
Prevalence of High-Risk Disordered Eating Amongst Adolescents and Young Adults in the Middle East: A Scoping Review


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility Criteria
2.3. Exclusion Criteria
2.4. Information Sources and Literature Search
2.5. Study Selection
2.6. Data Collection Process and Data Items
The Eating Attitudes Test
2.7. Summary Measures
3. Results
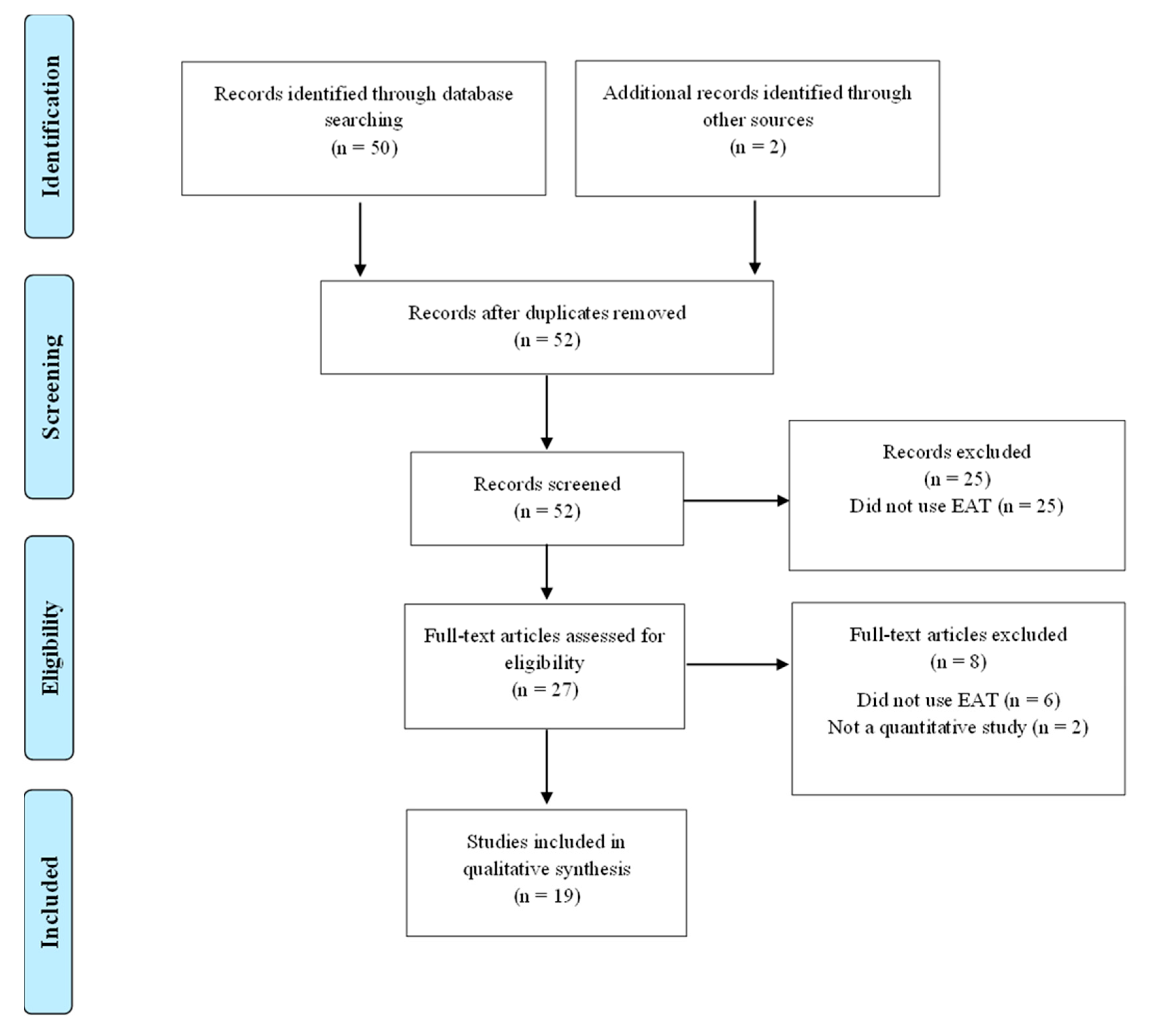
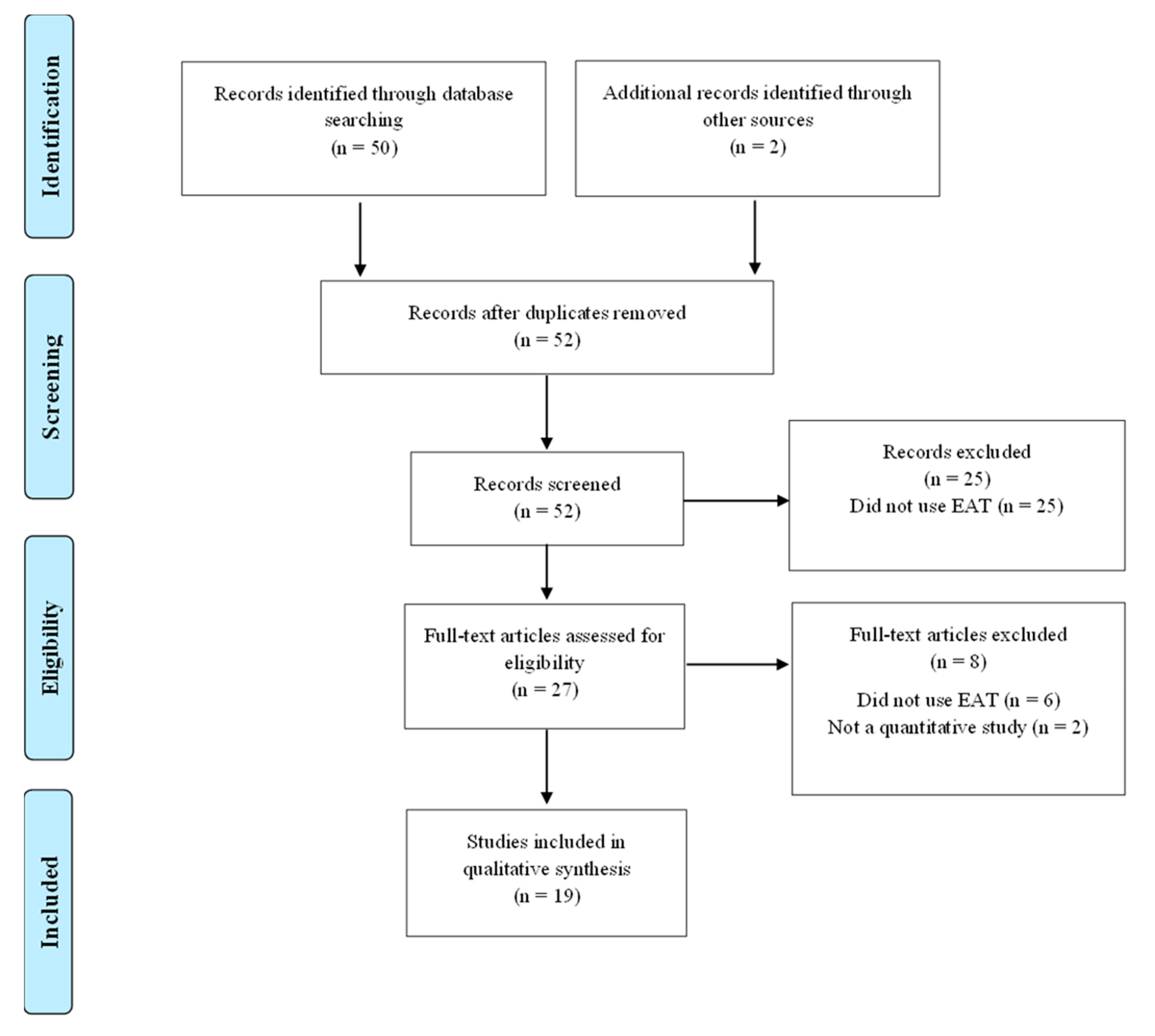
3.1. Study Selection and Characteristics
3.2. Study Characteristics
4. Discussion
4.1. Summary of Major Findings
4.2. Comparison with Prevalence Estimates from Other Countries
4.3. Strengths, Limitations, and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rikani, A.A.; Choudhry, Z.; Choudhry, A.M.; Ikram, H.; Asghar, M.W.; Kajal, D.; Waheed, A.; Mobassarah, N.J. A critique of the literature on aetiology of eating disorders. Ann. Neurosci. 2013, 20, 157–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; DSM-5; New York American Psychiatric Press Inc.: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Arcelus, J.; Mitchell, A.J.; Wales, J.; Nielsen, S. Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies. Arch. Gen. Psychiatry 2011, 68, 724–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Becker, A.E. Television, disordered eating, and young women in Fiji: Negotiating body image and identity during rapid social change. Cult. Med. Psychiatry 2004, 28, 533–559. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.H.; Richards, P.S.; Maglio, C.J. Examining the relationship between religious orientation and eating disturbances. Eat. Behav. 2004, 5, 171–180. [Google Scholar] [CrossRef]
- Dahlgren, C.V.; Stedal, K.; Wisting, L. A systematic review of eating disorder prevalence in the Nordic countries: 1994–2016. Nordic. Psychol. 2018, 70, 209–227. [Google Scholar] [CrossRef] [Green Version]
- Garner, D.M.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric Features and Clinical Correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef]
- Musaiger, A.O.; Al-Mannai, M.; Tayyem, R.; Al-Lalla, O.; Ali, E.Y.A.; Kalam, F.; Benhamed, M.M.; Saghir, S.; Halahleh, I.; Djoudi, Z.; et al. Risk of disordered eating attitudes among adolescents in seven Arab countries by gender and obesity: A cross-cultural study. Appetite 2013, 60, 162–167. [Google Scholar] [CrossRef]
- Ambwani, S.; Cardi, V.; Albano, G.; Cao, L.; Crosby, R.D.; Macdonald, P.; Schmidt, U.; Treasure, J. A multicenter audit of outpatient care for adult anorexia nervosa: Symptom trajectory, service use, and evidence in support of “early stage” versus “severe and enduring” classification. Int. J. Eat. Disord. 2020, 53, 1337–1348. [Google Scholar] [CrossRef]
- Treasure, J.; Russell, G. The case for early intervention in anorexia nervosa: Theoretical exploration of maintaining factors. Br. J. Psychiatry 2011, 199, 5–7. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Garner, D.M.; Garfinkel, P.E. The Eating Attitudes Test: An index of the symptoms of anorexia nervosa. Psychol. Med. 1979, 9, 273–279. [Google Scholar] [CrossRef] [PubMed]
- El-Bagoury, L.; Hassan, A.; AbouSeif, H. Eating attitudes and barriers to healthy eating and physical activity among a sample of university students in Egypt. J. Egypt. Public. Health Assoc. 2017, 92, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Eladawi, N.; Helal, R.; Niazy, N.A.; Abdelsalam, S. Prevalence and Associated Factors of Eating Disorders in Weight Management Centers in Tanta, Egypt. Chin. Med. J. (Engl). 2018, 131, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Gargari, B.P.; Khadem-Haghighian, M.; Taklifi, E.; Hamed-Behzad, M.; Shahraki, M. Eating attitudes, self-esteem and social physique anxiety among Iranian females who participate in fitness programs. J. Sports Med. Phys. Fitness 2010, 50, 79–84. [Google Scholar]
- Jalali-Farahani, S.; Chin, Y.S.; Mohd Nasir, M.T.; Amiri, P. Disordered eating and its association with overweight and health-related quality of life among adolescents in selected high schools of Tehran. Child. Psychiatry Hum. Dev. 2015, 46, 485–492. [Google Scholar] [CrossRef]
- Maor, N.R.; Sayag, S.; Dahan, R.; Hermoni, D. Eating attitudes among adolescents. Isr. Med. Assoc. J. 2006, 8, 627–629. [Google Scholar]
- Latzer, Y.; Azaiza, F.; Tzischinsky, O. Eating attitudes and dieting behaviour among religious subgroups of Israeli-Arab adolescent females. J. Relig. Health. 2009, 48, 189–199. [Google Scholar] [CrossRef]
- Katz, B. Gender and disordered eating of adolescents in Israel. Isr. J. Psychiatry Relat. Sci. 2014, 51, 137–144. [Google Scholar]
- Mousa, T.Y.; Al-Domi, H.A.; Mashal, R.H.; Jibril, M.A. Eating disturbances among adolescent schoolgirls in Jordan. Appetite 2010, 54, 196–201. [Google Scholar] [CrossRef]
- Al-Adawi, S.; Dorvlo, A.S.; Burke, D.T.; Moosa, S.; Al-Bahlani, S. A survey of anorexia nervosa using the Arabic version of the EAT-26 and “gold standard” interviews among Omani adolescents. Eat. Weight. Disord. 2002, 7, 304–311. [Google Scholar] [CrossRef]
- Abd El-Azeem Taha, A.A.; Abu-Zaid, H.A.; El-Sayed Desouky, D. Eating Disorders Among Female Students of Taif University, Saudi Arabia. Arch. Iran. Med. 2018, 21, 111–117. [Google Scholar] [PubMed]
- Elal, G.; Sabol, E.; Slade, P. Abnormal eating attitudes and sexual abuse experiences in Turkish university women. Eat. Weight Disord. 2004, 9, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Pinar, R. Disordered eating behaviours among Turkish adolescents with and without Type 1 diabetes. J. Pediatr. Nurs. 2005, 20, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Sanlier, N.; Yassibas, E.; Bilici, S.; Sahin, G.; Celik, B. Does the rise in eating disorders lead to increasing risk of orthorexia nervosa? Correlations with gender, education, and body mass index. Ecol. Food. Nutr. 2016, 55, 266–278. [Google Scholar] [CrossRef]
- Tozun, M.; Unsal, A.; Ayranci, U.; Arslan, G. Prevalence of disordered eating and its impact on quality of life among a group of college students in a province of west Turkey. Salud. Publica Mex. 2010, 52, 190–198. [Google Scholar] [CrossRef] [Green Version]
- Vardar, E.; Erzengin, M. The prevalence of eating disorders (EDs) and comorbid psychiatric disorders in adolescents: A two-stage community-based study. Turk. Psikiyatri. Derg. 2011, 22, 205–212. [Google Scholar]
- Sanlier, N.; Yabanci, N.; Alyakut, O. An evaluation of eating disorders among a group of Turkish university students. Appetite 2008, 51, 641–645. [Google Scholar] [CrossRef]
- Eapen, V.; Mabrouk, A.A.; Bin-Othman, S. Disordered eating attitudes and symptomatology among adolescent girls in the United Arab Emirates. Eat. Behav. 2006, 7, 53–60. [Google Scholar] [CrossRef]
- Musaiger, A.O.; Al-Mannai, M.; Al-Lalla, O. Risk of disordered eating attitudes among male adolescents in five Emirates of the United Arab Emirates. Int. J. Eat. Disord. 2014, 47, 898–900. [Google Scholar] [CrossRef]
- Udo, T.; Grilo, C.M. Prevalence and Correlates of DSM-5-Defined Eating Disorders in a Nationally Representative Sample of U.S. Adults. Biol. Psychiatry 2018, 84, 345–354. [Google Scholar] [CrossRef]
- Smink, F.R.; van Hoeken, D.; Hoek, H.W. Epidemiology of eating disorders: Incidence, prevalence, and mortality rates. Curr. Psychiatry Rep. 2012, 14, 406–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoek, H.W.; van Hoeken, D. Review of the prevalence and incidence of eating disorders. Int. J. Eat. Disord. 2003, 34, 383–396. [Google Scholar] [CrossRef]
- Hudson, J.I.; Hiripi, E.; Pope, H.G., Jr.; Kessler, R.C. The prevalence and correlates of eating disorders in the National Comorbidity Survey Replication. Biol. Psychiatry 2007, 61, 348–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preti, A.; Girolamo, G.D.; Vilagut, G.; Alonso, J.; Graaf, R.D.; Bruffaerts, R.; Demyttenaere, K.; Pinto-Meza, A.; Haro, J.M.; Morosini, P.; et al. The epidemiology of eating disorders in six European countries: Results of the ESEMeD-WMH project. J. Psychiatry Res. 2009, 43, 1125–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swanson, S.A.; Crow, S.J.; Le Grange, D.; Swendsen, J.; Merikangas, K.R. Prevalence and correlates of eating disorders in adolescents. Results from the national comorbidity survey replication adolescent supplement. Arch. Gen. Psychiatry 2011, 68, 714–723. [Google Scholar] [CrossRef] [Green Version]
- Al-Subaie, A.; Al-Shammari, S.; Bamgboye, E.; Al-Sabhan, K.; Al-Shehri, S.; Bannah, A.R. Validity of the Arabic version of the Eating Attitude Test. Int. J. Eat. Disord. 1996, 20, 321–324. [Google Scholar] [CrossRef]
- Koslowsky, M.; Scheinberg, Z.; Bleich, A.; Mark, M.; Apter, A.; Danon, Y.; Solomon, Z. The factor structure and criterion validity of the short form of the Eating Attitudes Test. J. Pers. Assess. 1992, 58, 27–35. [Google Scholar] [CrossRef]
- Savasir, I.; Erol, N. Yeme tutum testi: Anoreksiya nervosa belirtileri indeksi. (Eating Attitudes Test: An index of symptoms of anorexia nervosa). Psikoloji. Dergisi. 1989, 7, 19–25. [Google Scholar]
- Ward, Z.J.; Rodriguez, P.; Wright, D.R.; Austin, S.B.; Long, M.W. Estimation of Eating Disorders Prevalence by Age and Associations With Mortality in a Simulated Nationally Representative US Cohort. JAMA Netw. Open. 2019, 2, e1912925. [Google Scholar] [CrossRef]
- Nishizawa, Y.; Kida, K.; Nishizawa, K.; Hashiba, S.; Saito, K.; Mita, R. Perception of self-physique and eating behavior of high school students in Japan. Psychiatry Clin. Neurosci. 2003, 57, 189–196. [Google Scholar] [CrossRef]
- Tsai, M.R.; Chang, Y.J.; Lien, P.J.; Wong, Y. Survey on eating disorders related thoughts, behaviours and dietary intake in female junior high school students in Taiwan. Asia Pac. J. Clin. Nutr. 2011, 20, 196–205. [Google Scholar] [PubMed]
- Yang, S.; Choi, Y.; Lee, H. Eating Attitude, Ego-Identity, and Self-Esteem among the Urban High School Girls. J. Korean Neuropsych. Assoc. 2001, 40, 477–486. [Google Scholar]
- Makino, M.; Tsuboi, K.; Dennerstein, L. Prevalence of eating disorders: A comparison of Western and non-Western countries. MedGenMed 2004, 6, 49. [Google Scholar] [PubMed]
- Hoek, H.W.; Bartelds, A.I.; Bosveld, J.J.; van der Graaf, Y.; Limpens, V.E.; Maiwald, M.; Spaaij, C.J. Impact of urbanization on detection rates of eating disorders. Am. J. Psychiatry 1995, 152, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- van Son, G.E.; van Hoeken, D.; Bartelds, A.I.; van Furth, E.F.; Hoek, H.W. Urbanisation and the incidence of eating disorders. Br. J. Psychiatry 2006, 189, 562–563. [Google Scholar] [CrossRef] [Green Version]
- Keel, P.K.; Klump, K.L. Are eating disorders culture-bound syndromes? Implications for conceptualizing their etiology. Psychol. Bull. 2003, 129, 747–769. [Google Scholar] [CrossRef] [PubMed]
- Musaiger, A.O.; Al-Mannai, M. Association between exposure to media and body weight concern among female university students in five Arab countries: A preliminary cross-cultural study. J. Biosoc. Sci. 2014, 46, 240–247. [Google Scholar] [CrossRef]
- Abou-Saleh, M.T.; Younis, Y.; Karim, L. Anorexia nervosa in an Arab culture. Int. J. Eat. Disord. 1998, 23, 207–212. [Google Scholar] [CrossRef]
- Afifi-Soweid, R.A.; Najem Kteily, M.B.; Shediac-Rizkallah, M.C. Preoccupation with weight and disordered eating behaviors of entering students at a university in Lebanon. Int. J. Eat. Disord. 2002, 32, 52–57. [Google Scholar] [CrossRef]
- Musaiger, A.O. Body size preferences among young women in five Arab countries: A cross-cultural study. Int. J. Adolesc. Med. Health 2014, 26, 417–421. [Google Scholar] [CrossRef]
- World Health Organization. Global Health Observatory—Prevalence of Obesity among Adults, BMI ≥ 30, Age-Standardized Estimates by WHO Region. 2016. Available online: https://apps.who.int/gho/data/view.main.REGION2480A?lang=en (accessed on 18 January 2022).
- Spivak-Lavi, Z.; Peleg, O.; Tzischinsky, O.; Stein, D.; Latzer, Y. Differences in the Factor Structure of the Eating Attitude Test-26 (EAT-26) in Different Cultures in Israel: Jews, Muslims, and Christians. Nutrients 2021, 13, 1899. [Google Scholar] [CrossRef] [PubMed]
- Sysko, R.; Glasofer, D.R.; Hildebrandt, T.; Klimek, P.; Mitchell, J.E.; Berg, K.C.; Peterson, C.B.; Wonderlich, S.A.; Walsh, B.T. The eating disorder assessment for DSM-5 (EDA-5): Development and validation of a structured interview for feeding and eating disorders. Int. J. Eat. Disord. 2015, 48, 452–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Author (Year) | Country | Setting | Sample Size (Response Rate) | Sex (%) | Age Group/Mean Age (Years) | Test Used (Language) | Prevalence of High-Risk Disordered Eating (%) | Clinical Assessment Yes/No | Eating Disorders Prevalence (%) |
|---|---|---|---|---|---|---|---|---|---|
| El-Bagoury et al. (2018) [13] | Egypt | University | 445 (NA) | 59.3%  | (17–26) 20.3±1.50 | EAT-26 (Arabic) | 73.3% T 75.8% 69.6%  | No | NA |
| Eladawi, et al. (2018) [14] | Egypt | Weight Loss Centre | 400 (88.0%) | 72.0% | (NR) 35.2 ± 11.6 | EAT-40 (NA) | 65.0% T 66.7% 61.0% | No | NA |
| Gargari, et al. (2010) [15] | Iran | Fitness Program | 250 (92.6%) | 100% | (14–51) NR | EAT-26 (Persian) | 28.4% | No | NA |
| Jalali-Farahani et al. (2015) [16] | Iran | High School | 465 (95.8%) | 48.8% | (NR) 15.6 ± 0.9 | EAT-26 (English) | 18.9% T 26.4% 11.8% | No | NA |
| (Maor et al. (2006) [17] | Israel | High School | 283 (78.0%) | 51.0% | (NR) NR | EAT-26 (Hebrew) | 13.1% T 20.8% 5.0% | No | NA |
| Latzer et al. (2009) [18] | Israel | Middle, High School | 1141 (NA) | 100% | (12–18) NR | EAT-26 (Arabic) EAT-26 (English) EAT-26 (Hebrew) | 25.0% | No | NA |
| Katz (2014) [19] | Israel | Middle, High School | 323 (99.1%) | 56.0% | (NR) 14.4 ± 1.3 | EAT-40 (Hebrew) | 6.1% T 8.2% 2.8% | No | NA |
| Mousa et al. (2010) [20] | Jordan | Primary, Middle, High Schools | 326 (75.5%) | 100% | (10–16) 12.9 ± 1.8 | EAT-26 (Arabic) | 40.5% | Yes (EHQ) | 0% AN 0.6% BN 1.8% BED |
| Al-Adawi et al. (2002) [21] | Oman | Middle, High School | 262 (NA) | 48.0% | (NR) 15.4±1.4 | EAT-26 (Arabic) | 29.0% T 53.0% 47.0% | Yes (CIDI) | 9.5% AN |
| Abd El-Azeem Taha et al. (2018) [22] | Saudi Arabia | University | 1200 (NA) | 100% | (17–33) NR | EAT-26 (Arabic) | 35.4% | No | NA |
| Elal et al. (2004) [23] | Turkey | University | 532 (NA) | 100% | (NR) 19.9±1.7 | EAT-40 (Turkish) | 9.8% | No | NA |
| Pinar (2005) [24] | Turkey | High School | 100 (64.3%) | 50.0% | (12–18) 15.5± 1.4 | EAT-40 (Turkish) | 43.0% | No | NA |
| (Şanlier et al. (2008) [25] | Turkey | University | 610 (NA) | 44.6% | (17–23) NR | EAT-40 (Turkish) | 22.8% T 25.7% 20.4% | No | NA |
| Tozun et al. (2010) [26] | Turkey | University | 679 (91.1%) | 27.5% | (17–29) 21.6 ±2.2 | EAT-40 (Turkish) | 6.8% T 9.1% 5.9% | No | NA |
| Vardar & Erzengin (2011) [27] | Turkey | High School | 2907 (100%) | 54.0% | (NR) 17.04 ± 0.8 | EAT-40 (Turkish) | 8.0% | Yes (SCID) | 0.034% AN 0.79% BN 1.0% BED |
| Sanlier et al. 2016) [28] | Turkey | University | 900 (85.7%) | 58.0% | (17–23) 20.4 ± 1.7 | EAT-40 (Turkish) | 22.8% T 25.7% 20.4% | No | NA |
| Eapen et al. (2006) [29] | UAE | Middle, High School | 495 (99.0%) | 100% | (13–18) NR | EAT-40 (Arabic) | 23.4% | Yes (KSADS) | 1.0% AN 1.0% BN |
| Musaiger et al. (2013) [8] | Jordan Kuwait Libya Palestine Syria UAE | High School | 937 (NA) 628 (NA) 630 (NA) 477 (NA) 1062(NA) 505 (NA) | 52.3% | (15–18) NR | EAT-26 (Arabic) | 31.6% T, 32.7% , 20.1% 44.7% T, 42.8% , 47.3% 26.7% T, 32.6% , 19.3% 31.7% T, 38.9% , 23.2% 22.9% T, 32.0% , 14.6% 33.5% T, 37.4% , 29.8% | No | NA |
| Musaiger et al. 2014) [30] | UAE | High School | 731 (NA) | 100% | (15–18) NR | EAT-26 (Arabic) | 41.2% | No | NA |
= Females; = Males. AN = Anorexia Nervosa; BN = Bulimia Nervosa, BED = Binge Eating Disorder; EHQ = Eating habits questionnaire; CIDI = Composite International Diagnostic Interview; EAT = Eating Attitude Test; ED = Eating Disorders; KSADS = Schedule for Affective Disorders and Schizophrenia (KSADS) DSM-IV; NA = Not Applicable; NR = Not Reported; SCID = Structured Clinical Interview for DSM-III-R; T = Total.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azzeh, M.; Peachey, G.; Loney, T. Prevalence of High-Risk Disordered Eating Amongst Adolescents and Young Adults in the Middle East: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 5234. https://doi.org/10.3390/ijerph19095234
Azzeh M, Peachey G, Loney T. Prevalence of High-Risk Disordered Eating Amongst Adolescents and Young Adults in the Middle East: A Scoping Review. International Journal of Environmental Research and Public Health. 2022; 19(9):5234. https://doi.org/10.3390/ijerph19095234
Chicago/Turabian StyleAzzeh, Mahmoud, Gemma Peachey, and Tom Loney. 2022. "Prevalence of High-Risk Disordered Eating Amongst Adolescents and Young Adults in the Middle East: A Scoping Review" International Journal of Environmental Research and Public Health 19, no. 9: 5234. https://doi.org/10.3390/ijerph19095234
APA StyleAzzeh, M., Peachey, G., & Loney, T. (2022). Prevalence of High-Risk Disordered Eating Amongst Adolescents and Young Adults in the Middle East: A Scoping Review. International Journal of Environmental Research and Public Health, 19(9), 5234. https://doi.org/10.3390/ijerph19095234