
Enhancing Driving Ability in Older Adults through Health Exercises and Physical Activity: A Randomized Controlled Trial


Abstract
1. Introduction
2. Materials and Methods
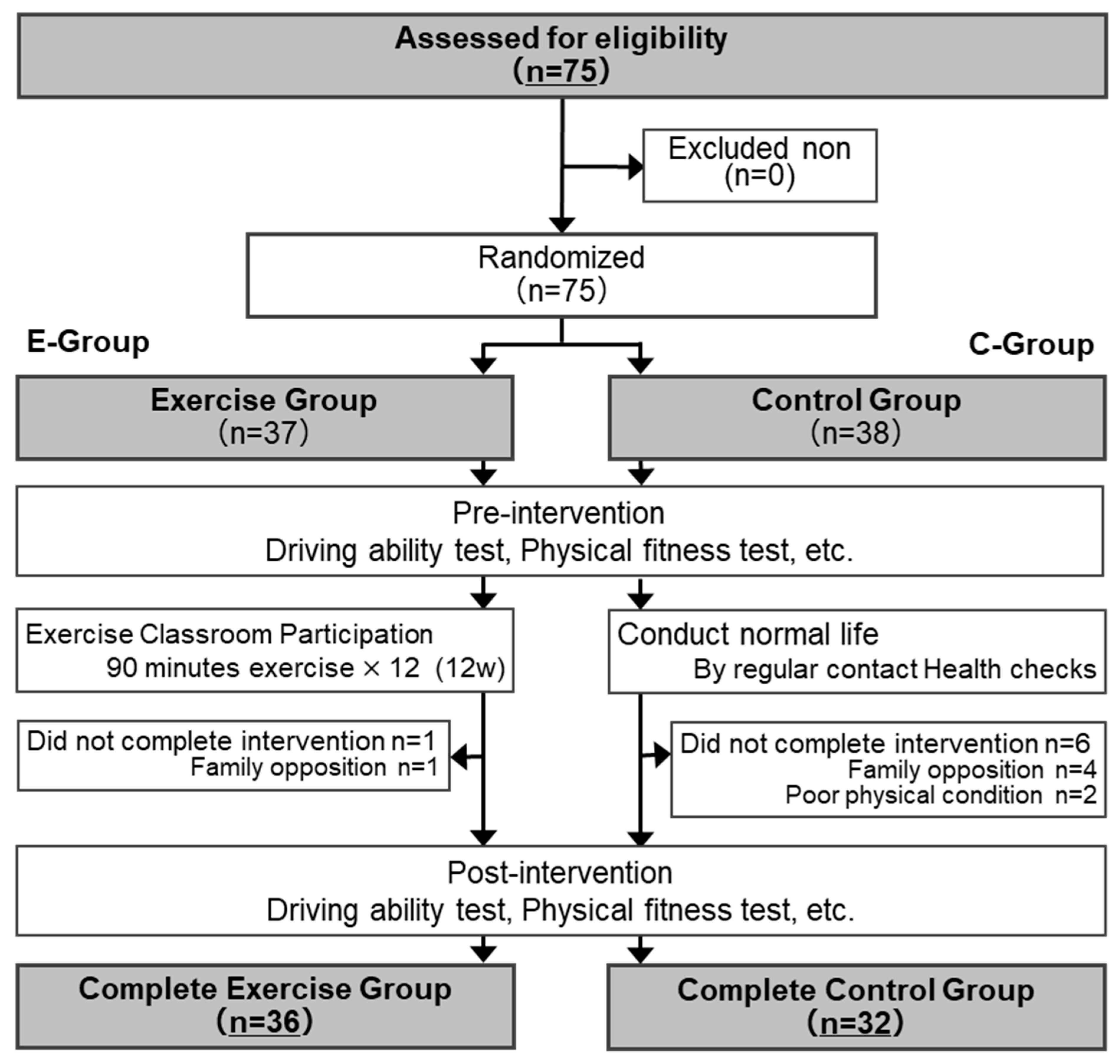
2.1. Participants
2.2. Study Design
2.3. Sample Size
2.4. Clinical Parameters and Measurements
2.5. Driving Ability Measurement
2.6. Physical Fitness
2.7. Measures of Executive Functioning and Attentional Functioning
2.8. Statistical Analysis
2.9. Response to Blinding
2.10. Ethics
3. Results
3.1. Clinical Characteristics of Enrolled Participants at Baseline
3.2. Comparison of the Changes in Parameters between the Two Groups
4. Discussion
4.1. Improvement of Driving Ability
4.2. Methods of Measuring Driving Ability
4.3. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fernandes, F.; Turra, C.M.; Rios Neto, E.L.G. World Population Aging as a Function of Period Demographic Conditions. Demogr. Res. 2023, 48, 353–372. [Google Scholar] [CrossRef]
- United Nations. World Population Prospects–Population Division. Available online: https://population.un.org/wpp/ (accessed on 14 August 2023).
- Mudrazija, S.; Angel, J.L. Population Aging and Public Policy. In International Handbook of Population Policies; May, J.F., Goldstone, J.A., Eds.; Springer International Publishing: Cham, Switzerland, 2022; pp. 551–570. ISBN 978-3-031-02040-7. [Google Scholar]
- Jeong, S.-H.; Kim, E.-Y.; Lee, S.-J.; Choi, W.-J.; Oh, C.; Sung, H.-J.; Kim, J. Health Status and Activity Discomfort among Elderly Drivers: Reality of Health Awareness. Healthcare 2023, 11, 563. [Google Scholar] [CrossRef] [PubMed]
- Mirabet, E.; Tortosa-Perez, M.; Tortosa, F.; González-Sala, F. Evaluation of Psychophysical Fitness in Drivers Over 65 Years of Age. Healthcare 2023, 11, 1927. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Status Report on Road Safety 2015; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-156506-6. [Google Scholar]
- Falkenstein, M.; Karthaus, M.; Brüne-Cohrs, U. Age-Related Diseases and Driving Safety. Geriatrics 2020, 5, 80. [Google Scholar] [CrossRef] [PubMed]
- Hagiya, H.; Takase, R.; Honda, H.; Nakano, Y.; Otsuka, Y.; Kataoka, H.; Uno, M.; Ueda, K.; Takahashi, M.; Ogawa, H.; et al. Prevalence of Medical Factors Related to Aging among Older Car Drivers: A Multicenter, Cross-Sectional, Descriptive Study. BMC Geriatr. 2022, 22, 792. [Google Scholar] [CrossRef]
- Park, K.; Renge, K.; Nakagawa, Y.; Yamashita, F.; Tada, M.; Kumagai, Y. Aging Brains Degrade Driving Safety Performances of the Healthy Elderly. Front. Aging Neurosci. 2022, 13, 783717. [Google Scholar] [CrossRef]
- Cabinet Office. 2020 Traffic Safety White Paper. Available online: https://www8.cao.go.jp/koutu/taisaku/r02kou_haku/zenbun/index.html (accessed on 14 August 2023).
- Voluntary Return of Driver’s License: Japan National Police Agency Web Site. Available online: http://www.npa.go.jp/policies/application/license_renewal/return_DL.html (accessed on 14 August 2023).
- Road Traffic Law Revised in 2020 (Measures for Elderly Drivers, Review of Eligibility for Second-Class Licenses, etc.) (Effective 13 May 2022): Japan National Police Agency Web Site. Available online: http://www.npa.go.jp/bureau/traffic/r2kaisei_main.html (accessed on 14 August 2023).
- Tang, K.F.; Teh, P.-L.; Lim, W.M.; Lee, S.W.H. Perspectives on Mobility among Older Adults Living with Different Frailty and Cognitive Statuses. J. Transp. Health 2022, 24, 101305. [Google Scholar] [CrossRef]
- Che Had, N.H.; Alavi, K.; Md Akhir, N.; Muhammad Nur, I.R.; Shuhaimi, M.S.Z.; Foong, H.F. A Scoping Review of the Factor Associated with Older Adults’ Mobility Barriers. Int. J. Environ. Res. Public Health 2023, 20, 4243. [Google Scholar] [CrossRef]
- Cirella, G.T.; Bąk, M.; Kozlak, A.; Pawłowska, B.; Borkowski, P. Transport Innovations for Elderly People. Res. Transp. Bus. Manag. 2019, 30, 100381. [Google Scholar] [CrossRef]
- Lajunen, T.; Sullman, M.J.M. Attitudes toward Four Levels of Self-Driving Technology among Elderly Drivers. Front. Psychol. 2021, 12, 682973. [Google Scholar] [CrossRef]
- Oxley, J.; Logan, D.B.; Coxon, S.; Koppel, S. Understanding Current and Future Transport Needs of Older Australian Drivers to Guide Development of Sustainable and Smart Initiatives to Support Safe Mobility of Older Adults. Sustainability 2022, 14, 5906. [Google Scholar] [CrossRef]
- Marottoli, R.A.; Allore, H.; Araujo, K.L.B.; Iannone, L.P.; Acampora, D.; Gottschalk, M.; Charpentier, P.; Kasl, S.; Peduzzi, P. A Randomized Trial of a Physical Conditioning Program to Enhance the Driving Performance of Older Persons. J. Gen. Intern. Med. 2007, 22, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Jalenques, I.; Rondepierre, F.; Rachez, C.; Lauron, S.; Guiguet-Auclair, C. Health-Related Quality of Life among Community-Dwelling People Aged 80 Years and over: A Cross-Sectional Study in France. Health Qual. Life Outcomes 2020, 18, 126. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; Brettschneider, C.; Lühmann, D.; van den Bussche, H.; Wiese, B.; Mamone, S.; Weyerer, S.; Werle, J.; Leve, V.; Fuchs, A.; et al. Driving Status and Health-Related Quality of Life among the Oldest Old: A Population-Based Examination Using Data from the AgeCoDe–AgeQualiDe Prospective Cohort Study. Aging Clin. Exp. Res. 2021, 33, 3109–3115. [Google Scholar] [CrossRef] [PubMed]
- Scarabottolo, C.C.; Tebar, W.R.; Gobbo, L.A.; Ohara, D.; Ferreira, A.D.; da Silva Canhin, D.; Christofaro, D.G.D. Analysis of Different Domains of Physical Activity with Health-Related Quality of Life in Adults: 2-Year Cohort. Health Qual. Life Outcomes 2022, 20, 71. [Google Scholar] [CrossRef]
- Kaushal, N.; Langlois, F.; Desjardins-Crépeau, L.; Hagger, M.S.; Bherer, L. Investigating Dose–Response Effects of Multimodal Exercise Programs on Health-Related Quality of Life in Older Adults. Clin. Interv. Aging 2019, 14, 209–217. [Google Scholar] [CrossRef]
- Kitaoka, H.; Kurahashi, T.; Mori, H.; Iwase, T.; Machida, T.; Kozato, A.; Yamashita, M.; Kisanuki, Y. A Development of a Traffic Simulator for Safety Evaluation–Reproduction of Traffic Accidents and Evaluation of Safety Systems. Rev. Automot. Eng. 2009, 30, 211–217. [Google Scholar] [CrossRef]
- Ministry of Education, Culture, Sports, Science, and Technology. New Physical Fitness Test Guidelines. Available online: https://www.mext.go.jp/a_menu/sports/stamina/03040901.htm (accessed on 14 August 2023).
- Sports Agency. New Fitness Test Guideline. Available online: https://www.mext.go.jp/sports/b_menu/sports/mcatetop03/list/detail/1408001.htm (accessed on 14 August 2023).
- Kawabata, Y.; Hiura, M. The CS-30 Test Is a Useful Assessment Tool for Predicting Falls in Community-Dwelling Elderly People. Rigakuryoho Kagaku 2008, 23, 441–445. [Google Scholar] [CrossRef]
- Nakazono, T.; Kamide, N.; Ando, M. The Reference Values for the Chair Stand Test in Healthy Japanese Older People: Determination by Meta-analysis. J. Phys. Ther. Sci. 2014, 26, 1729–1731. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Tiedemann, A.; Shimada, H.; Sherrington, C.; Murray, S.; Lord, S. The Comparative Ability of Eight Functional Mobility Tests for Predicting Falls in Community-Dwelling Older People. Age Ageing 2008, 37, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar] [CrossRef] [PubMed]
- Sprint, G.; Cook, D.J.; Weeks, D.L. Toward Automating Clinical Assessments: A Survey of the Timed Up and Go. IEEE Rev. Biomed. Eng. 2015, 8, 64–77. [Google Scholar] [CrossRef] [PubMed]
- Giovagnoli, A.R.; Del Pesce, M.; Mascheroni, S.; Simoncelli, M.; Laiacona, M.; Capitani, E. Trail Making Test: Normative Values from 287 Normal Adult Controls. Ital. J. Neurol. Sci. 1996, 17, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Tombaugh, T.N. Trail Making Test A and B: Normative Data Stratified by Age and Education. Arch. Clin. Neuropsychol. 2004, 19, 203–214. [Google Scholar] [CrossRef]
- Bowie, C.R.; Harvey, P.D. Administration and Interpretation of the Trail Making Test. Nat. Protoc. 2006, 1, 2277–2281. [Google Scholar] [CrossRef]
- Harada, H.; Notoya, M.; Nakanishi, M.; Fujiwara, N.; Inoue, K. Effects of Age and Years of Education on Neuropsychological Data of Japanese Healthy Elderly Persons. High. Brain Funct. Res. 2006, 26, 16–24. [Google Scholar] [CrossRef]
- Hirota, C.; Watanabe, M.; Tanimoto, Y.; Kono, R.; Higuchi, Y.; Kono, K. A Cross-Sectional Study on the Relationship between the Trail Making Test and Mobility–Related Functions in Community-Dwelling Elderly. Nihon Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2008, 45, 647–654. [Google Scholar] [CrossRef][Green Version]
- Yamada, M. Examination of the Preventive Effect of Attention Function Training on Falls for Community Dwelling Elderly: A Randomized Control Trial. Rigakuryoho Kagaku 2009, 24, 71–76. [Google Scholar] [CrossRef][Green Version]
- Kamide, N.; Tanaka, M.; Kawamorita, T. Physical Function as well as Cognitive Function Influences the Automobile Driving Ability of Older Adults: Investigation Using a Driving Simulator. Rigakuryoho Kagaku 2019, 34, 777–781. [Google Scholar] [CrossRef]
- Kose, Y.; Ikenaga, M.; Yamada, Y.; Takeda, N.; Morimura, K.; Kimura, M.; Kiyonaga, A.; Higaki, Y.; Nakagawa Study Group. Physical Parameters and Physical Function in Older Drivers with Driving-Related Anxiety: The Nakagawa Study. Nihon Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2020, 57, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, F.; Jacinto, M.; Figueiredo, N.; Monteiro, A.M.; Forte, P. Effects of a 24-Week Low-Cost Multicomponent Exercise Program on Health-Related Functional Fitness in the Community-Dwelling Aged and Older Adults. Medicina 2023, 59, 371. [Google Scholar] [CrossRef] [PubMed]
- Middleton, G.; Hambrook, R.; Bishop, D.C.; Crust, L.; Broom, D.R. Examining the New-Member Effect to an Established Community-Based Physical Activity Program for Older Adults in England. Int. J. Environ. Res. Public Health 2023, 20, 6161. [Google Scholar] [CrossRef] [PubMed]
- Carta, M.G.; Cossu, G.; Pintus, E.; Zaccheddu, R.; Callia, O.; Conti, G.; Pintus, M.; Aviles Gonzalez, C.I.; Massidda, M.V.; Mura, G.; et al. Moderate Exercise Improves Cognitive Function in Healthy Elderly People: Results of a Randomized Controlled Trial. Clin. Pract. Epidemiol. Ment. Health 2021, 17, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.B.; Xu, X.; Lin, J.-H.; Radwin, R.G. Evaluation of Older Driver Head Functional Range of Motion Using Portable Immersive Virtual Reality. Exp. Gerontol. 2015, 70, 150–156. [Google Scholar] [CrossRef]
- Gökçe, E.; Stojan, R.; Mack, M.; Bock, O.; Voelcker-Rehage, C. Lifestyle Matters: Effects of Habitual Physical Activity on Driving Skills in Older Age. Brain Sci. 2022, 12, 608. [Google Scholar] [CrossRef]
- Huisingh, C.; McGwin, G., Jr.; Orman, K.A.; Owsley, C. Frequent Falling and Motor Vehicle Collision Involvement of Older Drivers. J. Am. Geriatr. Soc. 2014, 62, 123–129. [Google Scholar] [CrossRef]
- Karthaus, M.; Falkenstein, M. Functional Changes and Driving Performance in Older Drivers: Assessment and Interventions. Geriatrics 2016, 1, 12. [Google Scholar] [CrossRef]
- Huang, C.H.; Okada, K.; Matsushita, E.; Uno, C.; Satake, S.; Martins, B.A.; Kuzuya, M. The Association of Social Frailty with Intrinsic Capacity in Community-Dwelling Older Adults: A Prospective Cohort Study. BMC Geriatr. 2021, 21, 515. [Google Scholar] [CrossRef]
- Ko, Y.; Lee, K. Social Frailty and Health-Related Quality of Life in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 5659. [Google Scholar] [CrossRef]
- Ayeni, A.; Sharples, A.; Hewson, D. The Association between Social Vulnerability and Frailty in Community Dwelling Older People: A Systematic Review. Geriatrics 2022, 7, 104. [Google Scholar] [CrossRef]
- Mehrabi, F.; Béland, F. Frailty as a Moderator of the Relationship between Social Isolation and Health Outcomes in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 1675. [Google Scholar] [CrossRef]
- Amagasa, S.; Fukushima, N.; Kikuchi, H.; Takamiya, T.; Odagiri, Y.; Oka, K.; Inoue, S. Drivers Are More Physically Active than Non-drivers in Older Adults. Int. J. Environ. Res. Public Health 2018, 15, 1094. [Google Scholar] [CrossRef]
- Maltese, G.; Corsonello, A.; Di Rosa, M.; Soraci, L.; Vitale, C.; Corica, F.; Lattanzio, F. Frailty and COVID-19: A Systematic Scoping Review. J. Clin. Med. 2020, 9, 2106. [Google Scholar] [CrossRef]
- Kodama, A.; Kume, Y.; Lee, S.; Makizako, H.; Shimada, H.; Takahashi, T.; Ono, T.; Ota, H. Impact of COVID-19 Pandemic Exacerbation of Depressive Symptoms for Social Frailty from the ORANGE Registry. Int. J. Environ. Res. Public Health 2022, 19, 986. [Google Scholar] [CrossRef]
- Lee, H.C.; Cameron, D.; Lee, A.H. Assessing the Driving Performance of Older Adult Drivers: On-Road versus Simulated Driving. Accid. Anal. Prev. 2003, 35, 797–803. [Google Scholar] [CrossRef] [PubMed]
- Groeger, J.A.; Murphy, G. Driver Performance under Simulated and Actual Driving Conditions: Validity and Orthogonality. Accid. Anal. Prev. 2020, 143, 105593. [Google Scholar] [CrossRef] [PubMed]
- Azuma, Y.; Kawano, T.; Moriwaki, T. Evaluation Methods for Driving Performance Using a Driving Simulator under the Condition of Drunk Driving or Talking Driving with a Cell Phone. In Mechatronics for Safety, Security and Dependability in a New Era; Arai, E., Arai, T., Eds.; Elsevier: Oxford, UK, 2007; pp. 181–184. ISBN 978-0-08-044963-0. [Google Scholar]
- Wynne, R.A.; Beanland, V.; Salmon, P.M. Systematic Review of Driving Simulator Validation Studies. Saf. Sci. 2019, 117, 138–151. [Google Scholar] [CrossRef]
- Matas, N.A.; Nettelbeck, T.; Burns, N.R. Dropout during a Driving Simulator Study: A Survival Analysis. J. Saf. Res. 2015, 55, 159–169. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| All Subjects (n = 68) | |||
|---|---|---|---|
| Mean ± SD | Minimum | Maximum | |
| Male, n (%) | 52 (76.5%) | ||
| Age (year) | 74.9 ± 3.8 | 65 | 82 |
| Height (cm) | 155.3 ± 9.0 | 139.7 | 185.0 |
| Body weight (kg) | 56.3 ± 10.6 | 36.6 | 90.0 |
| BMI (kg/m2) | 23.3 ± 3.3 | 17.8 | 37.5 |
| Grip strength (kg) | 23.7 ± 5.2 | 15.4 | 40.1 |
| Flexibility (cm) | 34.0 ± 9.7 | 13.0 | 57.0 |
| One leg with eye opened balance (seconds) | 51.1 ± 41.6 | 1.0 | 120.0 |
| 10 meters walking with obstacles (seconds) | 8.3 ± 1.4 | 6.1 | 12.2 |
| 30 s chair standing up test (times) | 20.9 ± 4.7 | 10.0 | 32.0 |
| Five times chair standing up test (seconds) | 6.6 ± 1.8 | 4.0 | 13.5 |
| Timed Up and Go Test (seconds) | 6.3 ± 1.1 | 4.5 | 9.3 |
| TMT-A: Trail Making Test part A (seconds) | 60.3 ± 23.5 | 38.0 | 176.0 |
| TMT-B: Trail Making Test part B (seconds) | 105.2 ± 45.7 | 37.0 | 300.0 |
| Driving ability Cognition | 9.0 ± 6.2 | 0 | 33 |
| Driving ability Judgment | 5.8 ± 5.2 | 0 | 23 |
| Driving ability Operation | 1.2 ± 2.0 | 0 | 8 |
| Driving ability Cognition + Judgment | 14.8 ± 7.5 | 3 | 34 |
| Driving ability Judgment + Operation | 7.0 ± 5.5 | 0 | 23 |
| Driving ability Cognition + Judgment + Operation | 16.0 ± 7.3 | 3 | 34 |
| E: Exercise Group (n = 36) | C: Control Group (n = 32) | |
|---|---|---|
| Mean ± SD | Mean ± SD | |
| Male, n (%) | 29 (80.1%) | 23 (71.9%) |
| Age (year) | 74.8 ± 3.9 | 75.0 ± 3.6 |
| Height (cm) | 155.6 ± 9.7 | 155.0 ± 8.0 |
| Body weight (kg) | 55.9 ± 12.8 | 56.8 ± 7.2 |
| BMI (kg/m2) | 22.9 ± 3.7 | 23.7 ± 2.7 |
| Grip strength (kg) | 23.4 ± 4.6 | 24.0 ± 5.7 |
| Flexibility (cm) | 34.8 ± 9.4 | 33.0 ± 9.8 |
| One leg with eye opened balance (seconds) | 46.5 ± 39.0 | 56.4 ± 43.1 |
| 10 meters walking with obstacles (seconds) | 8.3 ± 1.4 | 8.3 ± 1.5 |
| 30 s chair standing up test (times) | 21.3 ± 4.0 | 20.5 ± 5.3 |
| Five times chair standing up test (seconds) | 6.4 ± 1.3 | 6.8 ± 2.1 |
| Timed Up and Go Test (seconds) | 6.1 ± 1.0 | 6.5 ± 1.1 |
| TMT-A: Trail Making Test part A (seconds) | 58.5 ± 17.3 | 62.3 ± 28.5 |
| TMT-B: Trail Making Test part B (seconds) | 102.2 ± 37.9 | 108.5 ± 52.3 |
| Driving ability score Cognition | 9.0 ± 5.5 | 9.0 ± 6.8 |
| Driving ability score Judgment | 6.2 ± 5.7 | 5.4 ± 4.4 |
| Driving ability score Operation | 1.3 ± 1.9 | 1.0 ± 2.0 |
| Driving ability score Cognition + Judgment | 15.2 ± 7.3 | 14.3 ± 7.6 |
| Driving ability score Judgment + Operation | 7.5 ± 5.7 | 6.4 ± 5.1 |
| Driving ability score Total | 16.5 ± 7.0 | 15.4 ± 7.4 |
| E: Exercise Group (n = 36) | C: Control Group (n = 32) | ||
|---|---|---|---|
| Mean ± SD | Mean ± SD | p Value | |
| ΔGrip strength (kg) | −1.2 ± 2.5 | 0.2 ± 2.8 | 0.02 |
| ΔFlexibility (cm) | 1.0 ± 6.4 | 4.9 ± 10.9 | 0.04 |
| ΔOne leg with eye opened balance (seconds) | 15.6 ± 34.4 | −4.7 ± 34.0 | 0.01 |
| Δ10 meters walking with obstacles (seconds) | −0.4 ± 0.9 | −0.2 ± 1.0 | 0.24 |
| Δ30 s chair standing up test (times) | 5.7 ± 5.3 | −1.1 ± 5.3 | <0.001 |
| ΔFive times chair standing up test (seconds) | −0.1 ± 1.3 | −0.3 ± 1.3 | 0.23 |
| ΔTimed Up and Go Test (seconds) | −0.6 ± 0.9 | −0.8 ± 0.7 | 0.12 |
| ΔTMT-A: Trail Making Test part A (seconds) | −16.4 ± 12.3 | −19.6 ± 24.4 | 0.24 |
| ΔTMT-B: Trail Making Test part B (seconds) | −2.7 ± 33.9 | 2.1 ± 65.0 | 0.35 |
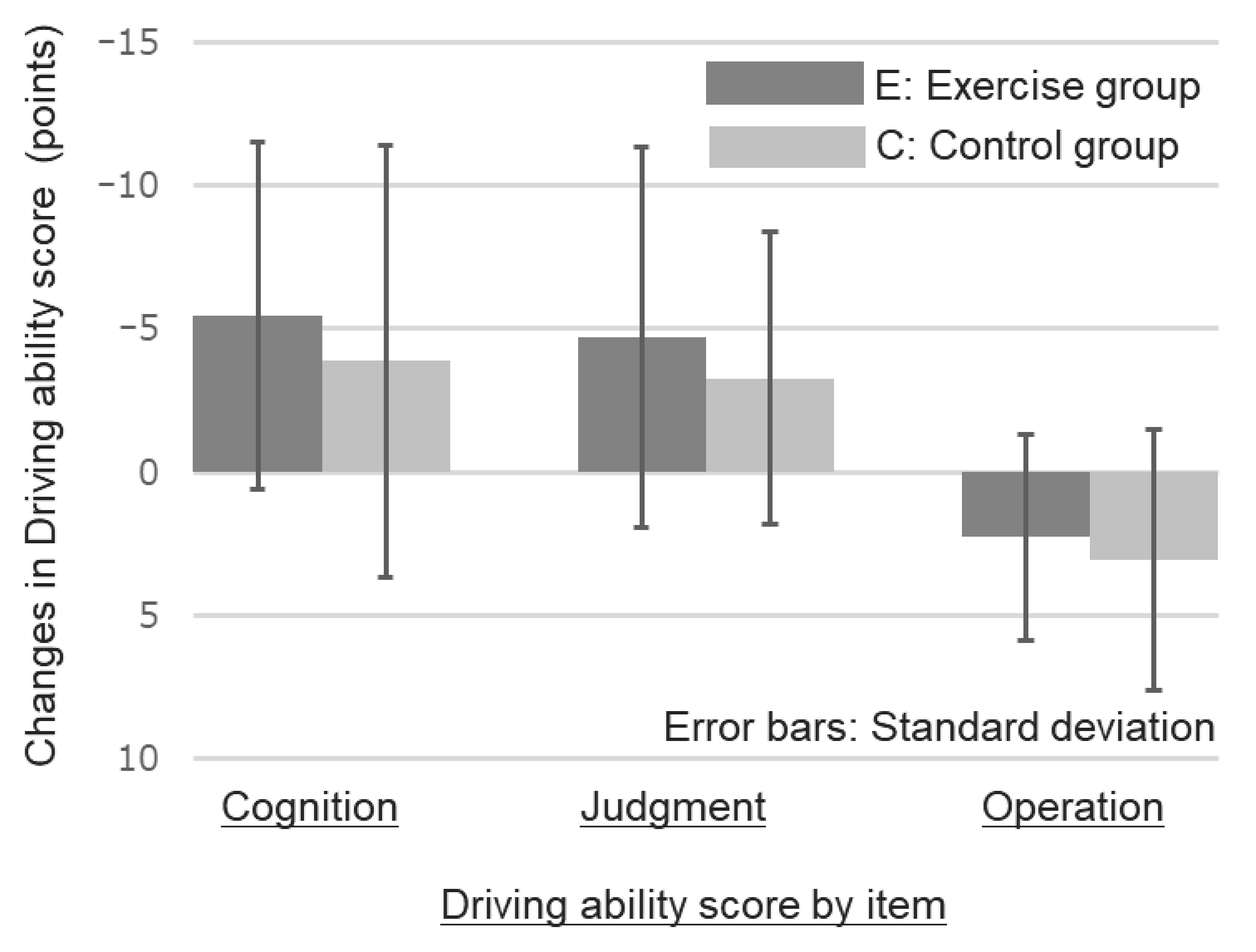
| ΔDriving ability Cognition | −5.44 ± 6.07 | −3.88 ± 7.52 | 0.17 |
| ΔDriving ability Judgment | −4.72 ± 6.63 | −3.28 ± 5.08 | 0.16 |
| ΔDriving ability Operation | 2.28 ± 3.58 | 3.09 ± 4.55 | 0.21 |
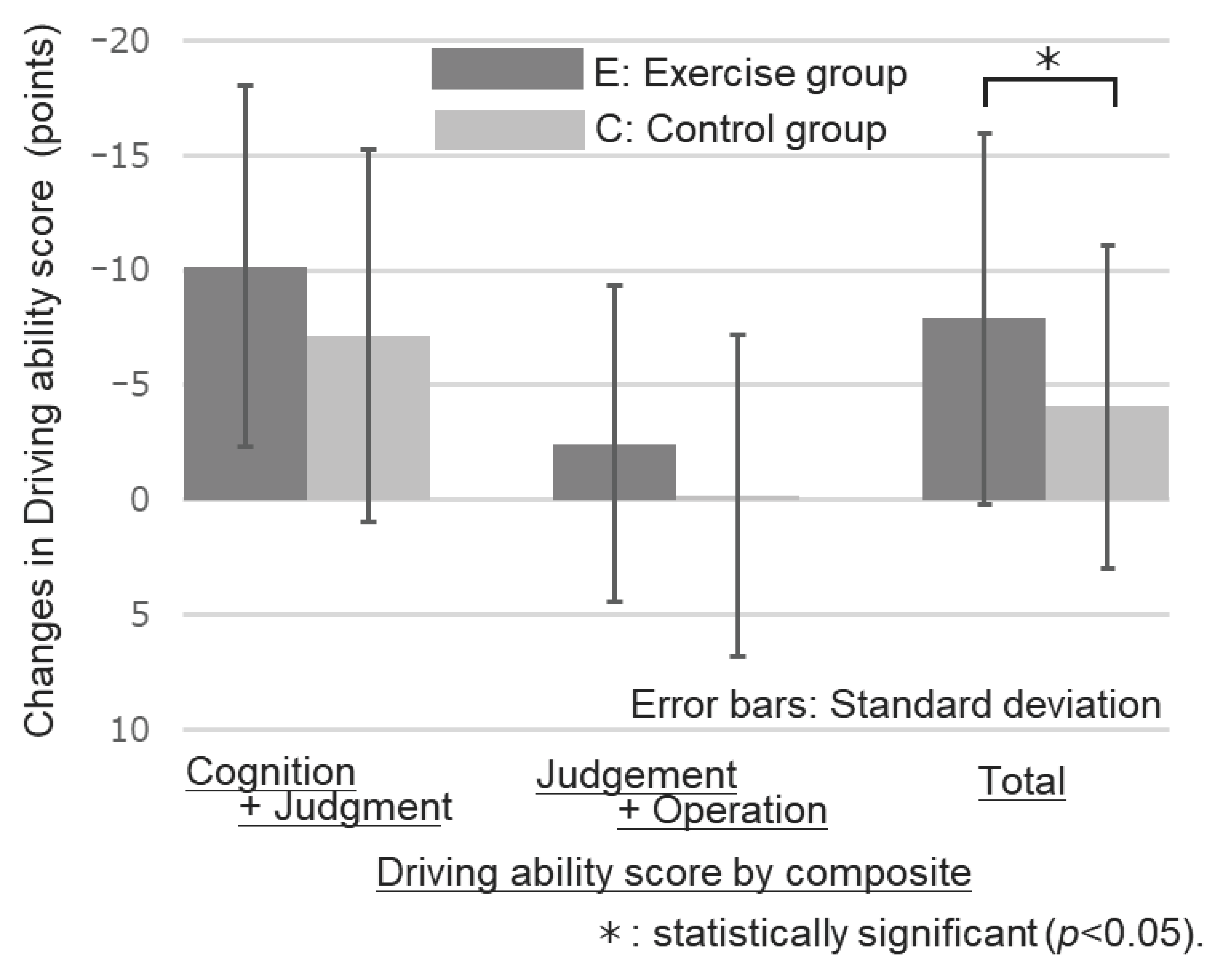
| ΔDriving ability Cognition + Judgment | −10.17 ± 7.84 | −7.16 ± 8.11 | 0.06 |
| ΔDriving ability Judgment + Operation | −2.44 ± 6.91 | −0.19 ± 7.00 | 0.09 |
| ΔDriving ability Total | −7.89 ± 8.07 | −4.06 ± 7.01 | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Katayama, A.; Hase, A.; Miyatake, N. Enhancing Driving Ability in Older Adults through Health Exercises and Physical Activity: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2023, 20, 6802. https://doi.org/10.3390/ijerph20196802
Katayama A, Hase A, Miyatake N. Enhancing Driving Ability in Older Adults through Health Exercises and Physical Activity: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2023; 20(19):6802. https://doi.org/10.3390/ijerph20196802
Chicago/Turabian StyleKatayama, Akihiko, Ayako Hase, and Nobuyuki Miyatake. 2023. "Enhancing Driving Ability in Older Adults through Health Exercises and Physical Activity: A Randomized Controlled Trial" International Journal of Environmental Research and Public Health 20, no. 19: 6802. https://doi.org/10.3390/ijerph20196802
APA StyleKatayama, A., Hase, A., & Miyatake, N. (2023). Enhancing Driving Ability in Older Adults through Health Exercises and Physical Activity: A Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 20(19), 6802. https://doi.org/10.3390/ijerph20196802