
Effects of Physical Activity on Inhibitory Function in Children with Attention Deficit Hyperactivity Disorder: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
2. Research Method
2.1. Literature Retrieval Strategy
2.2. Inclusion Criteria
2.3. Exclusion Criteria
2.4. Data Extraction and Coding
2.5. Literature Screening and Quality Evaluation
2.6. Statistical Method
3. Results
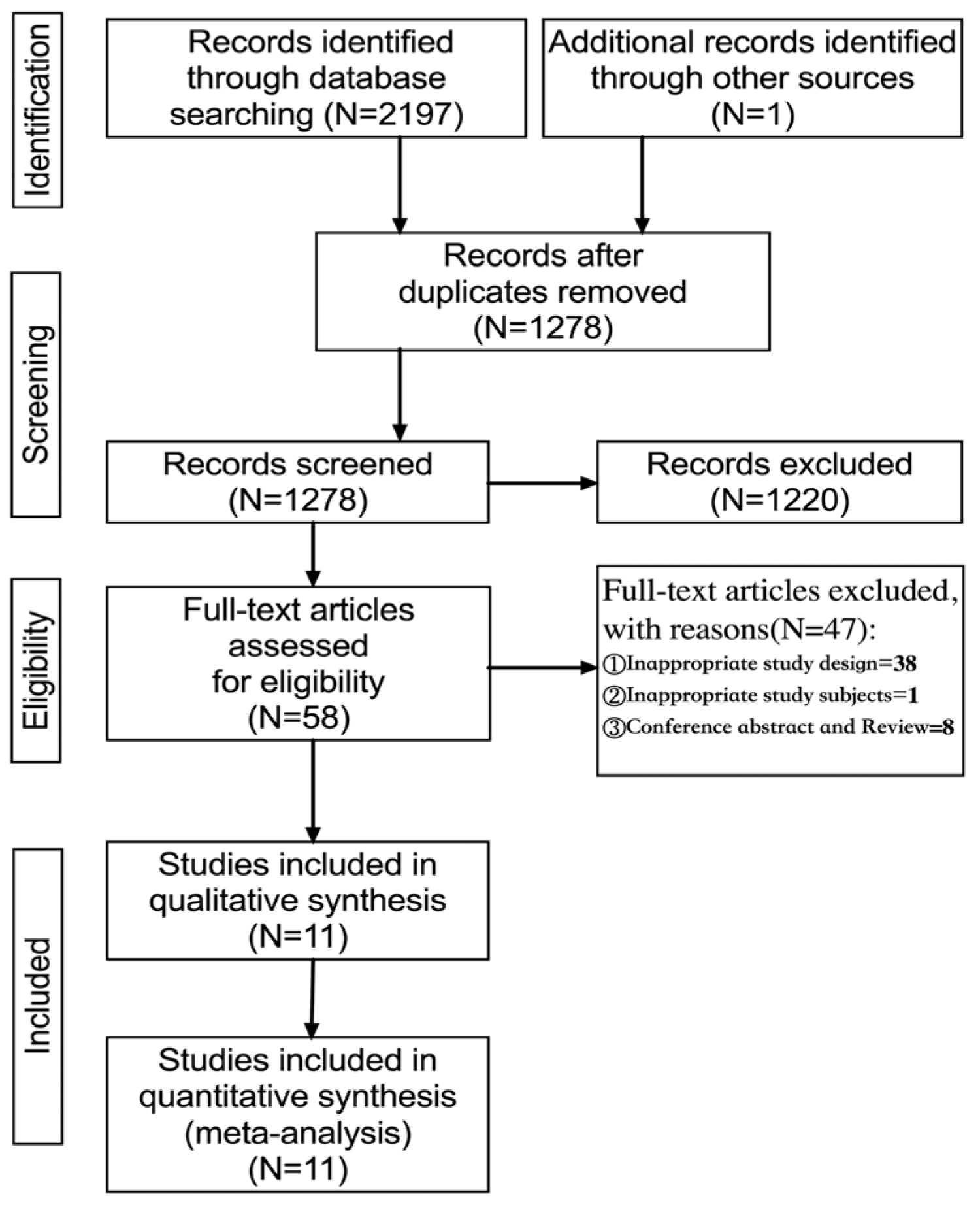
3.1. Literature Retrieval
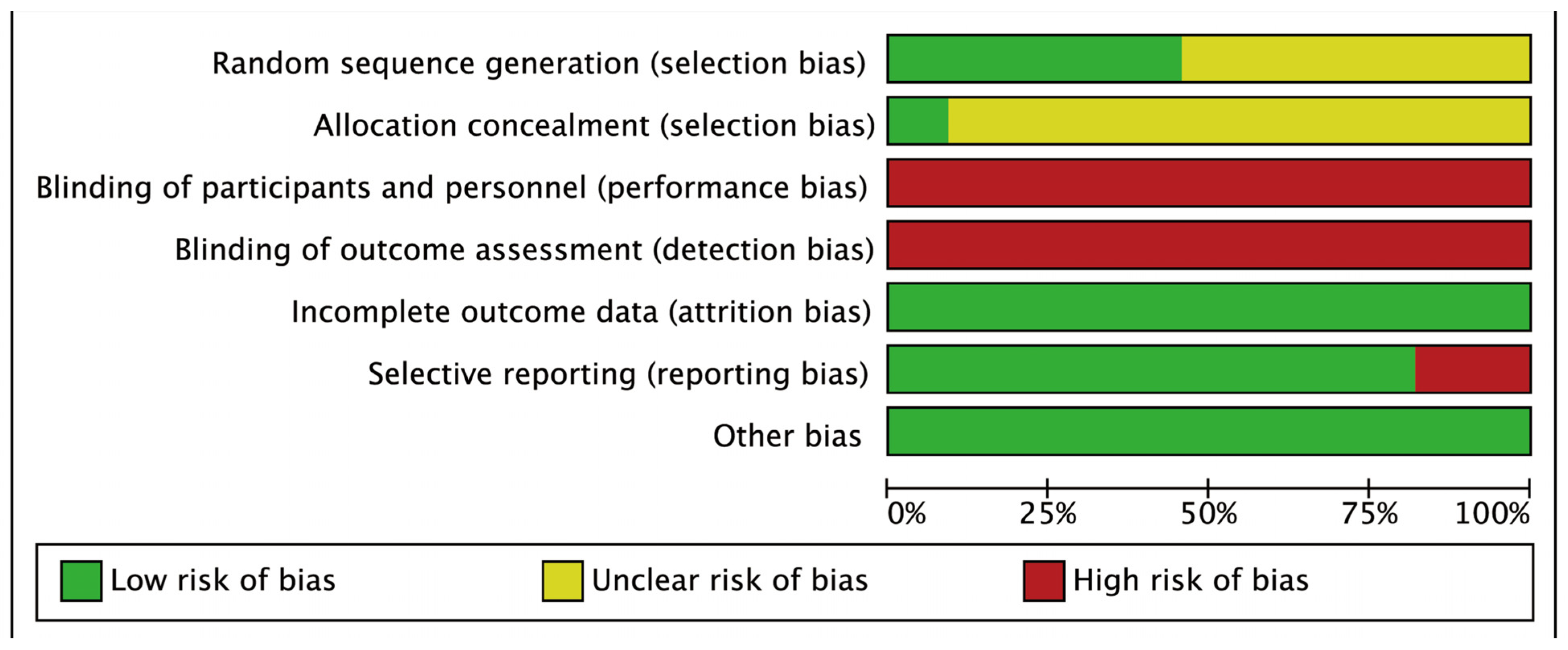
3.2. Characteristics and Quality Evaluation of the Included Literature
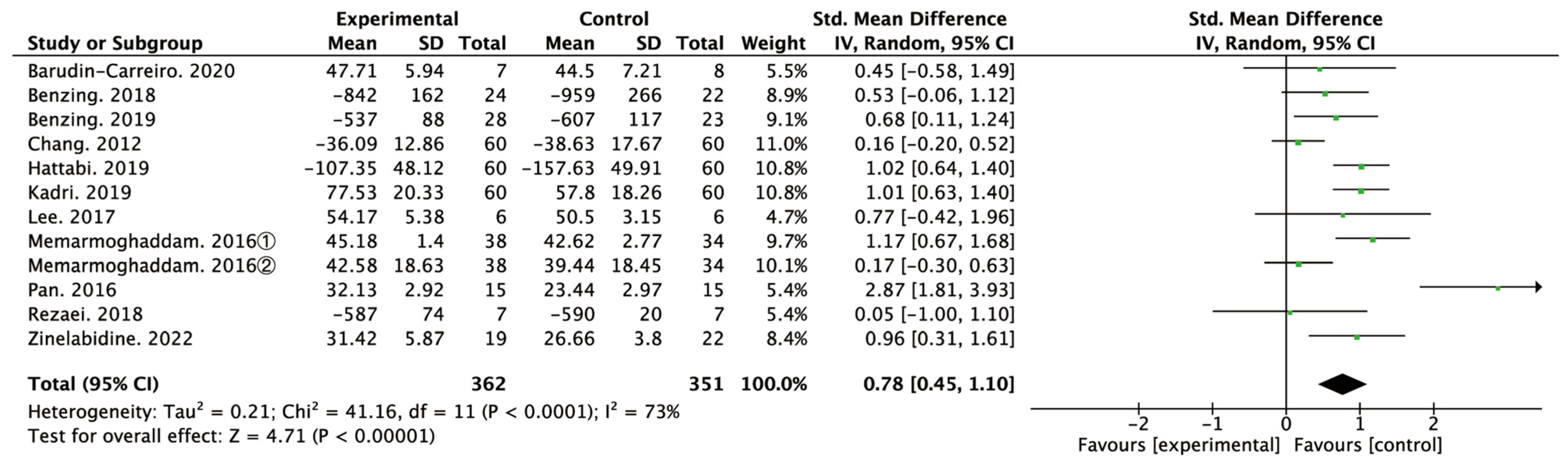
3.3. Results of Meta-Analysis
4. Discussion
4.1. Type of PA
4.2. Length of Intervention
4.3. Duration of PA
4.4. Frequency of PA
4.5. Intensity of PA
4.6. Inhibitory Function Types and PA
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomas, R.; Sanders, S.; Doust, J.; Beller, E.; Glasziou, P. Prevalence of attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Pediatrics 2015, 135, e994–e1001. [Google Scholar] [CrossRef]
- Cortese, S.; Coghill, D. Twenty years of research on attention-deficit/hyperactivity disorder (adhd): Looking back, looking forward. Evid. Based Ment. Health 2018, 21, 173–176. [Google Scholar] [CrossRef]
- Willoughby, M.T. Developmental course of adhd symptomatology during the transition from childhood to adolescence: A review with recommendations. J. Child Psychol. Psychiatry 2003, 44, 88–106. [Google Scholar] [CrossRef]
- Shaw, M.; Hodgkins, P.; Caci, H.; Young, S.; Kahle, J.; Woods, A.G.; Arnold, L.E. A systematic review and analysis of long-term outcomes in attention deficit hyperactivity disorder: Effects of treatment and non-treatment. BMC Med. 2012, 10, 99. [Google Scholar] [CrossRef]
- Sayal, K.; Prasad, V.; Daley, D.; Ford, T.; Coghill, D. Adhd in children and young people: Prevalence, care pathways, and service provision. Lancet Psychiatry 2018, 5, 175–186. [Google Scholar] [CrossRef]
- Sun, S.; Kuja-Halkola, R.; Faraone, S.V.; D’Onofrio, B.M.; Dalsgaard, S.; Chang, Z.; Larsson, H. Association of psychiatric. comor- bidity with the risk of premature death among children and adults with attention-deficit/hyperactivity disorder. JAMA Psychiatry 2019, 76, 1141–1149. [Google Scholar] [CrossRef]
- Sobanski, E. Psychiatric comorbidity in adults with attention-deficit/hyperactivity disorder (adhd). Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256 (Suppl. 1), i26–i31. [Google Scholar] [CrossRef]
- Hedges, D.; Farrer, T.J.; Bigler, E.D.; Hopkins, R.O. The Brain at Risk, 1st ed.; Springer: Cham, Switzerland, 2019; pp. 59–64. [Google Scholar]
- McAuley, T.; Crosbie, J.; Charach, A.; Schachar, R. The persistence of cognitive deficits in remitted and unremitted adhd: A case for the state-independence of response inhibition. J. Child Psychol. Psychiatry 2014, 55, 292–300. [Google Scholar] [CrossRef]
- Bai, Z.S.; Zhou, J. Inhibitory Control Functions: Concept, Measurement and Exercise Intervention. Fujian Sport. Sci. Technol. 2022, 41, 21–26. [Google Scholar]
- Barkley, R.A. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of adhd. Psychol. Bull. 1997, 121, 65–94. [Google Scholar] [CrossRef]
- Doyle, A.E. Executive functions in attention-deficit/hyperactivity disorder. J. Clin. Psychiatry 2006, 67, 21–26. [Google Scholar] [PubMed]
- Jingjing, C.; Fangzhong, X.; Luhan, T. Progress in computer aided training of response inhibition in attention deficit hyperactivity disorder. Prev. Med. 2018, 30, 1128–1132. [Google Scholar]
- Gejl, A.K.; Bugge, A.; Ernst, M.T.; Tarp, J.; Hillman, C.H.; Have, M.; Froberg, K.; Andersen, S.B. The acute effects of short. bouts. of exercise on inhibitory control in adolescents. Ment. Health Phys. Act. 2018, 15, 34–39. [Google Scholar] [CrossRef]
- Rhoades, B.L.; Greenberg, M.T.; Domitrovich, C.E. The contribution of inhibitory control to preschoolers’ social–emotional competence. J. Appl. Dev. Psychol. 2009, 30, 310–320. [Google Scholar] [CrossRef]
- Amodio, D.M.; Master, S.L.; Yee, C.M.; Taylor, S.E. Neurocognitive components of the behavioral inhibition and activation systems: Implications for theories of self-regulation. Psychophysiology 2008, 45, 11–19. [Google Scholar] [CrossRef]
- Blair, C.; Razza, R.P. Relating effortful control, executive function, and false belief understanding to emerging math and literacy ability in kindergarten. Child Dev. 2007, 78, 647–663. [Google Scholar] [CrossRef]
- Ng, Q.X. A systematic review of the use of bupropion for attention-deficit/hyperactivity disorder in children and adolescents. J. Child Adolesc. Psychopharmacol. 2017, 27, 112–116. [Google Scholar] [CrossRef]
- Pliszka, S.; AACAP Work Group on Quality Issues. Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 894–921. [Google Scholar] [CrossRef]
- Lan, S.; Li, Y.; Qingjiu, C.; Yufeng, W. Effect of methylphenidate on executive function for children with attention deficithy peractivity disorder. J. Peking Univ. Health Sci. 2007, 39, 293–298. [Google Scholar]
- DuPaul, G.J.; Evans, S.W.; Mautone, J.A.; Owens, J.S.; Power, T.J. Future directions for psychosocial interventions for children and adolescents with adhd. J. Clin. Child Adolesc. Psychol. 2020, 49, 134–145. [Google Scholar] [CrossRef]
- Wigal, S.B.; Emmerson, N.; Gehricke, J.G.; Galassetti, P. Exercise: Applications to childhood adhd. J. Atten. Disord. 2013, 17, 279–290. [Google Scholar] [CrossRef] [PubMed]
- Hansen, D.L.; Hansen, E.H. Caught in a balancing act: Parents’ dilemmas regarding their adhd child’s treatment with stimulant medication. Qual. Health Res. 2006, 16, 1267–1285. [Google Scholar] [CrossRef] [PubMed]
- Greenhill, L.L.; Swanson, J.M.; Vitiello, B.; Davies, M.; Clevenger, W.; Wu, M.; Arnold, L.E.; Abikoff, H.B.; Bukstein, O.G.; Conners, C.K.; et al. Impairment and deportment responses to different methylphenidate doses in children with adhd: The mta titration trial. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Benner-Davis, S.; Heaton, P.C. Attention deficit and hyperactivity disorder: Controversies of diagnosis and safety of pharmacological and nonpharmacological treatment. Curr. Drug Saf. 2007, 2, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Lambez, B.; Harwood-Gross, A.; Golumbic, E.Z.; Rassovsky, Y. Non-pharmacological interventions for cognitive difficulties in adhd: A systematic review and meta-analysis. J. Psychiatr. Res. 2020, 120, 40–55. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions. for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Wang, J.F.; Qi, C.Z.; Wei, X.N. Effects of Physical Activity on Executive Function: A Meta-analysis. Journal of Capital. Univ. Phys. Educ. Sport. 2019, 31, 375–384. [Google Scholar]
- Chang, Y.K.; Liu, S.; Yu, H.H.; Lee, Y.H. Effect of acute exercise on executive function in children with attention deficit hyperactivity disorder. Arch. Clin. Neuropsychol. 2012, 27, 225–237. [Google Scholar] [CrossRef]
- Jiang, D.L.; Zeng, C.Z. The effect of 8-week soccer exercise with medium intensity on executive function in preschool children. China Sport Sci. Technol. 2015, 51, 43–50. [Google Scholar]
- Chen, A.G.; Zhao, L.; Li, H.Y.; Yan, J.; Yin, H.C. Effects of acute basketball dribbling training of different intensity on executive function of primary students. J. Tianjin Univ. Sport 2014, 29, 352–355. [Google Scholar]
- Pontifex, M.B.; Saliba, B.J.; Raine, L.B.; Picchietti, D.L.; Hillman, C.H. Exercise improves behavioral, neurocognitive, and scholastic performance in children with attention-deficit/hyperactivity disorder. J. Pediatr. 2013, 162, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Piepmeier, A.T.; Shih, C.H.; Whedon, M.; Williams, L.M.; Davis, M.E.; Henning, D.A.; Park, S.Y.; Calkins, S.D.; Etnier, J.L. The effect of acute exercise on cognitive performance in children with and without adhd. J. Sport Health Sci. 2015, 4, 97–104. [Google Scholar] [CrossRef]
- Gawrilow, C.; Stadler, G.; Langguth, N.; Naumann, A.; Boeck, A. Physical activity, affect, and cognition in children with symptoms of adhd. J. Atten. Disord 2016, 20, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.P.; Prado, S.O.; Scardovelli, T.A.; Boschi, S.R.; Campos, L.C.; Frere, A.F. Measurement of the effect of physical exercise on the concentration of individuals with adhd. PLoS ONE 2015, 10, e0122119. [Google Scholar] [CrossRef] [PubMed]
- Formenti, D.; Trecroci, A.; Duca, M.; Cavaggioni, L.; D’Angelo, F.; Passi, A.; Longo, S.; Alberti, G. Differences in inhibitory control and motor fitness in children practicing open and closed skill sports. Sci. Rep. 2021, 11, 4033. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; Zou, L.; Loprinzi, P.D.; Quan, M.; Huang, T. Effects of open versus closed skill exercise on cognitive function: A systematic review. Front. Psychol. 2019, 10, 1707. [Google Scholar] [CrossRef]
- Hattabi, S.; Bouallegue, M.; Ben, Y.H.; Bouden, A. Rehabilitation of adhd children by sport intervention: A tunisian experience. Tunis Med. 2019, 97, 874–881. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Keith, M. Statistical power analysis for the behavioral sciences. J. Am. Stat. Assoc. 1989, 31, 499–500. [Google Scholar]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Barudin-Carreiro, A.M. Effects of Walking and Standing on Executive Function in Children with Attention Deficit/Hyperactivity Disorder. Ph.D. Thesis, Massachusetts Boston University, Boston, MA, USA, 2020. [Google Scholar]
- Benzing, V.; Chang, Y.K.; Schmidt, M. Acute physical activity enhances executive functions in children with adhd. Sci. Rep. 2018, 8, 12382. [Google Scholar] [CrossRef] [PubMed]
- Benzing, V.; Schmidt, M. The effect of exergaming on executive functions in children with adhd: A randomized clinical trial. Scand J. Med. Sci. Sport. 2019, 29, 1243–1253. [Google Scholar] [CrossRef]
- Kadri, A.; Slimani, M.; Bragazzi, N.L.; Tod, D.; Azaiez, F. Effect of taekwondo practice on cognitive function in adolescents with attention deficit hyperactivity disorder. Int. J. Environ. Res. Public Health 2019, 16, 204. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.K.; Song, J.; Park, J.H. Effects of combination exercises on electroencephalography and frontal lobe executive function measures in children with adhd: A pilot study. Biomed. Res. India 2017, 28, S455–S460. [Google Scholar]
- Memarmoghaddam, M.; Torbati, H.T.; Sohrabi, M.; Mashhadi, A.; Kashi, A. Effects of a selected exercise programon executive function of children with attention deficit hyperactivity disorder. J. Med. Life 2016, 9, 373–379. [Google Scholar] [PubMed]
- Pan, C.Y.; Chu, C.H.; Tsai, C.L.; Lo, S.Y.; Cheng, Y.W.; Liu, Y.J. A racket-sport intervention improves behavioral and cognitive performance in children with attention-deficit/hyperactivity disorder. Res. Dev. Disabil. 2016, 57, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Rezaei, M.; Salarpor Kamarzard, T.; Najafian Razavi, M. The effects of neurofeedback, yoga interventions on memory and cognitive activity in children with attention deficit/hyperactivity disorder: A randomized controlled trial. Ann. Appl. Sport Sci. 2018, 6, 17–27. [Google Scholar] [CrossRef]
- Zinelabidine, K.; Elghoul, Y.; Jouira, G.; Sahli, S. The effect of an 8-week aerobic dance program on executive function in children. Percept. Mot. Ski. 2022, 129, 153–175. [Google Scholar] [CrossRef]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sport. Med. 2018, 52, 154–160. [Google Scholar] [CrossRef]
- Colcombe, S.; Kramer, A.F. Fitness effects on the cognitive function of older adults: A meta-analytic study. Psychol. Sci. 2003, 14, 125–130. [Google Scholar] [CrossRef]
- Di Russo, F.; Bultrini, A.; Brunelli, S.; Delussu, A.S.; Polidori, L.; Taddei, F.; Traballesi, M.; Spinelli, D. Benefits of sports participation for executive function in disabled athletes. J. Neurotrauma 2010, 27, 2309–2319. [Google Scholar] [CrossRef] [PubMed]
- Voss, M.W.; Kramer, A.F.; Basak, C.; Prakash, R.S.; Roberts, B. Are expert athletes ‘expert’ in the cognitive laboratory? A meta-analytic review of cognition and sport expertise. Appl. Cogn. Psychol. 2010, 24, 812–826. [Google Scholar] [CrossRef]
- Sung, M.C.; Ku, B.; Leung, W.; MacDonald, M. The effect of physical activity interventions on executive function among people with neurodevelopmental disorders: A meta-analysis. J. Autism. Dev. Disord. 2022, 52, 1030–1050. [Google Scholar] [CrossRef]
- Haijun, Z.; Zhen, L.; Wenfeng, Z. A study on brain functional plasticity after aerobic exercise based on the dynamic low-frequency amplitude. J. Phys. Educ. 2021, 28, 139–144. [Google Scholar]
- Cerrillo-Urbina, A.J.; Garcia-Hermoso, A.; Sanchez-Lopez, M.; Pardo-Guijarro, M.J.; Santos Gomez, J.L.; Martinez-Vizcaino, V. The effects of physical exercise in children with attention deficit hyperactivity disorder: A systematic review and meta-analysis of randomized control trials. Child Care Health Dev. 2015, 41, 779–788. [Google Scholar] [CrossRef]
- Chueh, T.Y.; Chen, Y.C.; Hung, T.M. Acute effect of breaking up prolonged sitting on cognition: A systematic review. BMJ Open 2022, 12, e050458. [Google Scholar] [CrossRef]
- Liang, X.; Li, R.; Wong, S.H.S.; Sum, R.K.W.; Sit, C.H.P. The impact of exercise interventions concerning executive functions of children and adolescents with attention-deficit/hyperactive disorder: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 68. [Google Scholar] [CrossRef]
- Tan, B.W.; Pooley, J.A.; Speelman, C.P. A meta-analytic review of the efficacy of physical exercise interventions on cognition in individuals with autism spectrum disorder and adhd. J. Autism. Dev. Disord. 2016, 46, 3126–3143. [Google Scholar] [CrossRef]
- Crova, C.; Struzzolino, I.; Marchetti, R.; Masci, I.; Vannozzi, G.; Forte, R.; Pesce, C. Cognitively challenging physical activity benefits executive function in overweight children. J. Sport. Sci. 2014, 32, 201–211. [Google Scholar] [CrossRef]
- O’Brien, J.; Ottoboni, G.; Tessari, A.; Setti, A. One bout of open skill exercise improves cross-modal perception and immediate memory in healthy older adults who habitually exercise. PLoS ONE 2017, 12, e0178739. [Google Scholar] [CrossRef]
- Tsai, C.L.; Wang, C.H.; Pan, C.Y.; Chen, F.C.; Huang, S.Y.; Tseng, Y.T. The effects of different exercise types on visuospatial attention in the elderly. Psychol. Sport Exer. 2016, 26, 130–138. [Google Scholar] [CrossRef]
- Scisco, J.L.; Leynes, P.A.; Kang, J. Cardiovascular fitness and executive control during task-switching: An erp study. Int. J. Psychophysiol. 2008, 69, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Staiano, A.E.; Abraham, A.A.; Calvert, S.L. Competitive versus cooperative exergame play for african american adolescents’ executive function skills: Short-term effects in a long-term training intervention. Dev. Psychol. 2012, 48, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Lauenroth, A.; Ioannidis, A.E.; Teichmann, B. Influence of combined physical and cognitive training on cognition: A systematic review. BMC Geriatr. 2016, 16, 141. [Google Scholar] [CrossRef]
- Best, J.R. Exergaming immediately enhances children’s executive function. Dev. Psychol. 2012, 48, 1501–1510. [Google Scholar] [CrossRef]
- Tsai, C.L.; Pan, C.Y.; Chen, F.C.; Tseng, Y.T. Open- and closed-skill exercise interventions produce different neurocognitive effects on executive functions in the elderly: A 6-month randomized, controlled trial. Front. Aging Neurosci. 2017, 9, 294. [Google Scholar] [CrossRef]
- Brady, F. Sports skill classification, gender, and perceptual style. Percept. Mot. Ski. 1995, 81, 611–620. [Google Scholar] [CrossRef]
- Dishman, R.K.; Berthoud, H.R.; Booth, F.W.; Cotman, C.W.; Edgerton, V.R.; Fleshner, M.R.; Gandevia, S.C.; Gomez-Pinilla, F.; Greenwood, B.N.; Hillman, C.H.; et al. Neurobiology of exercise. Obes. Silver Spring 2006, 14, 345–356. [Google Scholar] [CrossRef]
- Hillman, C.H.; Erickson, K.I.; Kramer, A.F. Be smart, exercise your heart: Exercise effects on brain and cognition. Nat. Rev. Neurosci. 2008, 9, 58–65. [Google Scholar] [CrossRef]
- Hume, K.; Loftin, R.; Lantz, J. Increasing independence in autism spectrum disorders: A review of three focused interventions. J. Autism. Dev. Disord. 2009, 39, 1329–1338. [Google Scholar] [CrossRef]
- Best, J.R. Effects of physical activity on children’s executive function: Contributions of experimental research on aerobic exercise. Dev. Rev. 2010, 30, 331–551. [Google Scholar] [CrossRef] [PubMed]
- Cotman, C.W.; Berchtold, N.C.; Christie, L.A. Exercise builds brain health: Key roles of growth factor cascades and inflammation. Trends. Neurosci. 2007, 30, 464–472. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.J.; Liou, Y.J.; Tsai, S.J. Effects of bdnf polymorphisms on brain function and behavior in health and disease. Brain Res. Bull. 2011, 86, 287–297. [Google Scholar] [CrossRef] [PubMed]
- Den Heijer, A.E.; Groen, Y.; Tucha, L.; Fuermaier, A.B.; Koerts, J.; Lange, K.W.; Thome, J.; Tucha, O. Sweat it out? The effects of physical exercise on cognition and behavior in children and adults with adhd: A systematic literature review. J. Neural. Transm. Vienna 2017, 124, 3–26. [Google Scholar] [CrossRef] [PubMed]
- Chueh, T.Y.; Hsieh, S.S.; Tsai, Y.J.; Yu, C.L.; Hung, C.L.; Benzing, V.; Schmidt, M.; Chang, Y.K.; Hillman, C.H.; Hung, T.M. Effects of a single bout of moderate-to-vigorous physical activity on executive functions in children with attention-deficit/hyperactivity disorder: A systematic review and meta-analysis. Psychol. Sport Exerc. 2022, 58, 102097. [Google Scholar] [CrossRef]
- McKune, A.J.; Pautz, J.; Lomjbard, J. Behavioural response to exercise in children with attention-deficit/hyperactivity disorder. S. Afr. J. Sport. Med. 2003, 15, 17–21. [Google Scholar] [CrossRef]
- Yang, B. Meta analysis of exercise on executive function of children with adhd. China Spost Sci. Technol. 2021, 57, 96–102. [Google Scholar]
- Cian, C.; Barraud, P.A.; Melin, B.; Raphel, C. Effects of fluid ingestion on cognitive function after heat stress or exercise-induced dehydration. Int. J. Psychophysiol. 2001, 42, 243–251. [Google Scholar] [CrossRef]
- Cortese, S.; Moreira-Maia, C.R.; St Fleur, D.; Morcillo-Penalver, C.; Rohde, L.A.; Faraone, S.V. Association between adhd and obesity: A systematic review and meta-analysis. Am. J. Psychiatry 2016, 173, 34–43. [Google Scholar] [CrossRef]
- Cortese, S.; Castellanos, F.X. The relationship between adhd and obesity: Implications for therapy. Expert Rev. Neurother. 2014, 14, 473–479. [Google Scholar] [CrossRef]
- Harnishfeger, K.K. The Development of Cognitive Inhibition: Theories, Definitions, and Research Evidence, 1st ed.; Academic Press: New York, NY, USA, 1995; pp. 175–204. [Google Scholar]
- Nigg, J.T. On inhibition/disinhibition in developmental psychopathology: Views from cognitive and personality psychology. and a working inhibition taxonomy. Psychol. Bull. 2000, 126, 220–246. [Google Scholar] [CrossRef] [PubMed]
- Adams, Q.; Craft, J. Retained Primitive Reflexes and ADHD: Examining Atypical Symptomology in the School-Aged Population. Master’s Thesis, University of North Dakota UND Scholarly Commons, America, Grand Forks, ND, USA, 2014. [Google Scholar]
- Grandjean, A.; Suarez, I.; Miquee, A.; Da, F.D.; Casini, L. Differential response to pharmacological intervention in ADHD fur. thers our understanding of the mechanisms of interference control. Cogn. Neuropsychol. 2021, 38, 138–152. [Google Scholar] [CrossRef] [PubMed]
- Wodka, E.L.; Mark, M.E.; Blankner, J.G.; Gidley Larson, J.C.; Fotedar, S.; Denckla, M.B.; Mostofsky, S.H. Evidence that re. sponse inhibition is a primary deficit in ADHD. J. Clin. Exp. Neuropsychol. 2007, 29, 345–356. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Who Guidelines on Physical Activity and Sedentary Behavior; World Health Organization: Geneva, Switzerland, 2020; p. 464.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Diagnostic Criteria | PA Content | Research Design | Experimental Group | Control Group | End Indicator | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Session Time; Frequency; Period | Sample | Exercise Intensity | Sample | Activity Mode | ||||||
| Barudin-Carreiro 2020 [42] | America | DSM-IV | walk | RCT | 20 min/1 time | 7 | NA | 8 | sit | Stroop Test |
| Benzing 2018 [43] | Switzerland | ICD-10 | Body feeling game | RCT | 15 min/1 time | 24 | MVPA | 22 | watch video | Flanker Task |
| Benzing 2019 [44] | Switzerland | ICD-10 | Body feeling game | parallel group | 30 min/week 3 times/8 weeks | 28 | NA | 23 | Non Exercise | Simon Task |
| Chang 2012 [29] | Taiwan, China | DSM-IV | Run | RCT | 30 min/1 time | 20 | MPA | 20 | watch video | Stroop Test |
| Hattabi 2019 [38] | Tunisia | DSM-IV | water aerobic exercise | RCT | 90 min/week 3 times/12 weeks | 20 | MPA | 20 | Non Exercise | Stroop Test |
| Kadri 2019 [45] | Tunisia | NA | Taekwondo | RCT | 50 min/week 2 times/64 weeks | 20 | NA | 20 | Non Exercise | Stroop Test |
| Lee 2017 [46] | South Korea | DSM-IV | Ball; Rope-jumping | RCT | 60 min /week 3 times/12 weeks | 6 | MVPA | 6 | Non Exercise | Stroop Test |
| Memarmoghaddam 2016 [47] | Iran | DSM-IV | pingpong | RCT | 90 min/week 3 times/8 weeks | 19 | MVPA | 17 | Non Exercise | Stroop Test; Go-No Go Task |
| Pan 2016 [48] | Taiwan, China | DSM-IV | pingpong | Crossover | 70 min/week 2 times/12 weeks | 15 | NA | 15 | Non Exercise | Stroop Test |
| Rezaei 2018 [49] | Iran | DSM-5 | Yoga | parallel group | 45 min/week 3 times/8 weeks | 7 | NA | 7 | Non Exercise | CPT |
| Zinelabidine 2022 [50] | Tunisia | NA | Aerobic Dance | RCT | 45 min /week 2 times/8 weeks | 19 | MVPA | 22 | Non Exercise | Stroop Test |
| Moderator | Level | Hypothesis |
|---|---|---|
| Frequency of PA | (a) One time per week; (b) 2 times per week; (c) 3 times per week. | It is hypothesized that PA more than twice per week for children with ADHD leads to benign inhibitory function (code has previously been used) [51]. |
| Session time | (a) Short (<45 min); (b) Moderate (45–60 min); (c) Long (≥60 min). | We hypothesized that long-interval (≥60 min) PA intervention for children with ADHD produced more effects than moderate or short one (code previously used) [52]. |
| Length of intervention | (a) Acute; (b) Longitudinal. | (a) Acute PA within 10 to 60 min; (b) PA that was provided over several weeks in a long-term intervention plan. It was hypothesized that long-term intervention would lead to greater benign changes in inhibitory function for ADHD children than acute intervention (code previously used) [52]. |
| Type of PA | (a) Closed-skill sport (Aerobic exercise); (b) Open-skill sport (e.g., pingpong, Taekwondo); (c) Motor skill training; (d) Exergaming. | Closed-skill sport is defined as a sport in which the sport environment is relatively highly consistent, predictable, and self-controlled like running or swimming [53,54]. Open-skill sport is defined as a sport that requires reaction in a complex environment with dynamic changes, and unpredictable and uncontrollable rhythms (e.g., ping-pong, taekwondo) [54]. It is assumed that open-skill sports can improve children’s inhibitory function more effectively than other physical activities (code has been used before) [55]. |
| Intensity of PA | (a) Moderate to vigorous physical activity (MVPA); (b) Moderate physical activity (MPA). | We hypothesized that MVPA PA intervention in ADHD children would produce a larger effect than MPA. |
| Inhibition type | (a) Interference suppression; (b) Response inhibition. | The measurement of inhibition function is divided into two dimensions: response inhibition ability measurement and interference suppression ability measurement. The research paradigms of response inhibition mainly include Go/No-go tasks, stop-signal tasks, etc. The research paradigms of interference mainly include the Stroop task, Flanker task, etc [10]. The inhibition function is divided according to the research paradigms included in the article. We hypothesized that PA intervention would have a significant impact on interference suppression and response inhibition in children with ADHD. |
| Variable | Grouping Criteria | n | Heterogeneity Test Result | Effects Model | Effect Size Test | ||||
|---|---|---|---|---|---|---|---|---|---|
| Q | P | I2/% | ES (95% CI) | z | P | ||||
| Frequency of PA | one time per week | 3 | 1.19 | 0.55 | 0 | Fixed | 0.28 (−0.02, 0.57) | 1.85 | 0.06 |
| two times per week | 3 | 10.97 | 0 | 82 | Random | 1.49 (0.60, 2.37) | 3.29 | 0 | |
| three times per week | 6 | 12.48 | 0.03 | 60 | Random | 0.70 (0.31, 1.08) | 3.56 | 0 | |
| Session time | Short (<45 min) | 3 | 1.19 | 0.55 | 0 | Fixed | 0.28 (−0.02, 0.57) | 1.85 | 0.06 |
| Moderate (45–60 min) | 4 | 3.41 | 0.33 | 12 | Fixed | 0.86 (0.58, 1.13) | 6.13 | 0 | |
| Long (≥60 min) | 5 | 24.48 | 0 | 84 | Random | 1.11 (0.45, 1.78) | 3.27 | 0 | |
| Length of intervention | Acute | 3 | 1.19 | 0.55 | 0 | Fixed | 0.28 (−0.02, 0.57) | 1.85 | 0.06 |
| Longitudinal | 9 | 27.96 | 0 | 71 | Random | 0.92 (0.55, 1.29) | 4.89 | 0 | |
| Type of PA | closed-skill sport | 4 | 4.74 | 0.19 | 37 | Fixed | 0.33 (0.05, 0.62) | 2.27 | 0.02 |
| open-skill sport | 4 | 24.4 | 0 | 88 | Random | 1.18 (0.42, 1.94) | 3.05 | 0 | |
| Motor skill training | 2 | 0.15 | 0.69 | 0 | Fixed | 1.00 (0.63, 1.36) | 5.38 | 0 | |
| Exergaming | 2 | 0.13 | 0.72 | 0 | Fixed | 0.60 (0.20, 1.01) | 2.9 | 0 | |
| Intensity of PA | Moderate to vigorous physical activity (MVPA) | 4 | 9.38 | 0.05 | 57 | Random | 0.70 (0.28, 1.12) | 3.24 | 0 |
| Moderate physical activity (MPA) | 2 | 10.28 | 0 | 90 | Random | 0.59 (−0.25, 1.43) | 1.38 | 0.17 | |
| Inhibition type | Interference suppression | 10 | 34.89 | 0 | 74 | Random | 0.78 (0.45, 1.10) | 4.57 | 0 |
| Response inhibition | 2 | 1.84 | 0.17 | 46 | Random | 0.39 (−0.10, 0.89) | 1.56 | 0.12 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, M.; Yang, X.; Yu, J.; Zhu, J.; Kim, H.-D.; Cruz, A. Effects of Physical Activity on Inhibitory Function in Children with Attention Deficit Hyperactivity Disorder: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2023, 20, 1032. https://doi.org/10.3390/ijerph20021032
Wang M, Yang X, Yu J, Zhu J, Kim H-D, Cruz A. Effects of Physical Activity on Inhibitory Function in Children with Attention Deficit Hyperactivity Disorder: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2023; 20(2):1032. https://doi.org/10.3390/ijerph20021032
Chicago/Turabian StyleWang, Meng, Xinyue Yang, Jing Yu, Jian Zhu, Hyun-Duck Kim, and Angelita Cruz. 2023. "Effects of Physical Activity on Inhibitory Function in Children with Attention Deficit Hyperactivity Disorder: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 20, no. 2: 1032. https://doi.org/10.3390/ijerph20021032
APA StyleWang, M., Yang, X., Yu, J., Zhu, J., Kim, H.-D., & Cruz, A. (2023). Effects of Physical Activity on Inhibitory Function in Children with Attention Deficit Hyperactivity Disorder: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 20(2), 1032. https://doi.org/10.3390/ijerph20021032