
Management of Transcatheter Aortic Valve Implantation and Complex Aorta Anatomy: The Importance of Pre-Procedural Planning

{kind=link}
{kind=link}
Abstract
:1. Introduction
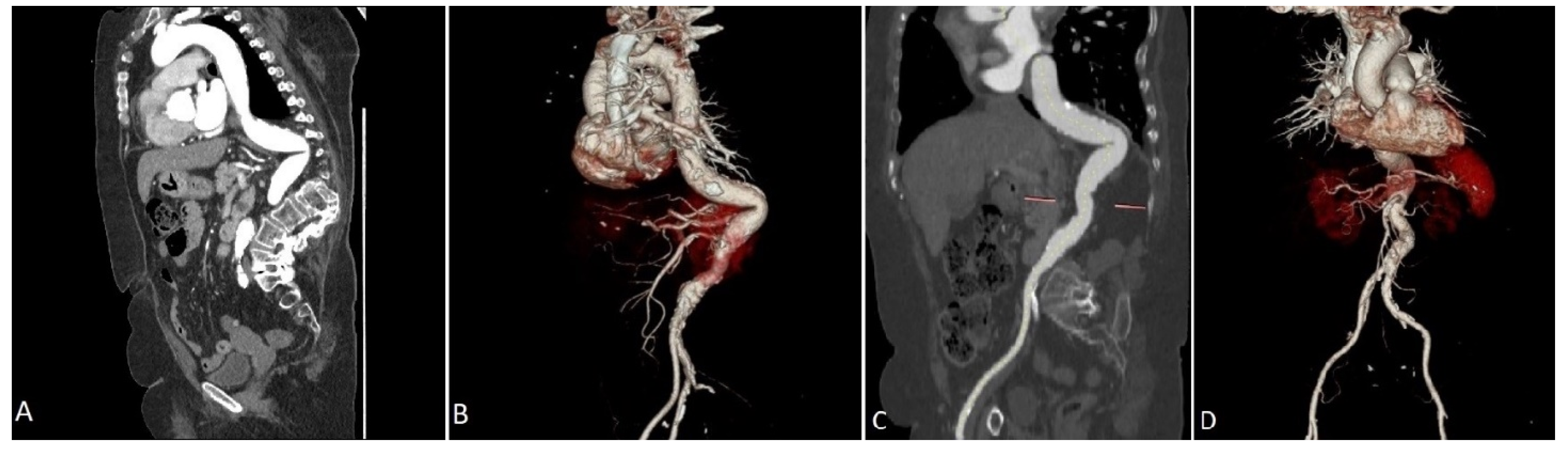
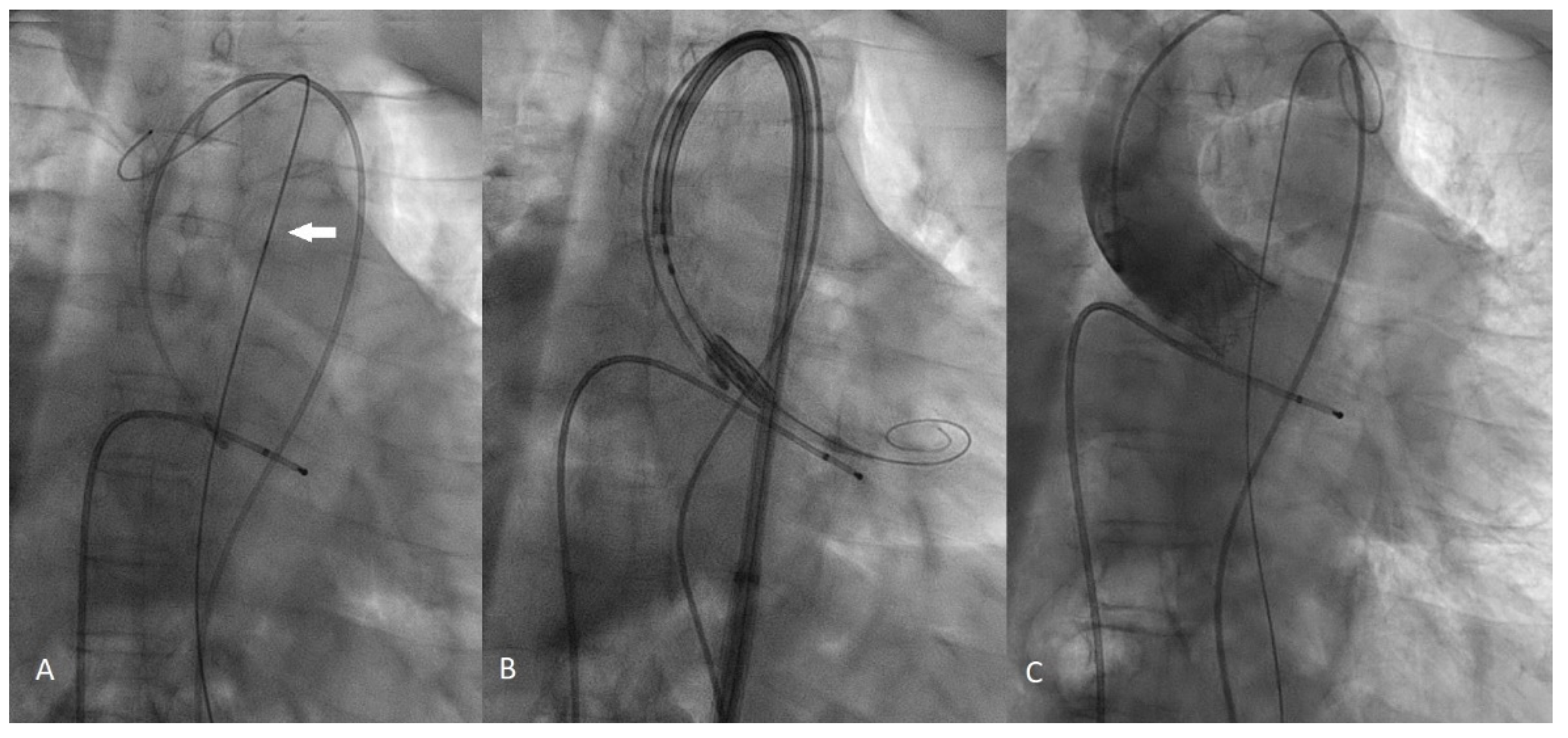
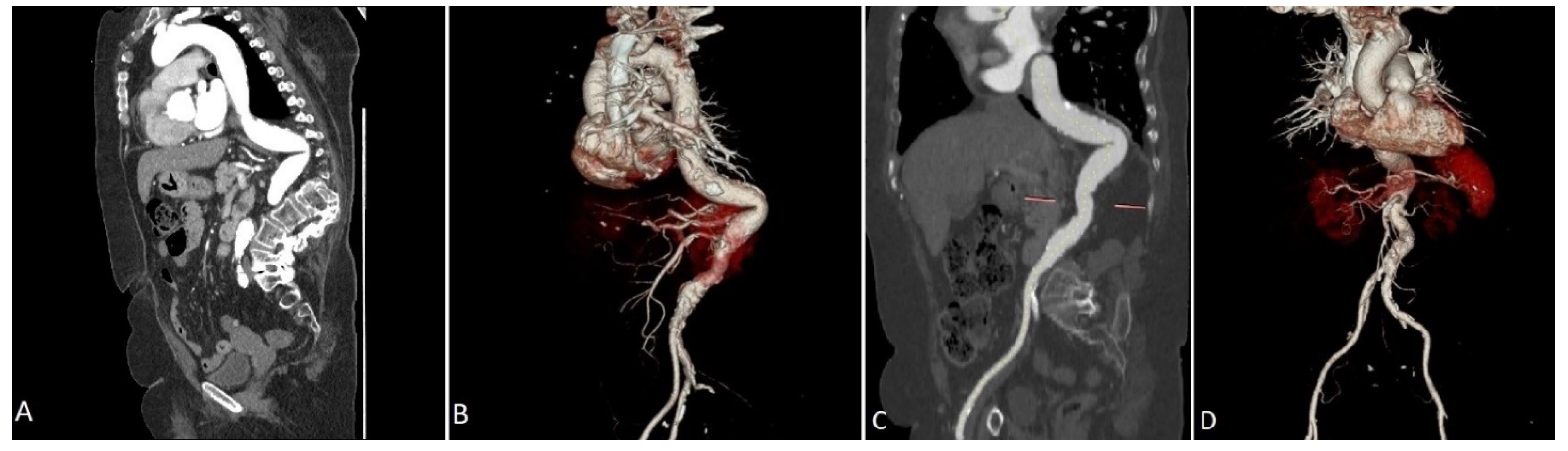
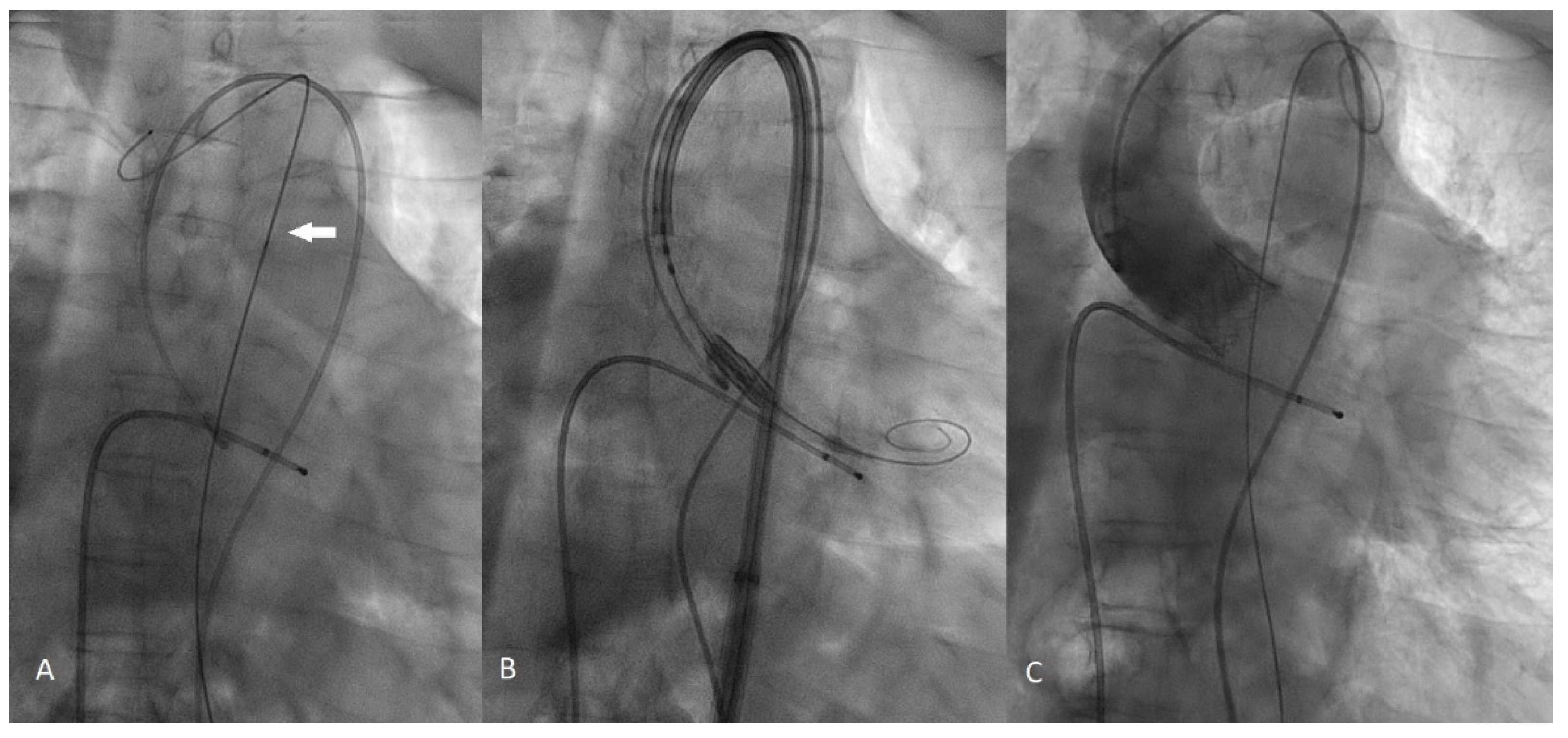
2. Case Presentation
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Danielsen, R.; Aspelund, T.; Harris, T.B.; Gudnason, V. The prevalence of aortic stenosis in the elderly in Iceland and predictions for the coming decades: The AGES-Reykjavík study. Int. J. Cardiol. 2014, 176, 916–922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campo, J.; Tsoris, A.; Kruse, J.; Karim, A.; Andrei, A.C.; Liu, M.; Bonow, R.O.; McCarthy, P.; Malaisrie, S.C. Prognosis of Severe Asymptomatic Aortic Stenosis with and without Surgery. Ann. Thorac. Surg. 2019, 108, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Cribier, A.; Eltchaninoff, H.; Bash, A.; Borenstein, N.; Tron, C.; Bauer, F.; Derumeaux, G.; Anselme, F.; Laborde, F.; Leon, M.B. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: First human case description. Circulation 2002, 106, 3006–3008. [Google Scholar] [CrossRef] [PubMed]
- Leon, M.B.; Smith, C.R.; Mack, M.J.; Makkar, R.R.; Svensson, L.G.; Kodali, S.K.; Thourani, V.H.; Tuzcu, E.M.; Miller, D.C.; Herrmann, H.C.; et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N. Engl. J. Med. 2016, 374, 1609–1620. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Toleva, O.; Ravandi, A.; Pozeg, Z.; Menkis, A.; Kass, M. Transcatheter Aortic Valve Implantation in an Extremely Tortuous S-Shaped Aorta. Case Rep. Cardiol. 2017, 2017, 2936513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hachinohe, D.; Shitan, H.; Kaneko, U.; Kobayashi, K.; Mitsube, K.; Koushima, R. Transfemoral transcatheter aortic valve implantation for bicuspid aortic stenosis with tortuous aorta after total arch replacement. Cardiovasc. Interv. Ther. 2020, 37, 238–239. [Google Scholar] [CrossRef] [PubMed]
- Bergman, H.; Ferrucci, L.; Guralnik, J.; Hogan, D.B.; Hummel, S.; Karunananthan, S.; Wolfson, C. Frailty: An emerging research and clinical paradigm—Issues and controversies. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 731–737. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Dawson, E.; Moodie, J.; Martin, J.; Bagur, R.; Cheng, D.; Kiaii, B.; John-Baptiste, A. Frailty in patients undergoing transcatheter aortic valve implantation: A protocol for a systematic review. BMJ Open 2019, 9, e024163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beurtheret, S.; Karam, N.; Resseguier, N.; Houel, R.; Modine, T.; Folliguet, T.; Chamandi, C.; Com, O.; Gelisse, R.; Bille, J.; et al. Femoral Versus Nonfemoral Peripheral Access for Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2019, 74, 2728–2739. [Google Scholar] [CrossRef] [PubMed]
- Buzzatti, N.; Mangieri, A.; Cota, L.; Ruparelia, N.; Romano, V.; Alfieri, O.; Colombo, A.; Montorfano, M. Use of double stiff wire allows successful transfemoral transcatheter aortic valve implantation through extreme thoracic aorta tortuosity. Cardiovasc. Interv. 2015, 8, e002331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashida, K.; Lefèvre, T.; Chevalier, B.; Hovasse, T.; Romano, M.; Garot, P.; Mylotte, D.; Uribe, J.; Farge, A.; Donzeau-Gouge, P.; et al. Transfemoral aortic valve implantation new criteria to predict vascular complications. JACC Cardiovasc. Interv. 2011, 4, 851–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langer, N.B.; Hamid, N.B.; Nazif, T.M.; Khalique, O.K.; Vahl, T.P.; White, J.; Terre, J.; Hastings, R.; Leung, D.; Hahn, R.T.; et al. Injuries to the Aorta, Aortic Annulus, and Left Ventricle During Transcatheter Aortic Valve Replacement: Management and Outcomes. Circ. Cardiovasc. Interv. 2017, 10, e004735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vavuranakis, M.; Kariori, M.; Voudris, V.; Kalogeras, K.; Vrachatis, D.; Aznaouridis, C.; Moldovan, C.; Masoura, C.; Thomopoulou, S.; Lazaros, G.; et al. Predictive factors of vascular complications after transcatheter aortic valve implantation in patients treated with a default percutaneous strategy. Cardiovasc. Ther. 2013, 31, e46–e54. [Google Scholar] [CrossRef] [PubMed]
- Sergi, D.; Acconcia, M.C.; Muscoli, S.; Perrone, M.A.; Cammalleri, V.; Di Luozzo, M.; Marchei, M.; Giannoni, M.F.; Barillà, F.; Gaudio, C.; et al. Meta-analysis of the impact on early and late mortality of TAVI compared to surgical aortic valve replacement in high and low- intermediate surgical risk patients. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 5402–5412. [Google Scholar] [PubMed]
- Perrone, M.A.; Donatucci, B.; Salvati, A.; Gualtieri, P.; De Lorenzo, A.; Romeo, F.; Bernardini, S. Inflammation, oxidative stress and gene expression: The postprandial approach in professional soccer players to reduce the risk of muscle injuries and early atherosclerosis. Med. Sport 2019, 72, 234–243. [Google Scholar] [CrossRef]
- Naganuma, T.; Mitomo, S.; Yabushita, H.; Nakao, T.; Lazarevic, A.; Nakamura, S. Buddy wire technique for successful transfemoral transcatheter aortic valve implantation through an extremely tortuous abdominal aorta: A basic technique in Asian patients? AsiaIntervention 2017, 3, 90–92. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Intorcia, A.; Ambrosini, V.; Capasso, M.; Granata, R.; Magliulo, F.; Carbone, G.L.; Capobianco, S.; Rotondi, F.; Lanni, F.; Manganelli, F.; et al. Management of Transcatheter Aortic Valve Implantation and Complex Aorta Anatomy: The Importance of Pre-Procedural Planning. Int. J. Environ. Res. Public Health 2022, 19, 4763. https://doi.org/10.3390/ijerph19084763
Intorcia A, Ambrosini V, Capasso M, Granata R, Magliulo F, Carbone GL, Capobianco S, Rotondi F, Lanni F, Manganelli F, et al. Management of Transcatheter Aortic Valve Implantation and Complex Aorta Anatomy: The Importance of Pre-Procedural Planning. International Journal of Environmental Research and Public Health. 2022; 19(8):4763. https://doi.org/10.3390/ijerph19084763
Chicago/Turabian StyleIntorcia, Alfredo, Vittorio Ambrosini, Michele Capasso, Riccardo Granata, Fabio Magliulo, Giannignazio Luigi Carbone, Stefano Capobianco, Francesco Rotondi, Francesca Lanni, Fiore Manganelli, and et al. 2022. "Management of Transcatheter Aortic Valve Implantation and Complex Aorta Anatomy: The Importance of Pre-Procedural Planning" International Journal of Environmental Research and Public Health 19, no. 8: 4763. https://doi.org/10.3390/ijerph19084763
APA StyleIntorcia, A., Ambrosini, V., Capasso, M., Granata, R., Magliulo, F., Carbone, G. L., Capobianco, S., Rotondi, F., Lanni, F., Manganelli, F., & Di Lorenzo, E. (2022). Management of Transcatheter Aortic Valve Implantation and Complex Aorta Anatomy: The Importance of Pre-Procedural Planning. International Journal of Environmental Research and Public Health, 19(8), 4763. https://doi.org/10.3390/ijerph19084763