
The Magnitude of NCD Risk Factors in Ethiopia: Meta-Analysis and Systematic Review of Evidence

 and
and
Abstract
1. Introduction
2. Methodology
2.1. Protocol
2.2. Context/Setting
2.3. Searches
2.4. Inclusion Criteria and Article Selection
2.5. Measurement of Outcome Variables
2.6. Assessment of Methodological Quality and Selection
2.7. Data Extraction
2.8. Data Analysis and Synthesis
3. Results
3.1. Description of Study Characteristics
3.2. Methodological Quality Appraisal
3.3. NCD Risk Factors Combined
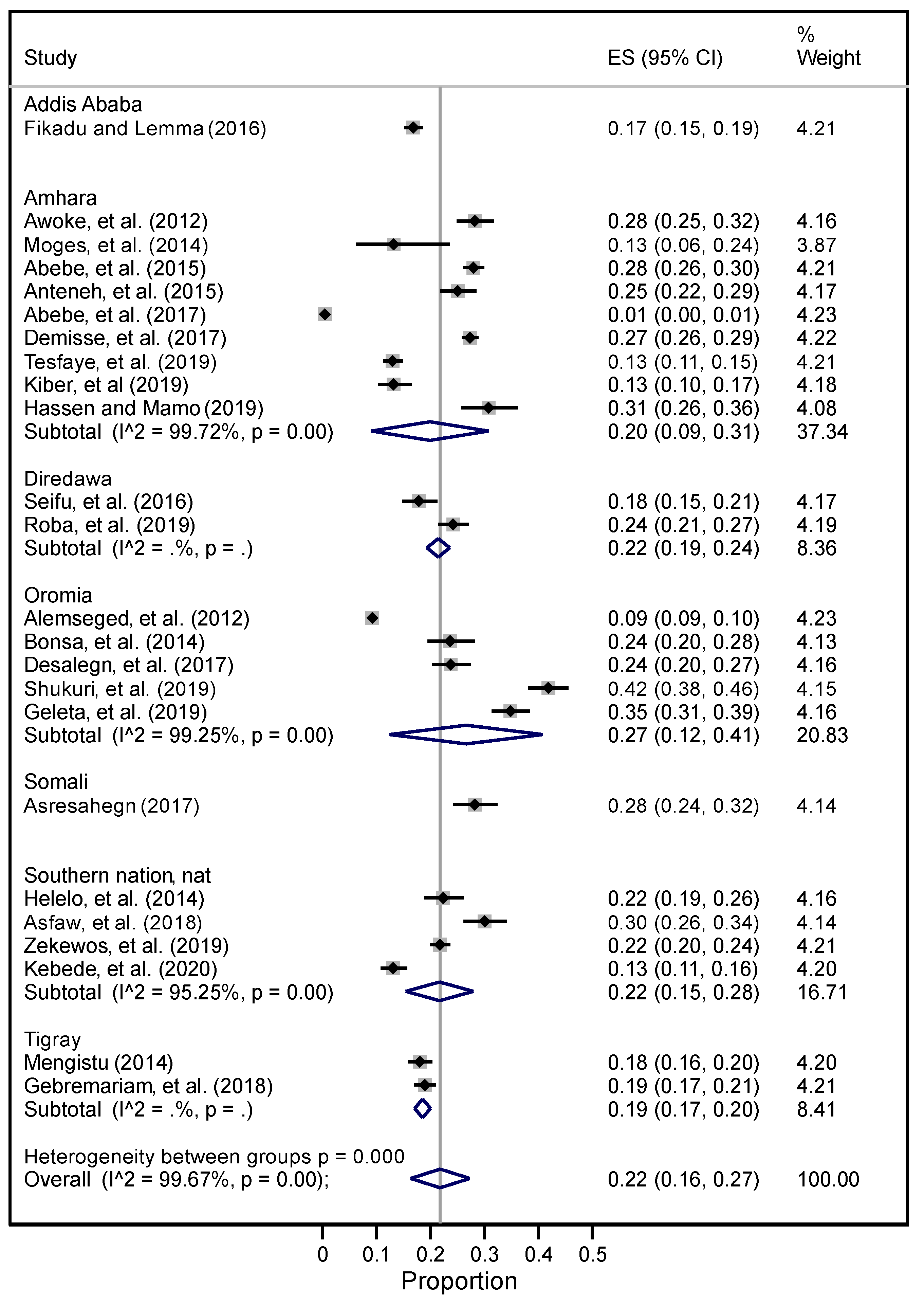
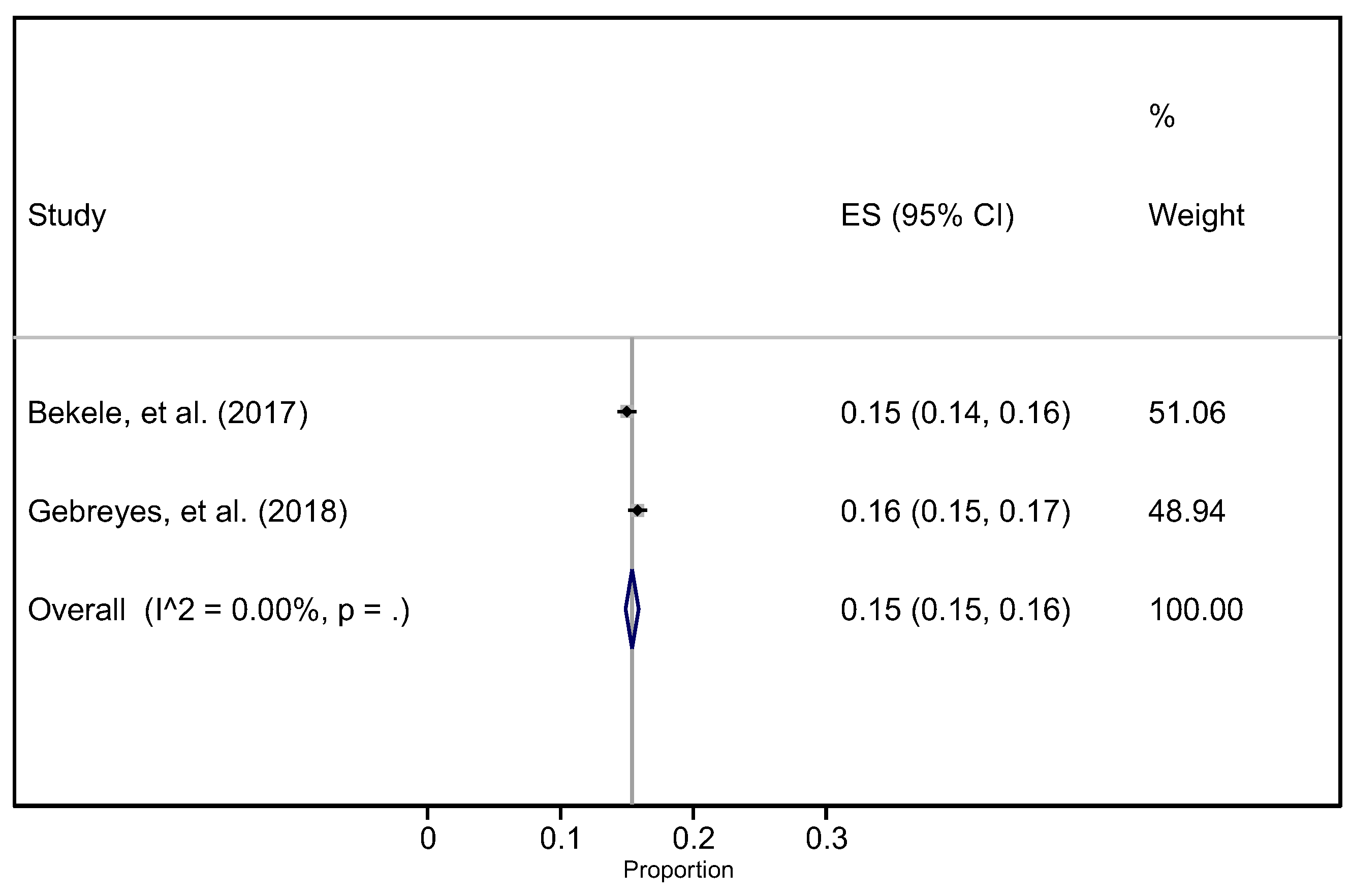
3.4. Hypertension
3.5. Overweight
3.6. Obesity
3.7. Overweight and Obesity Combined
3.8. Physical Inactivity
3.9. Smoking
3.10. Alcohol
3.11. Metabolic Syndrome and Cholestrol Level
3.12. NCD and Fruit and Vegetables
4. Discussion
4.1. Strengths and Limitations
4.2. Conclusions and Recommendation
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Ovid MEDLINE Searching Terms
References
- WHO. Noncommunicable Diseases: WHO 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 25 January 2022).
- Esmailnasab, N.; Moradi, G.; Delaveri, A. Risk factors of non-communicable diseases and metabolic syndrome. Iran. J. Public Health 2012, 41, 77. [Google Scholar] [PubMed]
- Miranda, J.J.; Barrientos-Gutierrez, T.; Corvalan, C.; Hyder, A.A.; Lazo-Porras, M.; Oni, T.; Wells, J.C. Understanding the rise of cardiometabolic diseases in low- and middle-income countries. Nat. Med. 2019, 25, 1667–1679. [Google Scholar] [CrossRef] [PubMed]
- Sliwa, K.; Acquah, L.; Gersh, B.J.; Mocumbi, A.O. Impact of Socioeconomic Status, Ethnicity, and Urbanization on Risk Factor Profiles of Cardiovascular Disease in Africa. Circulation 2016, 133, 1199–1208. [Google Scholar] [CrossRef] [PubMed]
- Khorrami, Z.; Etemad, K.; Yarahmadi, S.; Khodakarim, S.; Kameli, M.; Hezaveh, A.M.; Rahimi, E. Urbanization and noncommunicable disease (NCD) risk factors: WHO STEPwise Iranian NCD risk factors surveillance in 2011. East. Mediterr. Health J. 2017, 23, 469–479. [Google Scholar] [CrossRef]
- Schram, A.; Labonté, R.; Sanders, D. Urbanization and International Trade and Investment Policies as Determinants of Noncommunicable Diseases in Sub-Saharan Africa. Prog. Cardiovasc. Dis. 2013, 56, 281–301. [Google Scholar] [CrossRef] [PubMed]
- Rehm, J.; Hasan, O.S.; Imtiaz, S.; Probst, C.; Roerecke, M.; Shield, K. Alcohol and noncommunicable disease risk. Curr. Addict. Rep. 2018, 5, 72–85. [Google Scholar] [CrossRef]
- Ng, N.; Van Minh, H.; Tesfaye, F.; Bonita, R.; Byass, P.; Stenlund, H.; Weinehall, L.; Wall, S. Combining risk factors and demographic surveillance: Potentials of WHO STEPS and INDEPTH methodologies for assessing epidemiological transition. Scand. J. Public Health 2006, 34, 199–208. [Google Scholar] [CrossRef]
- Joffres, M.R.; Campbell, N.R.; Manns, B.; Tu, K. Estimate of the benefits of a population-based reduction in dietary sodium additives on hypertension and its related health care costs in Canada. Can. J. Cardiol. 2007, 23, 437–443. [Google Scholar] [CrossRef]
- Van Vliet, B.N.; Campbell, N.R.; Canadian Hypertension Education Program. Efforts to reduce sodium intake in Canada: Why, what, and when? Can. J. Cardiol. 2011, 27, 437–445. [Google Scholar] [CrossRef]
- Niebylski, M.L.; Redburn, K.A.; Duhaney, T.; Campbell, N.R.J.N. Healthy food subsidies and unhealthy food taxation: A systematic review of the evidence. Nutrition 2015, 31, 787–795. [Google Scholar] [CrossRef]
- Moodie, R.; Stuckler, D.; Monteiro, C.; Sheron, N.; Neal, B.; Thamarangsi, T.; Lincoln, P.; Casswell, S. Profits and pandemics: Prevention of harmful effects of tobacco, alcohol, and ultra-processed food and drink industries. Lancet 2013, 381, 670–679. [Google Scholar] [CrossRef]
- Allender, S.; Lacey, B.; Webster, P.; Rayner, M.; Deepa, M.; Scarborough, P.; Arambepola, C.; Datta, M.; Mohan, V. Level of urbanization and noncommunicable disease risk factors in Tamil Nadu, India. Bull. World Health Organ. 2010, 88, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Allender, S.; Wickramasinghe, K.; Goldacre, M.; Matthews, D.; Katulanda, P. Quantifying urbanization as a risk factor for noncommunicable disease. J. Urban Health 2011, 88, 906. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.; Williams, J.; Townsend, N.; Mikkelsen, B.; Roberts, N.; Foster, C.; Wickramasinghe, K. Socioeconomic status and non-communicable disease behavioural risk factors in low-income and lower-middle-income countries: A systematic review. Lancet Global Health 2017, 5, e277–e289. [Google Scholar] [CrossRef]
- Bigna, J.J.; Noubiap, J.J. The rising burden of non-communicable diseases in sub-Saharan Africa. Lancet Glob. Health 2019, 7, e1295–e1296. [Google Scholar] [CrossRef]
- Nyirenda, M.J. Non-communicable diseases in sub-Saharan Africa: Understanding the drivers of the epidemic to inform intervention strategies. Int. Health 2016, 8, 157–158. [Google Scholar] [CrossRef]
- Bloomfield, G.S.; Kimaiyo, S.; Carter, E.J.; Binanay, C.; Corey, G.R.; Einterz, R.M.; Tierney, W.M.; Velazquez, E.J. Chronic noncommunicable cardiovascular and pulmonary disease in sub-Saharan Africa: An academic model for countering the epidemic. Am. Heart J. 2011, 161, 842–847. [Google Scholar] [CrossRef][Green Version]
- Choukem, S.-P.; Tochie, J.N.; Sibetcheu, A.T.; Nansseu, J.R.; Hamilton-Shield, J.P. Overweight/obesity and associated cardiovascular risk factors in sub-Saharan African children and adolescents: A scoping review. Int. J. Pediatric Endocrinol. 2020, 2020, 6. [Google Scholar] [CrossRef]
- Faijer-Westerink, H.J.; Kengne, A.P.; Meeks, K.A.; Agyemang, C. Prevalence of metabolic syndrome in sub-Saharan Africa: A systematic review and meta-analysis. Nutr. Metab. Cardiovasc. Dis. 2020, 30, 547–565. [Google Scholar] [CrossRef]
- Nkambule, S.J.; Moodley, I.; Kuupiel, D.; Mashamba-Thompson, T.P. Association between food insecurity and key metabolic risk factors for diet-sensitive non-communicable diseases in sub-Saharan Africa: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 5178. [Google Scholar] [CrossRef]
- Puska, P. Why is Global Surveillance Necessary? In Global Behavioral Risk Factor Surveillance; Springer: Berlin, Germany, 2003; pp. 3–7. [Google Scholar]
- Riley, L.; Guthold, R.; Cowan, M.; Savin, S.; Bhatti, L.; Armstrong, T.; Bonita, R. The World Health Organization STEPwise approach to noncommunicable disease risk-factor surveillance: Methods, challenges, and opportunities. Am. J. Public Health 2016, 106, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Gebreyes, Y.F.; Goshu, D.Y.; Geletew, T.K.; Argefa, T.G.; Zemedu, T.G.; Lemu, K.A.; Waka, F.C.; Mengesha, A.B.; Degefu, F.S.; Deghebo, A.D.; et al. Prevalence of high bloodpressure, hyperglycemia, dyslipidemia, metabolic syndrome and their determinants in Ethiopia: Evidences from the National NCDs STEPS Survey, 2015. PLoS ONE 2018, 13, e0194819. [Google Scholar] [CrossRef] [PubMed]
- Murphy, G.A.; Asiki, G.; Ekoru, K.; Nsubuga, R.N.; Nakiyingi-Miiro, J.; Young, E.H.; Seeley, J.; Sandhu, M.S.; Kamali, A. Sociodemographic distribution of non-communicable disease risk factors in rural Uganda: A cross-sectional study. Int. J. Epidemiol. 2013, 42, 1740–1753. [Google Scholar] [CrossRef] [PubMed]
- Hosseinpoor, A.R.; Bergen, N.; Kunst, A.; Harper, S.; Guthold, R.; Rekve, D.; d’Espaignet, E.T.; Naidoo, N.; Chatterji, S. Socioeconomic inequalities in risk factors for non communicable diseases in low-income and middle-income countries: Results from the World Health Survey. BMC Public Health 2012, 12, 912. [Google Scholar] [CrossRef]
- Ali, S.; Misganaw, A.; Worku, A.; Destaw, Z.; Negash, L.; Bekele, A.; Briant, P.S.; Johnson, C.O.; Alam, T.; Odell, C.; et al. The burden of cardiovascular diseases in Ethiopia from 1990 to 2017: Evidence from the Global Burden of Disease Study. Int. Health 2020, 13, 318–326. [Google Scholar] [CrossRef]
- Misganaw, A.; Mariam, D.H.; Ali, A.; Araya, T. Epidemiology of major non-communicable diseases in Ethiopia: A systematic review. J. Health Popul. Nutr. 2014, 32, 1–13. [Google Scholar]
- Bekele, A.; Gelibo, T.; Amenu, K.; Getachew, T.; Defar, A.; Teklie, H.; Taddele, T.; Taye, G.; Getnet, M.; Gonfa, G.; et al. The hidden magnitude of raised blood pressure and elevated blood glucose in Ethiopia: A call for initiating community based NCDs risk factors screening program. Ethiop. J. Health Dev. 2017, 31, 362–369. [Google Scholar]
- Ethiopian Centeral Statistical Agency. Population and Housing Census Report-Country—2007; Ethiopian Centeral Statistical Agency: Addis Ababa, Ethiopia, 2007. [Google Scholar]
- The Federal Democratic Republic of Ethiopia. The Constitution of the Federal Democratic Republic of Ethiopia; Federal Negarit Gezeta: Addis Ababa, Ethiopia, 1995. [Google Scholar]
- WHO. Preventing Noncommunicable Diseases (NCDs) by Reducing Environmental Risk Factors; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Croke, K. The origins of Ethiopia’s primary health care expansion: The politics of state building and health system strengthening. Health Policy Plan. 2020, 35, 1318–1327. [Google Scholar] [CrossRef]
- Banteyerga, H. Ethiopia’s health extension program: Improving health through community involvement. MEDICC Rev. 2011, 13, 46–49. [Google Scholar] [CrossRef]
- Østebø, M.T.; Cogburn, M.D.; Mandani, A.S. The silencing of political context in health research in Ethiopia: Why it should be a concern. Health Policy Plan. 2018, 33, 258–270. [Google Scholar] [CrossRef]
- Netsanet, W.; Gandham, N. Health Extension Program in Ethiopia; Universal Health Coverage Studies Series (UNICO) No. 2013; World Bank: Washington, DC, USA, 2013. [Google Scholar]
- Lakew, G.A.; Wassie, E.; Ademe, A.; Fenta, A.; Wube, S.; Werede, M.; Kidane, A.; Mekonnen, L.; Hiwot, T.G.; Gallagher, K. Status of surveillance and routine immunization performances in Amhara Region, Ethiopia: Findings from in-depth peer review. Pan Afr. Med. J. 2017, 27, 6. [Google Scholar] [CrossRef] [PubMed]
- Ota, M.; Toyama, Y.; Kon, M.; Yoza, T.; Beyene, B.B. Strengthening the communicable disease surveillance and response system, Amhara Region, Ethiopia, 2012–2014: Review of a technical cooperation project. Kokusai Hoken Iryo (J. Int. Health) 2017, 32, 1–8. [Google Scholar]
- Ajemu, K.F.; Desta, A.A.; Berhe, A.A.; Woldegebriel, A.G.; Bezabih, N.M.; Negash, D.; Wuneh, A.D.; Woldearegay, T.W. Magnitude, components and predictors of metabolic syndrome in Northern Ethiopia: Evidences from regional NCDs STEPS survey, 2016. PLoS ONE 2021, 16, e0253317. [Google Scholar]
- Modesti, P.A.; Reboldi, G.; Cappuccio, F.P.; Agyemang, C.; Remuzzi, G.; Rapi, S.; Perruolo, E.; Parati, G.; ESH Working Group on CV Risk in Low Resource Settings. Panethnic differences in blood pressure in Europe: A systematic review and meta-analysis. PLoS ONE 2016, 11, e0147601. [Google Scholar] [CrossRef]
- Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada, 2011. [Google Scholar]
- Margulis, A.V.; Pladevall, M.; Riera-Guardia, N.; Varas-Lorenzo, C.; Hazell, L.; Berkman, N.D.; Viswanathan, M.; Perez-Gutthann, S. Quality assessment of observational studies in a drug-safety systematic review, comparison of two tools: The Newcastle–Ottawa scale and the RTI item bank. Clin. Epidemiol. 2014, 6, 359. [Google Scholar] [CrossRef]
- Munn, Z.; Tufanaru, C.; Aromataris, E. JBI’s systematic reviews: Data extraction and synthesis. AJN Am. J. Nurs. 2014, 114, 49–54. [Google Scholar] [CrossRef]
- Moons, K.G.; de Groot, J.A.; Bouwmeester, W.; Vergouwe, Y.; Mallett, S.; Altman, D.G.; Reitsma, J.B.; Collins, G.S. Critical appraisal and data extraction for systematic reviews of prediction modelling studies: The CHARMS checklist. PLoS Med. 2014, 11, e1001744. [Google Scholar] [CrossRef]
- StataCorp Launches. Stata Statistical Software: Release 16. 2019. Available online: https://www.businesswire.com/news/home/20190709005823/en/StataCorp-Launches-Stata-Release-16 (accessed on 25 January 2022).
- Nyaga, V.N.; Arbyn, M.; Aerts, M. Metaprop: A Stata command to perform meta-analysis of binomial data. Arch. Public Health 2014, 72, 39. [Google Scholar] [CrossRef]
- Dalton, J.E.; Bolen, S.D.; Mascha, E.J. Publication bias: The elephant in the review. Anesth. Analg. 2016, 123, 812. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Abebe, S.M.; Andargie, G.; Shimeka, A.; Alemu, K.; Kebede, Y.; Wubeshet, M.; Tariku, A.; Gebeyehu, A.; Bayisa, M.; Yitayal, M.; et al. The prevalence of non-communicable diseases in northwest Ethiopia: Survey of Dabat Health and Demographic Surveillance System. BMJ Open 2017, 7, e015496. [Google Scholar] [CrossRef] [PubMed]
- Moges, B.; Amare, B.; Fantahun, B.; Kassu, A. High prevalence of overweight, obesity, and hypertension with increased risk to cardiovascular disorders among adults in northwest Ethiopia: A cross sectional study. BMC Cardiovasc. Disord. 2014, 14, 155. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dagne, S.; Gelaw, Y.A.; Abebe, Z.; Wassie, M.M. Factors associated with overweight and obesity among adults in northeast Ethiopia: A cross-sectional study. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Hailemichael, D.; Sintayehu, F.; Amare, D. Clinical assessment of cardiovascular disease associated risk factors in Jimma town, southwest Ethiopia: Community-based cross-sectional study. Ethiop. Med. J. 2017, 55, 3–10. [Google Scholar]
- Abebe, S.M.; Berhane, Y.; Worku, A.; Getachew, A. Prevalence and associated factors of hypertension: A crossectional community based study in Northwest Ethiopia. PLoS ONE 2015, 10, e0125210. [Google Scholar] [CrossRef] [PubMed]
- Abrha, S.; Shiferaw, S.; Ahmed, K.Y. Overweight and obesity and its socio-demographic correlates among urban Ethiopian women: Evidence from the 2011 EDHS. BMC Public Health 2016, 16, 636. [Google Scholar] [CrossRef]
- Anteneh, Z.A.; Yalew, W.A.; Abitew, D.B. Prevalence and correlation of hypertension among adult population in Bahir Dar city, northwest Ethiopia: A community based cross-sectional study. Int. J. Gen. Med. 2015, 8, 175–185. [Google Scholar] [CrossRef] [PubMed]
- Awoke, A.; Awoke, T.; Alemu, S.; Megabiaw, B. Prevalence and associated factors of hypertension among adults in Gondar, Northwest Ethiopia: A community based cross-sectional study. BMC Cardiovasc. Disord. 2012, 12, 113. [Google Scholar] [CrossRef]
- Darebo, T.; Mesfin, A.; Gebremedhin, S. Prevalence and factors associated with overweight and obesity among adults in Hawassa city, southern Ethiopia: A community based cross-sectional study. BMC Obesity 2019, 6, 8. [Google Scholar] [CrossRef]
- Demisse, A.G.; Greffie, E.S.; Abebe, S.M.; Bulti, A.B.; Alemu, S.; Abebe, B.; Mesfin, N. High burden of hypertension across the age groups among residents of Gondar city in Ethiopia: A population based cross sectional study. BMC Public Health 2017, 17, 647. [Google Scholar] [CrossRef]
- Geleta, G.T.; Cheme, M.C.; Roro, E.M. Physical, behavioral and sociodemographic determinants of hypertension among the adult population in Nekemte town, western Ethiopia: Community based study. BMC Res. Notes 2019, 12, 764. [Google Scholar] [CrossRef] [PubMed]
- Getachew, T.; Defar, A.; Teklie, H.; Gonfa, G.; Bekele, A.; Bekele, A.; Gelibo, T.; Amenu, K.; Tadele, T.; Taye, G.; et al. Magnitude and predictors of excessive alcohol use in Ethiopia: Findings from the 2015 national non-communicable diseases STEPS survey. Ethiop. J. Health Dev. 2017, 31, 312–319. [Google Scholar]
- Guliani, H.; Gamtessa, S.; Çule, M. Factors affecting tobacco smoking in Ethiopia: Evidence from the demographic and health surveys. BMC Public Health 2019, 19, 938. [Google Scholar] [CrossRef] [PubMed]
- Kiber, M.; Wube, M.; Temesgen, H.; Woyraw, W.; Belay, Y.A. Prevalence of hypertension and its associated factors among adults in Debre Markos Town, Northwest Ethiopia: Community based cross-sectional study. BMC Res. Notes 2019, 12, 406. [Google Scholar] [CrossRef]
- Hassen, B.; Mamo, H. Prevalence and associated anthropometric and lifestyle predictors of hypertension among adults in Kombolcha town and suburbs, Northeast Ethiopia: A community-based cross-sectional study. BMC Cardiovasc. Disord. 2019, 19, 241. [Google Scholar] [CrossRef]
- Helelo, T.P.; Gelaw, Y.A.; Adane, A.A. Prevalence and associated factors of hypertension among adults in durame town, Southern Ethiopia. PLoS ONE 2014, 9, e112790. [Google Scholar] [CrossRef]
- Lakew, Y.; Haile, D. Tobacco use and associated factors among adults in Ethiopia: Further analysis of the 2011 Ethiopian Demographic and Health Survey. BMC Public Health 2015, 15, 487. [Google Scholar] [CrossRef]
- Mengesha, M.M.; Roba, H.S.; Ayele, B.H.; Beyene, A.S. Level of physical activity among urban adults and the socio-demographic correlates: A population-based cross-sectional study using the global physical activity questionnaire. BMC Public Health 2019, 19, 1160. [Google Scholar] [CrossRef]
- Mengistu, M.D. Pattern of blood pressure distribution and prevalence of hypertension and prehypertension among adults in Northern Ethiopia: Disclosing the hidden burden. BMC Cardiovasc. Disord. 2014, 14, 33. [Google Scholar] [CrossRef]
- Petersen, A.B.; Thompson, L.M.; Dadi, G.B.; Tolcha, A.; Cataldo, J.K. Factors associated with secondhand tobacco smoke in the home: An exploratory cross-sectional study among women in Aleta Wondo, Ethiopia. BMC Public Health 2016, 16, 910. [Google Scholar] [CrossRef]
- Shukuri, A.; Tewelde, T.; Shaweno, T. Prevalence of old age hypertension and associated factors among older adults in rural Ethiopia. Integr. Blood Press. Control. 2019, 12, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Tegegn, T.A. The prevalence of alcohol drinking behavior in public universities: A case of Ethiopia. Eur. Psychiatry 2013, 28, 1. [Google Scholar] [CrossRef]
- Tesfaye, T.D.; Temesgen, W.A.; Kasa, A.S.; Yismaw, Y.S. Prevalence and associated factors of hypertension in Amhara regional state city and its’ surrounding rural districts: A community-based cross-sectional study. Afr. Health Sci. 2019, 19, 2580–2590. [Google Scholar] [CrossRef] [PubMed]
- Teferra, S.; Selamu, M.; Medhin, G.; Bhana, A.; Hanlon, C.; Fekadu, A. Harmful use of alcohol and associated factors in a predominantly rural district in south-central Ethiopia: A cross-sectional community survey. South Afr. J. Psychiatry 2014, 20, 112–113. [Google Scholar] [CrossRef]
- Kebede, B.; Ayele, G.; Haftu, D.; Gebremichael, G. The Prevalence and Associated Factors of Hypertension among Adults in Southern Ethiopia. Int. J. Chronic Dis. Print 2020, 2020, 8020129. [Google Scholar] [CrossRef] [PubMed]
- Reda, A.A.; Kotz, D.; Biadgilign, S. Adult tobacco use practice and its correlates in eastern Ethiopia: A cross-sectional study. Harm Reduct. J. 2013, 10, 1–6. [Google Scholar] [CrossRef][Green Version]
- Mekonnen, T.; Animaw, W.; Seyum, Y. Overweight/obesity among adults in North-Western Ethiopia: A community-based cross sectional study. Arch. Public Health 2018, 76, 18. [Google Scholar] [CrossRef]
- Kassahun, A.; Terefe, G.; Misrak, G.; Tefera, T.; Theodros, G.; Atkure, D.; Habtamu, T.; Geremew, G.; Girum, T.; Fassil, S.; et al. Magnitude and determinants of physical inactivity in Ethiopia: Evidence from 2015 Ethiopia National NCD Survey. Ethiop. J. Health Dev. 2017, 31, 348–354. [Google Scholar]
- Asfaw, L.S.; Ayanto, S.Y.; Gurmamo, F.L. Hypertension and its associated factors in Hosanna town, Southern Ethiopia: Community based cross-sectional study. BMC Res. Notes 2018, 11, 306. [Google Scholar] [CrossRef]
- Kerie, S.; Menberu, M.; Geneto, M. Metabolic syndrome among residents of Mizan-Aman town, South West Ethiopia, 2017: A cross sectional study. PLoS ONE 2019, 14, e0210969. [Google Scholar] [CrossRef]
- Roba, H.S.; Beyene, A.S.; Mengesha, M.M.; Ayele, B.H. Prevalence of Hypertension and Associated Factors in Dire Dawa City, Eastern Ethiopia: A Community-Based Cross-Sectional Study. Int. J. Hypertens. 2019, 2019, 9878437. [Google Scholar] [CrossRef] [PubMed]
- Terefe, G.; Kassahun, A.; Tefera, T.; Girum, T.; Misrak, G.; Theodros, G.; Atkure, D.; Habtamu, T.; Alemayehu, B.; Fassil, S.; et al. Low fruit and vegetable intake and its associated factors in Ethiopia: A community based cross sectional NCD steps survey. Ethiop. J. Health Dev. 2017, 31, 355–361. [Google Scholar]
- Asresahegn, H.; Tadesse, F.; Beyene, E. Prevalence and associated factors of hypertension among adults in Ethiopia: A community based cross-sectional study. BMC Res. Notes 2017, 10, 629. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, M. Prevalence of overweight and obesity among office-based urban civil servants in southern nations, nationalities and peoples’ region, Ethiopia. Ethiop. Med. J. 2019, 57, 133–141. [Google Scholar]
- Zekewos, A.; Egeno, T.; Loha, E. The magnitude of hypertension and its risk factors in southern Ethiopia: A community based study. PLoS ONE 2019, 14, e0221726. [Google Scholar] [CrossRef]
- Fikadu, G.; Lemma, S. Socioeconomic Status and Hypertension among Teachers and Bankers in Addis Ababa, Ethiopia. Int. J. Hypertens. 2016, 2016, 4143962. [Google Scholar] [CrossRef]
- Workalemahu, T.; Gelaye, B.; Berhane, Y.; Williams, M.A. Physical activity and metabolic syndrome among ethiopian adults. Am. J. Hypertens. 2013, 26, 535–540. [Google Scholar] [CrossRef]
- Eticha, T.; Kidane, F. The prevalence of and factors associated with current smoking among college of health sciences students, Mekelle University in Northern Ethiopia. PLoS ONE 2014, 9, e111033. [Google Scholar] [CrossRef]
- Alemseged, F.; Haileamlak, A.; Tegegn, A.; Tessema, F.; Woldemichael, K.; Asefa, M.; Mamo, Y.; Tamiru, S.; Abebe, G. Risk factors for chronic non-communicable diseases at gilgel gibe field research center, southwest ethiopia: Population based study. Ethiop. J. Health Sci. 2012, 22, 19–28. [Google Scholar]
- Seifu, N.; Engida, Y.; Nejimu, B.; Yohannes, B.; Worku, E.; Belachew, M. Population based survey of chronic non-communicable diseases in Dubti and Asayita towns of afar region, Northeastern Ethiopia. Ann. Glob. Health 2016, 82, 531. [Google Scholar] [CrossRef]
- Gebremariam, L.W.; Chiang, C.; Yatsuya, H.; Hilawe, E.H.; Kahsay, A.B.; Godefay, H.; Abraham, L.; Hirakawa, Y.; Iso, H.; Aoyama, A. Non-communicable disease risk factor profile among public employees in a regional city in northern Ethiopia. Sci. Rep. 2018, 8, 9298. [Google Scholar] [CrossRef] [PubMed]
- Bonsa, F.; Gudina, E.K.; Hajito, K.W. Prevalence of hypertension and associated factors in Bedele Town, Southwest Ethiopia. Ethiop. J. Health Sci. 2014, 24, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Bhagavathula, A.S.; Tegegn, H.G.; Achaw, A. Alcohol use and related health problems among ethiopian adults in gondar: A cross sectional study. Value Health 2017, 20, A884. [Google Scholar] [CrossRef]
- Abebe, E.; Abebe, H. Types of Cancers Diagnosed and the Preference of Families of Adult Patients with Cancer about Disclosing Diagnosis to the Patients. Ethiop. J. Health Sci. 2017, 27, 255–262. [Google Scholar] [CrossRef][Green Version]
- Sinba Etu, E.; Hiko Gemeda, D.; Aman Hussen, M. Prevalence and factors that influence smokeless tobacco use among adults in pastoralist communities of Borena Zone, Ethiopia: Mixed method study. Tob. Induc. Dis. 2017, 15, 1. [Google Scholar] [CrossRef][Green Version]
- Solomon, S.; Mulugeta, W. Disease burden and associated risk factors for metabolic syndrome among adults in Ethiopia. BMC Cardiovasc. Disord. 2019, 19, 236. [Google Scholar] [CrossRef]
- Adeloye, D.; Basquill, C.; Aderemi, A.V.; Thompson, J.Y.; Obi, F.A. An estimate of the prevalence of hypertension in Nigeria: A systematic review and meta-analysis. J. Hypertens. 2015, 33, 230–242. [Google Scholar] [CrossRef]
- Legese, N.; Tadiwos, Y. Epidemiology of Hypertension in Ethiopia: A Systematic Review. Integr. Blood Press. Control 2020, 13, 135. [Google Scholar] [CrossRef]
- Kaze, A.D.; Schutte, A.E.; Erqou, S.; Kengne, A.P.; Echouffo-Tcheugui, J.B. Prevalence of hypertension in older people in Africa: A systematic review and meta-analysis. J. Hypertens. 2017, 35, 1345–1352. [Google Scholar] [CrossRef]
- Wamba, A.A.; Takah, N.F.; Johnman, C. The impact of interventions for the primary prevention of hypertension in Sub-Saharan Africa: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0219623. [Google Scholar] [CrossRef]
- Ahirwar, R.; Mondal, P.R. Prevalence of obesity in India: A systematic review. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of all-cause mortality with overweight and obesity using standard body mass index categories: A systematic review and meta-analysis. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Stevens, G.A.; Singh, G.M.; Lu, Y.; Danaei, G.; Lin, J.K.; Finucane, M.M.; Bahalim, A.N.; McIntire, R.K.; Gutierrez, H.R.; Cowan, M. National, regional, and global trends in adult overweight and obesity prevalences. Popul. Health Metr. 2012, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Haregu, T.N.; Oti, S.; Egondi, T.; Kyobutungi, C. Measurement of overweight and obesity an urban slum setting in sub-Saharan Africa: A comparison of four anthropometric indices. BMC Obes. 2016, 3, 46. [Google Scholar] [CrossRef]
- Lartey, S.T.; Si, L.; Otahal, P.; de Graaff, B.; Boateng, G.O.; Biritwum, R.B.; Minicuci, N.; Kowal, P.; Magnussen, C.G.; Palmer, A.J. Annual transition probabilities of overweight and obesity in older adults: Evidence from World Health Organization Study on global AGEing and adult health. Soc. Sci. Med. 2020, 247, 112821. [Google Scholar] [CrossRef]
- Nansseu, J.R.; Noubiap, J.J.; Bigna, J.J. Epidemiology of Overweight and Obesity in Adults Living in Cameroon: A Systematic Review and Meta-Analysis. Obesity 2019, 27, 1682–1692. [Google Scholar] [CrossRef]
- Ofori-Asenso, R.; Agyeman, A.A.; Laar, A.; Boateng, D. Overweight and obesity epidemic in Ghana—A systematic review and meta-analysis. BMC Public Health 2016, 16, 1239. [Google Scholar] [CrossRef]
- Fontes, F.; Damasceno, A.; Jessen, N.; Prista, A.; Silva-Matos, C.; Padrão, P.; Lunet, N. Prevalence of overweight and obesity in Mozambique in 2005 and 2015. Public Health Nutr. 2019, 22, 3118–3126. [Google Scholar] [CrossRef]
- Guwatudde, D.; Kirunda, B.E.; Wesonga, R.; Mutungi, G.; Kajjura, R.; Kasule, H.; Muwonge, J.; Bahendeka, S.K. Physical activity levels among adults in Uganda: Findings from a countrywide cross-sectional survey. J. Phys. Act. Health 2016, 13, 938–945. [Google Scholar] [CrossRef]
- John, B.; Todd, J.; Mboya, I.; Mosha, M.; Urassa, M.; Mtuy, T. Physical activity and associated factors from a cross-sectional survey among adults in northern Tanzania. BMC Public Health 2017, 17, 588. [Google Scholar] [CrossRef]
- Oyeyemi, A.L.; Oyeyemi, A.Y.; Omotara, B.A.; Lawan, A.; Akinroye, K.K.; Adedoyin, R.A.; Ramírez, A. Physical activity profile of Nigeria: Implications for research, surveillance and policy. Pan Afr. Med. J. 2018, 30, 175. [Google Scholar] [CrossRef] [PubMed]
- WHO. Physical Activity; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Brathwaite, R.; Addo, J.; Smeeth, L.; Lock, K. A Systematic Review of Tobacco Smoking Prevalence and Description of Tobacco Control Strategies in Sub-Saharan African Countries; 2007 to 2014. PLoS ONE 2015, 10, e0132401. [Google Scholar] [CrossRef]
- Sreeramareddy, C.T.; Pradhan, P.M.; Sin, S. Prevalence, distribution, and social determinants of tobacco use in 30 sub-Saharan African countries. BMC Med. 2014, 12, 243. [Google Scholar] [CrossRef] [PubMed]
- WHO. Global Status Report on Alcohol and Health 2018; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Ayano, G.; Yohannis, K.; Abraha, M.; Duko, B. The epidemiology of alcohol consumption in Ethiopia: A systematic review and meta-analysis. Subst. Abus. Treat. Prev. Policy 2019, 14, 26. [Google Scholar] [CrossRef] [PubMed]
- Bourne, R.R. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar]
- Crowther, N.J.; Norris, S.A. The current waist circumference cut point used for the diagnosis of metabolic syndrome in sub-Saharan African women is not appropriate. PLoS ONE 2012, 7, e48883. [Google Scholar] [CrossRef]
- Kaduka, L.U.; Kombe, Y.; Kenya, E.; Kuria, E.; Bore, J.K.; Bukania, Z.N.; Mwangi, M. Prevalence of metabolic syndrome among an urban population in Kenya. Diabetes Care 2012, 35, 887–893. [Google Scholar] [CrossRef]
- Ofori-Asenso, R.; Agyeman, A.A.; Laar, A. Metabolic syndrome in apparently “healthy” Ghanaian adults: A systematic review and meta-analysis. Int. J. Chronic Dis. 2017, 2017, 2562374. [Google Scholar] [CrossRef]
- Steyn, N.P.; Mchiza, Z.J. Obesity and the nutrition transition in Sub-Saharan Africa. Ann. N. Y. Acad. Sci. 2014, 1311, 88–101. [Google Scholar] [CrossRef]
- Kirunda, B.E.; Fadnes, L.T.; Wamani, H.; Van den Broeck, J.; Tylleskär, T. Population-based survey of overweight and obesity and the associated factors in peri-urban and rural Eastern Uganda. BMC Public Health 2015, 15, 1168. [Google Scholar] [CrossRef]
- Cois, A.; Day, C. Obesity trends and risk factors in the South African adult population. BMC Obes. 2015, 2, 42. [Google Scholar] [CrossRef] [PubMed]
- McCambridge, J.; McAlaney, J.; Rowe, R. Adult consequences of late adolescent alcohol consumption: A systematic review of cohort studies. PLoS Med. 2011, 8, e1000413. [Google Scholar] [CrossRef] [PubMed]
- Padrão, P.; Damasceno, A.; Silva-Matos, C.; Laszczyńska, O.; Prista, A.; Gouveia, L.; Lunet, N. Alcohol consumption in Mozambique: Regular consumption, weekly pattern and binge drinking. Drug Alcohol Depend. 2011, 115, 87–93. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hedge 1: Indicators | Hedge 2: NCD Risk Factors | Hedge 3: Ethiopia |
|---|---|---|
| Prevalence* OR Proportion* OR Magnitude* OR Epidemiology* OR Pattern* OR Trend* OR Burden | Risk factors OR Hypertension OR (high blood pressure [MeSH Terms]) OR OR (hypertension [MeSH Terms]) OR hyperten* OR (hypertension [MeSH Terms]) OR Alcohol* OR (alcohol drinking [MeSH Terms]) OR Smoking* or (smoking [MeSH Terms]) or smok* or Tobacco or (tobacco [MeSH Terms]) OR Dietary* OR Food habit OR (food habit [MeSH Terms]) OR Unhealthy diet OR (eating behaviors [MeSH Terms]) OR Metabolic disorders OR Overweight OR (overweight [MeSH Terms]) or obes* OR (obesity [MeSH Terms]) OR Sedentary lifestyle* OR exercise OR (physical exercise [MeSH Terms]) OR physical activ* OR Physical activity OR Cholesterol or (cholesterol [MeSH Terms]) | Ethiopia OR Tigray OR Amhara OR Oromia OR Afar OR Somali OR Gambela OR Benshangul Gumuz OR Addis Ababa OR Diredawa |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tesfay, F.H.; Backholer, K.; Zorbas, C.; Bowe, S.J.; Alston, L.; Bennett, C.M. The Magnitude of NCD Risk Factors in Ethiopia: Meta-Analysis and Systematic Review of Evidence. Int. J. Environ. Res. Public Health 2022, 19, 5316. https://doi.org/10.3390/ijerph19095316
Tesfay FH, Backholer K, Zorbas C, Bowe SJ, Alston L, Bennett CM. The Magnitude of NCD Risk Factors in Ethiopia: Meta-Analysis and Systematic Review of Evidence. International Journal of Environmental Research and Public Health. 2022; 19(9):5316. https://doi.org/10.3390/ijerph19095316
Chicago/Turabian StyleTesfay, Fisaha Haile, Kathryn Backholer, Christina Zorbas, Steven J. Bowe, Laura Alston, and Catherine M. Bennett. 2022. "The Magnitude of NCD Risk Factors in Ethiopia: Meta-Analysis and Systematic Review of Evidence" International Journal of Environmental Research and Public Health 19, no. 9: 5316. https://doi.org/10.3390/ijerph19095316
APA StyleTesfay, F. H., Backholer, K., Zorbas, C., Bowe, S. J., Alston, L., & Bennett, C. M. (2022). The Magnitude of NCD Risk Factors in Ethiopia: Meta-Analysis and Systematic Review of Evidence. International Journal of Environmental Research and Public Health, 19(9), 5316. https://doi.org/10.3390/ijerph19095316