
Snakebite Treatment in Tanzania: Identifying Gaps in Community Practices and Hospital Resources


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection
2.3. Participants
2.4. Ethical Statement
2.5. Quantitative Analysis
2.5.1. Demographic Information
2.5.2. Hospital Resources for Snakebite Treatment
2.5.3. Care of Snakebite Victim
2.6. Qualitative Analysis
3. Results
3.1. Demographics
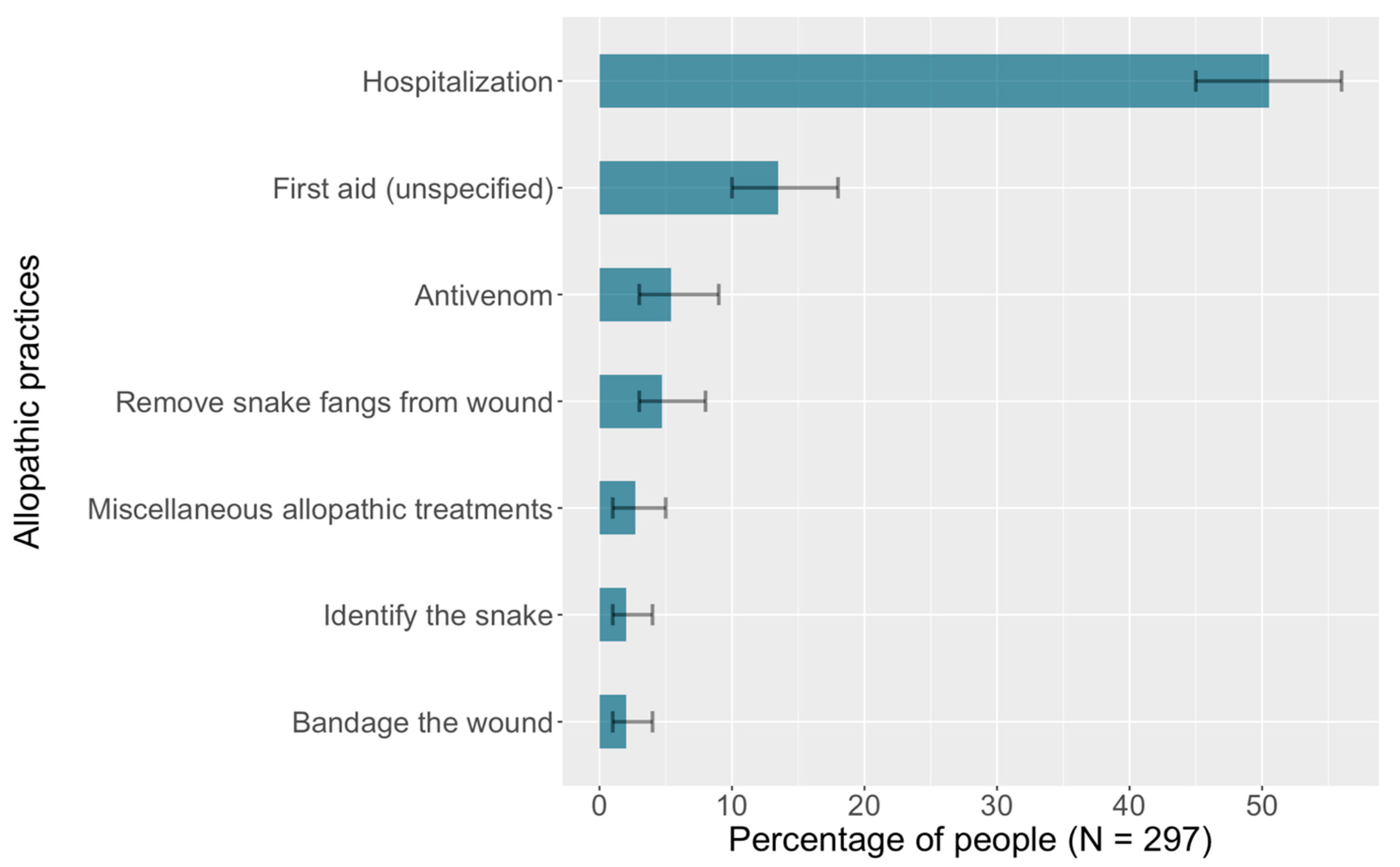
3.2. Community Practices to Treat Snakebite
3.3. Hospital Resources for Snakebite Treatment
3.4. Care of Snakebite Victim
4. Discussion
4.1. Community Practices to Treat Snakebite
4.2. Hospital Resources for Snakebite Treatment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Reassure the patient. Remove anything that may be restricted by swelling such as rings and bracelets.
- If the patient presents with a tourniquet, immediately ready an intravenous drip and artificial respiration.
- Remove any tourniquets very gradually in case there is sudden drop in blood pressure upon release.
- Clean the bitten site with clean water to remove any poison and remove any fangs.
- Elevate a painful swollen limb.
- Assess degree of envenomation. By vipers expect rapid swelling for 24 h. (In severe envenomation by vipers, rapid leg swelling from hemorrhage into anterior compartment of lower limb may contain as much as 2 units of blood.)
- Rarely will there be need to use specific antivenom.
- When indicated (by the degree of envenomation) use polyvalent anti-snakes venom (PAV).
- Infuse 80–100 mL of (PAV) diluted in 500 mL normal saline and start drip very slowly. If somebody is in serious condition on arrival, it can be helpful to give a direct push through the drip’s canula of the first 5–10 mL., and the 2nd/3rd vial can run through in the drip.
- Watch for sensitivity reaction and be prepared with already drawn out 100 mg Adrenaline. If reaction occurs, stop drip and give Adrenaline and restart drip after 1 h and again watch for reaction. For full-blown anaphylaxis or late serum sickness, give 100 mg. hydrocortisone.
- Note: Reaction is from horse serum contained in the polyvalent serum.
- Dose of polyvalent serum will depend on degree of envenomation. The usual dose is one vial of PAV antivenom with a second vial available if needed. Same for both adults and children. The SAMRI variety of polyvalent is best compared to others. Use polyvalent because often the type of snake is unknown. There are specific monovalent sera where type of snake is known.
- Debride necrotic tissue where necessary, once clotting times are back to normal.
- Analgesics (such as Aspirin, Ibruprofen, and others that can cause bleeding), antihistamines, and blood letting are all absolutely contraindicated. With reassurance and competent clinical observation, very few cases need active treatment because envenomation is rare.
- A 20 min Whole Blood Clotting Test is useful. A bleeding problem may not show clinically but would show in a test much earlier. Any bite at all that is not showing some very obvious symptoms should get at least a couple of tests, 3–6 h apart before any decision to discharge the patient.
- Debridement of necrotic tissue can only be undertaken if clotting times are back to normal.
- Snake venom spat into eyes must be washed thoroughly with water. Even after eyes have been thoroughly rinsed, they will remain red and painful and should be kept shaded until the redness clears. Secondary infection can be prevented by antibiotic eye-ointment/drops.
References
- Gutiérrez, J.M.; Calvete, J.J.; Habib, A.G.; Harrison, R.A.; Williams, D.J.; Warrell, D.A. Snakebite Envenoming. Nat. Rev. Dis. Primers 2017, 3, 17063. [Google Scholar] [CrossRef] [PubMed]
- Snakebite Envenoming. Available online: https://www.who.int/news-room/fact-sheets/detail/snakebite-envenoming (accessed on 19 March 2022).
- Kasturiratne, A.; Wickremasinghe, A.R.; de Silva, N.; Gunawardena, N.K.; Pathmeswaran, A.; Premaratna, R.; Savioli, L.; Lalloo, D.G.; de Silva, H.J. The Global Burden of Snakebite: A Literature Analysis and Modelling Based on Regional Estimates of Envenoming and Deaths. PLoS Med. 2008, 5, e218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Snakebite Envenoming—A Strategy for Prevention and Control. Available online: http://www.who.int/snakebites/resources/9789241515641/en/ (accessed on 20 December 2020).
- WHO. What Is Snakebite Envenoming? Available online: http://www.who.int/snakebites/disease/en/ (accessed on 7 March 2019).
- Goswami, P.K.; Samant, M.; Srivastava, R.S. Snake Venom, Anti-Snake Venom & Potential of Snake Venom. Int. J. Pharm. Pharm. Sci. 2014, 6, 4–7. [Google Scholar]
- Gopalakrishnakone, P.; Faiz, A.; Fernando, R.; Gnanathasan, C.A.; Habib, A.G.; Yang, C.-C. (Eds.) Clinical Toxinology in Asia Pacific and Africa; Springer: Dordrecht, The Netherlands, 2015; ISBN 978-94-007-6385-2. [Google Scholar]
- Chippaux, J.-P. Guidelines for the production, control and regulation of snake antivenom immunoglobulins. Biol. Aujourdhui 2010, 204, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Kasturiratne, A.; Lalloo, D.G.; Janaka de Silva, H. Chronic Health Effects and Cost of Snakebite. Toxicon X 2021, 9–10, 100074. [Google Scholar] [CrossRef]
- Harrison, R.A.; Hargreaves, A.; Wagstaff, S.C.; Faragher, B.; Lalloo, D.G. Snake Envenoming: A Disease of Poverty. PLoS Negl. Trop. Dis. 2009, 3, e569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halilu, S.; Iliyasu, G.; Hamza, M.; Chippaux, J.-P.; Kuznik, A.; Habib, A.G. Snakebite Burden in Sub-Saharan Africa: Estimates from 41 Countries. Toxicon 2019, 159, 1–4. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines for the Production, Control and Regulation of Snake Antivenom Immunoglobulins. Available online: https://www.medbox.org/pdf/5e148832db60a2044c2d4b8a (accessed on 19 December 2020).
- Consequences of Neglect: Analysis of the Sub-Saharan African Snake Antivenom Market and the Global Context. Available online: https://www.researchgate.net/publication/225281099_Consequences_of_Neglect_Analysis_of_the_Sub-Saharan_African_Snake_Antivenom_Market_and_the_Global_Context (accessed on 25 September 2021).
- Sloan, D.J.; Dedicoat, M.J.; Lalloo, D.G. Healthcare-Seeking Behaviour and Use of Traditional Healers after Snakebite in Hlabisa Sub-District, KwaZulu Natal. Trop. Med. Int. Health 2007, 12, 1386–1390. [Google Scholar] [CrossRef]
- Global Ecological Zones (GEZ) Mapping|Global Forest Resources Assessments|Food and Agriculture Organization of the United Nations. Available online: https://www.fao.org/forest-resources-assessment/remote-sensing/global-ecological-zones-gez-mapping/en/ (accessed on 27 November 2021).
- What Is a Shrubland?—WorldAtlas. Available online: https://www.worldatlas.com/articles/what-is-a-shrubland.html (accessed on 20 March 2022).
- Gradstein, S.; Homeier, J.; Gansert, D. The Tropical Mountain Forest—Patterns and Processes in a Biodiversity Hotspot; Universitätsverlag Göttingen: Göttingen, Germany, 2008; Volume 2, ISBN 978-3-940344-22-9. [Google Scholar]
- Mwinyi HDH. Minister for Health and Social Welfare. Standard Treatment Guidelines and Essential Medicines List, Fourth Edition, May 2013. Available online: https://www.pascar.org/uploads/files/Tanzania_-_Standard_Treatment_Guidelines_and_Essential_Medicines_List_-_Fourth_Edition.pdf (accessed on 27 November 2021).
- World Health Organization, Regional Office for Africa. Guidelines for the Prevention and Clinical Management of Snakebite in Africa; World Health Organization, Regional Office for Africa: Brazzaville, Congo, 2010; ISBN 978-92-9023-168-4. [Google Scholar]
- Traditional, Complementary and Integrative Medicine. Available online: https://www.who.int/westernpacific/health-topics/traditional-complementary-and-integrative-medicine (accessed on 16 October 2021).
- Bachelor of Science in Nursing in Tanzania. Available online: https://www.courseseye.com/course/58/bachelor-of-science-in-nursing/tanzania (accessed on 20 March 2022).
- UIS Statistics. Available online: http://data.uis.unesco.org/# (accessed on 31 July 2021).
- Taieb, F.; Dub, T.; Madec, Y.; Tondeur, L.; Chippaux, J.P.; Lebreton, M.; Medang, R.; Foute, F.N.N.; Tchoffo, D.; Potet, J.; et al. Knowledge, Attitude and Practices of Snakebite Management amongst Health Workers in Cameroon: Need for Continuous Training and Capacity Building. PLoS Negl. Trop. Dis. 2018, 12, e0006716. [Google Scholar] [CrossRef] [Green Version]
- Bhaumik, S.; Beri, D.; Lassi, Z.S.; Jagnoor, J. Interventions for the Management of Snakebite Envenoming: An Overview of Systematic Reviews. PLoS Negl. Trop. Dis. 2020, 14, e0008727. [Google Scholar] [CrossRef]
- Sutherland, S.K.; Coulter, A.R.; Harris, R.D. Rationalisation of First-Aid Measures for Elapid Snakebite. Lancet 1979, 1, 183–185. [Google Scholar] [CrossRef]
- Norris, R.L.; Ngo, J.; Nolan, K.; Hooker, G. Physicians and Lay People Are Unable to Apply Pressure Immobilization Properly in a Simulated Snakebite Scenario. Wilderness Environ. Med. 2005, 16, 16–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canale, E.; Isbister, G.K.; Currie, B.J. Investigating Pressure Bandaging for Snakebite in a Simulated Setting: Bandage Type, Training and the Effect of Transport. Emerg. Med. Australas. 2009, 21, 184–190. [Google Scholar] [CrossRef] [PubMed]
- Alberts, M.B.; Shalit, M.; LoGalbo, F. Suction for Venomous Snakebite: A Study of “Mock Venom” Extraction in a Human Model. Ann. Emerg. Med. 2004, 43, 181–186. [Google Scholar] [CrossRef]
- Avau, B.; Borra, V.; Vandekerckhove, P.; De Buck, E. The Treatment of Snake Bites in a First Aid Setting: A Systematic Review. PLoS Negl. Trop. Dis. 2016, 10, e0005079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pymm, R. ‘Serpent Stones’: Myth and Medical Application. Geol. Soc. Lond. Spec. Publ. 2017, 452, 163–180. [Google Scholar] [CrossRef]
- Chippaux, J.-P.; Ramos-Cerrillo, B.; Stock, R.P. Study of the Efficacy of the Black Stone on Envenomation by Snake Bite in the Murine Model. Toxicon 2007, 49, 717–720. [Google Scholar] [CrossRef]
- Blaylock, R. The Identification and Syndromic Management of Snakebite in South Africa. S. Afr. Fam. Pract. 2005, 47, 48–53. [Google Scholar] [CrossRef]
- Ozioma, E.-O.J.; NwamakaChinwe, O.A. Herbal Medicines in African Traditional Medicine; IntechOpen: London, UK, 2019; ISBN 978-1-78984-783-3. [Google Scholar]
- Tella, A. The Practice of Traditional Medicine in Africa. Niger. Med. J. 1979, 9, 607–612. [Google Scholar]
- Pucca, M.B.; Knudsen, C.; Oliveira, I.S.; Rimbault, C.; Cerni, F.A.; Wen, F.H.; Sachett, J.; Sartim, M.A.; Laustsen, A.H.; Monteiro, W.M. Current Knowledge on Snake Dry Bites. Toxins 2020, 12, 668. [Google Scholar] [CrossRef]
- Steinhorst, J.; Aglanu, L.M.; Ravensbergen, S.J.; Dari, C.D.; Abass, K.M.; Mireku, S.O.; Poku, J.K.A.; Enuameh, Y.A.K.; Blessmann, J.; Harrison, R.A.; et al. The Medicine Is Not for Sale’: Practices of Traditional Healers in Snakebite Envenoming in Ghana. PLoS Negl. Trop. Dis. 2021, 15, e0009298. [Google Scholar] [CrossRef] [PubMed]
- Fokunang, C.; Ndikum, V.; Tabi, O.; Jiofack, R.; Ngameni, B.; Guedje, N.; Tembe-Fokunang, E.; Tomkins, P.; Barkwan, S.; Kechia, F.; et al. Traditional Medicine: Past, Present and Future Research and Development Prospects and Integration in the National Health System of Cameroon. Afr. J. Tradit. Complement. Altern. Med. 2011, 8, 284–295. [Google Scholar] [CrossRef] [PubMed]
- Sani, I.; Hassan, S.; Faruq, U. Antisnake Venoms and Their Mechanisms of Action: A Review. Saudi J. Med. Pharm. Sci. 2018, 4, 512–520. [Google Scholar] [CrossRef]
- Jenkins, T.P.; Laustsen, A.H. Cost of Manufacturing for Recombinant Snakebite Antivenoms. Front. Bioeng. Biotechnol. 2020, 8, 703. [Google Scholar] [CrossRef] [PubMed]
- Potet, J.; Smith, J.; McIver, L. Reviewing Evidence of the Clinical Effectiveness of Commercially Available Antivenoms in Sub-Saharan Africa Identifies the Need for a Multi-Centre, Multi-Antivenom Clinical Trial. PLoS Negl. Trop. Dis. 2019, 13, e0007551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polyvalent Snake Antivenom (Australia-PNG). Available online: https://www.nps.org.au/medicine-finder/polyvalent-snake-antivenom-concentrate-for-infusion (accessed on 30 October 2021).
- Yates, V.M.; Lebas, E.; Orpiay, R.; Bale, B.J. Management of Snakebites by the Staff of a Rural Clinic: The Impact of Providing Free Antivenom in a Nurse-Led Clinic in Meserani, Tanzania. Ann. Trop. Med. Parasitol. 2010, 104, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, J.M.; Chippaux, J.-P.; Sambo, B.T.; Massougbodji, A. Delayed Double Reading of Whole Blood Clotting Test (WBCT) Results at 20 and 30 Minutes Enhances Diagnosis and Treatment of Viper Envenomation. J. Venom. Anim. Toxins Incl. Trop. Dis. 2018, 24, 14. [Google Scholar] [CrossRef] [Green Version]
- Gaus, D.P.; Herrera, D.F.; Troya, C.J.; Guevara, A.H. Management of Snakebite and Systemic Envenomation in Rural Ecuador Using the 20-Minute Whole Blood Clotting Test. Wilderness Environ. Med. 2013, 24, 345–350. [Google Scholar] [CrossRef] [Green Version]
- Wiedenmayer, K.; Ombaka, E.; Kabudi, B.; Canavan, R.; Rajkumar, S.; Chilunda, F.; Sungi, S.; Stoermer, M. Adherence to Standard Treatment Guidelines among Prescribers in Primary Healthcare Facilities in the Dodoma Region of Tanzania. BMC Health Serv. Res. 2021, 21, 272. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Factors | Level | % (95% CI) * |
|---|---|---|
| Age (years) | 20–25 26–50 | 78 (73–82) 22 (18–27) |
| Sex | Male Female | 60 (54–65) 40 (35–46) |
| Location | Rural Urban | 78 (73–83) 22 (17–27) |
| Tropical dry forest Tropical moist deciduous forest Tropical mountain system Tropical rainforest Tropical shrubland | 10 (7–14) 16 (12–21) 24 (20–29) 15 (11–20) 35 (29–40) | |
| Program | Bachelor of Science in Nursing Other | 80 (75–84) 20 (16–25) |
| Community Practices | % (95% CI) |
|---|---|
| Only traditional | 44 (39–50) |
| Only allopathic | 7 (5–11) |
| Both | 49 (43–54) |
| Factors | Level | % (95% CI) ** |
|---|---|---|
| Was an intravenous drip available? | Yes No | 75 (58–87) 25 (13–42) |
| Was artificial respiration available? | Yes No | 55 (38–71) 45 (29–62) |
| Were Ministry of Health guidelines for treating snakebite available? | Yes No | 42 (26–59) 58 (41–74) |
| Was polyvalent anti-snake venom available? | Yes No | 42 (26–59) 58 (41–74) |
| Was the whole blood clotting test available? | Yes No | 48 (32–65) 52 (35–68) |
| Factor | Level | % (95% CI) |
|---|---|---|
| How many hours before the patient arrived at the hospital for treatment? (N = 41) | <1 h 1–2 h 3–4 h 5–6 h 1 day or more | 27 (16–42) 29 (18–44) 15 (7–28) 15 (7–28) 14 (7–28) |
| Which of the following was done (before arrival to the hospital)? (N = 64) |
| 6 (2–15) 31 (21–43) 67 (55–77) 28 (19–40) 5 (2–13) 23 (15–35) 59 (47–71) 20 (12–32)
|
| Did the patient die? (N = 58) | Yes No | 14 (7–25) 86 (75–93) |
| Was the patient left with lasting damage? (N = 41) | Yes No | 32 (20–47) 68 (53–80) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Margono, F.; Outwater, A.H.; Lowery Wilson, M.; Howell, K.M.; Bärnighausen, T. Snakebite Treatment in Tanzania: Identifying Gaps in Community Practices and Hospital Resources. Int. J. Environ. Res. Public Health 2022, 19, 4701. https://doi.org/10.3390/ijerph19084701
Margono F, Outwater AH, Lowery Wilson M, Howell KM, Bärnighausen T. Snakebite Treatment in Tanzania: Identifying Gaps in Community Practices and Hospital Resources. International Journal of Environmental Research and Public Health. 2022; 19(8):4701. https://doi.org/10.3390/ijerph19084701
Chicago/Turabian StyleMargono, Felicia, Anne H. Outwater, Michael Lowery Wilson, Kim M. Howell, and Till Bärnighausen. 2022. "Snakebite Treatment in Tanzania: Identifying Gaps in Community Practices and Hospital Resources" International Journal of Environmental Research and Public Health 19, no. 8: 4701. https://doi.org/10.3390/ijerph19084701
APA StyleMargono, F., Outwater, A. H., Lowery Wilson, M., Howell, K. M., & Bärnighausen, T. (2022). Snakebite Treatment in Tanzania: Identifying Gaps in Community Practices and Hospital Resources. International Journal of Environmental Research and Public Health, 19(8), 4701. https://doi.org/10.3390/ijerph19084701