
Validation of a Harmonised, Three-Item Cognitive Screening Instrument for the Survey of Health, Ageing and Retirement in Europe (SHARE-Cog)



Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Cognitive Tests
2.2.1. SHARE Cognitive Instrument (SHARE-Cog)
2.2.2. Cognitive Battery
2.3. Descriptive Variables
2.4. Cognitive Classifications
2.4.1. Dementia (D)
2.4.2. Mild Cognitive Impairment (MCI)
2.4.3. Subjective Memory Complaints (SMC)
2.4.4. Normal Cognition (NC)
2.5. Statistical Analysis
3. Results
3.1. Sample Description
3.2. Regression Analysis and SHARE-Cog Weighting
3.2.1. Maximum Score for Verbal Fluency
3.2.2. Relative Importance of Each Subtest
3.2.3. Scoring of Each Subtest for SHARE-Cog
3.3. SHARE-Cog Items and Internal Consistency
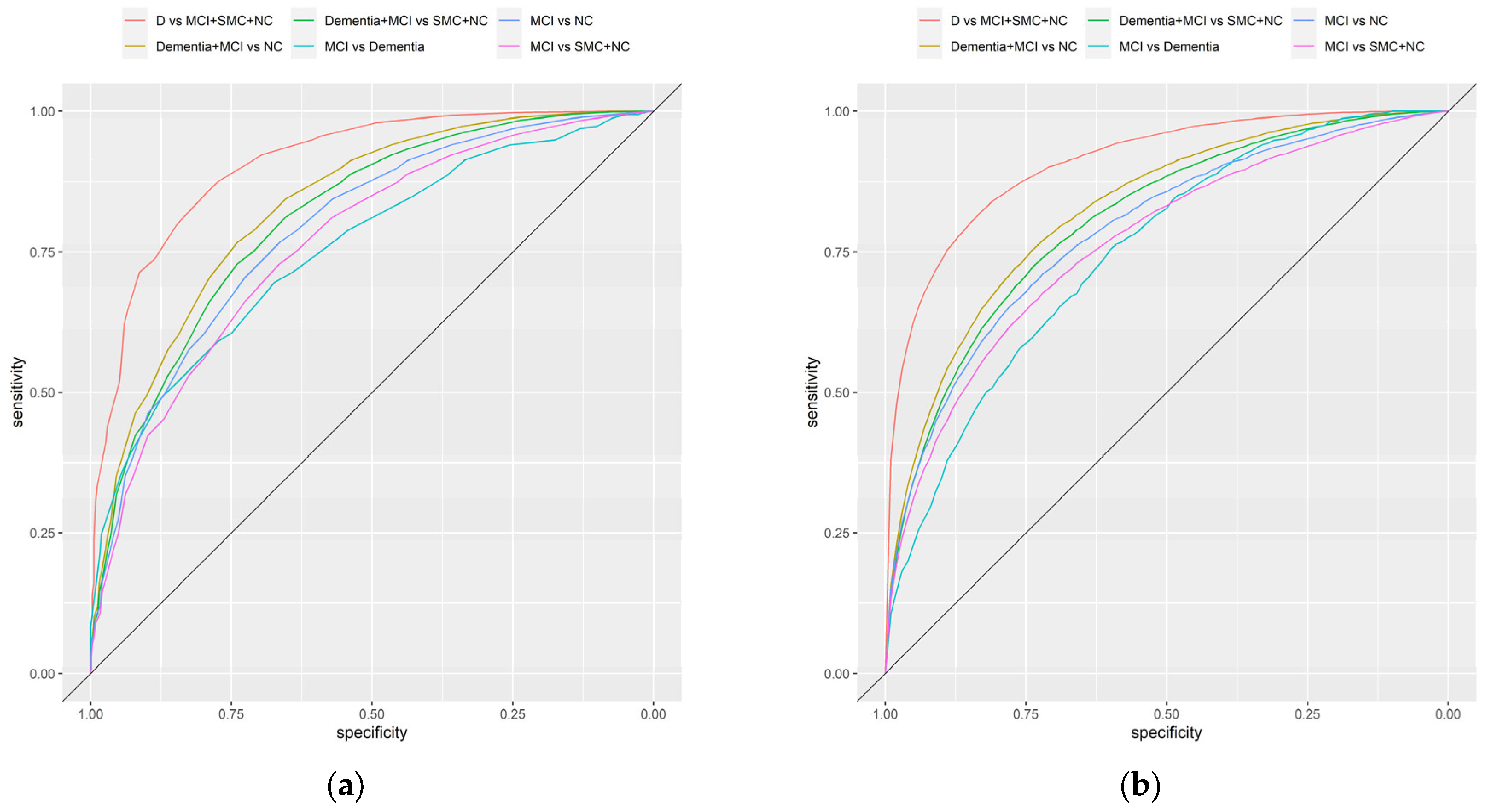
3.4. SHARE-Cog Diagnostic Accuracy
3.5. Adjusting for Covariates
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations. World Population Prospects 2022: Summary of Results; United Nations: New York, NY, USA, 2022; ISBN 978-92-1-001438-0. [Google Scholar]
- Park, H.L.; O’Connell, J.E.; Thomson, R.G. A Systematic Review of Cognitive Decline in the General Elderly Population. Int. J. Geriat. Psychiatry 2003, 18, 1121–1134. [Google Scholar] [CrossRef]
- Nichols, E.; Steinmetz, J.D.; Vollset, S.E.; Fukutaki, K.; Chalek, J.; Abd-Allah, F.; Abdoli, A.; Abualhasan, A.; Abu-Gharbieh, E.; Akram, T.T.; et al. Estimation of the Global Prevalence of Dementia in 2019 and Forecasted Prevalence in 2050: An Analysis for the Global Burden of Disease Study 2019. Lancet Public Health 2022, 7, e105–e125. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, A.J.; Shiri-Feshki, M. Rate of Progression of Mild Cognitive Impairment to Dementia—Meta-Analysis of 41 Robust Inception Cohort Studies. Acta Psychiatr. Scand. 2009, 119, 252–265. [Google Scholar] [CrossRef]
- Mendonça, M.D.; Alves, L.; Bugalho, P. From Subjective Cognitive Complaints to Dementia: Who Is at Risk? A Systematic Review. Am. J. Alzheimer’s Dis. Other Dement. 2016, 31, 105–114. [Google Scholar] [CrossRef]
- Ngandu, T.; Lehtisalo, J.; Solomon, A.; Levälahti, E.; Ahtiluoto, S.; Antikainen, R.; Bäckman, L.; Hänninen, T.; Jula, A.; Laatikainen, T.; et al. A 2 Year Multidomain Intervention of Diet, Exercise, Cognitive Training, and Vascular Risk Monitoring versus Control to Prevent Cognitive Decline in at-Risk Elderly People (FINGER): A Randomised Controlled Trial. Lancet 2015, 385, 2255–2263. [Google Scholar] [CrossRef] [PubMed]
- Cummings, J.; Passmore, P.; McGuinness, B.; Mok, V.; Chen, C.; Engelborghs, S.; Woodward, M.; Manzano, S.; Garcia-Ribas, G.; Cappa, S.; et al. Souvenaid in the Management of Mild Cognitive Impairment: An Expert Consensus Opinion. Alzheimer’s Res. Ther. 2019, 11, 73. [Google Scholar] [CrossRef] [PubMed]
- Canadian Task Force on Preventive Health Care; Pottie, K.; Rahal, R.; Jaramillo, A.; Birtwhistle, R.; Thombs, B.D.; Singh, H.; Gorber, S.C.; Dunfield, L.; Shane, A.; et al. Recommendations on Screening for Cognitive Impairment in Older Adults. CMAJ 2016, 188, 37–46. [Google Scholar] [CrossRef]
- Lin, J.S.; O’Connor, E.; Rossom, R.C.; Perdue, L.A.; Eckstrom, E. Screening for Cognitive Impairment in Older Adults: A Systematic Review for the U.S. Prev. Serv. Task Force. Ann. Intern. Med. 2013, 159, 601–612. [Google Scholar] [CrossRef]
- US Preventive Services Task Force; Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Doubeni, C.A.; Epling, J.W.; Kubik, M.; et al. Screening for Cognitive Impairment in Older Adults: US Preventive Services Task Force Recommendation Statement. JAMA 2020, 323, 757–763. [Google Scholar] [CrossRef]
- Borson, S.; Frank, L.; Bayley, P.J.; Boustani, M.; Dean, M.; Lin, P.; McCarten, J.R.; Morris, J.C.; Salmon, D.P.; Schmitt, F.A.; et al. Improving Dementia Care: The Role of Screening and Detection of Cognitive Impairment. Alzheimer’s Dement. 2013, 9, 151–159. [Google Scholar] [CrossRef]
- Karimi, L.; Mahboub–Ahari, A.; Jahangiry, L.; Sadeghi-Bazargani, H.; Farahbakhsh, M. A Systematic Review and Meta-Analysis of Studies on Screening for Mild Cognitive Impairment in Primary Healthcare. BMC Psychiatry 2022, 22, 97. [Google Scholar] [CrossRef]
- Larner, A. Performance-Based Cognitive Screening Instruments: An Extended Analysis of the Time versus Accuracy Trade-Off. Diagnostics 2015, 5, 504–512. [Google Scholar] [CrossRef]
- Casagrande, M.; Marselli, G.; Agostini, F.; Forte, G.; Favieri, F.; Guarino, A. The Complex Burden of Determining Prevalence Rates of Mild Cognitive Impairment: A Systematic Review. Front. Psychiatry 2022, 13, 960648. [Google Scholar] [CrossRef]
- Bai, W.; Chen, P.; Cai, H.; Zhang, Q.; Su, Z.; Cheung, T.; Jackson, T.; Sha, S.; Xiang, Y.-T. Worldwide Prevalence of Mild Cognitive Impairment among Community Dwellers Aged 50 Years and Older: A Meta-Analysis and Systematic Review of Epidemiology Studies. Age Ageing 2022, 51, afac173. [Google Scholar] [CrossRef]
- Pessoa, R.M.P.; Bomfim, A.J.L.; Ferreira, B.L.C.; Chagas, M.H.N. Diagnostic Criteria and Prevalence of Mild Cognitive Impairment in Older Adults Living in the Community: A Systematic Review and Meta-Analysis. Arch. Clin. Psychiatry 2019, 46, 72–79. [Google Scholar] [CrossRef]
- Luck, T.; Luppa, M.; Briel, S.; Riedel-Heller, S. Incidence of mild cognitive impairment—A systematic review. Dement. Geriatr. Cogn. Disord. 2010, 29, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Sachdev, P.S.; Lipnicki, D.M.; Kochan, N.A.; Crawford, J.D.; Thalamuthu, A.; Andrews, G.; Brayne, C.; Matthews, F.E.; Stephan, B.C.M.; Lipton, R.B.; et al. The Prevalence of Mild Cognitive Impairment in Diverse Geographical and Ethnocultural Regions: The COSMIC Collaboration. PLoS ONE 2015, 10, e0142388. [Google Scholar] [CrossRef]
- Gillis, C.; Mirzaei, F.; Potashman, M.; Ikram, M.A.; Maserejian, N. The Incidence of Mild Cognitive Impairment: A Systematic Review and Data Synthesis. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2019, 11, 248–256. [Google Scholar] [CrossRef]
- Maelstrom Research Integrative Analysis of Longitudinal Studies of Aging and Dementia. Available online: http://www.maelstrom-research.org/ (accessed on 24 July 2023).
- Lee, J.; Chien, S.; Phillips, D.; Weerman, B.; Wilkens, J.; Chen, Y.; Green, H.; Petrosyan, S.; Shao, K.; Young, C.; et al. Gateway to Global Aging Data. Available online: https://g2aging.org/ (accessed on 24 July 2023).
- NACDA NACDA: National Archive of Computerized Data on Aging. Available online: https://www.icpsr.umich.edu/web/pages/NACDA/index.html (accessed on 24 July 2023).
- Stefler, D.; Prina, M.; Wu, Y.-T.; Sánchez-Niubò, A.; Lu, W.; Haro, J.M.; Marmot, M.; Bobak, M. Socioeconomic Inequalities in Physical and Cognitive Functioning: Cross-Sectional Evidence from 37 Cohorts across 28 Countries in the ATHLOS Project. J. Epidemiol. Community Health 2021, 75, 980–986. [Google Scholar] [CrossRef]
- Céline, D.L.; Feeney, J.; Kenny, R.A. The CANDID Initiative. Leveraging Cognitive Ageing Dementia Data from Around the World; The Irish Longitudinal Study on Ageing: Dublin, Ireland, 2021. [Google Scholar]
- Börsch-Supan, A. Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 8. Release Version: 8.0.0. SHARE-ERIC. Data Set. 2022. Available online: https://share-eric.eu/data/data-documentation/waves-overview/wave-8 (accessed on 7 July 2023).
- Börsch-Supan, A.; Brandt, M.; Hunkler, C.; Kneip, T.; Korbmacher, J.; Malter, F.; Schaan, B.; Stuck, S.; Zuber, S. Data Resource Profile: The Survey of Health, Ageing and Retirement in Europe (SHARE). Int. J. Epidemiol. 2013, 42, 992–1001. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool For Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- UNESCO. International Standard Classification of Education ISCED 1997; English edition.-Re-edition.; UNESCO-UIS: Montreal, QC, Canada, 2006; ISBN 978-92-9189-035-4. [Google Scholar]
- Fernández-Alvira, J.M.; Mouratidou, T.; Bammann, K.; Hebestreit, A.; Barba, G.; Sieri, S.; Reisch, L.; Eiben, G.; Hadjigeorgiou, C.; Kovacs, E.; et al. Parental Education and Frequency of Food Consumption in European Children: The IDEFICS Study. Public Health Nutr. 2013, 16, 487–498. [Google Scholar] [CrossRef] [PubMed]
- van Oyen, H.; Van der Heyden, J.; Perenboom, R.; Jagger, C. Monitoring Population Disability: Evaluation of a New Global Activity Limitation Indicator (GALI). Soz. Präventivmed. 2006, 51, 153–161. [Google Scholar] [CrossRef] [PubMed]
- Romero-Ortuno, R.; Walsh, C.D.; Lawlor, B.A.; Kenny, R.A. A Frailty Instrument for Primary Care: Findings from the Survey of Health, Ageing and Retirement in Europe (SHARE). BMC Geriatr. 2010, 10, 57. [Google Scholar] [CrossRef]
- Mast, B.T.; Yochim, B.P. Alzheimer’s Disease and Dementia; Advances in Psychotherapy Series; Hogrefe: Boston, MA, USA; Göttingen, Germany, 2018; ISBN 978-1-61676-503-3. [Google Scholar]
- Petersen, R.C.; Caracciolo, B.; Brayne, C.; Gauthier, S.; Jelic, V.; Fratiglioni, L. Mild Cognitive Impairment: A Concept in Evolution. J. Intern. Med. 2014, 275, 214–228. [Google Scholar] [CrossRef] [PubMed]
- Estrella, A. WHICH PSEUDO R-SQUARED? CONCLUSIVE NEW EVIDENCE; Finance, Economics and Monetary Policy Discussion Papers; Discussion Paper No. 2202. 2022. Available online: http://financeecon.com/DPs/DP2202.pdf (accessed on 28 July 2023).
- Estrella, A. A New Measure of Fit for Equations With Dichotomous Dependent Variables. J. Bus. Econ. Stat. 1998, 16, 198–205. [Google Scholar] [CrossRef]
- Azen, R.; Traxel, N. Using Dominance Analysis to Determine Predictor Importance in Logistic Regression. J. Educ. Behav. Stat. 2009, 34, 319–347. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong, D.M.; Clarke-Pearson, D.L. Comparing the Areas under Two or More Correlated Receiver Operating Characteristic Curves: A Nonparametric Approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef]
- Janes, H.; Pepe, M.S. Adjusting for Covariate Effects on Classification Accuracy Using the Covariate-Adjusted Receiver Operating Characteristic Curve. Biometrika 2009, 96, 371–382. [Google Scholar] [CrossRef]
- Šimundić, A.-M. Measures of Diagnostic Accuracy: Basic Definitions. EJIFCC 2009, 19, 203–211. [Google Scholar]
- Adawi, M.; Zerbetto, R.; Re, T.S.; Bisharat, B.; Mahamid, M.; Amital, H.; Del Puente, G.; Bragazzi, N.L. Psychometric Properties of the Brief Symptom Inventory in Nomophobic Subjects: Insights from Preliminary Confirmatory Factor, Exploratory Factor, and Clustering Analyses in a Sample of Healthy Italian Volunteers. Psychol. Res. Behav. Manag. 2019, 12, 145. [Google Scholar] [CrossRef] [PubMed]
- O’Caoimh, R.; Gao, Y.; Gallagher, P.F.; Eustace, J.; McGlade, C.; Molloy, D.W. Which part of the Quick mild cognitive impairment screen (Qmci) discriminates between normal cognition, mild cognitive impairment and dementia? Age Ageing 2013, 42, 324–330. [Google Scholar] [CrossRef]
- Ahrenfeldt, L.J.; Lindahl-Jacobsen, R.; Rizzi, S.; Thinggaard, M.; Christensen, K.; Vaupel, J.W. Comparison of Cognitive and Physical Functioning of Europeans in 2004–05 and 2013. Int. J. Epidemiol. 2018, 47, 1518–1528. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, R.; Midão, L.; Almada, M.; Costa, E. Cognitive Performance in Older Adults across Europe Based on the SHARE Database. Aging Neuropsychol. Cogn. 2021, 28, 584–599. [Google Scholar] [CrossRef] [PubMed]
- Formanek, T.; Kagstrom, A.; Winkler, P.; Cermakova, P. Differences in Cognitive Performance and Cognitive Decline across European Regions: A Population-Based Prospective Cohort Study. Eur. Psychiatry 2019, 58, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Casaletto, K.B.; Marx, G.; Dutt, S.; Neuhaus, J.; Saloner, R.; Kritikos, L.; Miller, B.; Kramer, J.H. Is “Learning” Episodic Memory? Distinct Cognitive and Neuroanatomic Correlates of Immediate Recall during Learning Trials in Neurologically Normal Aging and Neurodegenerative Cohorts. Neuropsychologia 2017, 102, 19–28. [Google Scholar] [CrossRef]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-Mental State”. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- O’Caoimh, R.; Gao, Y.; McGlade, C.; Healy, L.; Gallagher, P.; Timmons, S.; Molloy, D.W. Comparison of the Quick Mild Cognitive Impairment (Qmci) Screen and the SMMSE in Screening for Mild Cognitive Impairment. Age Ageing 2012, 41, 624–629. [Google Scholar] [CrossRef]
- Pellicer-Espinosa, I.; Díaz-Orueta, U. Cognitive Screening Instruments for Older Adults with Low Educational and Literacy Levels: A Systematic Review. J. Appl. Gerontol. 2022, 41, 1222–1231. [Google Scholar] [CrossRef]
- Goldberg, T.E.; Harvey, P.D.; Wesnes, K.A.; Snyder, P.J.; Schneider, L.S. Practice Effects Due to Serial Cognitive Assessment: Implications for Preclinical Alzheimer’s Disease Randomized Controlled Trials. Alzheimer’s Dement. Diagn. Assess. Dis. Monit. 2015, 1, 103–111. [Google Scholar] [CrossRef]
- Hu, M.; Gao, Y.; Kwok, T.C.Y.; Shao, Z.; Xiao, L.D.; Feng, H. Derivation and Validation of the Cognitive Impairment Prediction Model in Older Adults: A National Cohort Study. Front. Aging Neurosci. 2022, 14, 755005. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
| Descriptive Variable | Total (n = 20,752) | Dementia (n = 335) | MCI (n = 778) | SMC (n = 4957) | NC (n = 14,682) | Difference (p-Value) |
|---|---|---|---|---|---|---|
| Age: 65–74 years | 56% | 27% | 49% | 46% | 61% | <0.001 |
| Age: 75–84 years | 35% | 47% | 37% | 42% | 33% | |
| Age: ≥85 years | 8% | 26% | 14% | 12% | 6% | |
| Female | 55% | 59% | 58% | 54% | 55% | 0.046 |
| Education level: low | 35% | 50% | 49% | 39% | 33% | <0.001 |
| Education level: medium | 40% | 33% | 31% | 39% | 41% | |
| Education level: high | 24% | 17% | 19% | 21% | 26% | |
| GALI 1: activities not limited | 51% | 12% | 33% | 40% | 57% | <0.001 |
| GALI 1: limited but not severely | 35% | 31% | 41% | 40% | 32% | |
| GALI 1: severely limited | 14% | 57% | 26% | 19% | 11% | |
| Lives alone | 29% | 37% | 36% | 32% | 27% | <0.001 |
| Employed | 4% | 0% | 2% | 4% | 5% | <0.001 |
| Multimorbidity | 53% | 72% | 65% | 59% | 50% | <0.001 |
| Eyesight problems | 18% | 43% | 33% | 27% | 14% | <0.001 |
| Hearing problems | 22% | 42% | 37% | 36% | 15% | <0.001 |
| Low self-rated health | 37% | 80% | 64% | 57% | 28% | <0.001 |
| Physical frailty | 7% | 43% | 15% | 9% | 5% | <0.001 |
| Hospitalisation 2 | 16% | 34% | 20% | 19% | 15% | <0.001 |
| Diagnostic Comparisons | Regression Coefficients | Scoring * | Model Performance | Dominance Analysis ** | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Groups Being Compared | (Intercept) | Word Registration | Verbal Fluency | Delayed Recall | Rounded Score per Word | AUC | Word Registration | Verbal Fluency | Delayed Recall | |
| (D + MCI) vs. (SMC + NC) | 0.877 | −0.218 | −0.109 | −0.296 | 2:1:3 | 0.811 | 0.141 | 0.025 | 0.032 | 0.028 |
| (D + MCI) vs. (NC) | 1.524 | −0.244 | −0.109 | −0.347 | 2:1:3 | 0.831 | 0.199 | 0.038 | 0.044 | 0.045 |
| MCI vs. D | −1.722 | 0.322 | 0.106 | 0.054 | 6:2:1 | 0.765 | 0.212 | 0.076 | 0.086 | 0.036 |
| MCI vs. (SMC + NC) | −0.228 | −0.12 | −0.085 | −0.288 | 1:1:3 | 0.767 | 0.053 | 0.01 | 0.014 | 0.015 |
| MCI vs. NC | 0.511 | −0.158 | −0.088 | −0.334 | 2:1:4 | 0.791 | 0.091 | 0.017 | 0.021 | 0.026 |
| D vs. (MCIc+ SMC + NC) | 1.312 | −0.444 | −0.186 | −0.353 | 2:1:2 | 0.908 | 0.211 | 0.022 | 0.027 | 0.017 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Donovan, M.R.; Cornally, N.; O’Caoimh, R. Validation of a Harmonised, Three-Item Cognitive Screening Instrument for the Survey of Health, Ageing and Retirement in Europe (SHARE-Cog). Int. J. Environ. Res. Public Health 2023, 20, 6869. https://doi.org/10.3390/ijerph20196869
O’Donovan MR, Cornally N, O’Caoimh R. Validation of a Harmonised, Three-Item Cognitive Screening Instrument for the Survey of Health, Ageing and Retirement in Europe (SHARE-Cog). International Journal of Environmental Research and Public Health. 2023; 20(19):6869. https://doi.org/10.3390/ijerph20196869
Chicago/Turabian StyleO’Donovan, Mark R., Nicola Cornally, and Rónán O’Caoimh. 2023. "Validation of a Harmonised, Three-Item Cognitive Screening Instrument for the Survey of Health, Ageing and Retirement in Europe (SHARE-Cog)" International Journal of Environmental Research and Public Health 20, no. 19: 6869. https://doi.org/10.3390/ijerph20196869
APA StyleO’Donovan, M. R., Cornally, N., & O’Caoimh, R. (2023). Validation of a Harmonised, Three-Item Cognitive Screening Instrument for the Survey of Health, Ageing and Retirement in Europe (SHARE-Cog). International Journal of Environmental Research and Public Health, 20(19), 6869. https://doi.org/10.3390/ijerph20196869