
Risk Perception towards COVID-19: A Systematic Review and Qualitative Synthesis




Abstract
:1. Introduction
2. Materials and Methods
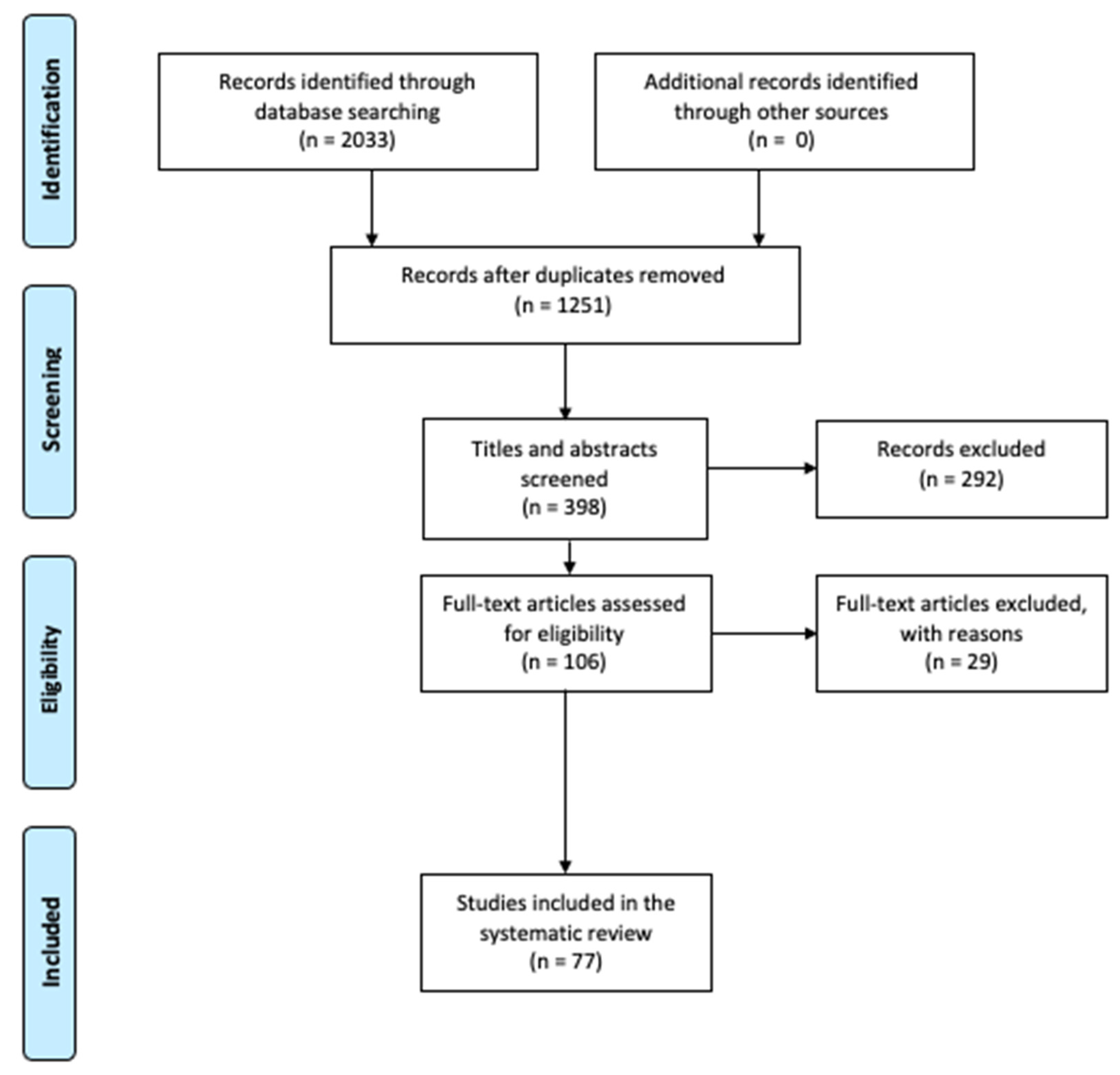
2.1. Search Strategy
2.2. Study Selection and Inclusion Criteria
2.3. Data Extraction
3. Results
3.1. Engagement in Preventive Behaviors and Compliance with Government Recommendations
3.2. Demographic Factors
3.2.1. Age
3.2.2. Gender
3.2.3. Income
3.2.4. Employment
3.2.5. Education
3.3. Personal Factors
3.3.1. Health Status
3.3.2. Mass Media Exposure
3.3.3. COVID-19 Knowledge
3.3.4. Wellbeing
3.3.5. Political Orientation
3.3.6. Trust
3.3.7. Personality and Conspiracy Mentality
3.3.8. Optimistic Bias and Positivity
3.3.9. Direct and Indirect Experience of COVID-19
3.3.10. Propensity to Vaccinate
3.4. Geographical Factors
3.5. Timing
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Authors | Country | Sample | Data Collection Methods | Risk Perception Measures | Key Findings |
|---|---|---|---|---|---|
| Germani et al., 2020 [7] | Italy | 1045 emerging adults (30% M, 70% F) | Cross-sectional online survey carried out in March | Five-point scale answers to 3 items (Perceived Risk Scale) | High perceived risk scores were reported, and risk awareness was positively correlated with anxiety |
| Yıldırım and Güler 2021 [8] | Turkey | 3109 adults (49.98% M, 50.02% F) | Cross-sectional online survey developed in April | Likert-type five-point scale answers to 8 items (COVID-19 Perceived Risk Scale) | Risk perception presented a significant direct effect on death distress, positivity, and happiness |
| Faasse and Newby 2020 [9] | Australia | 2174 residents (503 M, 1635 F, 36 other) | Cross-sectional online survey developed in March | 1 question with a five-point scale answer; 3 questions with Visual Analogue Scale (VAS) answers; 1 question with closed-ended options | Higher perceived personal severity of COVID-19 was a predictor of involvement in protective implementations |
| Wise et al., 2020 [13] | United States | 1591 adults (55% F, 40% M, 5% other) | A combined cross-sectional and longitudinal online survey (both held in March) | VAS-type scale answers | Optimistic bias was observed among participants, and risk perception increased on later dates. Education predicted higher risk perceptions and engagement in precautionary behaviors |
| Lohiniva et al., 2020 [14] | Finland | 116 social media posts and emails from the public | Cross-sectional qualitative data collection done in February | Analysis of social media posts and emails to build a thematic analysis of risk perception | Five different risk perception domains were observed, and people showed low personal control over the situation |
| Kuang et al., 2020 [15] | India | 2044 adults (46% F, 54% M) | Cross-sectional phone call surveys (open-ended questions) were conducted in May | 1 open question about perceived personal risk of contracting COVID-19 | Low perceived risk of contracting coronavirus was found |
| Moyce et al., 2021 [16] | United States | 20 Latinos living in a rural American community | 14 semi-structured interviews with participants over the phone conducted in April | 3 open questions | Latinos are less likely to fear the virus because they tend to be more worried with having a pay cut or a job loss |
| Casanova et al., 2020 [17] | Italy | 25 patients receiving treatment, 25 patients that had completed treatment, and 25 healthy peers | A semi-structured online qualitative questionnaire held in March | 6 closed-ended questions | The majority presented high risk perceptions and feared for the consequences of being infected with COVID-19 |
| Ilesanmi and Afolabi 2020 [18] | Nigeria | 360 adults (62.5% F, 37.5% M) | Cross-sectional interviewer-administered questionnaire driven in June | 3 closed-ended questions | The sample presented poor knowledge and low risk awareness towards the new coronavirus |
| Mouchtouri et al., 2020 [19] | Greece | 1858 residents (41.2% M, 58.8% F) | Cross-sectional telephone questionnaire (closed- and open-ended questions) conducted between April and May | Four- or five-point scale type of answers | Most respondents had a sound knowledge of COVID-19, but good practices were not reported on the same level |
| Asefa et al., 2020 [20] | Ethiopia | 416 waiters (191 M, 225 F) | Cross-sectional structured face-to-face questionnaire conducted in June | Likert-type five-point scale answers to 12 items | 53.4% of participants presented high risk perception related with being older, knowledge about COVID-19, and partaking preventive behaviors |
| de Bruin and Bennett 2020 [21] | United States | 6684 adults (3226 M, 3458 F) | Extensive cross-sectional online survey carried out in March | 2 items with a 0–100% visual linear scale type of answer | Low perceived infection and fatality risks. Perceiving greater risks was linked with implementation of protective behaviors |
| Duan et al., 2020 [22] | China | 3837 adults (1985 M, 1852 F) | Cross-sectional online questionnaire held in February | Five-point scale answers to 3 items | Risk perception was the mediating factor between government intervention and public’s engagement in preventive behaviors |
| Lee et al., 2021 [23] | South Korea | 328 middle school students: 146 boys, 182 girls | Cross-sectional online survey collected from September to October | Likert-type five-point scale answers to 4 items | Risk perception was significantly related to protective behaviors as well as gender and health status |
| Rivas et al., 2021 [24] | Bolivia | 886 Bolivians: 65.1% F, 34.9% M | Cross-sectional online survey carried out during April and May | Likert-type seven-point scale answers to 4 items | COVID-19 information exposure, gender, and adoption of preventive behaviors were positively correlated with risk perception |
| Savadori and Lauriola 2020 [25] | Italy | 572 citizens (54% M, 46% F) | Cross-sectional online survey developed in March | 10 items covering risk perception with scale type of answer | Respect for social norms and risk perceptions predicted protective behaviors |
| Xie et al., 2020 [26] | China | 317 adults (48.3% F, 51.7% M) | Cross-sectional online survey conducted in May | Likert-type five-point scale answers to 7 items | Changes in safety behaviors are associated with risk perception and COVID-19 knowledge |
| Zanin et al., 2020 [27] | Italy | 8713 citizens (3490 M, 5223 F). 8282 lived in Italy and 431 abroad | Cross-sectional online questionnaire conducted in March | 1 closed-ended question with 4 options | People’s risk perception plays a key role in the adoption of safety actions, in people’s feelings, and in their daily habits |
| Park et al., 2021 [28] | United States | 260 adults (61.77% M, 38.23% F). | Cross-sectional online survey | Likert-type seven-point scale answers to 5 items | OB is negatively related to risk perception, and risk perception increases the use of COVID-19 preventive behaviors |
| Ahmad et al., 2020 [29] | China | 302 participants from 6 Chinese Universities and 2 hospitals (59.93% M, 40.07% F) | Cross-sectional online survey | Likert-type five-point scale answers to 5 items | Government’s guidelines, risk perception, and epidemic knowledge influenced engagement in protective behaviors |
| Atchison et al., 2021 [30] | United Kingdom | 2108 adults (987 M, 1094 F) | Cross-sectional online survey developed in March | Closed-ended questions regarding perceived susceptibility and severity | There was a high engagement in preventive measures correlated with government’s guidance and income |
| Tomczyk et al., 2020 [31] | Germany | 157 adults (80% F, 20% M) | Cross-sectional online survey developed in March | 2 items with 0–100% type of answer | Compliance with COVID-19 behavioral recommendations was associated with gender, age, education, and risk perception |
| McFadden et al., 2020 [32] | United States | 718 adults (330 M, 386 F) | Cross-sectional online survey developed in February | Likert-type five-point scale answers to 10 items | Risk perception score was low, and most participants supported the use of restrictive policies for infection prevention |
| Taghrir et al., 2020 [33] | Iran | 240 medical students (98 M, 142 F) | Cross-sectional online survey performed in February | Likert-type four-point scale answers to 2 items | High levels of knowledge and adoption of preventive behaviors were reported as well as moderate risk perceptions. A negative correlation between preventive behaviors and risk perception was present |
| Mansilla Domínguez et al., 2020 [34] | Spain | 16201 adults (51.5% F, 48.5% M) | Cross-sectional online survey was conducted for 5 consecutive days | 59 items divided in 4 content areas (including risk perception) and different answer types | Gender, age, direct contact with the virus, employment, and health perception were associated with risk awareness |
| Mora-Rodríguez and Melero-López 2021 [35] | Spain | 2034 citizens (52% F, 48% M) | Cross-sectional online questionnaire carried out in March | Likert-type five-point scale answers to 4 items | Greater exposure to COVID-19 news increased personal risk perception. Being older and female predicted higher risk awareness |
| Roupa et al., 2021 [36] | Cyprus | 494 Healthcare workers (HCW) (66.7% F, 33.3% M) and nurses (75.4%) | Cross-sectional online questionnaire that took place in May | Likert-type four-point scale answers to 5 items | No significant correlation was found between COVID-19 perceptions and knowledge |
| Iorfa et al., 2020 [37] | Nigeria | 1554 adults (42.7% F, 57.3% M) | Cross-sectional online survey developed in April | Likert-type seven-point scale answers to 9 items | Risk perception mediates the link between COVID-19 knowledge and adoption of preventive behaviors. Age and gender influence this adoption |
| Lanciano et al., 2020 [38] | Italy | 980 adults (544 F, 436 M) | Cross-sectional online survey conducted in April | Ten-point scale answers to 11 items | Financial and work risk perceptions were higher than the health one. Involvement in preventive measures was related with age, gender, and education |
| Ciancio et al., 2020 [39] | United States | 5414 adults | Cross-sectional online survey that was driven in March | 4 items with 0–100 scales | An overestimated mortality risk was observed; risk perception was related to age, education, sources of news, and location |
| Germani et al., 2020 [40] | Italy | 1011 emerging adults (291 M, 720 F) | Cross-sectional online survey developed in March | Five-point scale answers to 3 risk perception dimensions: general/social, self/personal, and relatives/others | Participants showed a higher risk tolerance for their relatives than for themselves |
| Ding et al., 2020 [41] | China | 1461 college students (639 M, 822 F) | Cross-sectional online survey conducted in February | Five-point scale answers to 4 items | Chinese college students expressed high risk awareness (especially females and the ones located in the Hubei area) |
| Yang et al., 2020 [42] | Canada | 3037 adolescents and young adults from Quebec (74.6% F, 25.4% M) | Cross-sectional online survey collected in April | 11-point VAS scale answers to 2 items | Factors associated with higher risk perception include higher disease knowledge, presence of a chronic disease, and partaking in precautionary behaviors |
| Kabito et al., 2020 [43] | Ethiopia | 623 residents (402 F, 221 M) | Cross-sectional face-to-face structured questionnaires conducted in April | Five-point scale answers to 5 items | Participants showed low levels of risk perceptions. Age, education, and knowledge were associated with risk awareness |
| Harapan et al., 2020 [44] | Indonesia | 1379 adults (65.7% F, 34.3% M) | Cross-sectional online questionnaire driven between March and April | 1 item with 0–100% type of answer | High risk perception was linked with age, income, being unmarried, living area, and profession. Participants showed low risk awareness |
| Dryhurst et al., 2020 [45] | Australia, Germany, Italy, Japan, South Korea, Spain, Sweden, UK, and USA | 6991 participants | Cross-sectional online survey (data were collected between March and April) | Likert-type seven-point/five-point scale answers to 6 items | Levels of concern are higher in the UK, and being male was associated with lower perceived risk |
| Jahangiry et al., 2020 [46] | Iran | 3727 adults (1933 F, 1794 M) | Cross-sectional online survey carried out between March and April | Likert-type five-point scale answers to 8 items | 56.4% of participants were implementing preventive behaviors |
| Abir et al., 2020 [47] | Bangladesh | Two samples (N1 = 322 and N2 = 683) | Two cross-sectional online surveys (one conducted in March and the other in May) | Likert-type five-point scale answers to 5 items | Low risk perception was associated with gender and education. Perceived risk scores decreased between early and late lockdown |
| Karasneh et al., 2021 [48] | Jordan | 486 pharmacists (382 F, 104 M) | Cross-sectional online questionnaire | Likert-type three-point scale answers | Risk was highly perceived among participants, and it was predicted by gender and location. Media use influenced risk awareness |
| Wang et al., 2020 [49] | China | 2058 participants (54.2% F, 45.8% M) | Cross-sectional online survey developed in March | Closed-ended questions | Most participants stated they would get vaccinated in the future. This was related with gender, being married, and high-risk perceptions |
| Karout et al., 2020 [50] | United States | 410 Latino participants (65.9% F, 34.1% M) | Cross-sectional semi-structured questionnaire/interview collected between July and August | Three-point scale answers to 9 items | Low risk perception scores and low engagement in preventive behaviors were found among respondents |
| Chou et al., 2020 [51] | China (Taiwan region) | 1954 adults (649 M, 1305 F; 640 HCW and 1314 members of the general public) | Cross-sectional online questionnaire developed in April | Five-item questionnaire with answers in scale-type | Healthcare professionals had a higher coronavirus risk perception and adopted more protective behaviors than the general public |
| Peres et al., 2020 [52] | Portugal | 3403 residents (2672 F, 731 M). HCW = 545 | Cross-sectional online questionnaire conducted in March | Likert-scale type of answers to 6 items | Healthcare workers presented higher COVID-19 risk perception scores than the general population |
| Gorini et al., 2020 [53] | Italy | 650 HCW (439 F, 211 M) from two hospitals in Lombardy | Cross-sectional online questionnaire conducted in May | Slider-scale type of answer (0–100) to 4 items | Healthcare professionals believed they were more at risk for contracting COVID-19 than their family members. Nurses showed the highest risk perception scores |
| González et al., 2021 [54] | Spain | 557 nurses from 26 different public hospitals in Madrid (87.4% F, 12.6% M) | Cross-sectional online questionnaire collected in April | Likert-type four-point scale answers to 4 items | 37.5% of nurses were afraid of becoming infected and its consequences, and 62.8% were concerned about infecting their relatives |
| Niepel et al., 2020 [55] | United States | Two samples (N1 = 1182 and N2 = 953) | Cross-sectional online survey done in March and repeated in April | 9-point scale (0–75%) | There was a low perceived fatality risk among participants, but the numbers increased in the second survey done |
| Tran and Ravaud 2020 [56] | France | 7169 participants (5616 F, 1553 M) with chronic conditions | Cross-sectional online survey collected between March and April | 1 question with yes/no type of answer | 63% of the patients felt at risk of presenting severe illness if contracting COVID-19 because of their condition |
| Heydari et al., 2021 [57] | Iran | 3213 adults (1591 M, 1620 F) | Cross-sectional online survey performed in March | Likert-type five-point scale answers to 4 items | Risk perception mediates the relationship between risk communication and preventive behaviors |
| Seale et al., 2020 [58] | Australia | 1420 adults (740 F, 680 M) | Cross-sectional online survey carried out in March | Likert-type five-point scale answers to 10 items | Low risk perception scores were informed, and adopting preventive behaviors was associated with government trust |
| Vai et al., 2020 [59] | Italy | 2223 adults (675 M, 1548 F) | Cross-sectional online survey conducted between February and March | 2 questions with scale-type of answers | Attitude to vaccinate and utility of prevention behaviors were associated to COVID-19 risk perception and media use |
| Nazione et al., 2021 [60] | United States | 698 adults (53.7% F, 45.1% M, and 0.9% other) | Cross-sectional online survey collected in March | 8 items with closed-ended questions | Information exposure was not related with COVID-19 risk perception |
| Capone et al., 2020 [61] | Italy | 1124 University students (79.6% F, 20.4% M) | Cross-sectional online questionnaire performed in March | Likert-type seven-point scale answers to 2 items | University students presenting high levels of information seeking also showed higher levels of wellbeing and risk perception |
| Huang and Yang 2020 [62] | United States | 381 adults (58% M, 42% F) | A two-wave, cross-sectional online survey design conducted in April | Likert-type five-point scale answers to 2 items | Risk perception and uncertainty promote information seeking |
| Jiang 2020 [63] | China | 472 Chinese students (227 M, 245 F) | Cross-sectional online survey collected in February | 90-item symptom checklist scale with Likert-type five-point answers | 56% of students had sufficient knowledge of COVID-19 typical symptoms, and 57% of them reported high risk perception |
| Soni et al., 2021 [64] | India | 217 Delhi adults (116 F, 101 M) | Cross-sectional online survey opened between April and May | Five-point Likert scale answers to 6 items | Having knowledge about COVID-19 is essential to change someone’s perception and attitudes towards it |
| Geldsetzer 2020 [65] | USA and the UK | 2986 adults residing in the USA and 2988 in the UK | Cross-sectional online survey collected in February | 0–100% type of answers | The general public held several misconceptions regarding COVID-19 |
| Gollust et al., 2020 [66] | United States | 1007 American adults (62.6% were white, 12% Black, 16.5% Hispanic, and 8.9% other) | Cross-sectional online survey done in April | 4 items with closed-ended questions | Perceptions of mortality disparities were found among health status and age but not race or finances |
| Ding et al., 2020 [67] | China | 1081 adults (38.85% M, 61.15% F) | Cross-sectional online survey implemented in February | Five-point scale answers to 14 items | Risk perception strongly affects the public’s mental health. |
| Krok and Zarzycka 2020 [68] | Poland | 226 HCW (58.8% F, 41.2% M) | Cross-sectional online questionnaire held between March and May | Five-point scale answers to 18 items | Risk awareness is negatively related to psychological well-being and increases coping strategies |
| Liu et al., 2020 [69] | China | 4991 adults (2514 F, 2477 M) | Cross-sectional online survey held in February | Five-point Likert scale answers to 2 items | Respondents reported low-to-medium levels of risk perception, and high risk awareness was linked to more anxiety |
| Orte et al., 2020 [70] | Spain | 806 adults (248 M, 556 F, 1 other) | Cross-sectional online survey conducted in March | Five-point Likert scale answers to 17 items | There was a positive correlation between distress and COVID-19 risk perception |
| Qian and Li 2020 [71] | China | 351 adults (162 M, 189 F) | Cross-sectional online survey collected in February | 2 closed-ended questions | Risk event involvement was positively related to COVID-19 risk perception as well as anxiety |
| Spinelli et al., 2020 [72] | Italy | 854 parents of children aged between 2 and 14 years old (797 F, 57 M) | Cross-sectional online survey conducted in April | Scale-type of answers | Parents’ perceptions of the COVID-19 situation are deeply linked with parents’ stress levels and children’s psychological disturbances |
| Li et al., 2021 [73] | China (Taiwan region) | 1970 adults (1305 F, 650 M, 15 transgender) | Cross-sectional online survey completed in April | 5 questions with scale-type of answers | High risk perceptions mediated the association between lower perceived support and higher active coping with COVID-19 |
| de Bruin et al., 2020 [74] | United States | 5517 adults (48% M, 52% F; 37% Democrats, 32% Republicans, and 31% other) | Cross-sectional online survey that was driven in March | 4 questions with VAS-scale type of answers | Democrats showed higher perceived risk scores and likelihood to engage in preventive behaviors than Republicans |
| Lachlan et al., 2021 [75] | United States | 5000 residents (2435 M, 2558 F, 25 other, and 1 did not answer) | Cross-sectional online survey developed between April and June | Event Hazard/Outrage scale (32 items) | Risk perceptions may vary across preferences for conservative or liberal bias, but there are no differences in mitigation behavior across patterns of media use |
| Siegrist et al., 2021 [76] | Switzerland | 1585 citizens from the German-speaking part (50.9% F, 49.1% M) | Cross-sectional online survey that was driven between March and April | Seven-point scale type of answers to 7 items | People with high general trust perceive less risks associated with COVID-19 but not the ones with high social trust |
| Ye and Lyu 2020 [77] | China | 11783 adults | Cross-sectional online survey | Chinese General Social Survey | Social trust is linked to a higher risk perception and a lower infection rate, and generalized trust is the opposite |
| Zajenkowski et al., 2020 [78] | Poland | 263 adults (27.8% M, 71.5% F, 0.8% other) | Cross-sectional online survey collected in April | Situational Eight Diamonds Scale (40 items) with seven-point scale answers | Grave situations (like the coronavirus pandemic) leave less room for personality traits in predicting behaviors because they overpower dispositional tendencies |
| Marinthe et al., 2020 [79] | France | Two samples (N1 = 762 and N2 = 229) | Two cross-sectional online questionnaires. The first was conducted in early March and the second in later March | Perceived risk of contamination of the French population, personal contamination, and death were measured by single items (percentage) | Conspiracy was associated with a higher perceived COVID-19 risk of death but not with other risks |
| Monzani et al., 2021 [80] | Italy | 414 adults (70.3% F, 29.7% M). | Cross-sectional online questionnaire completed by participants between March and April | 0–100 slider scale answers to 8 items | People presenting more dispositional optimism indicated elevated levels of optimistic bias |
| Puci et al., 2020 [81] | Italy | 2078 HCW (78.8% F, 21.2% M) | Cross-sectional online survey developed from May to June | Five-point scale answers to 7 items | The majority presented high risk infection perceptions (especially nurses and physicians) |
| Ferdous et al., 2020 [82] | Bangladesh | 2017 residents (59.8% M, 40.2% F) | Cross-sectional online survey conducted between March and April | Closed-ended questions to 4 items | Participants showed a high COVID-19 risk perception and high partaking in safety behaviors |
| Serwaa et al., 2020 [83] | Ghana | 350 adults (56% M, 44% F) | Cross-sectional online questionnaire collected in March | 3 closed-ended questions | Participants had a good COVID-19 knowledge and high risk awareness |
| Samadipour et al., 2020 [84] | Iran | 364 adults (154 M, 201 F, and 9 did not answer) | Cross-sectional online survey conducted between February and March | Five-point Likert scale answers to 26 items | Iranians have a moderate risk perception of COVID-19. Five factors contribute to it: cultural, political, emotional, cognitive, and social |
| Shiina et al., 2020 [85] | UK, Spain, and Japan | 4000 people from Japan, 2000 from the UK, and 2000 from Spain | Cross-sectional online survey. Data were gathered between March and April | Nine-point scale type of answers | Knowledge, anxiety, and the frequency of precautionary behaviors was higher in the UK and Spain than in Japan |
| Soiné et al., 2021 [86] | Germany | Young adults (24–26 y) that belong to different ethnic groups | Data from the CILS4COVID survey were used | 2 closed-ended questions comparing financial and health risk perceptions | Ethnic minorities show more health and financial risk perceptions than the general population |
References
- Archived: WHO Timeline—COVID-19. Available online: https://www.who.int/news/item/27-04-2020-who-timeline—COVID-19 (accessed on 24 March 2022).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Taquet, M.; Luciano, S.; Geddes, J.R.; Harrison, P.J. Bidirectional associations between COVID-19 and psychiatric disorder: Retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry 2021, 8, 130–140. [Google Scholar] [CrossRef]
- Diamond, R.; Byrd, E. Standing up for health—Improving mental wellbeing during COVID-19 isolation by reducing sedentary behaviour. J. Affect. Disord. 2020, 277, 232–234. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.J.; Wessely, S. The psychological effects of quarantining a city. BMJ 2021, 368, m313. [Google Scholar] [CrossRef]
- Harper, C.A.; Satchell, L.P.; Fido, D.; Latzman, R.D. Functional Fear Predicts Public Health Compliance in the COVID-19 Pandemic. Int. J. Ment. Health Addict. 2020, 19, 1875–1888. [Google Scholar] [CrossRef]
- Germani, A.; Buratta, L.; Delvecchio, E.; Gizzi, G.; Mazzeschi, C. Anxiety Severity, Perceived Risk of COVID-19 and Individual Functioning in Emerging Adults Facing the Pandemic. Front. Psychol. 2020, 11, 567505. [Google Scholar] [CrossRef]
- Yıldırım, M.; Güler, A. Positivity explains how COVID-19 perceived risk increases death distress and reduces happiness. Personal. Individ. Differ. 2021, 168, 110347. [Google Scholar] [CrossRef]
- Faasse, K.; Newby, J.M. Public Perceptions of COVID-19 in Australia: Perceived Risk, Knowledge, Health-Protective Behaviors, and Vaccine Intentions. Front. Psychol. 2020, 11, 551004. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; for the PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Pearson, A.; White, H.; Bath-Hextall, F.; Salmond, S.; Apostolo, J.; Kirkpatrick, P. A mixed-methods approach to systematic reviews. JBI Evid. Implement. 2015, 13, 121–131. [Google Scholar] [CrossRef]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic reviews of etiology and risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; Joanna Briggs Institute: Adelaide, Australia, 2020; Available online: https://synthesismanual.jbi.global (accessed on 24 March 2022).
- Wise, T.; Zbozinek, T.D.; Michelini, G.; Hagan, C.C.; Mobbs, D. Changes in risk perception and self-reported protective behaviour during the first week of the COVID-19 pandemic in the United States. R. Soc. Open Sci. 2020, 7, 200742. [Google Scholar] [CrossRef] [PubMed]
- Lohiniva, A.-L.; Sane, J.; Sibenberg, K.; Puumalainen, T.; Salminen, M. Understanding coronavirus disease (COVID-19) risk perceptions among the public to enhance risk communication efforts: A practical approach for outbreaks, Finland, February 2020. Eurosurveillance 2020, 25, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Kuang, J.; Ashraf, S.; Das, U.; Bicchieri, C. Awareness, Risk Perception, and Stress during the COVID-19 Pandemic in Communities of Tamil Nadu, India. Int. J. Environ. Res. Public Health 2020, 17, 7177. [Google Scholar] [CrossRef] [PubMed]
- Moyce, S.; Velazquez, M.; Claudio, D.; Thompson, S.; Metcalf, M.; Aghbashian, E.; Vanderwood, K.; Sisson, N. Exploring a rural Latino community’s perception of the COVID-19 pandemic. Ethn. Health 2021, 26, 126–138. [Google Scholar] [CrossRef]
- Casanova, M.; Bagliacca, E.; Silva, M.; Patriarca, C.; Veneroni, L.; Clerici, C.A.; Spreafico, F.; Luksch, R.; Terenziani, M.; Meazza, C.; et al. How young patients with cancer perceive the COVID-19 (coronavirus) epidemic in Milan, Italy: Is there room for other fears? Pediatric Blood Cancer 2020, 67, e28318. [Google Scholar] [CrossRef]
- Ilesanmi, O.; Afolabi, A. Perception and practices during the COVID-19 pandemic in an urban community in Nigeria: A cross-sectional study. PeerJ 2020, 8, e10038. [Google Scholar] [CrossRef]
- Mouchtouri, V.A.; Agathagelidou, E.; Kofonikolas, K.; Rousou, X.; Dadouli, K.; Pinaka, O.; Agathocleous, E.; Anagnostopoulou, L.; Chatziligou, C.; Christoforidou, E.P.; et al. Nationwide Survey in Greece about Knowledge, Risk Perceptions, and Preventive Behaviors for COVID-19 during the General Lockdown in April 2020. Int. J. Environ. Res. Public Health 2020, 17, 8854. [Google Scholar] [CrossRef]
- Asefa, A.; Qanche, Q.; Hailemariam, S.; Dhuguma, T.; Nigussie, T. Risk Perception Towards COVID-19 and Its Associated Factors Among Waiters in Selected Towns of Southwest Ethiopia. Risk Manag. Healthc. Policy 2020, 13, 2601–2610. [Google Scholar] [CrossRef]
- de Bruin, W.B.; Bennett, D. Relationships Between Initial COVID-19 Risk Perceptions and Protective Health Behaviors: A National Survey. Am. J. Prev. Med. 2020, 59, 157–167. [Google Scholar] [CrossRef]
- Duan, W.; Bu, H.; Chen, Z. COVID-19-related stigma profiles and risk factors among people who are at high risk of contagion. Soc. Sci. Med. 2020, 266, 113425. [Google Scholar] [CrossRef]
- Lee, J.; Allen, J.; Lim, H.; Choi, G. Determinants of Behavioral Changes Since COVID-19 among Middle School Students. Healthcare 2021, 9, 75. [Google Scholar] [CrossRef] [PubMed]
- Rivas, D.R.Z.; Jaldin, M.L.L.; Canaviri, B.N.; Escalante, L.F.P.; Fernández, A.M.C.A.; Ticona, J.P.A. Social media exposure, risk perception, preventive behaviors and attitudes during the COVID-19 epidemic in La Paz, Bolivia: A cross sectional study. PLoS ONE 2021, 16, e0245859. [Google Scholar] [CrossRef]
- Savadori, L.; Lauriola, M. Risk Perception and Protective Behaviors During the Rise of the COVID-19 Outbreak in Italy. Front. Psychol. 2020, 11, 577331. [Google Scholar] [CrossRef]
- Xie, K.; Liang, B.; Dulebenets, M.A.; Mei, Y. The Impact of Risk Perception on Social Distancing during the COVID-19 Pandemic in China. Int. J. Environ. Res. Public Health 2020, 17, 6256. [Google Scholar] [CrossRef] [PubMed]
- Zanin, G.M.; Gentile, E.; Parisi, A.; Spasiano, D. A Preliminary Evaluation of the Public Risk Perception Related to the COVID-19 Health Emergency in Italy. Int. J. Environ. Res. Public Health 2020, 17, 3024. [Google Scholar] [CrossRef] [PubMed]
- Park, T.; Ju, I.; Ohs, J.E.; Hinsley, A. Optimistic bias and preventive behavioral engagement in the context of COVID-19. Res. Soc. Adm. Pharm. RSAP 2021, 17, 1859–1866. [Google Scholar] [CrossRef]
- Ahmad, M.; Iram, K.; Jabeen, G. Perception-based influence factors of intention to adopt COVID-19 epidemic prevention in China. Environ. Res. 2020, 190, 109995. [Google Scholar] [CrossRef]
- Atchison, C.; Bowman, L.R.; Vrinten, C.; Redd, R.; Pristerà, P.; Eaton, J.; Ward, H. Early perceptions and behavioural responses during the COVID-19 pandemic: A cross-sectional survey of UK adults. BMJ Open 2021, 11, e043577. [Google Scholar] [CrossRef]
- Tomczyk, S.; Rahn, M.; Schmidt, S. Social Distancing and Stigma: Association Between Compliance with Behavioral Recommendations, Risk Perception, and Stigmatizing Attitudes During the COVID-19 Outbreak. Front. Psychol. 2020, 11, 1821. [Google Scholar] [CrossRef]
- McFadden, S.M.; Malik, A.A.; Aguolu, O.G.; Willebrand, K.S.; Omer, S.B. Perceptions of the adult US population regarding the novel coronavirus outbreak. PLoS ONE 2020, 15, e0231808. [Google Scholar] [CrossRef]
- Taghrir, M.H.; Borazjani, R.; Shiraly, R. COVID-19 and Iranian Medical Students; A Survey on Their Related-Knowledge, Preventive Behaviors and Risk Perception. Arch. Iran. Med. 2020, 23, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Mansilla Dominguez, J.M.; Font Jimenez, I.; Belzunegui Eraso, A.; Pena Otero, D.; Diaz Perez, D.; Vivas, A.M. Risk Perception of COVID-19 Community Transmission among the Spanish Population. Int. J. Environ. Res. Public Health 2020, 17, 8967. [Google Scholar] [CrossRef] [PubMed]
- Mora-Rodríguez, A.; Melero-López, I. News Consumption and Risk Perception of COVID-19 in Spain. Comun. Media Educ. Res. J. 2021, 29, 67–77. [Google Scholar] [CrossRef]
- Roupa, Z.; Polychronis, G.; Latzourakis, E.; Nikitara, M.; Ghobrial, S.; Chrysafi, A.; Noula, M. Assessment of Knowledge and Perceptions of Health Workers Regarding COVID-19: A Cross-Sectional Study from Cyprus. J. Community Health 2021, 46, 251–258. [Google Scholar] [CrossRef]
- Iorfa, S.K.; Ottu, I.F.A.; Oguntayo, R.; Ayandele, O.; Kolawole, S.O.; Gandi, J.C.; Dangiwa, A.L.; Olapegba, P.O. COVID-19 Knowledge, Risk Perception, and Precautionary Behavior Among Nigerians: A Moderated Mediation Approach. Front. Psychol. 2020, 11, 566773. [Google Scholar] [CrossRef]
- Lanciano, T.; Graziano, G.; Curci, A.; Costadura, S.; Monaco, A. Risk Perceptions and Psychological Effects During the Italian COVID-19 Emergency. Front. Psychol. 2020, 11, 580053. [Google Scholar] [CrossRef]
- Ciancio, A.; Kampfen, F.; Kohler, I.; Bennett, D.; de Bruin, W.B.; Darling, J.; Kapteyn, A.; Maurer, J.; Kohler, H.-P. Know your epidemic, know your response: Early perceptions of COVID-19 and self-reported social distancing in the United States. PLoS ONE 2020, 15, e0238341. [Google Scholar] [CrossRef]
- Germani, A.; Buratta, L.; Delvecchio, E.; Mazzeschi, C. Emerging Adults and COVID-19: The Role of Individualism-Collectivism on Perceived Risks and Psychological Maladjustment. Int. J. Environ. Res. Public Health 2020, 17, 3497. [Google Scholar] [CrossRef]
- Ding, Y.; Du, X.; Li, Q.; Zhang, M.; Zhang, Q.; Tan, X.; Liu, Q. Risk perception of coronavirus disease 2019 (COVID-19) and its related factors among college students in China during quarantine. PLoS ONE 2020, 15, e0237626. [Google Scholar] [CrossRef]
- Yang, X.Y.; Gong, R.N.; Sassine, S.; Morsa, M.; Tchogna, A.S.; Drouin, O.; Chadi, N.; Jantchou, P. Risk Perception of COVID-19 Infection and Adherence to Preventive Measures among Adolescents and Young Adults. Children 2020, 7, 311. [Google Scholar] [CrossRef]
- Kabito, G.G.; Alemayehu, M.; Mekonnen, T.H.; Wami, S.D.; Azanaw, J.; Adane, T.; Azene, Z.N.; Merid, M.W.; Muluneh, A.G.; Geberu, D.M.; et al. Community’s perceived high risk of coronavirus infections during early phase of epidemics are significantly influenced by socio-demographic background, in Gondar City, Northwest Ethiopia: A cross-sectional-study. PLoS ONE 2020, 15, e0242654. [Google Scholar] [CrossRef] [PubMed]
- Harapan, H.; Anwar, S.; Nainu, F.; Setiawan, A.M.; Yufika, A.; Winardi, W.; Gan, A.K.; Sofyan, H.; Mudatsir, M.; Oktari, R.S.; et al. Perceived Risk of Being Infected With SARS-CoV-2: A Perspective from Indonesia. Disaster Med. Public Health Prep. 2020, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; van der Bles, A.M.; Spiegelhalter, D.; van der Linden, S. Risk perceptions of COVID-19 around the world. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Jahangiry, L.; Bakhtari, F.; Sohrabi, Z.; Reihani, P.; Samei, S.; Ponnet, K.; Montazeri, A. Risk perception related to COVID-19 among the Iranian general population: An application of the extended parallel process model. Bmc Public Health 2020, 20, 1571. [Google Scholar] [CrossRef] [PubMed]
- Abir, T.; Kalimullah, N.A.; Osuagwu, U.L.; Yazdani, D.M.N.-A.; Al Mamun, A.; Husain, T.; Basak, P.; Permarupan, P.Y.; Agho, K.E. Factors Associated with the Perception of Risk and Knowledge of Contracting the SARS-CoV-2 among Adults in Bangladesh: Analysis of Online Surveys. Int. J. Environ. Res. Public Health 2020, 17, 5252. [Google Scholar] [CrossRef]
- Karasneh, R.; Al-Azzam, S.; Muflih, S.; Soudah, O.; Hawamdeh, S.; Khader, Y. Media’s effect on shaping knowledge, awareness risk perceptions and communication practices of pandemic COVID-19 among pharmacists. Res. Soc. Adm. Pharm. 2021, 17, 1897–1902. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef]
- Karout, L.; Serwat, A.; El Mais, H.; Kassab, M.; Khalid, F.; Mercedes, B.R. COVID-19 Prevalence, Risk Perceptions, and Preventive Behavior in Asymptomatic Latino Population: A Cross-Sectional Study. Cureus 2020, 12, e10707. [Google Scholar] [CrossRef]
- Chou, W.-P.; Wang, P.-W.; Chen, S.-L.; Chang, Y.-P.; Wu, C.-F.; Lu, W.-H.; Yen, C.-F. Risk Perception, Protective Behaviors, and General Anxiety during the Coronavirus Disease 2019 Pandemic among Affiliated Health Care Professionals in Taiwan: Comparisons with Frontline Health Care Professionals and the General Public. Int. J. Environ. Res. Public Health 2020, 17, 9329. [Google Scholar] [CrossRef]
- Peres, D.; Monteiro, J.; Almeida, M.A.; Ladeira, R. Risk perception of COVID-19 among Portuguese healthcare professionals and the general population. J. Hosp. Infect. 2020, 105, 434–437. [Google Scholar] [CrossRef]
- Gorini, A.; Fiabane, E.; Sommaruga, M.; Barbieri, S.; Sottotetti, F.; La Rovere, M.T.; Tremoli, E.; Gabanelli, P. Mental health and risk perception among Italian healthcare workers during the second month of the COVID-19 pandemic. Arch. Psychiatr. Nurs. 2020, 34, 537–544. [Google Scholar] [CrossRef] [PubMed]
- González-Gil, M.T.; González-Blázquez, C.; Parro-Moreno, A.I.; Pedraz-Marcos, A.; Palmar-Santos, A.; Otero-García, L.; Navarta-Sánchez, M.V.; Alcolea-Cosín, M.T.; Argüello-López, M.T.; Canalejas-Pérez, C.; et al. Nurses’ perceptions and demands regarding COVID-19 care delivery in critical care units and hospital emergency services. Intensive Crit. Care Nurs. 2021, 62, 102966. [Google Scholar] [CrossRef] [PubMed]
- Niepel, C.; Kranz, D.; Borgonovi, F.; Emslander, V.; Greiff, S. The coronavirus (COVID-19) fatality risk perception of US adult residents in March and April 2020. Br. J. Health Psychol. 2020, 25, 883–888. [Google Scholar] [CrossRef] [PubMed]
- Tran, V.-T.; Ravaud, P. COVID-19-related perceptions, context and attitudes of adults with chronic conditions: Results from a cross-sectional survey nested in the ComPaRe e-cohort. PLoS ONE 2020, 15, e0237296. [Google Scholar] [CrossRef]
- Heydari, S.T.; Zarei, L.; Sadati, A.K.; Moradi, N.; Akbari, M.; Mehralian, G.; Lankarani, K.B. The effect of risk communication on preventive and protective Behaviours during the COVID-19 outbreak: Mediating role of risk perception. BMC Public Health 2021, 21, 54. [Google Scholar] [CrossRef]
- Seale, H.; Heywood, A.E.; Leask, J.; Sheel, M.; Thomas, S.; Durrheim, D.N.; Bolsewicz, K.; Kaur, R. COVID-19 is rapidly changing: Examining public perceptions and behaviors in response to this evolving pandemic. PLoS ONE 2020, 15, e0235112. [Google Scholar] [CrossRef]
- Vai, B.; Cazzetta, S.; Ghiglino, D.; Parenti, L.; Saibene, G.; Toti, M.; Verga, C.; Wykowska, A.; Benedetti, F. Risk Perception and Media in Shaping Protective Behaviors: Insights from the Early Phase of COVID-19 Italian Outbreak. Front. Psychol. 2020, 11, 3426. [Google Scholar] [CrossRef]
- Nazione, S.; Perrault, E.; Pace, K. Impact of Information Exposure on Perceived Risk, Efficacy, and Preventative Behaviors at the Beginning of the COVID-19 Pandemic in the United States. Health Commun. 2021, 36, 23–31. [Google Scholar] [CrossRef]
- Capone, V.; Caso, D.; Donizzetti, A.R.; Procentese, F. University Student Mental Well-Being during COVID-19 Outbreak: What Are the Relationships between Information Seeking, Perceived Risk and Personal Resources Related to the Academic Context? Sustainability 2020, 12, 7039. [Google Scholar] [CrossRef]
- Huang, Y.; Yang, C. A Metacognitive Approach to Reconsidering Risk Perceptions and Uncertainty: Understand Information Seeking During COVID-19. Sci. Commun. 2020, 42, 616–642. [Google Scholar] [CrossRef]
- Jiang, R. Knowledge, attitudes and mental health of university students during the COVID-19 pandemic in China. Child. Youth Serv. Rev. 2020, 119, 105494. [Google Scholar] [CrossRef] [PubMed]
- Soni, R.; Riyal, S.; Tomar, M. Concern, perceived risk and attitudes of the general public towards COVID-19: Special reference to Delhi-NCR. J. Stat. Manag. Syst. 2021, 24, 229–249. [Google Scholar] [CrossRef]
- Geldsetzer, P. Use of Rapid Online Surveys to Assess People’s Perceptions During Infectious Disease Outbreaks: A Cross-sectional Survey on COVID-19. J. Med. Internet Res. 2020, 22, e18790. [Google Scholar] [CrossRef]
- Gollust, S.E.; Vogel, R.I.; Rothman, A.; Yzer, M.; Fowler, E.F.; Nagler, R.H. Americans’ perceptions of disparities in COVID-19 mortality: Results from a nationally-representative survey. Prev. Med. 2020, 141, 106278. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Xu, J.; Huang, S.; Li, P.; Lu, C.; Xie, S. Risk Perception and Depression in Public Health Crises: Evidence from the COVID-19 Crisis in China. Int. J. Environ. Res. Public Health 2020, 17, 5728. [Google Scholar] [CrossRef] [PubMed]
- Krok, D.; Zarzycka, B. Risk Perception of COVID-19, Meaning-Based Resources and Psychological Well-Being amongst Healthcare Personnel: The Mediating Role of Coping. J. Clin. Med. 2020, 9, 3225. [Google Scholar] [CrossRef]
- Liu, M.; Zhang, H.; Huang, H. Media exposure to COVID-19 information, risk perception, social and geographical proximity, and self-rated anxiety in China. Bmc Public Health 2020, 20, 1649. [Google Scholar] [CrossRef]
- Orte, C.; Sanchez-Prieto, L.; Dominguez, D.C.; Barrientos-Baez, A. Evaluation of Distress and Risk Perception Associated with COVID-19 in Vulnerable Groups. Int. J. Environ. Res. Public Health 2020, 17, 9207. [Google Scholar] [CrossRef]
- Qian, D.; Li, O. The Relationship between Risk Event Involvement and Risk Perception during the COVID-19 Outbreak in China. Appl. Psychol.-Health Well Being 2020, 12, 983–999. [Google Scholar] [CrossRef]
- Spinelli, M.; Lionetti, F.; Pastore, M.; Fasolo, M. Parents’ Stress and Children’s Psychological Problems in Families Facing the COVID-19 Outbreak in Italy. Front. Psychol. 2020, 11, 1713. [Google Scholar] [CrossRef]
- Li, D.-J.; Ko, N.-Y.; Chang, Y.-P.; Yen, C.-F.; Chen, Y.-L. Mediating Effects of Risk Perception on Association between Social Support and Coping with COVID-19: An Online Survey. Int. J. Environ. Res. Public Health 2021, 18, 1550. [Google Scholar] [CrossRef]
- de Bruin, W.B.; Saw, H.-W.; Goldman, D.P. Political polarization in US residents’ COVID-19 risk perceptions, policy preferences, and protective behaviors. J. Risk Uncertain. 2020, 61, 177–194. [Google Scholar] [CrossRef]
- Lachlan, K.A.; Hutter, E.; Gilbert, C. COVID-19 Echo Chambers: Examining the Impact of Conservative and Liberal News Sources on Risk Perception and Response. Health Secur. 2021, 19, 21–30. [Google Scholar] [CrossRef]
- Siegrist, M.; Luchsinger, L.; Bearth, A. The Impact of Trust and Risk Perception on the Acceptance of Measures to Reduce COVID-19 Cases. Risk Anal. 2021, 41, 787–800. [Google Scholar] [CrossRef]
- Ye, M.; Lyu, Z. Trust, risk perception, and COVID-19 infections: Evidence from multilevel analyses of combined original dataset in China. Soc. Sci. Med. 2020, 265, 113517. [Google Scholar] [CrossRef]
- Zajenkowski, M.; Jonason, P.K.; Leniarska, M.; Kozakiewicz, Z. Who complies with the restrictions to reduce the spread of COVID-19?: Personality and perceptions of the COVID-19 situation. Personal. Individ. Differ. 2020, 166, 110199. [Google Scholar] [CrossRef]
- Marinthe, G.; Brown, G.; Delouvee, S.; Jolley, D. Looking out for myself: Exploring the relationship between conspiracy mentality, perceived personal risk, and COVID-19 prevention measures. Br. J. Health Psychol. 2020, 25, 957–980. [Google Scholar] [CrossRef]
- Monzani, D.; Gorini, A.; Mazzoni, D.; Pravettoni, G. Brief report—“Every little thing gonna be all right” (at least for me): Dispositional optimists display higher optimistic bias for infection during the Italian COVID-19 outbreak. Personal. Individ. Differ. 2021, 168, 110388. [Google Scholar] [CrossRef]
- Puci, M.V.; Nosari, G.; Loi, F.; Puci, G.V.; Montomoli, C.; Ferraro, O.E. Risk Perception and Worries among Health Care Workers in the COVID-19 Pandemic: Findings from an Italian Survey. Healthcare 2020, 8, 535. [Google Scholar] [CrossRef]
- Ferdous, M.Z.; Islam, M.S.; Sikder, M.T.; Mosaddek, A.S.M.; Zegarra-Valdivia, J.A.; Gozal, D. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: An online-based cross-sectional study. PLoS ONE 2020, 15, e0239254. [Google Scholar] [CrossRef]
- Serwaa, D.; Lamptey, E.; Appiah, A.B.; Senkyire, E.K.; Ameyaw, J.K. Knowledge, risk perception and preparedness towards coronavirus disease-2019 (COVID-19) outbreak among Ghanaians: A quick online cross-sectional survey. Pan Afr. Med. J. 2020, 35, 44. [Google Scholar] [CrossRef] [PubMed]
- Samadipour, E.; Ghardashi, F.; Aghaei, N. Evaluation of Risk Perception of COVID-19 Disease: A Community-Based Participatory Study. Disaster Med. Public Health Prep. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shiina, A.; Niitsu, T.; Kobori, O.; Idemoto, K.; Hashimoto, T.; Sasaki, T.; Igarashi, Y.; Shimizu, E.; Nakazato, M.; Hashimoto, K.; et al. Relationship between perception and anxiety about COVID-19 infection and risk behaviors for spreading infection: A national survey in Japan. Brain Behav. Immun. Health 2020, 6, 100101. [Google Scholar] [CrossRef]
- Soine, H.; Kriegel, L.; Dollmann, J. The impact of the COVID-19 pandemic on risk perceptions: Differences between ethnic groups in Germany. Eur. Soc. 2021, 23, S289–S306. [Google Scholar] [CrossRef]
- Luszczynska, A.; Szczuka, Z.; Abraham, C.; Baban, A.; Brooks, S.; Cipolletta, S.; Wolf, H. The interplay between strictness of policies and individuals’ self-regulatory efforts: Associations with handwashing during the COVID-19 pandemic. Ann. Behav. Med. 2022, 56, 368–380. [Google Scholar] [CrossRef]
- Schwarzer, R. Modeling Health Behavior Change: How to Predict and Modify the Adoption and Maintenance of Health Behaviors. Appl. Psychol. Int. Rev. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Hagger, M.S.; Smith, S.R.; Keech, J.J.; Moyers, S.A.; Hamilton, K. Predicting social distancing intention and behavior during the COVID-19 pandemic: An integrated social cognition model. Ann. Behav. Med. 2020, 54, 713–727. [Google Scholar] [CrossRef]
- Nerini, A.; Matera, C.; Policardo, G.R.; Di Gesto, C. Containment measures against COVID-19 in Italy: The role of protection motivation and values. J. Hum. Behav. Soc. Environ. 2021. [Google Scholar] [CrossRef]
- Becker, M.H. The health belief model and personal health behavior. Health Educ. Monogr. 1974, 2, 324–473. [Google Scholar] [CrossRef]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Beck, U. Risk Society: Towards a New Modernity; Sage Publications: Thousand Oaks, CA, USA, 1992. [Google Scholar]
- Ajzen, I. Theory of reasoned action. In Encyclopedia of Psychology; Kazdin, A.E., Ed.; American Psychological Association: New York, NY, USA, 2000; Volume 8, pp. 61–63. [Google Scholar]
- Brashers, D.E. A Theory of Communication and Uncertainty Management. In Explaining Communication: Contemporary Theories and Exemplars; Whaley, B.B., Samter, W., Eds.; Lawrence Erlbaum Associates Publisher: Mahwah, NJ, USA, 2007; pp. 201–218. [Google Scholar]
- Merle, H. The Measurement of Uncertainty in Illness. Nurs. Res. 1981, 30, 258–263. [Google Scholar]
- Rogers, R.W. A protection motivation theory of fear appeals and attitude change. J. Psychol. Interdiscip. Appl. 1975, 91, 93–114. [Google Scholar] [CrossRef] [PubMed]
- Hobfoll, S.E. Conservation of resources: A new attempt at conceptualizing stress. Am. Psychol. 1989, 44, 513–524. [Google Scholar] [CrossRef]
- Stolle, D.; Rothstein, B. Political Institutions and Generalized Trust; Oxford University Press: Oxford, UK, 2008. [Google Scholar]
- McCrae, R.R.; Costa, P.T., Jr. The five-factor theory of personality. In Handbook of Personality: Theory and Research; John, O.P., Robins, R.W., Pervin, L.A., Eds.; The Guilford Press: New York, NY, USA, 2008; pp. 159–181. [Google Scholar]
- Paulhus, D.L.; Williams, K.M. The Dark Triad of personality: Narcissism, Machiavellianism, and psychopathy. J. Res. Personal. 2002, 36, 556–563. [Google Scholar] [CrossRef]
- Herbert, A. Administrative Behavior: A Study of Decision-Making Processes in Administrative Organization, 1st ed.; Macmillan: New York, NY, USA, 1947. [Google Scholar]
- Lindell, K.; Perry, W. The Protective Action Decision Model: Theoretical Modifications and Additional Evidence. Risk Anal. 2012, 32, 616–632. [Google Scholar] [CrossRef]
- Ferrer, R.A.; Klein, W.M.; Persoskie, A.; Avishai-Yitshak, A.; Sheeran, P. The Tripartite Model of Risk Perception (TRIRISK): Distinguishing Deliberative, Affective, and Experiential Components of Perceived Risk. Ann. Behav. Med. 2016, 50, 653–663. [Google Scholar] [CrossRef] [PubMed]
- Hofstede, G. Culture’s Consequences: Comparing Values, Behaviors, Institutions, and Organizations across Nations; Sage Publications: Thousand Oaks, CA, USA, 2001. [Google Scholar]
- van der Linden, S. The social-psychological determinants of climate change risk perceptions: Towards a comprehensive model. J. Environ. Psychol. 2015, 41, 112–124. [Google Scholar] [CrossRef]
- Witte, K. Putting the fear back into fear appeals: The extended parallel process model. Commun. Monogr. 1992, 59, 329–349. [Google Scholar] [CrossRef]
- Griffin, R.J.; Dunwoody, S.; Neuwirth, K. Proposed model of the relationship of risk information seeking and processing to the development of preventive behaviors. Env. Res. 1999, 80, S230–S245. [Google Scholar] [CrossRef] [PubMed]
- Tsoy, D.; Tirasawasdichai, T.; Kurpayanidi, K. Role of Social Media in Shaping Public Risk Perception during COVID-19 Pandemic: A Theoretical Review. Int. J. Manag. Sci. Bus. Adm. 2021, 7, 35–41. [Google Scholar] [CrossRef]
- Gao, J.; Zheng, P.; Jia, Y.; Chen, H.; Mao, Y.; Chen, S.; Wang, Y.; Fu, H.; Dai, J. Mental health problems and social media exposure during COVID-19 outbreak. PLoS ONE 2020, 15, e0231924. [Google Scholar] [CrossRef] [PubMed]
- Cipolletta, S.; Gris, F. Older People’s Lived Perspectives of Social Isolation during the First Wave of the COVID-19 Pandemic in Italy. Int. J. Environ. Res. Public Health 2021, 18, 11832. [Google Scholar] [CrossRef]
- Oh, S.H.; Lee, S.Y.; Han, C. The Effects of Social Media Use on Preventive Behaviors during Infectious Disease Outbreaks: The Mediating Role of Self-relevant Emotions and Public Risk Perception. Health Commun. 2021, 36, 972–981. [Google Scholar] [CrossRef] [PubMed]
- Shepperd, J.A.; Waters, E.A.; Weinstein, N.D.; Klein, W.M.P. A primer on unrealistic optimism. Curr. Direct. Psychol. Sci. 2015, 24, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Galić, M.; Mustapić, L.; Šimunić, A.; Sić, L.; Cipolletta, S. COVID-19 Related Knowledge and Mental Health: Case of Croatia. Front. Psychol. 2020, 11, 567368. [Google Scholar] [CrossRef]
- Lindner-Pawłowicz, K.; Mydlikowska-Śmigórska, A.; Łampika, K.; Sobieszczańska, M. COVID-19 Vaccination Acceptance among Healthcare Workers and General Population at the Very Beginning of the National Vaccination Program in Poland: A Cross-Sectional, Exploratory Study. Vaccines 2022, 10, 66. [Google Scholar] [CrossRef]
- Ellis, K.L. Britain is First in Europe to Hit 50,000 COVID Deaths; Health Editor. Rosa. Available online: https://www.thetimes.co.uk/article/coronavirus-britain-is-first-in-europe-to-hit-50-000-deaths-j0v2j35zq (accessed on 24 March 2022).
- A Timeline of COVID-19 Developments in 2020. Available online: https://www.ajmc.com/view/a-timeline-of-covid19-developments-in-2020 (accessed on 18 February 2021).
- Cipolletta, S.; Ortu, M.C. COVID-19: Common Constructions of the Pandemic and Their Implications. J. Constr. Psychol. 2021, 34, 278–294. [Google Scholar] [CrossRef]
- Milman, E.; Lee, S.A.; Neimeyer, R.A. Social isolation and the mitigation of coronavirus anxiety: The mediating role of meaning. Death Stud. 2020, 46, 1–13. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cipolletta, S.; Andreghetti, G.R.; Mioni, G. Risk Perception towards COVID-19: A Systematic Review and Qualitative Synthesis. Int. J. Environ. Res. Public Health 2022, 19, 4649. https://doi.org/10.3390/ijerph19084649
Cipolletta S, Andreghetti GR, Mioni G. Risk Perception towards COVID-19: A Systematic Review and Qualitative Synthesis. International Journal of Environmental Research and Public Health. 2022; 19(8):4649. https://doi.org/10.3390/ijerph19084649
Chicago/Turabian StyleCipolletta, Sabrina, Gabriela Rios Andreghetti, and Giovanna Mioni. 2022. "Risk Perception towards COVID-19: A Systematic Review and Qualitative Synthesis" International Journal of Environmental Research and Public Health 19, no. 8: 4649. https://doi.org/10.3390/ijerph19084649
APA StyleCipolletta, S., Andreghetti, G. R., & Mioni, G. (2022). Risk Perception towards COVID-19: A Systematic Review and Qualitative Synthesis. International Journal of Environmental Research and Public Health, 19(8), 4649. https://doi.org/10.3390/ijerph19084649