
The Impact of Lockdowns on Caffeine Consumption: A Systematic Review of the Evidence


 , ,
, ,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion-Exclusion Criteria
2.3. Data Extraction-Quality Assessment
3. Results
3.1. Search Results
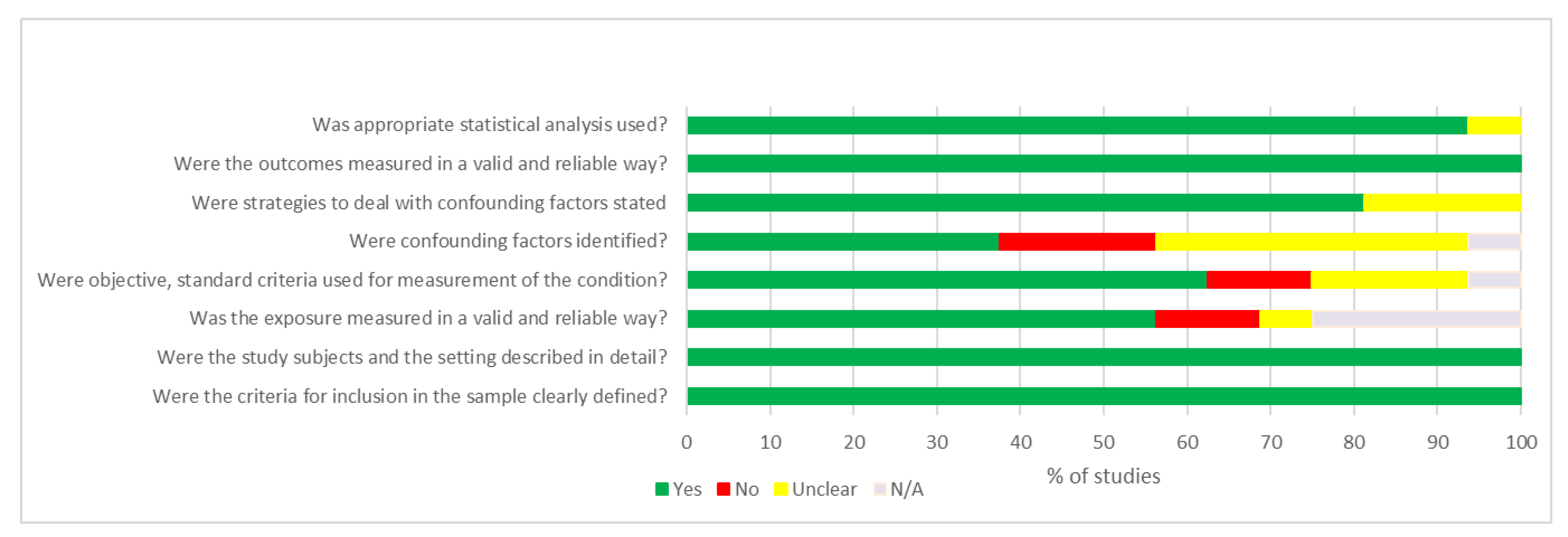
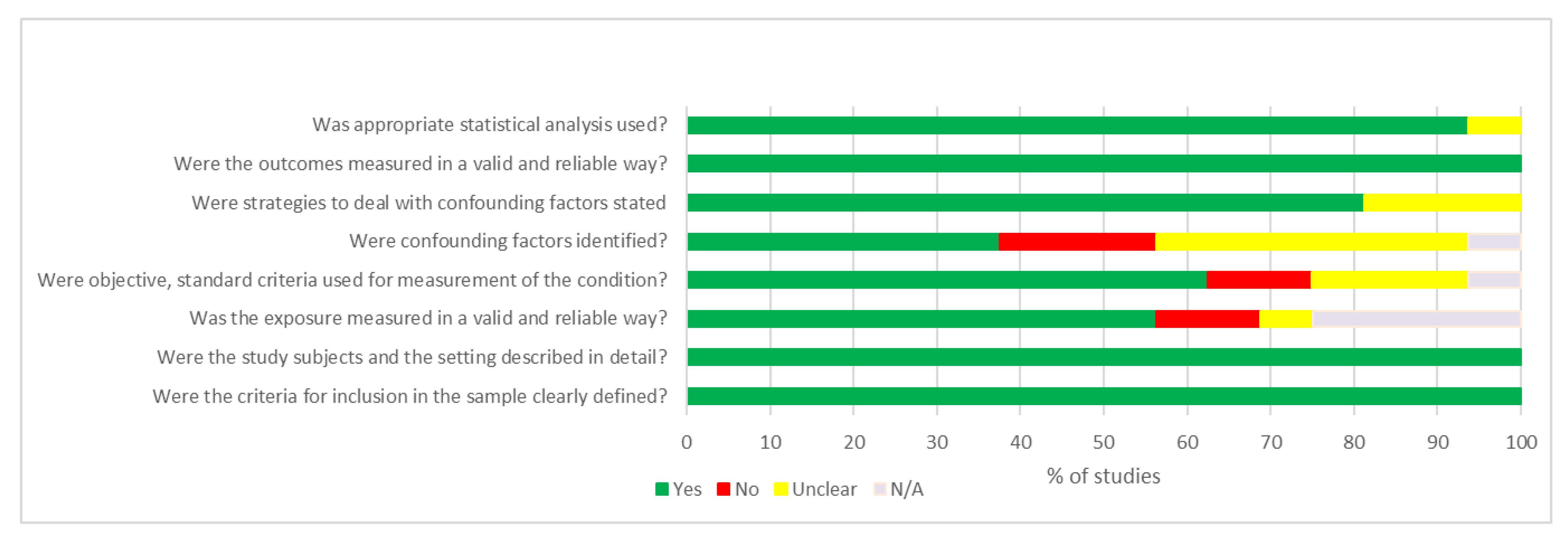
3.2. Quality Assessment
3.3. Coffee Consumption
3.4. Energy Drinks
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Baloch, S.; Baloch, M.A.; Zheng, T.; Pei, X. The Coronavirus Disease 2019 (COVID-19) Pandemic. Tohoku J. Exp. Med. 2020, 250, 271–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Worldometer. COVID-19 Coronavirus Pandemic 2020. 2020. Available online: https://www.worldometers.info/coronavirus/ (accessed on 25 December 2021).
- Gibson, P.G.; Qin, L.; Puah, S.H. COVID-19 acute respiratory distress syndrome (ARDS): Clinical features and differences from typical pre-COVID-19 ARDS. Med. J. Aust. 2020, 213, 54–56.e1. [Google Scholar] [CrossRef] [PubMed]
- Koh, D. COVID-19 lockdowns throughout the world. Occup. Med. 2020, 70, 322. [Google Scholar] [CrossRef]
- Mohamed, A.E.; Yousef, A.M. Depressive, anxiety, and post-traumatic stress symptoms affecting hospitalized and home-isolated COVID-19 patients: A comparative cross-sectional study. Middle East Curr. Psychiatry 2021, 28, 1–12. [Google Scholar] [CrossRef]
- van der Werf, E.T.; Busch, M.; Jong, M.C.; Hoenders, H.J.R. Lifestyle changes during the first wave of the COVID-19 pandemic: A cross-sectional survey in the Netherlands. BMC Public Health 2021, 21, 1226. [Google Scholar] [CrossRef]
- Enriquez-Martinez, O.G.; Martins, M.C.T.; Pereira, T.S.S.; Pacheco, S.O.S.; Pacheco, F.J.; Lopez, K.V.; Huancahuire-Vega, S.; Silva, D.A.; Mora-Urda, A.I.; Rodriguez-Vásquez, M.; et al. Diet and Lifestyle Changes During the COVID-19 Pandemic in Ibero-American Countries: Argentina, Brazil, Mexico, Peru, and Spain. Front. Nutr. 2021, 8, 671004. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Balanzá-Martínez, V.; Kapczinski, F.; Cardoso, T.D.A.; Atienza-Carbonell, B.; Rosa, A.R.; Mota, J.C.; De Boni, R.B. The assessment of lifestyle changes during the COVID-19 pandemic using a multidimensional scale. Rev. Psiquiatr. Y Salud Ment. 2021, 14, 16–26. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Jeyakumar, D.T.; Jayawardena, R.; Chourdakis, M. The impact of COVID-19 lockdown on snacking habits, fast-food and alcohol consumption: A systematic review of the evidence. Clin. Nutr. 2021; in press. [Google Scholar] [CrossRef]
- Bakaloudi, D.R.; Barazzoni, R.; Bischoff, S.C.; Breda, J.; Wickramasinghe, K.; Chourdakis, M. Impact of the first COVID-19 lockdown on body weight: A combined systematic review and a meta-analysis. Clin. Nutr. 2021; in press. [Google Scholar] [CrossRef]
- Haskell, C.F.; Kennedy, D.; Wesnes, K.; Scholey, A. Cognitive and mood improvements of caffeine in habitual consumers and habitual non-consumers of caffeine. Psychopharmacol. 2005, 179, 813–825. [Google Scholar] [CrossRef]
- Haskell-Ramsay, C.F.; Jackson, P.A.; Forster, J.S.; Dodd, F.L.; Bowerbank, S.L.; Kennedy, D.O. The Acute Effects of Caffeinated Black Coffee on Cognition and Mood in Healthy Young and Older Adults. Nutrients 2018, 10, 1386. [Google Scholar] [CrossRef] [Green Version]
- European Food Safety Authority (EFSA). Scientific opinion on the substantiation of health claims related to caffeine and increased fat oxidation leading to a reduction in body fat mass (ID 735, 1484), increased energy expenditure leading to a reduction in body weight (ID 1487), increased alertness (ID 736, 1101, 1187, 1485, 1491, 2063, 2103) and increased attention (ID 736, 1485, 1491, 2375) pursuant to article 13(1) of regulation (EC) No. 1924/2006. EFSA J. 2011, 9, 2054. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 105906. [Google Scholar] [CrossRef]
- The Joanna Briggs Institute Critical Appraisal Tools. Checklist for Analytical Cross Sectional Studies. Available online: https://jbi.global/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Analytical_Cross_Sectional_Studies2017_0.pdf (accessed on 25 March 2022).
- Al-Musharaf, S.; Aljuraiban, G.; Bogis, R.; Alnafisah, R.; Aldhwayan, M.; Tahrani, A. Lifestyle changes associated with COVID-19 quarantine among young Saudi women: A prospective study. PLoS ONE 2021, 16, e0250625. [Google Scholar] [CrossRef]
- Błaszczyk-Bębenek, E.; Jagielski, P.; Bolesławska, I.; Jagielska, A.; Nitsch-Osuch, A.; Kawalec, P. Nutrition Behaviors in Polish Adults before and during COVID-19 Lockdown. Nutrients 2020, 12, 3084. [Google Scholar] [CrossRef]
- Cirillo, M.; Rizzello, F.; Badolato, L.; De Angelis, D.; Evangelisti, P.; Coccia, M.E.; Fatini, C. The effects of COVID-19 lockdown on lifestyle and emotional state in women undergoing assisted reproductive technology: Results of an Italian survey. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 102079. [Google Scholar] [CrossRef] [PubMed]
- Coppi, F.; Nasi, M.; Farinetti, A.; Manenti, A.; Gallina, S.; Mattioli, A.V. Physical Activity, Sedentary Behaviour, and Diet in Menopausal Women: Comparison Between COVID19 “first wave” and “second wave” of pandemic in Italy. Prog. Nutr. 2021, 23, e2021194. [Google Scholar]
- Deschasaux-Tanguy, M.; Druesne-Pecollo, N.; Esseddik, Y.; de Edelenyi, F.S.; Allès, B.; Andreeva, V.A.; Baudry, J.; Charreire, H.; Deschamps, V.; Egnell, M.; et al. Diet and physical activity during the coronavirus disease 2019 (COVID-19) lockdown (March–May 2020): Results from the French NutriNet-Sante cohort study. Am. J. Clin. Nutr. 2021, 113, 924–938. [Google Scholar] [CrossRef]
- Di Santo, S.G.; Franchini, F.; Filiputti, B.; Martone, A.; Sannino, S. The Effects of COVID-19 and Quarantine Measures on the Lifestyles and Mental Health of People Over 60 at Increased Risk of Dementia. Front. Psychiatry 2020, 11, 578628. [Google Scholar] [CrossRef]
- Ogaš, Z.; Kalcina, L.L.; Dodig, I.P.; Demirović, S.; Madirazza, K.; Valić, M.; Pecotić, R. The effect of COVID-19 lockdown on lifestyle and mood in Croatian general population: A cross-sectional study. Croat. Med. J. 2020, 61, 309–318. [Google Scholar] [CrossRef]
- Górnicka, M.; Drywień, M.E.; Zielinska, M.A.; Hamułka, J. Dietary and Lifestyle Changes During COVID-19 and the Subsequent Lockdowns among Polish Adults: A Cross-Sectional Online Survey PLifeCOVID-19 Study. Nutrients 2020, 12, 2324. [Google Scholar] [CrossRef]
- Husain, W.; Ashkanani, F. Does COVID-19 change dietary habits and lifestyle behaviours in Kuwait: A community-based cross-sectional study. Environ. Health Prev. Med. 2020, 25, 61. [Google Scholar] [CrossRef]
- Jia, P.; Liu, L.; Xie, X.; Yuan, C.; Chen, H.; Guo, B.; Zhou, J.; Yang, S. Changes in dietary patterns among youths in China during COVID-19 epidemic: The COVID-19 impact on lifestyle change survey (COINLICS). Appetite 2020, 158, 105015. [Google Scholar] [CrossRef] [PubMed]
- Maffoni, S.; Brazzo, S.; De Giuseppe, R.; Biino, G.; Vietti, I.; Pallavicini, C.; Cena, H. Lifestyle Changes and Body Mass Index during COVID-19 Pandemic Lockdown: An Italian Online-Survey. Nutrients 2021, 13, 1117. [Google Scholar] [CrossRef] [PubMed]
- Palmer, K.; Bschaden, A.; Stroebele-Benschop, N. Changes in lifestyle, diet, and body weight during the first COVID 19 ‘lockdown’ in a student sample. Appetite 2021, 167, 105638. [Google Scholar] [CrossRef]
- Pertuz-Cruz, S.L.; Molina-Montes, E.; Rodríguez-Pérez, C.; Guerra-Hernández, E.J.; de Rangel, O.P.C.; Artacho, R.; Verardo, V.; Ruiz-Lopez, M.D.; García-Villanova, B. Exploring Dietary Behavior Changes Due to the COVID-19 Confinement in Colombia: A National and Regional Survey Study. Front. Nutr. 2021, 8, 644800. [Google Scholar] [CrossRef]
- Shaw, K.A.; Bertrand, L.; Deprez, D.; Ko, J.; Zello, G.A.; Chilibeck, P.D. The impact of the COVID-19 pandemic on diet, fitness, and sedentary behaviour of elite para-athletes. Disabil. Health J. 2021, 14, 101091. [Google Scholar] [CrossRef]
- Skotnicka, M.; Karwowska, K.; Kłobukowski, F.; Wasilewska, E.; Małgorzewicz, S. Dietary Habits before and during the COVID-19 Epidemic in Selected European Countries. Nutrients 2021, 13, 1690. [Google Scholar] [CrossRef]
- Yilmaz, H.Ö.; Aslan, R.; Unal, C. The Effect of the COVID-19 Outbreak on Eating Habits and Food Purchasing Behaviors of University Students. Kesmas Natl. Public Health J. 2020, 15, 154–159. [Google Scholar] [CrossRef]
- Nieber, K. The Impact of Coffee on Health. Planta Med. 2017, 83, 1256–1263. [Google Scholar] [CrossRef] [Green Version]
- Poole, R.; Kennedy, O.J.; Roderick, P.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee consumption and health: Umbrella review of meta-analyses of multiple health outcomes. BMJ 2017, 359, j5024. [Google Scholar] [CrossRef] [Green Version]
- McLellan, T.M.; Caldwell, J.A.; Lieberman, H.R. A review of caffeine’s effects on cognitive, physical and occupational performance. Neurosci. Biobehav. Rev. 2016, 71, 294–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clark, I.; Landolt, H.-P. Coffee, caffeine, and sleep: A systematic review of epidemiological studies and randomized controlled trials. Sleep Med. Rev. 2017, 31, 70–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lara, D.R. Caffeine, Mental Health, and Psychiatric Disorders. J. Alzheimer’s Dis. 2010, 20, S239–S248. [Google Scholar] [CrossRef]
- Qi, H.; Li, S. Dose-response meta-analysis on coffee, tea and caffeine consumption with risk of Parkinson’s disease. Geriatr. Gerontol. Int. 2013, 14, 430–439. [Google Scholar] [CrossRef]
- Kang, D.; Kim, Y.; Je, Y. Non-alcoholic beverage consumption and risk of depression: Epidemiological evidence from observational studies. Eur. J. Clin. Nutr. 2018, 72, 1506–1516. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, B.; Roberts, R.S.; Davis, P.; Doyle, L.; Barrington, K.; Ohlsson, A.; Solimano, A.; Tin, W. Long-Term Effects of Caffeine Therapy for Apnea of Prematurity. N. Engl. J. Med. 2007, 357, 1893–1902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Welsh, E.J.; Bara, A.; Barley, E.; Cates, C. Caffeine for asthma. Cochrane Database Syst. Rev. 2010, 2010, CD001112. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, O.J.; Roderick, P.; Buchanan, R.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Systematic review with meta-analysis: Coffee consumption and the risk of cirrhosis. Aliment. Pharmacol. Ther. 2016, 43, 562–574. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, O.J.; Roderick, P.; Buchanan, R.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee, including caffeinated and decaffeinated coffee, and the risk of hepatocellular carcinoma: A systematic review and dose-response meta-analysis. BMJ Open 2017, 7, e013739. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Thongprayoon, C.; Ungprasert, P. Coffee consumption and risk of nonalcoholic fatty liver disease. Eur. J. Gastroenterol. Hepatol. 2017, 29, e8–e12. [Google Scholar] [CrossRef]
- O’Keefe, J.H.; DiNicolantonio, J.J.; Lavie, C.J. Coffee for Cardioprotection and Longevity. Prog. Cardiovasc. Dis. 2018, 61, 38–42. [Google Scholar] [CrossRef] [Green Version]
- Andersen, L.F.; Jacobs, D.R.; Carlsen, M.H.; Blomhoff, R. Consumption of coffee is associated with reduced risk of death attributed to inflammatory and cardiovascular diseases in the Iowa Women’s Health Study. Am. J. Clin. Nutr. 2006, 83, 1039–1046. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greer, F.; Hudson, R.; Ross, R.; Graham, T. Caffeine Ingestion Decreases Glucose Disposal during a Hyperinsulinemic-Euglycemic Clamp in Sedentary Humans. Diabetes 2001, 50, 2349–2354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alperet, D.J.; Rebello, S.A.; Khoo, E.Y.-H.; Tay, Z.; Seah, S.S.-Y.; Tai, B.-C.; Tai, E.S.; Emady-Azar, S.; Chou, C.J.; Darimont, C.; et al. The effect of coffee consumption on insulin sensitivity and other biological risk factors for type 2 diabetes: A randomized placebo-controlled trial. Am. J. Clin. Nutr. 2019, 111, 448–458. [Google Scholar] [CrossRef] [PubMed]
- Al Reef, T.; Ghanem, E. Caffeine: Well-known as psychotropic substance, but little as immunomodulator. Immunobiol. 2018, 223, 818–825. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Yao, K.; Zhang, W.; Zhou, J.; Wu, T.; He, C. Coffee consumption and risk of fractures: A meta-analysis. Arch. Med. Sci. 2012, 8, 776–783. [Google Scholar] [CrossRef] [PubMed]
- Lerner, U. Bone Remodeling in Post-menopausal Osteoporosis. J. Dent. Res. 2006, 85, 584–595. [Google Scholar] [CrossRef]
- Faubion, S.S.; Sood, R.; Thielen, J.M.; Shuster, L.T. Caffeine and menopausal symptoms. Menopause 2015, 22, 155–158. [Google Scholar] [CrossRef]
- Vieira, L.; Soares, A.; Freitas, R. Caffeine as a contaminant of concern: A review on concentrations and impacts in marine coastal systems. Chemosphere 2021, 286, 131675. [Google Scholar] [CrossRef]
- EFSA. Furan in Food—EFSA Confirms Health Concerns; EFSA: Parma, Italy, 2017; Available online: https://www.efsa.europa.eu/en/press/news/furan-food-efsa-confirms-health-concerns (accessed on 21 April 2022).
- EFSA. Acrylamide; EFSA: Parma, Italy, 2015; Available online: https://www.efsa.europa.eu/en/topics/topic/acrylamide (accessed on 21 April 2022).
- EFSA Panel on Contaminants in the Food Chain (CONTAM); Schrenk, D.; Bodin, L.; Chipman, J.K.; Del Mazo, J.; GraslKraupp, B.; Hogstrand, C.; Hoogenboom, L.; Leblanc, J.-C.; Nebbia, C.S.; et al. Risk assessment of ochratoxin A in food. EFSA J. 2020, 18, e06113. [Google Scholar] [CrossRef]
- Lafranconi, A.; Micek, A.; De Paoli, P.; Bimonte, S.; Rossi, P.; Quagliariello, V.; Berretta, M. Coffee Intake Decreases Risk of Postmenopausal Breast Cancer: A Dose-Response Meta-Analysis on Prospective Cohort Studies. Nutrients 2018, 10, 112. [Google Scholar] [CrossRef] [Green Version]
- Giri, A.; Sturgeon, S.R.; Luisi, N.; Bertone-Johnson, E.; Balasubramanian, R.; Reeves, K.W. Caffeinated Coffee, Decaffeinated Coffee and Endometrial Cancer Risk: A Prospective Cohort Study among US Postmenopausal Women. Nutrients 2011, 3, 937–950. [Google Scholar] [CrossRef] [PubMed]
- Van Dam, R.M.; Hu, F.B.; Willett, W.C. Coffee, Caffeine, and Health. N. Engl. J. Med. 2020, 383, 369–378. [Google Scholar] [CrossRef]
- Grosso, G.; Godos, J.; Galvano, F.; Giovannucci, E.L. Coffee, Caffeine, and Health Outcomes: An Umbrella Review. Annu. Rev. Nutr. 2017, 37, 131–156. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.E.S.; Felimban, F.M. A Study of the Impact of Arabic Coffee Consumption on Serum Cholesterol. J. R. Soc. Health 1993, 113, 288–291. [Google Scholar] [CrossRef]
- Cai, L.; Ma, D.; Zhang, Y.; Liu, Z.; Wang, P. The effect of coffee consumption on serum lipids: A meta-analysis of randomized controlled trials. Eur. J. Clin. Nutr. 2012, 66, 872–877. [Google Scholar] [CrossRef]
- Alsunni, A.A. Energy Drink Consumption: Beneficial and Adverse Health Effects. Int. J. Health Sci. 2015, 9, 459–465. [Google Scholar] [CrossRef]
- Goldfarb, M.; Tellier, C.; Thanassoulis, G. Review of Published Cases of Adverse Cardiovascular Events after Ingestion of Energy Drinks. Am. J. Cardiol. 2014, 113, 168–172. [Google Scholar] [CrossRef]
- Scott, M.; El-Hassan, M.; Khan, A.A. Myocardial infarction in a young adult following the consumption of a caffeinated energy drink. BMJ Case Rep. 2011, 2011, bcr0220113854. [Google Scholar] [CrossRef] [Green Version]
- Pommerening, M.J.; Cardenas, J.C.; Radwan, Z.A.; Wade, C.E.; Holcomb, J.B.; Cotton, B.A. Hypercoagulability after energy drink consumption. J. Surg. Res. 2015, 199, 635–640. [Google Scholar] [CrossRef]
- Jovel, C.E.; Mejía, F.S. Caffeine and headache: Specific remarks. Neurología 2017, 32, 394–398. [Google Scholar] [CrossRef]
- Juliano, L.M.; Evatt, D.P.; Richards, B.D.; Griffiths, R.R. Characterization of individuals seeking treatment for caffeine dependence. Psychol. Addict. Behav. 2012, 26, 948–954. [Google Scholar] [CrossRef] [Green Version]
- Dikici, S.; Saritas, A.; Besir, F.H.; Tasci, A.H.; Kandis, H. Do energy drinks cause epileptic seizure and ischemic stroke? Am. J. Emerg. Med. 2013, 31, 274-e1. [Google Scholar] [CrossRef]
- Vivekanandarajah, A.; Ni, S.; Waked, A. Acute hepatitis in a woman following excessive ingestion of an energy drink: A case report. J. Med. Case Rep. 2011, 5, 227. [Google Scholar] [CrossRef] [Green Version]
- Huang, B.; Kunkel, D.; El Kabany, M. Acute Liver Failure Following One Year of Daily Consumption of a Sugar-Free Energy Drink. ACG Case Rep. J. 2014, 1, 214–216. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| First Author, Year (Country) | Individuals (F/M/O) Specific Subgroup of Included Population | Age | Time of Survey Conduction | Coffee before Lockdown | Coffee After/during Lockdown | p Value | Coffee Increased | Coffee Decreased | Coffee No Change |
|---|---|---|---|---|---|---|---|---|---|
| Al Musaraf, 2021 (Saudi Arabia) | 297 (297/0/0) | 19–30 | February 2019–May 2020 | 11.6 (17 ) * g/d 143 (199) * mL/d | 11.3 (19) * g/d 159.4 (243) * mL/d | 0.87 0.35 | |||
| Cirilo, 2021 (Italy) | 140 (140/0/0) Infertile women | 18–49 /39.4 (5) * | 20 April–4 May 2020 | 5% | 20.30% | 74.70% | |||
| Coppi, 2021 (Italy) | 320 (320/0/0) Menopausal women | 45–54 | 1st: 24 March–3 May 2020 & 2nd: 10–20 December 2020 | 1st: 28.6% 2nd: 29% | 1st: 18% 2nd: 16% | 1st: 53.4% 2nd: 55% | |||
| Deschasaux-Tanguy, 2021 (France) | 37,252 (19,483/17,769/0) General population | 52.1 (16.6) * | April–May 2020 | 13.5% | 8.40% | ||||
| Di Santo, 2020 (Italy) | 126 (102/24/0) Seniors >60 years of age with mild cognitive impairment or subjective cognitive decline | 74.29 (6.51) * | 21 April–7 May 2020 | 6.60% | 8.50% | 84.9% | |||
| Dogas, 2020 (Croatia) | 3027 (1989/506/0) | 40 (30–50) # | 25 April–5 May 2020 | 2.1 (1.0) cups/d | 2.1 (1.1) cups/d | 0.003 | |||
| Husain, 2020 (Kuwait) | 415 (285/130/0) | 18–73/38.47 12.73) * | 30 March–15 April 2020 | Americano coffee: None: 22.7% <1: 24.1% 1–2/d: 41.4% 3–4/d: 8.7% 5–6/d: 1.9% >6/d: 1.2% Arabic coffee: None: 46.3% <1: 17.3% 1–2/d: 15.4% 3–4/d: 10.6% 5–6/d: 5.8% > 6/d: 4.6% | Americano coffee: None: 31.6% <1: 25.5% 1–2/d: 33% 3–4/d: 5.5% 5–6/d: 2.9% >6/d: 1.4% Arabic coffee: None: 54.7% <1: 13.7% 1–2/d: 13.5% 3–4/d: 7. % 5–6/d: 5.5% >6/d: 4.8% | ||||
| Jia, 2021 (China) | 10,082 | 15–28/19.8 (2.3) * | 9–12 May 2020 | 2.50% | 16% | Never: 96.4% Constant: 12.65% | |||
| Maffoni, 2021 (Italy) | 1304 (973/331/0) | 30 April–10 May 2020 | 7.9% | 26.4% | 65.7% | ||||
| Palmer 2021 (Germany) | 827 (622/205) | >18 | 12 March–3 May 2020 | 31.9% | 8.4% | 59.7% | |||
| Pertuz-Cruz 2021 (Colombia) | 11,490 (4012/7478) | >18 | 6 April and 22 May 2020 | 1.57 ^ | 1.61 ^ | ||||
| Shaw 2021 (USA) | 24 (15/10) | 37.6 (9.3) * | May to mid-June 2020 | 247 (160) * mg | 234 (128) * mg | ||||
| Skotnicka. 2021 (Poland, Austria) | 1071 (604/467) | >18 | 1 October to 30 October 2020 | Poland: at least once a day: 76.9% Austria: 62.61% UK: 54.34% | Poland: at least once a day: 76.2% Austria: 62.32% UK: 49.84% | ||||
| Yilmaz 2020 (Turkey) | 866 (677/189) | 21.2 (1.4) * | 5–6 April 2020 | 30.6% | 6.7% | 62.7% |
| First Author, Year (Country) | Subjects (F/M/O) | Age | Time of Survey Conducting | Energy Drinks before Lockdown | Energy Drinks after/during Lockdown | p Value | Energy Drinks Increased | Energy Drinks Decreased | Energy Drinks No Change |
|---|---|---|---|---|---|---|---|---|---|
| Błaszczyk-Bebenek, 2020 (Poland) | 312 (200/112) | 41.12 (12.04) * | 29 April–19 May | Never: 78.5 % 1–3/month: 14.7% Once a week: 1.6% Few times a week: 4.2% Once a day: 0.3% Few times a day: 0.6% | Never: 85.3% 1–3/month: 8.3% Once a week: 3.2% Few times a week: 1.9% Once a day: 0.6% Few times a day: 0.6% | 0.015 | |||
| Górnicka, 2020 (Poland) | 1381 (2138/243) | >18 | 30 April–23 May 2020 | 1.60% | 5% | 93.40% |
| First Author, Year | Were the Criteria for Inclusion in the Sample Clearly Defined? | Were the Study Subjects and the Setting Described in Detail? | Was the Exposure Measured in a Valid and Reliable Way? | Were Objective, Standard Criteria Used for Measurement of the Condition? | Were Confounding Factors Identified? | Were Strategies to Deal with Confounding Factors Stated? | Were the Outcomes Measured in a Valid and Reliable Way? | Was Appropriate Statistical Analysis Used? |
|---|---|---|---|---|---|---|---|---|
| Al Musharaf, 2021 | ||||||||
| Blaszczyk-Bebenek, 2021 | ||||||||
| Cirilo, 2021 | ||||||||
| Coppi, 2021 | ||||||||
| Deschaseaux-Tanguy, 2021 | ||||||||
| Di Santo, 2020 | ||||||||
| Dogas, 2020 | ||||||||
| Górnica, 2020 | ||||||||
| Husain, 2020 | ||||||||
| Jia, 2020 | ||||||||
| Maffoni, 2021 | ||||||||
| Palmer, 2021 | ||||||||
| Pertuz-Cruz, 2021 | ||||||||
| Shaw, 2021 | ||||||||
| Skotnicka, 2021 | ||||||||
| Yilmaz, 2020 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bakaloudi, D.R.; Evripidou, K.; Jayawardena, R.; Breda, J.; Dardavessis, T.; Poulia, K.-A.; Chourdakis, M. The Impact of Lockdowns on Caffeine Consumption: A Systematic Review of the Evidence. Int. J. Environ. Res. Public Health 2022, 19, 5255. https://doi.org/10.3390/ijerph19095255
Bakaloudi DR, Evripidou K, Jayawardena R, Breda J, Dardavessis T, Poulia K-A, Chourdakis M. The Impact of Lockdowns on Caffeine Consumption: A Systematic Review of the Evidence. International Journal of Environmental Research and Public Health. 2022; 19(9):5255. https://doi.org/10.3390/ijerph19095255
Chicago/Turabian StyleBakaloudi, Dimitra Rafailia, Kleo Evripidou, Ranil Jayawardena, João Breda, Theodoros Dardavessis, Kalliopi-Anna Poulia, and Michail Chourdakis. 2022. "The Impact of Lockdowns on Caffeine Consumption: A Systematic Review of the Evidence" International Journal of Environmental Research and Public Health 19, no. 9: 5255. https://doi.org/10.3390/ijerph19095255
APA StyleBakaloudi, D. R., Evripidou, K., Jayawardena, R., Breda, J., Dardavessis, T., Poulia, K.-A., & Chourdakis, M. (2022). The Impact of Lockdowns on Caffeine Consumption: A Systematic Review of the Evidence. International Journal of Environmental Research and Public Health, 19(9), 5255. https://doi.org/10.3390/ijerph19095255