
Kidney Function in Rice Workers Exposed to Heat and Dehydration in Costa Rica

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
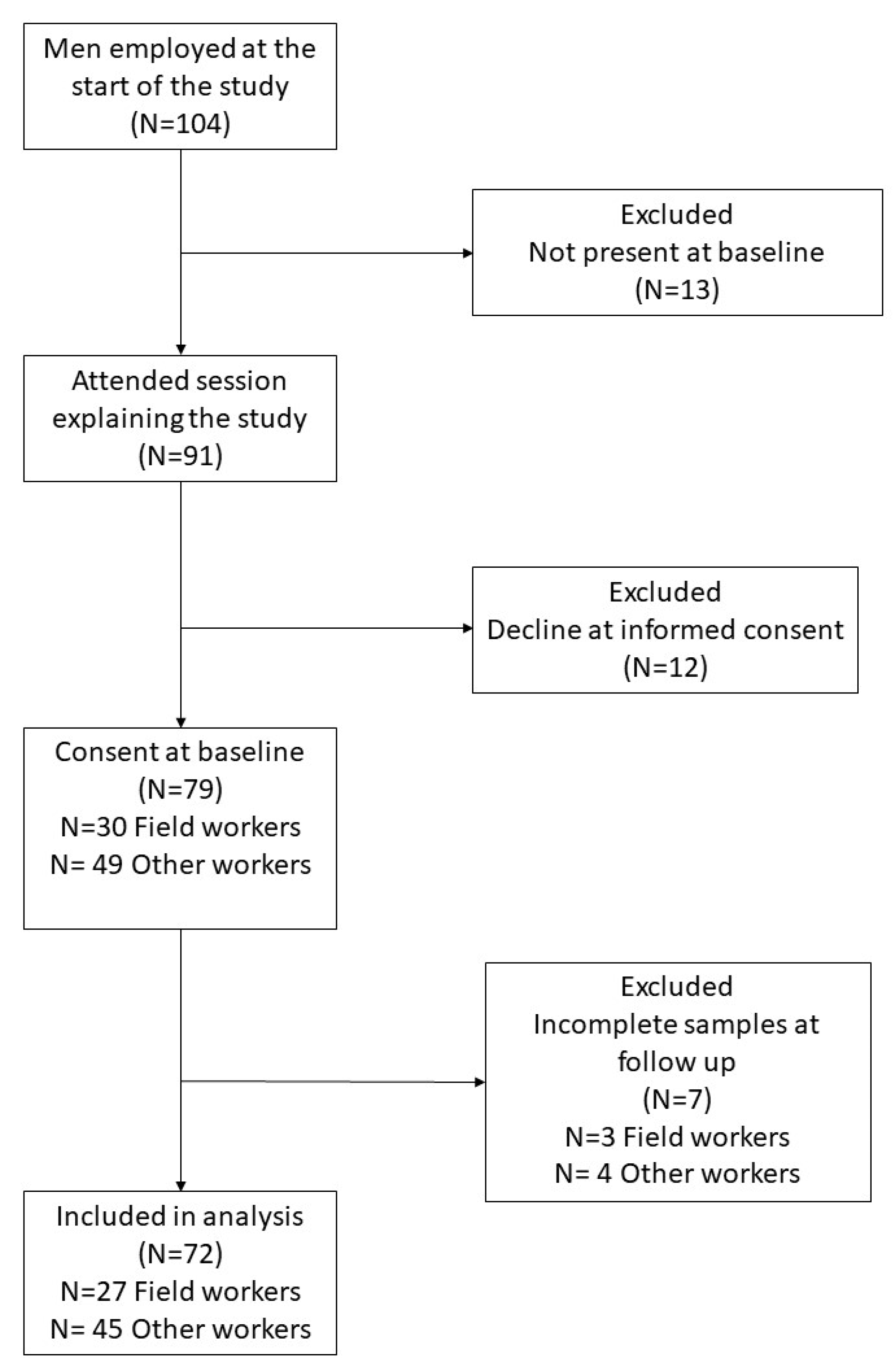
2.1. Study Design and Participant Selection
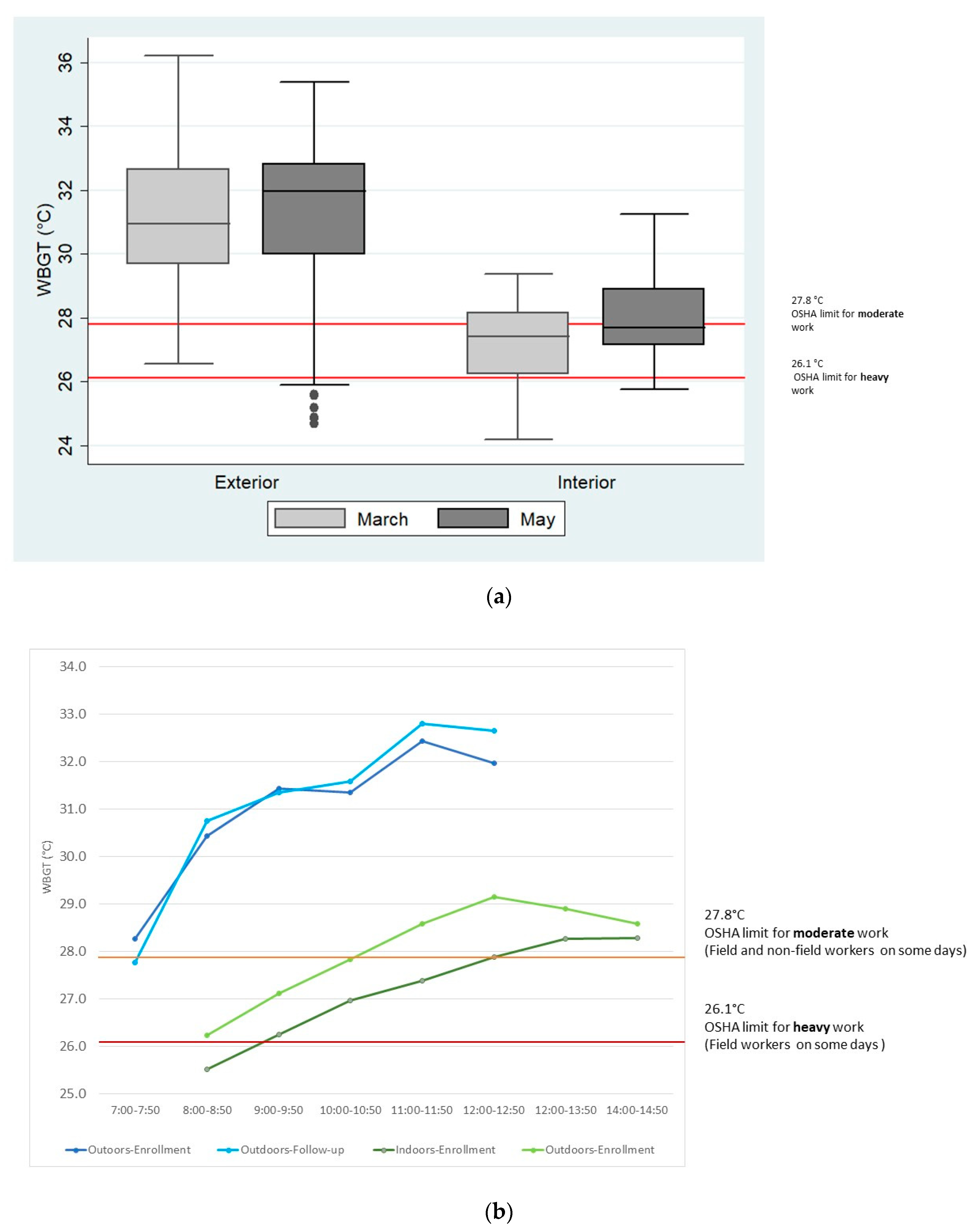
2.2. WBGT and Workload
2.3. Biomarker Analysis
2.4. Data Analysis
2.5. Study Population
3. Results
3.1. WBGT and Workload
3.2. Urinary Biomarkers
3.2.1. USG
3.2.2. Other Urinary Biomarkers
3.3. Serum Biomarkers
3.4. Kidney Function Outcomes: eGFR at Enrollment, Change in eGFR over Three Months and IKI
4. Discussion
4.1. Urinary Biomarkers
4.2. Serum Biomarkers
4.3. eGFR, AKI & IKI
4.4. Possible Risk Factors
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wegman, D.; Crowe, J.; Hogstedt, C.; Jakobsson, K.; Wesseling, C. (Eds.) Report from the Second International Research Workshop on Mesoamerican Nephropathy; SALTRA/IRET-UNA: Heredia, Costa Rica, 2016; p. 193. Available online: http://www.regionalnephropathy.org/wp-content/uploads/2016/08/MeN-2015-Scientific-Report-high-resolution_final.pdf (accessed on 13 February 2022).
- Johnson, R.J.; Wesseling, C.; Newman, L.S. Chronic kidney disease of unknown cause in agricultural communities. N. Engl. J. Med. 2019, 380, 1843–1852. [Google Scholar] [CrossRef] [PubMed]
- González-Quiroz, M.; Pearce, N.; Caplin, B.; Nitsch, D. What do epidemiological studies tell us about chronic kidney disease of undetermined cause in Meso-America? A systematic review and meta-analysis. Clin. Kidney J. 2018, 11, 496–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chapman, E.; Haby, M.M.; Illanes, E.; Sanchez-Viamonte, J.; Elias, V.; Reveiz, L. Risk factors for chronic kidney disease of non-traditional causes: A systematic review. Pan Am. J. Public Health Rev. Panam. Salud Publica 2019, 43, e35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wesseling, C.; de Joode, B.V.W.; Crowe, J.; Rittner, R.; Sanati, N.A.; Hogstedt, C.; Jakobsson, K. Mesoamerican nephropathy: Geographical distribution and time trends of chronic kidney disease mortality between 1970 and 2012 in Costa Rica. Occup. Environ. Med. 2015, 72, 714–721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong-McClure, R.; Cervantes-Loaiza, M.; Arbarca-Gómez, L.; Mcclure, R.W.; Loaiza, M.C.; Gomez, L.A. Factores Asociados a Enfermedad Renal Crónica, Región Chorotega. Informe Final de Resultados. Factors Associated wtih Chronic Kidney Disease, Chorotega Region; Final Report; Caja Costarricense de Seguro Social: San José, Costa Rica, 2014; Available online: https://repositorio.binasss.sa.cr/repositorio/bitstream/handle/20.500.11764/350/EnfermedadRenal2014.pdf?sequence=1&isAllowed=y (accessed on 14 February 2022).
- Jayasumana, C.; Orantes, C.; Herrera, R.; Almaguer, M.; Lopez, L.; Silva, L.C.; Ordunez, P.; Siribaddana, S.; Gunatilake, S.; De Broe, M.E. Chronic interstitial nephritis in agricultural communities: A worldwide epidemic with social, occupational and environmental determinants. Nephrol. Dial. Transpl. 2017, 32, 234–241. [Google Scholar] [CrossRef]
- Rajapakse, S.; Shivanthan, M.C.; Selvarajah, M. Chronic kidney disease of unknown etiology in Sri Lanka. Int. J. Occup. Environ. Health 2016, 22, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Tatapudi, R.R.; Rentala, S.; Gullipalli, P.; Komarraju, A.L.; Singh, A.K.; Tatapudi, V.S.; Goru, K.B.; Bhimarasetty, D.M.; Narni, H. High Prevalence of CKD of Unknown Etiology in Uddanam, India. Kidney Int. Rep. 2019, 4, 380–389. [Google Scholar] [CrossRef] [Green Version]
- Wesseling, C.; Glaser, J.; Rodríguez-Guzmán, J.; Weiss, I.; Lucas, R.; Peraza, S.; Da Silva, A.S.; Hansson, E.; Johnson, R.J.; Hogstedt, C.; et al. Chronic kidney disease of non-traditional origin in Mesoamerica: A disease primarily driven by occupational heat stress. Rev. Panam. Salud Pública 2020, 44, e15. [Google Scholar] [CrossRef] [Green Version]
- Glaser, J.; Hansson, E.; Weiss, I.; Wesseling, C.; Jakobsson, K.; Ekström, U.; Apelqvist, J.; Lucas, R.; Monge, E.A.; Peraza, S.; et al. Preventing kidney injury among sugarcane workers: Promising evidence from enhanced workplace interventions. Occup. Environ. Med. 2020, 77, 527–534. [Google Scholar] [CrossRef]
- Wegman, D.H.; Apelqvist, J.; Bottai, M.; Ekström, U.; García-Trabanino, R.; Glaser, J.; Hogstedt, C.; Jakobsson, K.; Jarquín, E.; Lucas, R.A.; et al. Intervention to diminish dehydration and kidney damage among sugarcane workers. Scand. J. Work Environ. Health 2018, 44, 16–24. [Google Scholar] [CrossRef]
- Bodin, T.; García-Trabanino, R.; Weiss, I.; Jarquín, E.; Glaser, J.; Jakobsson, K.; Lucas, R.A.; Wesseling, C.; Hogstedt, C.; Wegman, D.H.; et al. Intervention to reduce heat stress and improve efficiency among sugarcane workers in El Salvador: Phase 1. Occup. Environ. Med. 2016, 73, 409–416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laws, R.L.; Brooks, D.R.; Amador, J.J.; Weiner, D.E.; Kaufman, J.S.; Ramírez-Rubio, O.; Riefkohl, A.; Scammell, M.K.; López-Pilarte, D.; Sánchez, J.M.; et al. Biomarkers of Kidney Injury among Nicaraguan Sugarcane Workers. Am. J. Kidney Dis. 2016, 67, 209–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler-Dawson, J.; Krisher, L.; Asensio, C.; Cruz, A.; Tenney, L.; Weitzenkamp, D.; Dally, M.; Asturias, E.; Newman, L.S. Risk Factors for Declines in Kidney Function in Sugarcane Workers in Guatemala. J. Occup. Environ. Med. 2018, 60, 548–558. [Google Scholar] [CrossRef] [PubMed]
- García-Trabanino, R.; Jarquín, E.; Wesseling, C.; Johnson, R.J.; González-Quiroz, M.; Weiss, I.; Glaser, J.; Vindell, J.J.; Stockfelt, L.; Roncal, C.; et al. Heat stress, dehydration, and kidney function in sugarcane cutters in El Salvador—A cross-shift study of workers at risk of Mesoamerican nephropathy. Environ. Res. 2015, 142, 746–755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peraza, S.; Wesseling, C.; Aragon, A.; Leiva, R.; García-Trabanino, R.A.; Torres, C.; Jakobsson, K.; Elinder, C.G.; Hogstedt, C. Decreased kidney function among agricultural workers in El Salvador. Am. J. Kidney Dis. 2012, 59, 531–540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torres, C.; Aragón, A.; Gonzalez-Quiroz, M.; López, I.; Jakobsson, K.; Elinder, C.-G.; Lundberg, I.; Wesseling, C. Decreased Kidney Function of Unknown Cause in Nicaragua: A Community-Based Survey. Am. J. Kidney Dis. 2010, 55, 485–496. [Google Scholar] [CrossRef] [Green Version]
- Wesseling, C.; Aragón, A.; González, M.; Weiss, I.; Glaser, J.; Rivard, C.J.; Roncal-Jiménez, C.; Correa-Rotter, R.; Johnson, R.J. Heat stress, hydration and uric acid: A cross-sectional study in workers of three occupations in a hotspot of Mesoamerican nephropathy in Nicaragua. BMJ Open 2016, 6, e011034. Available online: http://www.ncbi.nlm.nih.gov/pubmed/27932336 (accessed on 13 December 2016). [CrossRef] [Green Version]
- Gallo-Ruiz, L.; Sennett, C.M.; Sánchez-Delgado, M.; García-Urbina, A.; Gámez-Altamirano, T.; Basra, K.; Laws, R.L.; Amador, J.J.; Lopez-Pilarte, D.; Tripodis, Y.; et al. Prevalence and Risk Factors for CKD Among Brickmaking Workers in La Paz Centro, Nicaragua. Am. J. Kidney Dis. 2019, 74, 239–247. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0272638619300976 (accessed on 15 May 2019). [CrossRef]
- Crowe, J.; Wesseling, C.; Solano-Román, B.; Umaña-Pinto, M.; Robles-Ramírez, A.; Kjellstrom, T.; Morales, D.; Nilsson, M. Heat exposure in sugarcane harvesters in Costa Rica. Am. J. Ind. Med. 2013, 56, 1157–1164. [Google Scholar] [CrossRef]
- Crowe, J.; Nilsson, M.; Kjellstrom, T.; Wesseling, C. Heat-related symptoms in sugarcane harvesters. Am. J. Ind. Med. 2015, 58, 541–548. [Google Scholar] [CrossRef]
- Reglamento Para la Prevención y Protección de las Personas Trabajadoras Expuestas a Estrés Térmico Por Calor [Regulation for Prevention and Protection of Working People Exposed to Heat Stress from Heat]; Ministerio de Trabajo y Seguridad Social/Ministerio de Salud: San José, Costa Rica. 2015. Available online: https://www.imprentanacional.go.cr/pub/2015/09/18/COMP_18_09_2015.pdf (accessed on 14 February 2022).
- CDC-NIOSH. Criteria for a Recommended Heat Standard: Occupational Exposure to Heat and Hot Environments; 2016-106; CDC-NIOSH US Department of Health and Human Services, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication: Cincinnati, OH, USA, 2016; p. 192. Available online: https://www.cdc.gov/niosh/docs/2016-106/ (accessed on 14 February 2022).
- OSHA. OSHA Technical Manual (OTM) Section III: Chapter 4—Heat Stress. In OSHA Technical Manual; U.S. Department of Labor Occupational Safety and Health Administration: Washington, DC, USA, 2017. Available online: https://www.osha.gov/dts/osta/otm/otm_iii/otm_iii_4.html (accessed on 15 September 2018).
- INSHT. NTP 323: Determinación del Metabolismo Energético [Determination of Energetic Metabolism]; National Institute for Safety and Hygiene in Work: Madrid, Spain, 1993. [Google Scholar]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A New Equation to Estimate Glomerular Filtration Rate. Ann. Intern. Med. 2009, 150, 604. Available online: http://annals.org/article.aspx?doi=10.7326/0003-4819-150-9-200905050-00006 (accessed on 28 April 2019). [CrossRef] [PubMed]
- Sawka, M.N.; Burke, L.M.; Eichner, E.R.; Maughan, R.J.; Montain, S.J.; Stachenfeld, N.S. Exercise and Fluid Replacement. Med. Sci. Sports Exerc. 2007, 39, 337–390. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17277604 (accessed on 23 May 2019).
- Casa, D.J.; Armstrong, L.E.; Hillman, S.K.; Montain, S.J.; Reiff, R.V.; Rich, B.S.E.; Roberts, W.O.; Stone, J.A. National Athletic Trainers’ Association position statement: Fluid replacement for athletes. J. Athl. Train. 2000, 35, 212–224. [Google Scholar] [PubMed]
- Hansson, E.; Glaser, J.; Weiss, I.; Ekström, U.; Apelqvist, J.; Hogstedt, C.; Peraza, S.; Lucas, R.; Jakobsson, K.; Wesseling, C.; et al. Workload and cross-harvest kidney injury in a Nicaraguan sugarcane worker cohort. Occup. Environ. Med. 2019, 76, 818–826. [Google Scholar] [CrossRef] [Green Version]
- Armstrong, L.E. Assessing Hydration Status: The Elusive Gold Standard. J. Am. Coll. Nutr. 2007, 26 (Suppl. 5), 575S–584S. Available online: http://www.tandfonline.com/doi/abs/10.1080/07315724.2007.10719661 (accessed on 13 February 2022).
- Binkley, H.M.; Beckett, J.; Casa, D.J.; Kleiner, D.M.; Plummer, P.E. National Athletic Trainers’ Association position statement: Exertional heat illnesses. J. Athl. Train. 2002, 37, 329–343. [Google Scholar]
- Casa, D.J. Exercise in the Heat. II. Critical Concepts in Rehydration, Exertional Heat Illnesses, and Maximizing Athletic Performance. J. Athl. Train. 1999, 34, 253–262. [Google Scholar]
- Kenefick, R.W.; Sawka, M.N. Hydration at the work site. J. Am. Coll. Nutr 2007, 26 (Suppl. 5), 597S–603S. Available online: http://www.ncbi.nlm.nih.gov/pubmed/17921472 (accessed on 8 July 2014).
- Decree Number 39147-S-TSS; Regulation for the Prevention and Protection of Worker Persons Exposed to Heat Stress [Reglamento Para la Prevención y Protección de las Personas Trabajadoras Expuestas a Estrés Térmico por Calor]. La Gaceta No 182: San José, Costa Rica. 2015, pp. 2–6. Available online: https://www.cso.go.cr/legislacion/decretos_normativa_reglamentaria/Decreto%20N%C2%B0%2039147%20S%20TSS%20Reglamento%20para%20la%20Prevencion%20Proteccion%20de%20las%20Personas%20Trabajadoras%20Expuestas%20a%20Estres%20Termico%20por%20calor.pdf (accessed on 10 December 2019).
- Wesseling, C.; Aragón, A.; González, M.; Weiss, I.; Glaser, J.; Bobadilla, N.A.; Roncal-Jiménez, C.; Correa-Rotter, R.; Johnson, R.J.; Barregard, L. Kidney function in sugarcane cutters in Nicaragua—A longitudinal study of workers at risk of Mesoamerican nephropathy. Environ. Res. 2016, 147, 125–132. [Google Scholar] [CrossRef]
- Crowe, J. Heat Exposure and Health Outcomes in Costa Rican Sugarcane Harvesters. Doctoral Thesis, Umeå Universitet, Umea, Sweden, 2014. Available online: http://umu.diva-portal.org/smash/record.jsf?pid=diva2%3A750638&dswid=1145 (accessed on 13 February 2022).
- Roncal-Jimenez, C.; García-Trabanino, R.; Barregard, L.; Lanaspa, M.A.; Wesseling, C.; Harra, T.; Aragón, A.; Grases, F.; Jarquin, E.R.; Gonzalez-Quiroz, M.; et al. Heat Stress Nephropathy from Exercise-Induced Uric Acid Crystalluria: A Perspective on Mesoamerican Nephropathy. Am. J. Kidney Dis. 2016, 67, 20–30. [Google Scholar] [CrossRef]
- Khan, S.R. Crystal-induced inflammation of the kidneys: Results from human studies, animal models, and tissue-culture studies. J. Clin. Exp. Nephrol. 2004, 8, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Mix, J.; Elon, L.; Vi Thien Mac, V.; Flocks, J.; Economos, E.; Tovar-Aguilar, A.J.; Hertzberg, V.S.; McCauley, L.A. Hydration Status, Kidney Function, and Kidney Injury in Florida Agricultural Workers. J. Occup. Environ. Med. 2018, 60, e253–e260. [Google Scholar] [CrossRef] [PubMed]
- Butler-Dawson, J.; Krisher, L.; Yoder, H.; Dally, M.; Sorensen, C.; Johnson, R.J.; Asensio, C.; Cruz, A.; Johnson, E.C.; Carlton, E.J.; et al. Evaluation of heat stress and cumulative incidence of acute kidney injury in sugarcane workers in Guatemala. Int. Arch. Occup. Environ. Health 2019, 92, 977–990. Available online: http://link.springer.com/10.1007/s00420-019-01426-3 (accessed on 14 February 2022). [CrossRef] [PubMed] [Green Version]
- Paula Santos, U.; Zanetta, D.M.T.; Terra-Filho, M.; Burdmann, E.A. Burnt sugarcane harvesting is associated with acute renal dysfunction. Kidney Int. 2015, 87, 792–799. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moyce, S.; Mitchell, D.; Armitage, T.; Tancredi, D.; Joseph, J.; Schenker, M. Heat strain, volume depletion and kidney function in California agricultural workers. Occup. Environ. Med. 2017, 74, 402–409. [Google Scholar] [CrossRef] [Green Version]
- Laws, R.L.; Brooks, D.R.; Amador, J.J.; Weiner, D.E.; Kaufman, J.S.; Ramírez-Rubio, O.; Riefkohl, A.; Scammell, M.K.; López-Pilarte, D.; Sánchez, M.J.; et al. Changes in kidney function among Nicaraguan sugarcane workers. Int. J. Occup. Environ. Health 2015, 21, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Kupferman, J.; Ramírez-Rubio, O.; Amador, J.J.; López-Pilarte, D.; Wilker, E.H.E.H.; Laws, R.L.; Sennett, C.; Robles, N.V.; Lau, J.L.; Salinas, A.J.; et al. Acute kidney injury in sugarcane workers at risk for Mesoamerican Nephropathy. Am. J. Kidney Dis. 2018, 72, 475–482. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30042041 (accessed on 8 September 2019). [CrossRef]

{kind=link}
{kind=link}
| Variables | Field Workers (n = 27) | Other Workers (n = 45) | ||
|---|---|---|---|---|
| Median (IQR) | Median (IQR) | |||
| Age (years), median (IQR) | 42 (30–54) | 40 (34–49) | ||
| Education (years), median (IQR) | 6 (2–7) | 8 (6–9) | ||
| Current job (years), median (IQR) | 9 (4–12) | 10 (3–18) | ||
| Farmworker (years), median (IQR) | 11 (8–20) | 0 | ||
| n | % | n | % | |
| Loss-to-follow-up | 3 | 11% | 4 | 9% |
| Incomplete primary education * | 11 | 41% | 4 | 9% |
| Born in Costa Rica * | 15 | 56% | 44 | 98% |
| Married/living as married | 20 | 43% | 35 | 78% |
| Past work agricultural work at another company | 15 | 56% | 29 | 64% |
| Past work in sugarcane fields (cutter/irrigation/planter) * | 9 | 33% | 2 | 4% |
| Past work as a sugarcane cutter * | 8 | 30% | 1 | 2% |
| Past work in construction | 11 | 41% | 12 | 27% |
| Consumption of alcohol | 19 | 70% | 35 | 78% |
| Current smoker | 3 | 11% | 3 | 7% |
| High blood pressure | 6 | 22% | 9 | 20% |
| Diabetes | 6 | 22% | 4 | 9% |
| Urinary tract infection during (ever) | 3 | 11% | 10 | 22% |
| Chistate (ever) * | 16 | 59% | 37 | 82% |
| Obese (BMI ≥ 30) | 7 | 26% | 13 | 29% |
| Pain medication last week at enrollment (a) | 10 | 42% | 11 | 29% |
| NSAID last week at enrollment (a) | 3 | 13% | 5 | 13% |
| Pain medication last week at followup | 6 | 22% | 9 | 20% |
| NSAID last week at followup | 1 | 4% | 3 | 7% |
| Ever pesticide use (b) | 21 | 84% | 27 | 60% |
| Ever paraquat use (b) | 18 | 72% | 25 | 56% |
| Ever glyphosate use (b) | 15 | 60% | 19 | 42% |
| Ever fungicide use (b, c) | 3 | 12% | 8 | 18% |
| Dehydrated at (USG ≥ 1.025) enrollment * | 10 | 37% | 29 | 64% |
| Dehydrated (USG ≥ 1.025) at 3-month follow-up | 12 | 44% | 20 | 44% |
| Dehydrated at enrollment and 3-month follow-up | 7 | 26% | 18 | 40% |
| Proteinuria one plus or higher enrollment * | 2 | 7% | 12 | 27% |
| Proteinuria one plus or higher 3-month follow-up * | 8 | 30% | 4 | 9% |
| Hematuria (dipstick, traces or more) enrollment | 1 | 4% | 1 | 2% |
| Hematuria (dipstick, traces or more) at 3-month follow-up | 6 | 22% | 4 | 9% |
| >3 Erythrocytes (microscopic) (enrollment) (d) | 1 | 5% | 0 | 0% |
| >3 Erythrocytes (microscopic) at 3-month follow-up | 2 | 7% | 1 | 2% |
| >5 Leucocytes (microscopic) (enrollement) (d) | 0 | 0% | 0 | 0% |
| >5 Leucocytes (microscopic) 3-month follow-up | 0 | 0% | 0 | 0% |
| Casts (any) enrollment (d, e) | 3 | 13% | 2 | 5% |
| Casts (any) 3 month follow-up (e) | 1 | 4% | 0 | 0% |
| Crystals (any) enrollment (d, f) | 4 | 18% | 8 | 17% |
| Crystals (any) 3 month follow-up (f) | 2 | 7% | 6 | 13% |
| BUN: Creatinine ratio at enrollment >20 at enrollment | 17 | 63% | 33 | 73% |
| BUN: Creatinine ratio at enrollment >20 at follow-up * | 16 | 59% | 35 | 78% |
| S-Cr >1.25 mg/dL enrollment * | 11 | 41% | 5 | 11% |
| S-Cr > 1.25 mg/dL at followup * | 11 | 41% | 8 | 18% |
| eGFR < 60 enrollment | 5 | 19% | 2 | 4% |
| eGFR < 60 at 3-month follow-up * | 7 | 26% | 3 | 7% |
| eGFR < 60 at enrollment and 3-month follow-up * | 3 | 11% | 0 | 0% |
| eGFR < 90 at enrollment | 18 | 67% | 35 | 78% |
| eGFR < 90 at 3-month follow-up | 24 | 89% | 32 | 71% |
| eGFR < 90 at enrollment and 3-month follow-up | 16 | 59% | 28 | 62% |
| IKI 3 months follow-up * | 7 | 26% | 1 | 2% |
| Variable | Field Workers (n = 27) | Other Workers (n = 45) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Min | p50 | Max | Mean | SD | Min | p50 | Max | |
| Urine specific gravity (µg/L) at enrollment * | 1.017 | 0.009 | 1.000 | 1.015 | 1.030 | 1.024 | 0.008 | 1.005 | 1.030 | 1.030 |
| Urine specific gravity (µg/L) at 3-month visit | 1.02 | 0.007 | 1.005 | 1.02 | 1.030 | 1.019 | 0.009 | 1.005 | 1.020 | 1.030 |
| Serum creatinine at enrollment (mg/dL) | 1.22 | 0.308 | 0.57 | 1.13 | 1.96 | 1.12 | 0.146 | 0.85 | 1.12 | 1.55 |
| Serum creatinine at 3-month visit (mg/dL) * | 1.35 | 0.392 | 0.89 | 1.18 | 2.37 | 1.12 | 0.139 | 0.85 | 1.13 | 1.46 |
| eGFR at enrollment (ml/min/1.73 m2) | 77.8 | 21.4 | 40.7 | 80.9 | 128.4 | 82.6 | 13.7 | 51.3 | 81.7 | 118.6 |
| eGFR at 3-month visit (ml/min/1.73 m2) * | 70.2 | 18.7 | 33.3 | 75.2 | 105.5 | 82.7 | 14.0 | 54.5 | 80.9 | 118.6 |
| Difference eGFR (3-month enrollment) | −7.6 | 23.4 | −55.7 | −9.3 | 43.4 | 0.02 | 13.5 | −25.8 | 0 | 43.6 |
| S-glucose at enrollment (mg/dL) (a) | 97.22 | 27.4 | 31.6 | 90 | 252.9 | 27.43 | 100.0 | 69.6 | 93.6 | 233.8 |
| S-glucose at at 3-month visit (mg/dL) (a) | 134.03 | 86.7 | 70.7 | 104.4 | 450.4 | 111.68 | 37.5 | 80 | 102.8 | 331.7 |
| S-urea N (BUN) at enrollment (mg/dL) | 27.63 | 9.5 | 5.5 | 25.6 | 41.5 | 27.91 | 7.0 | 14.9 | 27.3 | 45.7 |
| S-urea N (BUN) at 3-month visit (mg/dL) | 30.94 | 11.6 | 4.9 | 29.1 | 59.1 | 27.47 | 5.6 | 16.7 | 27.8 | 38.3 |
| BUN: Creatinine ratio at enrollment (mg/dL) | 23.0 | 6.7 | 5.3 | 22.8 | 37.6 | 25.1 | 6.6 | 11.5 | 24.4 | 43.9 |
| BUN: Creatinine ratio at 3-month visit (mg/dL) | 23.7 | 7.9 | 2.6 | 23.1 | 37.9 | 24.8 | 5.8 | 12.1 | 25.3 | 36.8 |
| S-uric acid at enrollment (mg/dL) | 5.84 | 1.8 | 1.33 | 6.01 | 8.81 | 5.67 | 1.1 | 3.16 | 5.45 | 8.61 |
| S-uric acid at 3-month visit (mg/dL) | 6.29 | 1.4 | 4.19 | 6.01 | 9.73 | 5.73 | 1.2 | 3.84 | 5.47 | 8.92 |
| S-albumin at enrollment (g/dL) | 4.31 | 1.0 | 1.67 | 4.42 | 5.99 | 4.48 | 0.2 | 4.05 | 4.46 | 4.92 |
| S-albumin at 3-month visit (g/dL) | 4.48 | 0.3 | 3.63 | 4.5 | 4.88 | 4.53 | 0.2 | 3.97 | 4.57 | 4.95 |
| S-CPK at enrollment (Ul/L) | 213.48 | 174.9 | 18 | 176 | 893 | 160.09 | 71.2 | 43 | 138 | 343 |
| S-CPK at 3-month visit (Ul/L) | 216.78 | 192.9 | 62 | 150 | 672 | 196.43 | 116.3 | 62 | 159.5 | 400 |
| S-Na at enrollment (mmol/L) | 141.08 | 7.8 | 104.7 | 142.8 | 149.6 | 143.50 | 4.4 | 137.6 | 142.1 | 153.5 |
| S-Na at 3-month visit (mmol/L) * | 139.05 | 4.2 | 130.85 | 139.58 | 147.93 | 143.84 | 4.0 | 134.39 | 144.39 | 149.9 |
| S-K at enrollment (mmol/L) | 3.96 | 0.5 | 2.84 | 3.9 | 5.05 | 4.11 | 0.4 | 2.96 | 4.06 | 5.01 |
| S-K at 3-month visit (mmol/L) | 4.05 | 0.4 | 3.16 | 4.1 | 4.75 | 4.37 | 0.4 | 3.15 | 4.46 | 4.95 |
| S-Cl at enrollment (mmol/L) | 98.28 | 3.1 | 92.52 | 98.5 | 106 | 99.59 | 3.8 | 91.24 | 100.17 | 107.7 |
| S-Cl at 3-month visit (mmol/L) | 97.26 | 3.9 | 88.32 | 97.66 | 102.82 | 98.51 | 2.6 | 91.74 | 98.92 | 104.61 |
| S-Ca at enrollment (mmol/L) * | 2.16 | 0.2 | 1.24 | 2.22 | 2.41 | 2.26 | 0.1 | 2.04 | 2.25 | 2.52 |
| S-Ca at 3-month visit (mmol/L) | 2.27 | 0.1 | 2.12 | 2.25 | 2.48 | 2.30 | 0.1 | 2.06 | 2.3 | 2.58 |
| S-Mg at enrollment (mmol/L) * | 0.77 | 0.1 | 0.44 | 0.79 | 0.94 | 0.92 | 0.1 | 0.61 | 0.94 | 1.12 |
| S-Mg at 3-month visit (mmol/L) | 0.81 | 0.1 | 0.51 | 0.8 | 1.07 | 0.82 | 0.1 | 0.58 | 0.81 | 1.28 |
| Y | Term | Estimate | p | Lower 95% | Upper 95% |
|---|---|---|---|---|---|
| eGFR at enrollment | Intercept | 110.69 | <0.00 | 95.61 | 125.76 |
| Age (41 ± 10) | −0.71 | <0.00 | −1.06 | −0.36 | |
| Current field worker (38%) | −2.75 | 0.15 | −6.49 | 0.99 | |
| Past work in construction (32%) | 3.75 | 0.06 | −0.14 | 7.64 |
| Term | β Estimate Difference in eGFR Month 3-Baseline | p | Lower 95% | Upper 95% |
|---|---|---|---|---|
| Intercept | −11.78 | 0.01 | −19.93 | −3.62 |
| Current field worker (38%) | −3.9 | 0.07 | −8.19 | 0.4 |
| Current smoker (8%) | −6.2 | 0.1 | −13.72 | 1.31 |
| Dehydrated at both visits (USG ≥ 1.025) (35%) | −3.19 | 0.15 | −7.58 | 1.2 |
| Pain medication at follow up (21%) (a) | −3.15 | 0.22 | −8.24 | 1.95 |
| Variables | Exp(β) (=IR Estimate, 95%CI) | p | ||
|---|---|---|---|---|
| (Intercept) | 0.14 | 0.00 | 0.28 | <0.001 |
| Diabetes | 1.83 | 0.90 | 3.60 | 0.08 |
| Current field worker * | 2.22 | 1.08 | 5.81 | 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crowe, J.; Rojas-Valverde, D.; Rojas-Garbanzo, M.; Gutiérrez-Vargas, R.; Ugalde-Ramírez, J.A.; Ledezma-Rojas, J.P.; Cabrera-Alpizar, W.; Salazar-Salazar, M.; Mauricio-La Torre, R.; Valera-Amador, L.; et al. Kidney Function in Rice Workers Exposed to Heat and Dehydration in Costa Rica. Int. J. Environ. Res. Public Health 2022, 19, 4962. https://doi.org/10.3390/ijerph19094962
Crowe J, Rojas-Valverde D, Rojas-Garbanzo M, Gutiérrez-Vargas R, Ugalde-Ramírez JA, Ledezma-Rojas JP, Cabrera-Alpizar W, Salazar-Salazar M, Mauricio-La Torre R, Valera-Amador L, et al. Kidney Function in Rice Workers Exposed to Heat and Dehydration in Costa Rica. International Journal of Environmental Research and Public Health. 2022; 19(9):4962. https://doi.org/10.3390/ijerph19094962
Chicago/Turabian StyleCrowe, Jennifer, Daniel Rojas-Valverde, Marianela Rojas-Garbanzo, Randall Gutiérrez-Vargas, José Alexis Ugalde-Ramírez, José Pablo Ledezma-Rojas, William Cabrera-Alpizar, Minor Salazar-Salazar, Rodrigo Mauricio-La Torre, Lázara Valera-Amador, and et al. 2022. "Kidney Function in Rice Workers Exposed to Heat and Dehydration in Costa Rica" International Journal of Environmental Research and Public Health 19, no. 9: 4962. https://doi.org/10.3390/ijerph19094962
APA StyleCrowe, J., Rojas-Valverde, D., Rojas-Garbanzo, M., Gutiérrez-Vargas, R., Ugalde-Ramírez, J. A., Ledezma-Rojas, J. P., Cabrera-Alpizar, W., Salazar-Salazar, M., Mauricio-La Torre, R., Valera-Amador, L., & van Wendel de Joode, B. (2022). Kidney Function in Rice Workers Exposed to Heat and Dehydration in Costa Rica. International Journal of Environmental Research and Public Health, 19(9), 4962. https://doi.org/10.3390/ijerph19094962