, 14 papers were selected for this systematic review (Figure 1).
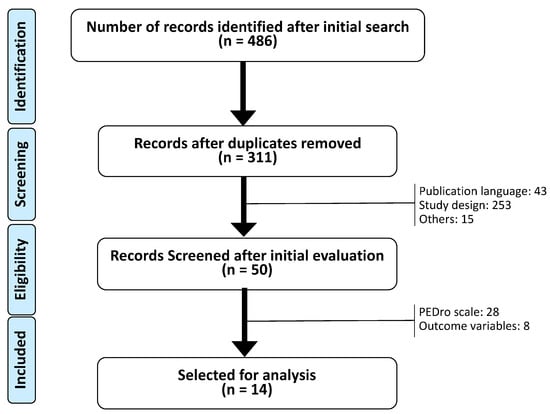
Figure 1.
Flowchart CONSORT.
Table 1 shows the structural characteristics of the different studies selected. The total sample of all the studies included in this study was 533 patients (Table 1) with a minimum of 22 patients [28] and a maximum of 79 [29], with a mean age of 44.5 years, ranging from 14 [30] to 75 years [28]. The different types of interventions employed were aerobic exercise [31] and strength exercise [29]. In the selected papers, the session frequencies ranged from one to three sessions per week [31,32], while the intervention duration ranged from one session [32] to 16 weeks [29].

Table 1.
Results of the internal assessment of the documents selected according to the PEDro scale.
3.1. Functionality (Objective Outcomes)
Table 2 shows all the studies that assessed the functionality outcome from an objective point of view. For the outcome variable “time”, a mean of 6.87 s with a minimum of 5.5 s and a maximum of 8.25 s was recorded in the Time Up and Go Test, showing similarities between the results of both studies that used this tool [33,40]; in the variable “distance”, a mean of 367 m was obtained, with a minimum of 120 m and a maximum of 614 m, showing differences between the beginning and the end of the intervention of the two studies that employed this instrument [31,38]; in the variable “repetitions”, a mean of 14.65 repetitions was obtained, with a difference between 10.5 and 18.8 repetitions, showing similar results [33,40]; and in the variables “speed” and “power”, a direct comparison of the results could not be made, since the corresponding studies used different evaluation tools or presented a single study for the outcome variable. In general, all of the studies collected results during the first 3 months of the intervention and did not perform a post-intervention follow-up, except for the studies by Lamberti et al. and Segal et al. [38,41], who continued to collect data at a 3-month follow-up interval.
Table 2.
Characteristics of the studies included in this systematic review.
3.2. Functionality (Subjective Outcomes)
Table 3 presents the results related to functionality extracted from the selected studies. Up to 10 assessment tools were used such as the Short Physical Performance Battery, Late Life Function and Disability Instrument [35], International Knee Documentation Committee [30,37], Lysholm Knee-Scoring Scale, Tegner Activity Scale, Knee Osteoarthritis Outcome Score, Lower Extremity Function Scale [37], Inclusion Body Myositis Functional Rating Scale [28], Health Assessment Questionnaire [28,40], and Berg Balance Scale [38]. In the different tools, the International Knee Documentation Committee stood out, with a mean score of 26.88 and values between 6.08 and 42.69 points, in which the results of both studies reflect the disparity [30,37], which occurs in the Health Assessment Questionnaire, which presents a mean value of 1.03 points, with a minimum of 0.16 and a maximum of 1.9 points [28,40]. The results of all of the studies were collected in the first 3 months of the intervention, since most of them did not present a follow-up like the studies by Lamberti et al. and Segal et al. [38,41].
Table 3.
Results of the functionality variable (objective outcomes), analyzed in the short-, medium- and long-term, both during the intervention period and in a follow-up that could be longer than 6 months after the end of the intervention.
3.3. Pain
Regarding the outcome variable “pain”, Table 4 shows eight assessment tools. Among the different measurement instruments, the questionnaires with the highest frequency of use are the Kujala Patellofemoral Score, with an average value of 44.33 between 0 and 88.7 points [41,42,43], and the Visual Analogue Scale with an average score of 42.85, a minimum of 0 points, and a maximum of 85.7 points [29,35,40]. All of the studies collected data during the first 3 months of the intervention, and only five studies carried out a follow-up 3 months after the intervention.
Table 4.
Functionality (subjective outcomes) analyzed in the short-, medium-, and long-term, both during the intervention period and in a follow-up that could be longer than 6 months after the end of the intervention.
3.4. Quality of Life
Data were collected from four assessment tools (Table 5), showing less heterogeneity among the results. Likewise, the results obtained in the different studies were collected up to 3 months after the intervention (follow-up), and only two studies [28,38] evaluated the data after the intervention in up to 3 months of follow-up, where the Short Form-36 Health Survey stands out with a mean of 57.35 points, whose minimum and maximum values were 14.7 and 100 points, respectively, although with differences in the collection of results, recording them globally or by areas, and showing a lack of homogeneity among the results [33].
Table 5.
Pain analyzed in the short-, medium-, and long-term, both during the intervention period and in a follow-up that could be longer than 6 months after the end of the intervention.
4. Discussion
Based on the results of this systematic review analyzing the effects of BFR intervention and different exercise methodologies, it appears that there is a favorable trend of BFR intervention in the short-term for each of the aforementioned variables despite the great heterogeneity of the population groups. This tends to normalize in the medium- and long-term, although there are not enough studies to be consistent. In addition, after analyzing the results presented in this systematic review, it was observed how the use of BFR intervention, as an adjuvant methodology during treatment in patients with neurological or musculoskeletal pathologies, achieved greater or similar benefits compared to high-load exercises in the initial processes of recovery due to the metabolic stress and the lower mechanical stress it induced. In this way, high intensity would be simulated through low load, as long as the treated structure allows for the introduction of BFR intervention as a complement to exercise, although there are aspects that must be analyzed specifically depending on the studied variable.
4.1. Functionality
4.1.1. Time
In terms of the functional outcome time (Table 6), it was observed that the BFR intervention group improved between 2.9 and 6 s in the sit-to-stand 5 times (STS5), performed by patients with pathologies such as multiple sclerosis or knee arthroscopy [38,43]. This difference in the results may indicate that a lower pressure and walking with BFR intervention obtains better results than higher pressures and strength exercises. However, other factors such as the rating of perceived exertion or the total elimination of pressure between exercises could influence the losses in the metabolic effect induced by the BFR intervention [44,45]. Regarding the other tests, there was a trend in favor of the BFR intervention, with a 2 s difference with respect to the control group in the Four Square Step Test (FSST), and 4.4 s in the Timed Stair Ascent (TSA) [43]. One possible consequence is the metabolic stress that the study subjects were subjected to with this tool rather than the mechanical stress provided by high loads [2]. However, mechanical stress may also play a role, as the control group did not add any strength exercise compared to the BFR intervention group, which may benefit from specific metabolic responses when performing the low-load exercises [46].
Table 6.
Quality of life analyzed in the short-, medium-, and long-term, both during the intervention period and in a follow-up that may be longer than 6 months after the end of the intervention.
In the medium-term, intra-group changes of up to 0.75 s are shown in the Time Up and Go Test [33,40]. These improvements were very similar in all intervention groups, even when using different exercise methodologies such as high loads, low loads, or BFR intervention, except for the control group, which did not perform any intervention. This could indicate that the subjects improved, regardless of the metabolic or mechanical stress produced by the exercises [47]. In the long-term, only one study carried out a short-term follow-up in which the improvements obtained were slightly reduced [38].
4.1.2. Speed
With respect to the speed category, in the short-term, benefits were observed in the Timed 25-Foot Walk Test (T25FW) of 0.12 m per second in favor of the BFR intervention group [38]. This difference may be relevant as a change of 15% could be significant [48] and the fact that the control group walked at a high-intensity level controlled by rating perceived exertion. Nonetheless, the intervention group introduced this intensity by metabolic stress with the BFR intervention, and controlled the rests with a metronome, which may have produced better results at the brain level, especially anticipatory motor control [49]. In self-selected walking velocity (SSWV), both groups improved between 0.46 and 0.49 m per second, which may indicate that subjects with knee arthroscopy obtain the same benefits from BFR intervention and mechanical stimulus of the loads [43]. In the same way, similar results were seen in the 400-m-walk gait speed, where the BFR intervention group presented −0.01 m per second, which might explain why they did not achieve enough adaptations [35], regardless of whether exercises with different loads are used, even with the application of BFR intervention [50].
The lack of medium-term changes shown for the 400-m-walk gait speed tool suggests the same aforementioned before [35,51]. Long-term data were only recorded for short-term follow-up, with a decrease of 0.03 m per second for both groups at T25FW [38]. This suggests that BFR intervention, in combination with functional exercise, is maintained over time and is of interest in populations with neurological pathologies, which may have accentuated corticomotor activation after metronome use [52].
4.1.3. Distance
For this category, short-term changes were found in favor of the BFR intervention, with a 49-m difference in the 6-min-walk test [38]. Nevertheless, the BFR intervention and control groups improved regardless of the type of intervention, although the BFR intervention group showed greater benefits, specifically about 17 more meters, suggesting that it is an interesting tool during aerobic exercise, enhancing its main physiological effect [2]. In a similar way, the modified Star Excursion Balance Test (SEBT) showed better results in each of the categories for the BFR intervention group, although these data cannot be assumed to be due to the application of this tool [37]. However, the origin of this improvement may lie in the improvement of the quadriceps muscle activation deficits shown by patients with anterior cruciate ligament reconstruction, thanks to the corticomotor activation of the BFR intervention; even the effects induced by cross-training can improve the functional deficits in both lower limbs [53,54].
The results shown in the modified SEBT are favorable in the medium-term for the BFR intervention group in both healthy and injured limbs, with mean changes of 10.3% and 10.6% in the anterior axis, 10.8% and 13% in the posteromedial axis, and 8.9% and 11.5% in the posterolateral axis, respectively [37]. The improvements presented in the BFR intervention group suggest that the effects of using this tool with low loads are superior, as they introduce less mechanical intensity. This benefit may be given that, in the early phase, the tissue used for anterior cruciate ligament reconstruction does not have sufficient tolerance and adaptation to high loads [55].
In relation to the long-term, only one study using the 6-min-walk test showed that the changes produced during the short-term follow-up were maintained [38]. Thus, BFR intervention could be used as a complement of training to enhance the effects of therapeutic physical exercise in patients with multiple sclerosis, despite being a relative contraindication in neuropathy or spinal cord injury [8].
4.1.4. Other Objective Functional Outcomes
The timed stand test showed a difference of up to 2.25 repetitions for the experimental group, which performed exercises with high loads [33,40]. This may explain that the mechanical stress and the progression with loads were better in high loads rather than the metabolic stress induced by BFR intervention. Even so, BFR intervention is therefore considered another alternative to improve in patients with rheumatoid arthritis in the short-term [56,57]. Regarding long-term and follow-up, no results were shown.
According to the outcome “power”, this only presented data in the short-term follow-up, showing a mean difference of 53.4 watts in the stair climb power in favor of the control group [41]. One possible cause could be the use of different pressures throughout the trial, and the other might be the degree of occlusion controlled by a Doppler ultrasound, which could not reach the necessary parameters to create adaptations in terms of the metabolic stress required [45].
4.2. Subjective Functionality
According to the subjectivity of functionality, the Berg Balance Scale (BBS) showed an increase of two points in both groups in the short-term [38]. This indicates that BFR intervention provides the same benefits as a functional activity, as both work at aerobic thresholds.
In the medium-term, differences of 0.8 points were found in the BFR intervention group for the Short Physical Performance Battery [35]. This datum may suggest that the use of this tool may be beneficial in the early stages, instead of using high loads due to the control and progression in the degree of occlusion between sessions using systolic blood pressure and thigh thickness as a reference [58]. The Health Assessment Questionnaire (HAQ) showed a mean difference of 0.05 points in favor of the BFR intervention compared to doing nothing or training with high loads [40]. It is possible that muscle hypertrophy due to the effect of active hyperemia during BFR intervention sessions is interacting with the benefits obtained or unknown physiological mechanisms [59]. For the Late Life Function and Disability Instrument (LLFDI), data of −0.5 points in a total frequency for the BFR intervention group and one point in total limitation for the control group were achieved, thus both high loads and BFR intervention may provide the same benefits in rheumatoid arthritis [40]. In fact, this may be a consequence of the work proposed in the endurance strength groups, where the aerobic threshold can be reached, which is beneficial for the pathology [56].
Relative to the changes shown between the short- and medium-term, intra-group differences of 13.19 points were found for the BFR intervention group in the International Knee Documentation Committee (IKDC), thus we could assert that the younger the person, the greater the adaptation to this tool [37]. It should be noted that BFR intervention was used with high loads instead of low loads, and with high pressures, generating greater stress on the tissue and at a central level, which can influence muscle fatigue and, in turn, increase muscle thickness [60]. The BFR intervention group improved function by 14.81 points on the Lower Extremity Function Scale (LEFS) and 14.83 on the Lysholm Knee-Scoring Scale as a result of better adaptation to low loads. However, the Knee Osteoarthritis Outcome Score (KOOS) showed benefits in the control group for pain with 10.33 points, and symptoms with 12.33 points, and in the BFR intervention group for activities of daily living with 10.5 points, and quality of life with 14.38 points [37,39]. Despite these data, the differences between high loads or low loads with BFR intervention were not large, providing the same benefits for functionality in anterior cruciate ligament reconstruction.
No long-term data were recorded, as with the Tegner Activity Scale, which does not collect data at any time except for the initial assessment and with homogeneous results [37]. In the short-term follow-up, the BBS did not change independently of the intervention [38]. According to the IBMFRS, the control group decreased both sections by up to 17 points compared to the BFR intervention group, which could be due to the fact that they did not perform any particular activity [28] or that the level of self-efficacy was maintained in those patients who practiced exercise [61]. The same is true for the medium-term follow-up where the control group improved compared to the BFR intervention group by 11 points [39]. This may be due to the loss of BFR intervention properties such as metabolic stress when this adjuvant treatment is withdrawn, despite continued exercise [62].
4.3. Pain
For the pain outcome, short-term changes of 5.6 points were shown for the control group in the KOOS [42]. Perhaps the lack of specificity in applying the necessary pressure to occlude the artery is not enough to create adaptations in the subject as well as to work on progression [58]. Furthermore, another study showed changes for the BFR intervention group of 13.2 points in the pain section, up to 30 points in the symptoms and activities of daily living section, 28 points in the quality of life section, and 37.5 points in the sport section [43]. This suggests that strength training, especially low-load strength training in conjunction with BFR intervention, may be vital for patients with knee arthroscopy to increase the pain threshold [63]. Likewise, a mean decrease in pain was found on the Numeric Pain Rating Scale (NPRS) in favor of the BFR intervention group of 2.6 points in single leg squat shallow, 2.7 points in single leg squat deep, and 2 points in the side-down test [32]. The decrease in both groups may have been due to the use of the metronome [64] as it modulates tendon pain and corticospinal control of the muscle, especially in the BFR intervention group, where the perception of pain due to cuff pressure was altered [65]. The same was true for the Kujala Patellofemoral Score, where both groups improved equally by around 20–22 points, with the BFR intervention group being slightly higher by almost two points [34]. One consequence of both groups obtaining similar values may be evidence that an exercise program focused on the hip and knee favors the perception of pain intensity [66].
In the medium-term, there was an average improvement of 22.3–26.6 mm in the Visual Analogue Scale (VAS) [29,40] and almost 13 points in the Kujala Patellofemoral Scale [29] in BFR intervention group. The BFR intervention application was superior to high loads in reducing the sensation of pain in subjects of different ages with knee pathologies such as rheumatoid arthritis, knee osteoarthritis, and patellofemoral pain. This finding might be related to the application of high pressures with the cuff, which induces the hypoalgesia mechanism during exercise, thereby increasing the pain threshold [57]. For the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain subscale, changes of almost seven points were observed for the control group [35]. Nevertheless, the BFR intervention group did not differ much from the results obtained in the control group, thus performing resistance training at moderate intensity and low-load exercises with BFR intervention obtained the same results for knee osteoarthritis, indicating that BFR intervention is a good alternative to improving strength and functionality with lower pain sensation [67].
Between the short- and medium-term, the Pain Börg Scale reports changes in muscle soreness in the BFR intervention group of 0.25 points for the injured leg and 0.7 points for the uninjured leg, while the experimental group improved in the knee soreness scores by 1.3 points for the injured leg and 3.3 points for the uninjured leg [36]. This indicates that the BFR intervention and high-load groups are compatible in accelerating the recovery process in patients with an anterior cruciate ligament reconstruction and decreasing the level of pain. The BFR intervention group would generate this through cuff pressure, metabolic stress, and lower loads, while the control group would use higher mechanical stress [68].
In the long-term, no data were collected for the pain variable, although data were collected for the short- and medium-term post-intervention follow-up, all groups maintained the improvements obtained, with a slight increase in pain for the BFR intervention group in one study [29]. Perhaps this phenomenon could be due to the fact that the subjects could not practice the exercises with this tool once the intervention was over and did not benefit from the effects provided by the exercise practiced in isolation. Along the same lines, the control group improved to a greater extent than the BFR intervention group, with a total benefit of 8.6 points on the KOOS [28]. In the Myositis Damage Index (MDI), the BFR intervention group improved 22.3 points in global patient damage, the control group improved 17 points for global physical damage and, in the global damage section, there was no change for any of the groups [28]. The same was shown for the Kujala Patellofemoral pain, with both groups improving slightly by up to four points [34]. This variation in results may be due to several factors. First, the BFR intervention group improved the global damage section due to the strength exercises. Second, the control group improved the overall physical injury possibly due to a regression to the mean. Finally, none of the groups improved in the global damage section, possibly because there was no progression in the pressures applies by the BFR intervention [45].
4.4. Quality of Life
With regard to the quality of life variable, in the short-term, changes were observed in each of the areas of the Health Questionnaire SF-36, with 10 points in the physical function area, 13 points in bodily pain, foour points in vitality, 13 points in social function, 18 points in emotional role, and 11 points in mental health for the control group whereas the BFR intervention group improved 29 points in the physical role section and six points in general health [38]. However, both groups improved similarly in all sections, which may indicate that aerobic exercise with or without BFR intervention produces the same impact on the subjects’ quality of life, although the application of below-average pressures may have influenced the benefits presented by the BFR intervention, such as metabolic stress [2]. Along the same lines, the Multiple Sclerosis Impact Scale-29 (MSIS-29) showed differences in favor of the control group, especially in the motor area, with a change of 10 points, and, in the psychological area, both groups improved equally by three points [38]. For the Veterans RAND 12-Item Health Survey (VR-12), the BFR intervention group showed changes in the physical area of 15.44 points and 19 points in the mental area [43]. These data may have to do with the fact that the BFR intervention group added strength exercises to the routine of the control group including the use of high pressure with the BFR intervention cuff, which may allow for hypoalgesia and exercise with less pain.
In the medium-term, mean differences in the SF-36 of between 4 and 11 points for the mental area, 10 and 13 points in the physical area, 28 points in the physical role, almost 13 points in bodily pain, more than five points in general health, and around eight points in emotional role were found for the BFR intervention group. In the control group, improvements of almost 10 points were observed in the vitality and social role [33,40]. These results show that all exercise modalities are very interesting options to improve the functional and psychological area of the patient with knee pathology. In addition, improvements of 16.7 points on the WOMAC scale were reported for Experimental group 2 [33]. The use of low-load exercise without BFR was slightly superior to the group using BFR intervention; however, this was not statistically significant.
Although no long-term results were found, short-term data were collected at follow-up, varying slightly from the time of intervention in the case of the SF-36 [28,38], and they were maintained for the study using the MSIS-29. This may suggest that the benefits of the BFR intervention are maintained in the long-term or that patient self-efficacy is high for the intervention program developed by the researchers [61]. Nonetheless, in one of the SF-36 studies, there was heterogeneity between the groups from the beginning, even when performing exercises, possibly due to the lack of transfer of the exercises to the patient’s daily life [69].
4.5. Physical Activity and BFR Intervention
According to the results analyzed from the different studies included in this systematic review, it can be observed how the BFR intervention acts as a therapeutic adjuvant that can be used with different objectives depending on the conditions of the execution of the intervention (including the patient, environment, therapist...). In this sense, it is important to highlight that it is an adjunctive technique to physical exercise, aimed therefore at enhancing the effects of execution in different conditions. An improvement in different functional capacities related to strength and aerobic capacity was observed (Table 3), which was comparable to that produced during physical activity performed at a higher intensity. In this sense, the BFR intervention can be used to “simulate” higher physical capacity intensities when the subject is not capable of working on his own at these intensities. On the other hand, if the subject is capable of working at high intensities, it is possible that the BFR intervention could be an adjuvant that helps to enhance the effects that physical activity causes by itself.
4.6. Strengths and Limitations
There are several systematic reviews focusing on BFR intervention. However, this study can be considered as one of the few to have focused on different neuro-musculoskeletal populations and on a wide adult age range, which is interesting from a clinical point of view. For example, the application of BFR intervention with low-load exercises obtains improvements in pain and functionality in the short-term with respect to high-load exercises. These results allow for the clinical consideration of BFR intervention, since the LOP used in the different studies remained between 30% and 80%, which indicates that there is a wide range where benefits are obtained in the patients who use it. Another point to highlight is the absence of adverse effects mentioned in the literature such as rhabdomyolysis and deep vein thrombosis, whose incidence is reported to be 0.07–0.2%, thus the methodologies used comply with good practice in the use of BFR intervention and would not have exceeded the workloads or the predetermined values of creatine kinase [45].
However, this study had some limitations that must be taken into account when analyzing the results obtained. In this sense, the search was carried out in eight international databases, and studies published in two different languages were included: English, the language of scientific publications worldwide, and Spanish, the authors’ native language and one of the most widely spoken globally. However, there may be some relevant studies published in another language or database that were excluded from those selected due to these criteria. In addition, future studies should take into account the age of the participants as an independent variable in the analysis of the results, seeking a greater personalization of the treatment and an improvement in the proposed interventions. In addition, it could be interesting to investigate in depth their possible effects on the physiological, biological, and subjective variables of the patient in order to analyze their relationship. On the other hand, it is important to consider that, although common variables were analyzed between the different selected studies, there was heterogeneity in the pathologies of the participants in the different studies. For this reason, it would be necessary to design and develop more studies in each of the pathologies analyzed in order to compare the results presented in this systematic review.
5. Conclusions
The main conclusion that can be drawn after analyzing the different studies included in this systematic review is that BFR intervention is an adjuvant to physical exercise that seems to help improve performance in both strength and aerobic training. In this sense, the observed benefits include a decrease in the pain threshold and an improvement in the functionality and quality of life of neuro-musculoskeletal patients during the first six weeks. In addition, in the short-term, it was observed that the results are better or equal than strength exercises at high loads. However, the results provided by this tool are still not clear for medium- and long-term interventions. Therefore, further studies along this line of research may find it interesting to discern whether the effects of BFR intervention are maintained or, in contrast, tend to equalize with strength exercises at high loads due to a lack of mechanical stress.
Author Contributions
Conceptualization, Á.J.R.-R., G.M.-T., A.G.-M. and M.G.-S.; methodology, Á.J.R.-R., J.M.-C., G.M.-T., R.-P.R.-G., E.C.-V. and M.G.-S.; investigation, Á.J.R.-R., G.M.-T., R.-P.R.-G., A.G.-M. and M.G.-S.; resources; Á.J.R.-R., J.M.-C., G.M.-T., E.C.-V. and M.G.-S.; data curation, Á.J.R.-R., J.M.-C., G.M.-T., A.G.-M., E.C.-V. and M.G.-S.; writing—original draft preparation, Á.J.R.-R., J.M.-C., G.M.-T., R.-P.R.-G., A.G.-M., E.C.-V. and M.G.-S.; writing—review and editing, Á.J.R.-R., J.M.-C., G.M.-T., R.-P.R.-G., A.G.-M., E.C.-V. and M.G.-S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available under request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Caru, M.; Levesque, A.; Lalonde, F.; Curnier, D. An overview of ischemic preconditioning in exercise performance: A systematic review. J. Sport Health Sci. 2019, 8, 355–369. [Google Scholar] [CrossRef] [PubMed]
- Castilla-López, C.; Molina-Mula, J.; Romero-Franco, N. Blood flow restriction during training for improving the aerobic capacity and sport performance of trained athletes: A systematic review and meta-analysis. J. Exerc. Sci. Fit. 2022, 20, 190–197. [Google Scholar] [CrossRef] [PubMed]
- Pearson, S.J.; Hussain, S.R. A Review on the Mechanisms of Blood-Flow Restriction Resistance Training-Induced Muscle Hypertrophy. Sports Med. 2015, 45, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Slysz, J.; Stultz, J.; Burr, J.F. The efficacy of blood flow restricted exercise: A systematic review & meta-analysis. J. Sci. Med. Sports 2016, 19, 669–675. [Google Scholar] [CrossRef]
- Teixeira, E.L.; Barroso, R.; Silva-batista, C.; Laurentino, C.; Loenneke, J.P.; Roschel, H.; Ugrinowitsch, C.; Tricoli, V. Blood Flow Restriction Increases Metabolic Stress But Decreases Muscle Activation During High-Load Resistance Exercise. Muscle Nerve 2017, 57, 107–111. [Google Scholar] [CrossRef]
- Ganesan, G.; Cotter, J.A.; Reuland, W.; Cerussi, A.E.; Tromberg, B.J.; Galassetti, P. Effect of blood flow restriction on tissue oxygenation during knee extension. Med. Sci. Sports Exerc. 2015, 47, 185–193. [Google Scholar] [CrossRef]
- Manini, T.M.; Vincent, K.R.; Leeuwenburgh, C.L.; Lees, H.A.; Kavazis, A.N.; Borst, S.E.; Clark, B.C. Myogenic and proteolytic mRNA expression following blood flow restricted exercise. Acta Physiol. 2011, 201, 255–263. [Google Scholar] [CrossRef]
- Heitkamp, H.C. Training with blood flow restriction. Mechanisms, gain in strength and Safety. J. Sports Med. Phys. Fit. 2015, 55, 446–456. [Google Scholar]
- Kacin, A.; Rosenblatt, B.; Žargi, T.G.; Biswas, A. Safety Considerations With Blood Flow Restricted Resistance Training. Ann. Kinesiol. 2015, 6, 3–26. [Google Scholar]
- Yinghao, L.; Jing, Y.; Yongqi, W.; Jianming, Z.; Zeng, G.; Yiting, T.; Shuoqi, L. Effects of a blood flow restriction exercise under different pressures on testosterone, growth hormone, and insulin-like growth factor levels. J. Int. Med. Res. 2021, 49, 03000605211039564. [Google Scholar] [CrossRef]
- Clarkson, M.J.; May, A.K.; Warmington, S.A. Is there rationale for the cuff pressures prescribed for blood flow restriction exercise? A systematic review. Scand. J. Med. Sci. Sports 2020, 30, 1318–1336. [Google Scholar] [CrossRef]
- Centner, C.; Lauber, B. A Systematic Review and Meta-Analysis on Neural Adaptations Following Blood Flow Restriction Training: What We Know and What We Don’t Know. Front. Physiol. 2020, 11, 887. [Google Scholar] [CrossRef]
- Baker, B.S.; Stannard, M.S.; Duren, D.L.; Cook, J.L.; Stannard, J.P. Does Blood Flow Restriction Therapy in Patients Older Than Age 50 Result in Muscle Hypertrophy, Increased Strength, or Greater Physical Function? A Systematic Review. Clin. Orthop. Relat. Res. 2020, 478, 593–606. [Google Scholar] [CrossRef]
- Minniti, M.C.; Statkevich, A.P.; Kelly, R.L.; Rigsby, V.P.; Exline, M.M.; Rhon, D.I.; Clewley, D. The Safety of Blood Flow Restriction Training as a Therapeutic Intervention for Patients With Musculoskeletal Disorders: A Systematic Review. Am. J. Sports Med. 2020, 48, 1773–1785. [Google Scholar] [CrossRef]
- Vinolo-gil, M.J.; Rodr, M.; Martin-vega, F.J.; Garcia-munoz, C.; Lagares-franco, C.; Garcia-campanario, I. Effectiveness of Blood Flow Restriction in Neurological Disorders: A Systematic Review. Healthcare 2022, 10, 2407. [Google Scholar] [CrossRef]
- Van Cant, J.; Dawe-Coz, A.; Aoun, E.; Esculier, J.-F. Quadriceps strengthening with blood flow restriction for the rehabilitation of patients with knee conditions: A systematic review with meta-analysis. J. Back Musculoskelet. Rehabil. 2020, 1, 529–544. [Google Scholar] [CrossRef]
- Clarkson, M.J.; May, A.K.; Warmington, S.A. Chronic Blood Flow Restriction Exercise Improves Objective Physical Function: A Systematic Review. Front. Physiol. 2019, 10, 1058. [Google Scholar] [CrossRef]
- Hughes, L.; Paton, B.; Rosenblatt, B.; Gissane, C.; Patterson, S.D. Blood flow restriction training in clinical musculoskeletal rehabilitation: A systematic review and meta-analysis. Br. J. Sports Med. 2017, 51, 1003–1011. [Google Scholar] [CrossRef]
- Centner, C.; Zdzieblik, D.; Roberts, L.; Gollhofer, A.; König, D. Effects of blood flow restriction training with protein supplementation on muscle mass and strength in older men. J. Sports Sci. Med. 2019, 18, 471–478. [Google Scholar]
- Bobes Álvarez, C.; Issa-khozouz Santamaría, P.; Fernández-Matías, R.; Pecos-martín, D.; Achalandabaso-Ochoa, A.; Fernández-Carnero, S.; Martínez-Amat, A.; Gallego-Izquierdo, T. Comparison of Blood Flow Restriction Training versus Non-Occlusive Training in Patients with Anterior Cruciate Ligament Reconstruction or Knee Osteoarthritis: A Systematic Review. J. Clin. Med. 2020, 10, E68. [Google Scholar] [CrossRef]
- Wortman, R.J.; Brown, S.M.; Savage-Elliott, I.; Finley, Z.J.; Mulcahey, M.K. Blood Flow Restriction Training for Athletes: A Systematic Review. Am. J. Sports Med. 2021, 49, 1938–1944. [Google Scholar] [CrossRef] [PubMed]
- Lixandrao, M.E.; Ugrinowitsch, C.; Berton, R.; Vechin, F.C.; Conceição, M.S.; Damas, F.; Libardi, C.A.; Roschel, H. Magnitude of Muscle Strength and Mass Adaptations Between High-Load Resistance Training Versus Low-Load Resistance Training Associated with Blood-Flow Restriction: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 361–378. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Rev. Esp. Nutr. Hum. Diet 2014, 18, 172–181. [Google Scholar] [CrossRef]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef] [PubMed]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Vidal Fuentes, J. Versión actualizada de la definición de dolor de la IASP: Un paso adelante o un paso atrás. Rev. Soc. Esp. Dolor 2020, 27, 232–233. [Google Scholar] [CrossRef]
- Bouça-Machado, R.; Duarte, G.S.; Patriarca, M.; Castro Caldas, A.; Alarcão, J.; Fernandes, R.M.; Mestre, T.A.; Matias, R.; Ferreira, J.J. Measurement Instruments to Assess Functional Mobility in Parkinson’s Disease: A Systematic Review. Mov. Disord. Clin. Pract. 2020, 7, 129–139. [Google Scholar] [CrossRef]
- Haraldstad, K.; Wahl, A.; Andenæs, R.; Andersen, J.R.; Andersen, M.H.; Beisland, E.; Borge, C.R.; Engebretsen, E.; Eisemann, M.; Halvorsrud, L.; et al. A systematic review of quality of life research in medicine and health sciences. Qual. Life Res. 2019, 28, 2641–2650. [Google Scholar] [CrossRef]
- Jørgensen, A.N.; Aagaard, P.; Frandsen, U.; Boyle, E.; Diederichsen, L.P. Blood-flow restricted resistance training in patients with sporadic inclusion body myositis: A randomized controlled trial. Scand. J. Rheumatol. 2018, 47, 400–409. [Google Scholar] [CrossRef]
- Giles, L.; Webster, K.E.; Mcclelland, J.; Cook, J.L. Quadriceps strengthening with and without blood flow restriction in the treatment of patellofemoral pain: A double-blind randomised trial. Br. J. Sports Med. 2017, 51, 1688–1694. [Google Scholar] [CrossRef]
- Curran, M.T.; Bedi, A.; Mendias, C.L.; Wojtys, E.M.; Kujawa, M.V.; Palmieri-Smith, R.M. Blood Flow Restriction Training Applied with High-Intensity Exercise Does Not Improve Quadriceps Muscle Function after Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial. Am. J. Sports Med. 2020, 48, 825–837. [Google Scholar] [CrossRef]
- Korakakis, V.; Whiteley, R.; Giakas, G. Low load resistance training with blood flow restriction decreases anterior knee pain more than resistance training alone. A pilot randomised controlled trial. Phys. Ther. Sport 2018, 34, 121–128. [Google Scholar] [CrossRef]
- Branco Ferraz, R.; Gualano, B.; Rodrigues, R.; Kurimori, C.O.; Fuller, R.; Lima, F.R.; De Sa-Pinto, A.L.; Roschel, H. Benefits of Resistance Training with Blood Flow Restriction in Knee Osteoarthritis. Med. Sci. Sports Exerc. 2018, 50, 897–905. [Google Scholar] [CrossRef]
- Constantinou, A.; Mamais, I.; Papathanasiou, G. Comparing hip and knee focused exercises versus hip and knee focused exercises with the use of blood flow restriction training in adults with patellofemoral pain. Eur. J. Phys. Rehabil. Med. 2022, 58, 225–235. [Google Scholar] [CrossRef]
- Harper, S.; Roberts, L.; Layne, A.; Jaeger, B.; Gardner, A.; Sibille, K.; Wu, S.S.; Vincent, K.R.; Fillingim, R.B.; Manini, T.M.; et al. Blood-Flow Restriction Resistance Exercise for Older Adults with Knee Osteoarthritis: A Pilot Randomized Clinical Trial. J. Clin. Med. 2019, 8, 265. [Google Scholar] [CrossRef]
- Hughes, L.; Patterson, S.D.; Haddad, F.; Rosenblatt, B.; Gissane, C.; McCarthy, D.; Clarke, T.; Ferris, G.; Dawes, J.; Paton, B. Examination of the comfort and pain experienced with blood flow restriction training during post-surgery rehabilitation of anterior cruciate ligament reconstruction patients: A UK National Health Service trial. Phys. Ther. Sport 2019, 39, 90–98. [Google Scholar] [CrossRef]
- Hughes, L.; Rosenblatt, B.; Haddad, F.; Gissane, C.; McCarthy, D.; Clarke, T.; Ferris, G.; Dawes, J.; Paton, B.; Patterson, S.D. Comparing the Effectiveness of Blood Flow Restriction and Traditional Heavy Load Resistance Training in the Post-Surgery Rehabilitation of Anterior Cruciate Ligament Reconstruction Patients: A UK National Health Service Randomised Controlled Trial. Sports Med. 2019, 49, 1787–1805. [Google Scholar] [CrossRef]
- Lamberti, N.; Straudi, S.; Donadi, M.; Tanaka, H.; Basaglia, N.; Manfredini, F. Effectiveness of blood flow-restricted slow walking on mobility in severe multiple sclerosis: A pilot randomized trial. Scand. J. Med. Sci. Sports 2020, 30, 1999–2009. [Google Scholar] [CrossRef]
- Mason, J.S.; Crowell, M.S.; Brindle, R.A.; Dolbeer, J.A.; Miller, E.M.; Telemeco, T.A.; Goss, D.L. The Effect of Blood Flow Restriction Training on Muscle Atrophy following Meniscal Repair or Chondral Restoration Surgery in Active Duty Military: A Randomized Controlled Trial. J. Sport Rehabil. 2022, 31, 77–84. [Google Scholar] [CrossRef]
- Rodrigues, R.; Ferraz, R.B.; Kurimori, C.O.; Guedes, L.K.; Lima, F.R.; de Sá-Pinto, A.L.; Gualano, B.; Roschel, H. Low-load resistance training with blood flow restriction increases muscle function, mass and functionality in women with rheumatoid arthritis. Arthritis Care Res. 2019, 72, 787–797. [Google Scholar] [CrossRef]
- Segal, N.A.; Williams, G.N.; Davis, M.C.; Wallace, R.B.; Mikesky, A.E. Efficacy of Blood Flow-Restricted, Low-Load Resistance Training in Women with Risk Factors for Symptomatic Knee Osteoarthritis. PM&R 2015, 7, 376–384. [Google Scholar] [CrossRef]
- Segal, N.; Davis, M.D.; Mikesky, A.E. Efficacy of Blood Flow-Restricted Low-Load Resistance Training For Quadriceps Strengthening in Men at Risk of Symptomatic Knee Osteoarthritis. Geriatr. Orthop. Surg. Rehabil. 2015, 6, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Tennent, D.J.; Hylden, C.M.; Johnson, A.E.; Burns, T.C.; Wilken, J.M.; Owens, J.G. Blood flow restriction training after knee arthroscopy: A randomized controlled pilot study. Clin. J. Sport Med. 2017, 27, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Abbiss, C.R.; Peiffer, J.J.; Meeusen, R.; Skorski, S. Role of Ratings of Perceived Exertion during Self-Paced Exercise: What are We Actually Measuring? Sports Med. 2015, 45, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Patterson, S.D.; Hughes, L.; Warmington, S.; Burr, J.; Scott, B.R.; Owens, J.; Abe, T.; Nielsen, J.L.; Libardi, C.A.; Laurentino, G.; et al. Blood flow restriction exercise position stand: Considerations of methodology, application, and safety. Front. Physiol. 2019, 10, 533. [Google Scholar] [CrossRef]
- Helms, E.; Fitschen, P.J.; Aragon, A.; Cronin, J.; Schoenfeld, B.J. Recommendations for Natural Bodybuilding Contest Preparation: Resistance and Cardiovascular Training. J. Sports Med. Phys. Fit. 2013, 55, 164–178. [Google Scholar]
- Nieman, D.C.; Wentz, L.M. The compelling link between physical activity and the body’s defense system. J. Sport Health Sci. 2019, 8, 201–217. [Google Scholar] [CrossRef]
- Hobart, J.; Blight, A.R.; Goodman, A.; Lynn, F.; Putzki, N. Timed 25-Foot Walk meaningful in MS. Neurology 2013, 80, 1509–1517. [Google Scholar] [CrossRef]
- Kirkland, M.C.; Chen, A.; Downer, M.B.; Holloway, B.J.; Wallack, E.M.; Lockyer, E.J.; Buckle, N.C.; Abbott, C.L.; Ploughman, M. Bipedal hopping timed to a metronome to detect impairments in anticipatory motor control in people with mild multiple sclerosis. Clin. Biomech. 2018, 55, 45–52. [Google Scholar] [CrossRef]
- Sayers, S.P.; Gibson, K.; Cook, C.R. Effect of high-speed power training on muscle performance, function, and pain in older adults with knee osteoarthritis: A pilot investigation. Arthritis Care Res. 2012, 64, 46–53. [Google Scholar] [CrossRef]
- Campbell, C.M.; Buenaver, L.F.; Finan, P.; Bounds, S.C.; Redding, M.; McCauley, L.; Robinson, M.; Edwards, R.R.; Smith, M.T. Sleep, Pain Catastrophizing, and Central Sensitization in Knee Osteoarthritis Patients With and Without Insomnia. Arthritis Care Res. 2015, 67, 1387–1396. [Google Scholar] [CrossRef]
- Brandner, C.R.; Warmington, S.A.; Kidgell, D.J. Corticomotor Excitability is Increased Following an Acute Bout of Blood Flow Restriction Resistance Exercise. Front. Hum. Neurosci. 2015, 9, 652. [Google Scholar] [CrossRef]
- Urbach, D.; Awiszus, F. Impaired Ability of Voluntary Quadriceps Activation Bilaterally Interferes with Function Testing after Knee Injuries. A Twitch Interpolation Study. Int. J. Sports Med. 2002, 23, 231–236. [Google Scholar] [CrossRef]
- Zult, T.; Gokeler, A.; Van Raay, J.J.; Brouwer, R.W.; Zijdewind, I.; Farthing, J.P. Cross-education does not accelerate the rehabilitation of neuromuscular functions after ACL reconstruction: A randomized controlled clinical trial. Eur. J. Appl. Physiol. 2018, 118, 1609–1623. [Google Scholar] [CrossRef]
- Glasgow, P.; Phillips, N.; Bleakley, C. Optimal loading: Key variables and mechanisms. Br. J. Sports Med. 2015, 49, 278–279. [Google Scholar] [CrossRef]
- Hurkmans, E.; van der Giesen, F.J.; Vlieland, T.P.V.; Schoones, J.; Van den Ende, E.C. Dynamic exercise programs (aerobic capacity and/or muscle strength training) in patients with rheumatoid arthritis (Review). Cochrane Database Syst. Rev. 2009, 4. [Google Scholar] [CrossRef]
- Hughes, L.; Patterson, S.D. The effect of blood flow restriction exercise on exercise-induced hypoalgesia and endogenous opioid and endocannabinoid mechanisms of pain modulation. J. Appl. Physiol. 2020, 128, 914–924. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Thiebaud, R.S.; Mattocks, K.T.; Abe, T.; Bemben, M.G. Blood flow restriction pressure recommendations: A tale of two cuffs. Front. Physiol. 2013, 4, 249. [Google Scholar] [CrossRef]
- Gundermann, D.M.; Fry, C.S.; Dickinson, J.M.; Walker, D.K.; Timmerman, K.L.; Drummond, M.J.; Volpi, E.; Rasmussen, B.B. Reactive hyperemia is not responsible for stimulating muscle protein synthesis following blood flow restriction exercise. J. Appl. Physiol. 2012, 112, 1520–1528. [Google Scholar] [CrossRef]
- Yasuda, T.; Fukumura, K.; Iida, H. Effect of low-load resistance exercise with and without blood flow restriction to volitional fatigue on muscle swelling. Eur. J. Appl. Physiol. 2014, 115, 919–926. [Google Scholar] [CrossRef]
- Jones, F.; Harris, P.; Waller, H.; Coggins, A. Adherence to an exercise prescription scheme: The role of expectations, self-efficacy, stage of change and psychological well-being. Br. J. Health Psychol. 2005, 10, 359–378. [Google Scholar] [CrossRef] [PubMed]
- Lauver, J.D.; Cayot, T.E.; Rotarius, T.R.; Scheuermann, B.W. Acute Neuromuscular and Microvascular Responses to Concentric and Eccentric Exercises with Blood Flow Restriction. J. Strength Cond. Res. 2020, 34, 2725–2733. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.L.; Andersen, C.H.; Sundstrup, E.; Jakobsen, M.D.; Mortensen, O.S.; Zebis, M.K. Central Adaptation of Pain Perception in Response to Rehabilitation of Musculoskeletal Pain: Randomized Controlled Trial. Pain Physician 2012, 15, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Rio, E.; Kidgell, D.; Purdam, C.; Gaida, J.; Moseley, G.L.; Pearce, A.J.; Cook, J. Isometric exercise induces analgesia and reduces inhibition in patellar tendinopathy. Br. J. Sports Med. 2015, 49, 1277–1283. [Google Scholar] [CrossRef] [PubMed]
- Hollander, D.B.; Reeves, G.V.; Clavier, J.D.; Francois, M.R.; Thomas, C.; Kraemer, R.R. Partial Occlusion during resistance exercise alters effort sense and pain. J. Strength Cond. Res. 2010, 24, 235–243. [Google Scholar] [CrossRef]
- Van der Heijden, R.A.; Lankhorst, N.E.; van Linschoten, R.; Bierma-Zeinstra, S.M.; van Middelkoop, M. Exercise for treating patellofemoral pain syndrome. Cochrane Database Syst. Rev. 2015, 1, CD010387. [Google Scholar] [CrossRef]
- Ferlito, J.V.; Pecce, S.A.P.; Oselame, L.; De Marchi, T. The blood flow restriction training effect in knee osteoarthritis people: A systematic review and meta-analysis. Clin. Rehabil. 2020, 34, 1378–1390. [Google Scholar] [CrossRef]
- Lu, Y.; Patel, B.H.; Kym, C.; Nwachukwu, B.U.; Beletksy, A.; Forsythe, B.; Chahla, J. Perioperative Blood Flow Restriction Rehabilitation in Patients Undergoing ACL Reconstruction: A Systematic Review. Orthop. J. Sports Med. 2020, 8, 2325967120906822. [Google Scholar] [CrossRef]
- Sallis, J.F.; Kraft, K.; Linton, L.S. How the environment shapes physical activity. A transdisciplinary research agenda. Am. J. Prev. Med. 2002, 22, 208. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).