
Risk Assessment of Early Lung Cancer with LDCT and Health Examinations


Abstract
:1. Introduction
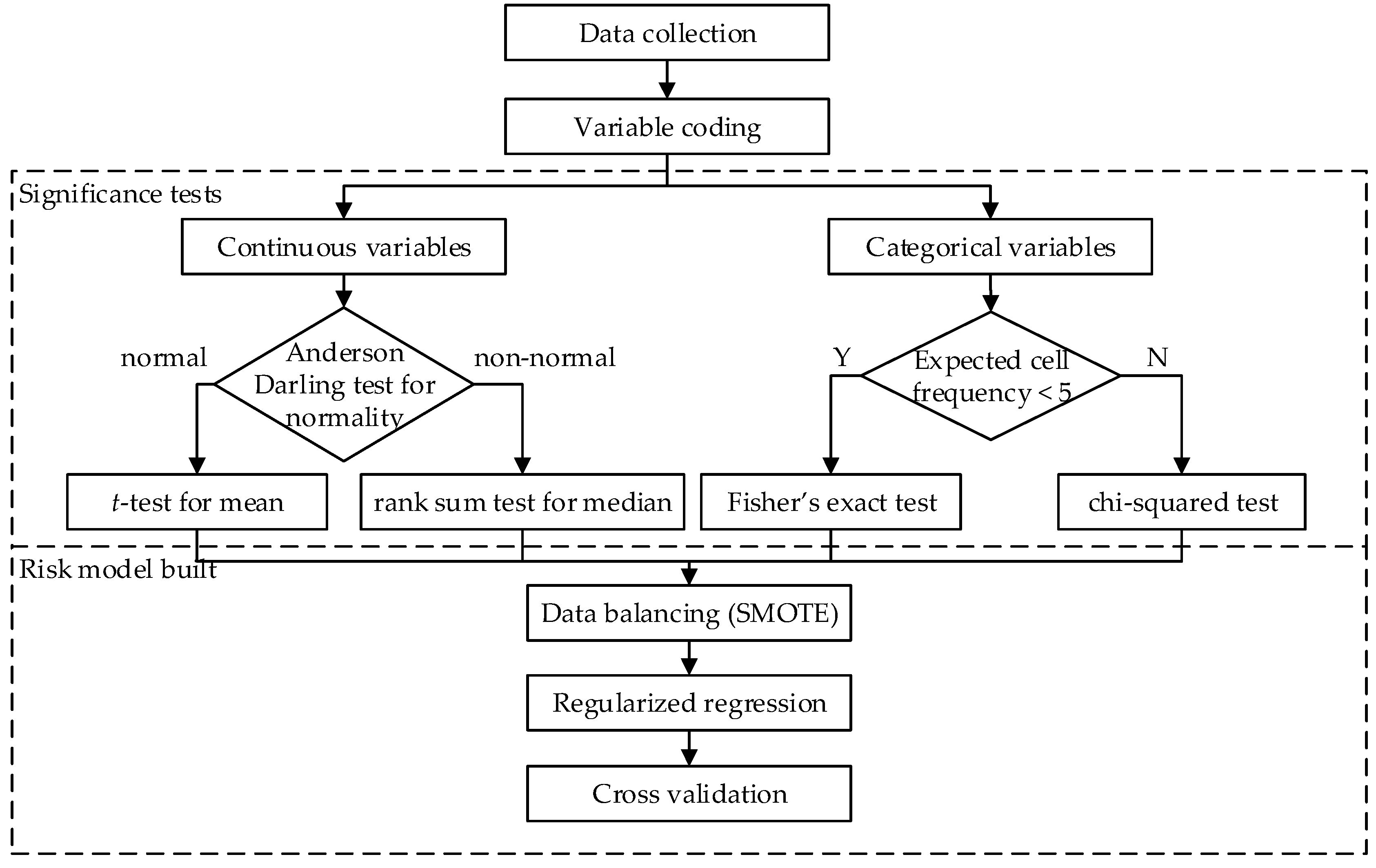
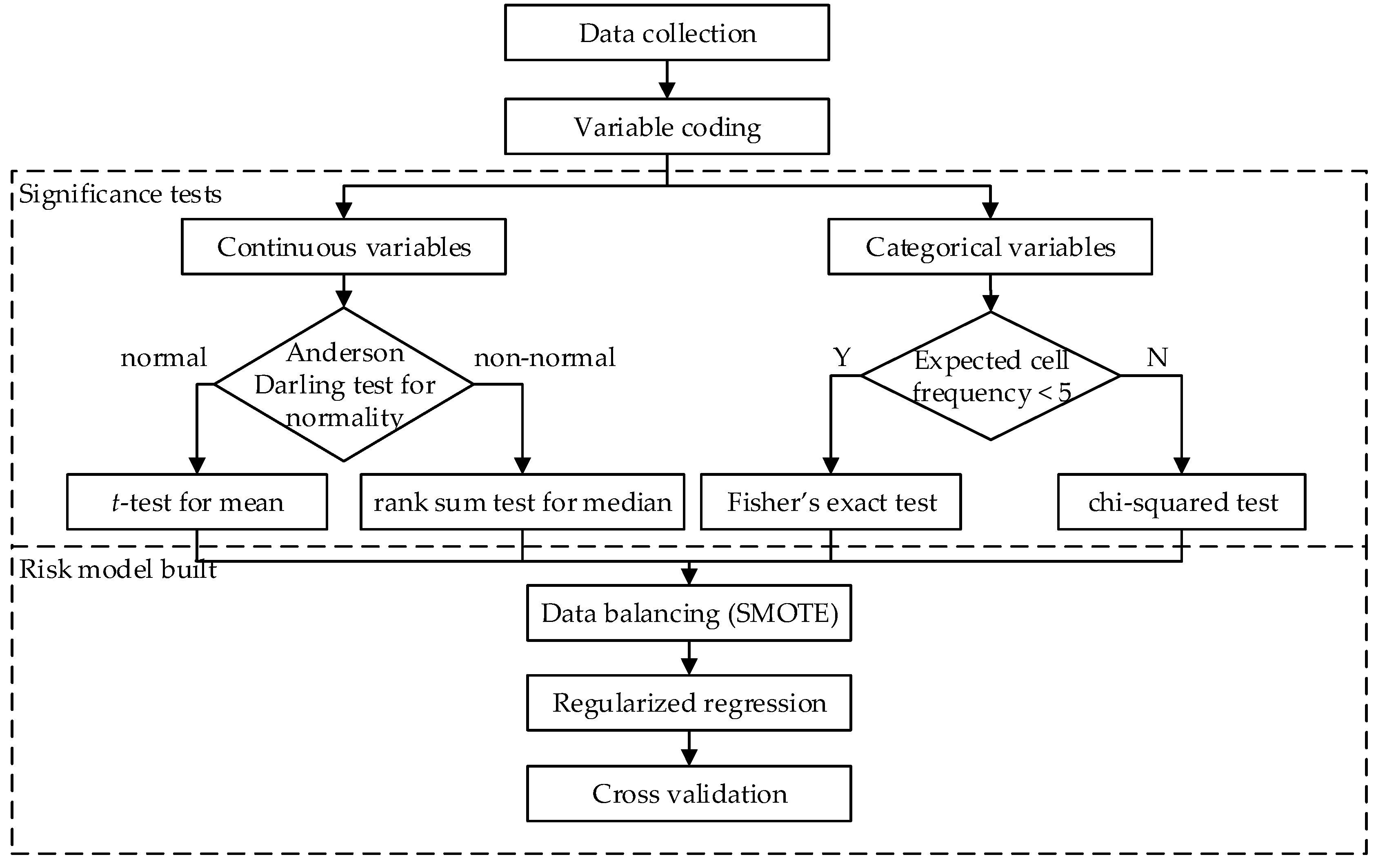
2. Materials and Methods
3. Results
3.1. Summary Statistics
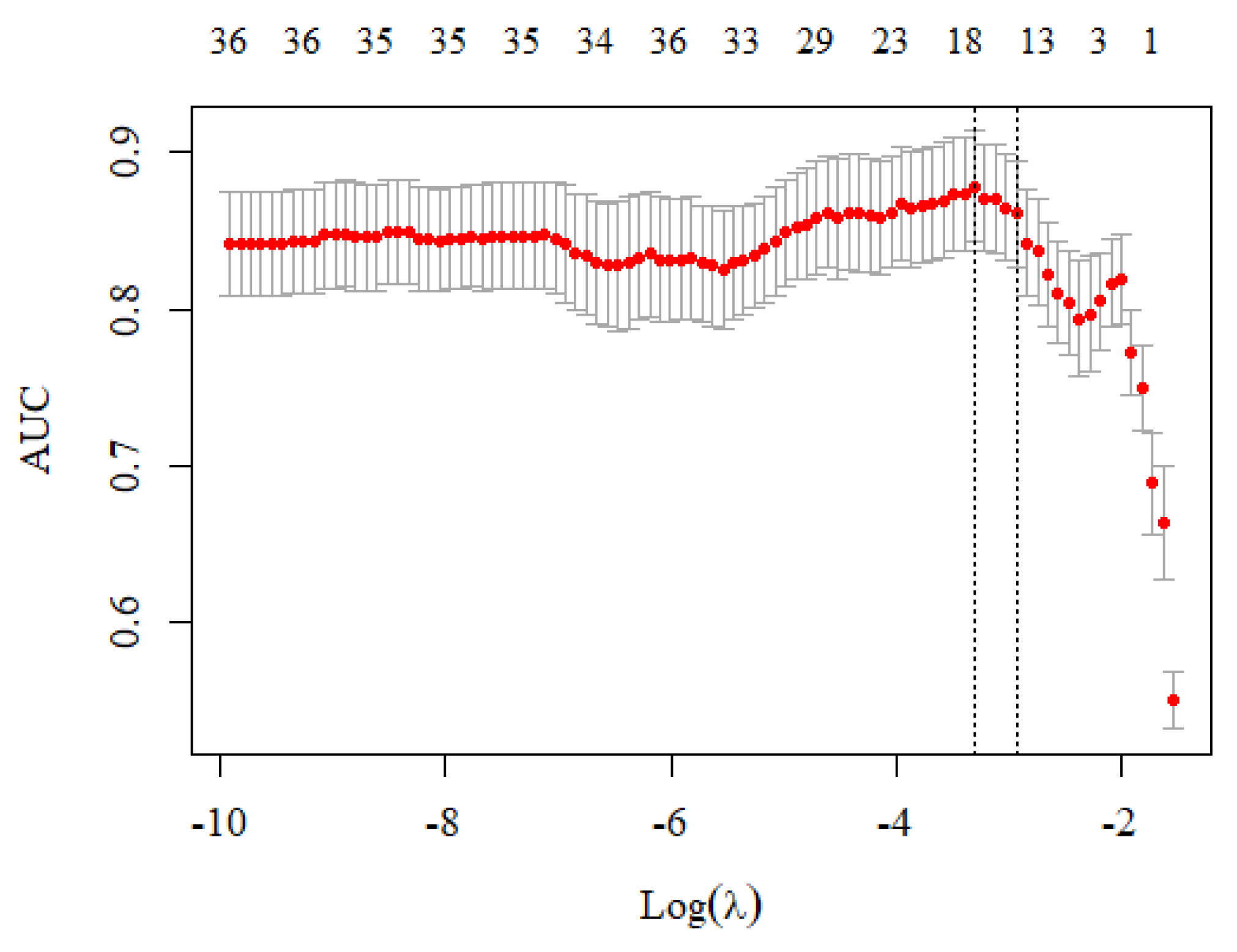
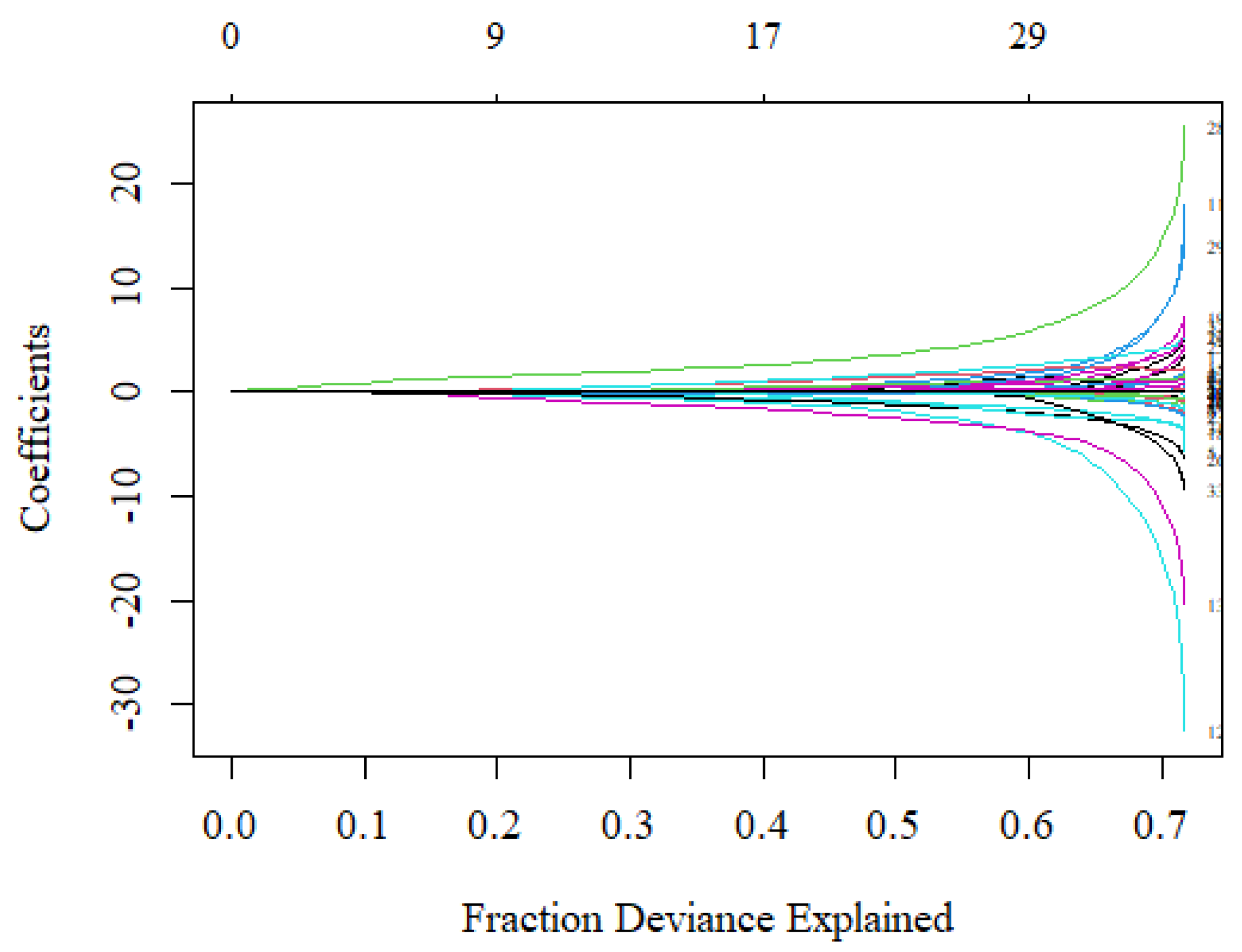
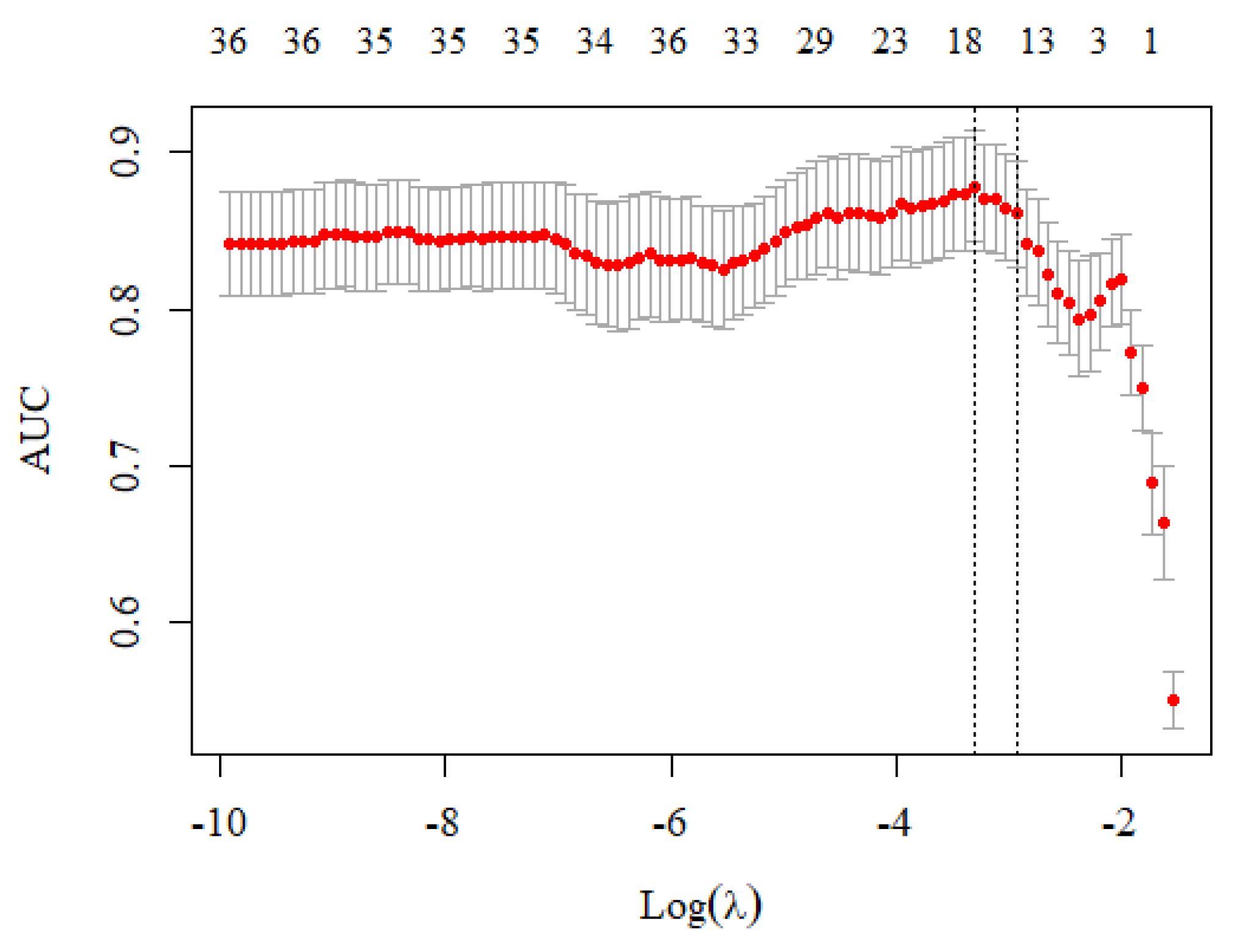
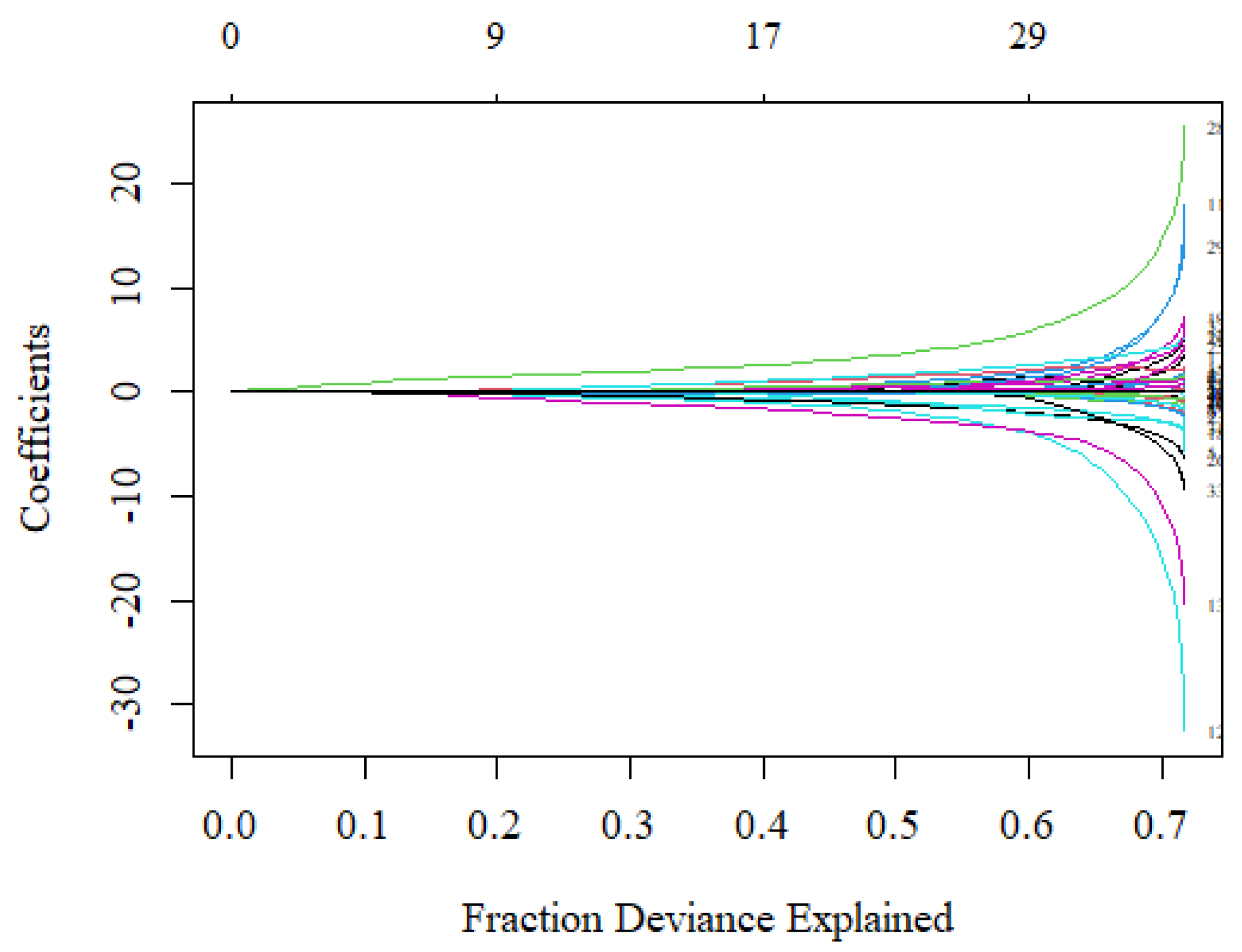
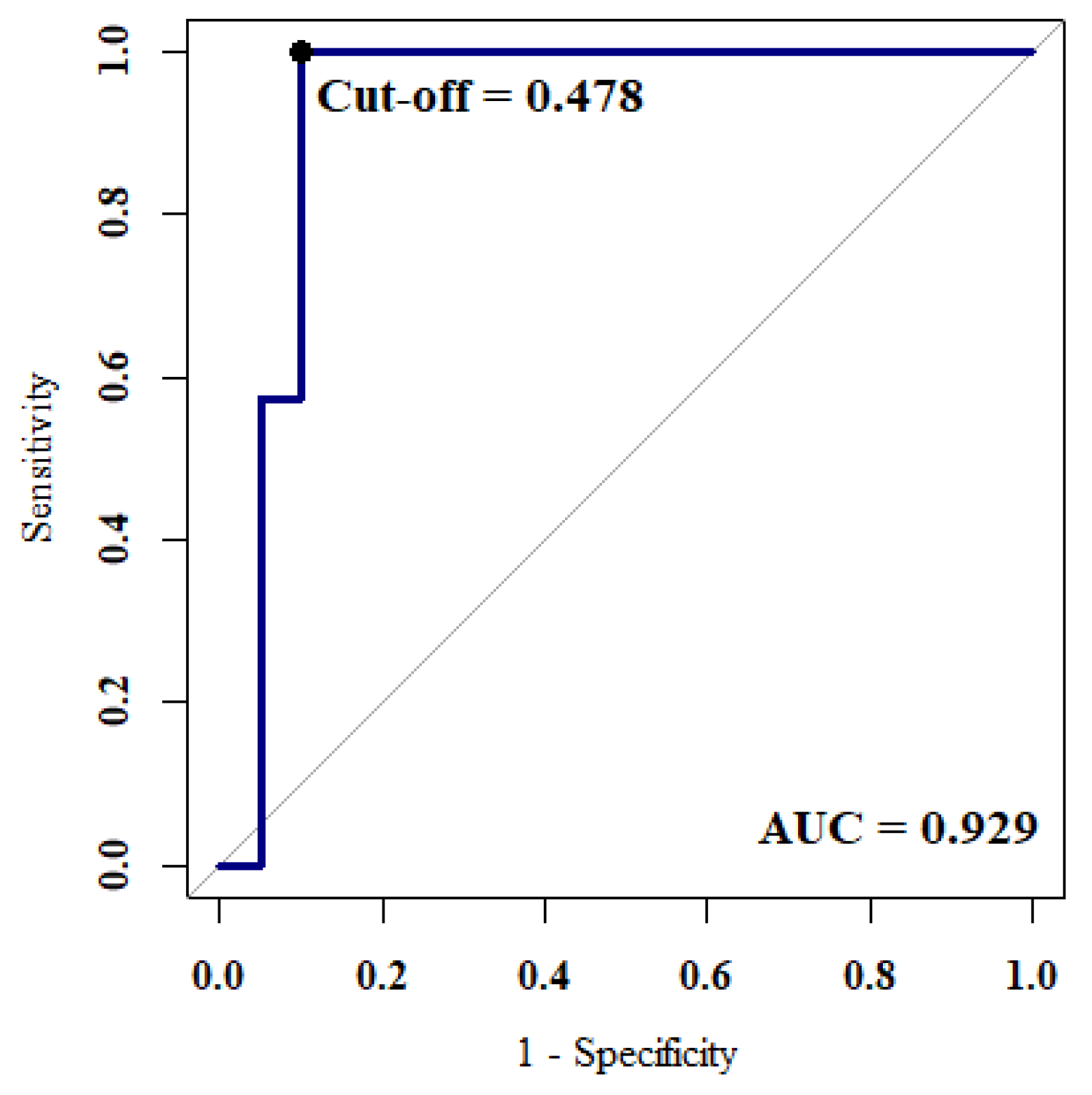
3.2. Model Evaluation
− 0.153 × Solid − 0.324 × Calcified − 0.802 × Middle + 0.997 × Diabetes
+ 0.383 × Gout + 0.321 × COPD + 0.249 × Other Cancer + 0.100 × WBC
+ 0.016 × BUN + 0.002 × Age − 0.717 × Thyroid − 1.118 × Liver
− 1.733 × Digestive System
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. SEER Cancer Statistics Review, 1975–2018. Available online: https://seer.cancer.gov/csr/1975_2018/results_merged/sect_01_overview.pdf (accessed on 2 April 2022).
- Del Ciello, A.; Franchi, P.; Contegiacomo, A.; Cicchetti, G.; Bonomo, L.; Larici, A.R. Missed lung cancer: When, where, and why? Diagn. Interv. Radiol. 2017, 23, 118–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, P.K.; Austin, J.H.; White, C.S.; Patel, P.; Haramati, L.B.; Pearson, G.D.; Shiau, M.C.; Berkmen, Y.M. Missed non–small cell lung cancer: Radiographic findings of potentially resectable lesions evident only in Retrospect. Radiology 2003, 226, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Tack, D.; Howarth, N. Missed lung lesions: Side by side comparison of chest radiography with MDCT. In Diseases of the Chest and Heart 2015–2018: Diagnostic Imaging and Interventional Techniques; Hodler, J., von Schulthess, G.K., Kubik-Huch, R.A., Zollikofer, C.L., Eds.; Springer: Milan, Italy, 2015; pp. 80–87. [Google Scholar]
- Blanchon, T.; Bréchot, J.M.; Grenier, P.A.; Ferretti, G.R.; Lemarié, E.; Milleron, B.; Chagué, D.; Laurent, F.; Martinet, Y.; Beigelman-Aubry, C.; et al. Baseline results of the Depiscan study: A French randomized pilot trial of lung cancer screening comparing low dose CT scan (LDCT) and chest X-ray (CXR). Lung Cancer 2007, 58, 50–58. [Google Scholar] [CrossRef] [PubMed]
- The National Lung Screening Trial Research Team. Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Koning, H.J.; van der Aalst, C.M.; de Jong, P.A.; Scholten, E.T.; Nackaerts, K.; Heuvelmans, M.A.; Lammers, J.W.J.; Weenink, C.; Yousaf-Khan, U.; Horeweg, N.; et al. Reduced lung-cancer mortality with volume CT screening in a randomized trial. N. Engl. J. Med. 2020, 382, 503–513. [Google Scholar] [CrossRef]
- Becker, N.; Motsch, E.; Trotter, A.; Heussel, C.P.; Dienemann, H.; Schnabel, P.A.; Kauczor, H.U.; Maldonado, S.G.; Miller, A.B.; Kaaks, R.; et al. Lung cancer mortality reduction by LDCT screening–Results from the randomized German LUSI trial. Int. J. Cancer 2020, 146, 1503–1513. [Google Scholar] [CrossRef]
- Field, J.K.; Vulkan, D.; Davies, M.P.; Baldwin, D.R.; Brain, K.E.; Devaraj, A.; Eisen, T.; Gosney, J.; Green, B.A.; Holemans, J.A.; et al. Lung cancer mortality reduction by LDCT screening: UKLS randomised trial results and international meta-analysis. Lancet Reg. Health Eur. 2021, 10, 100179. [Google Scholar] [CrossRef]
- Saltybaeva, N.; Martini, K.; Frauenfelder, T.; Alkadhi, H. Organ dose and attributable cancer risk in lung cancer screening with low-dose computed tomography. PLoS ONE 2016, 11, e0155722. [Google Scholar] [CrossRef] [Green Version]
- Fu, C.; Liu, Z.; Zhu, F.; Li, S.; Jiang, L. A meta-analysis: Is low-dose computed tomography a superior method for risky lung cancers screening population? Clin. Respir. J. 2016, 10, 333–341. [Google Scholar] [CrossRef]
- Tammemagi, M.C.; Lam, S. Screening for lung cancer using low dose computed tomography. BMJ 2014, 348, 2253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patz, E.F.; Pinsky, P.; Gatsonis, C.; Sicks, J.D.; Kramer, B.S.; Tammemagi, M.C.; Chiles, C.; Black, W.C.; Aberle, D.R. Overdiagnosis in low-dose computed tomography screening for lung cancer. JAMA Intern. Med. 2014, 174, 269–274. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.W.; Li, W.; Han, F.J.; Liu, Y.D. Screening for lung cancer using low-dose computed tomography: Concerns about the application in low-risk individuals. Transl. Lung Cancer Res. 2015, 4, 275–286. [Google Scholar] [PubMed]
- Jonas, D.E.; Reuland, D.S.; Reddy, S.M.; Nagle, M.; Clark, S.D.; Weber, R.P.; Enyioha, C.; Malo, T.L.; Brenner, A.T.; Armstrong, C.; et al. Screening for lung cancer with low-dose computed tomography: Updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2021, 325, 971–987. [Google Scholar] [CrossRef] [PubMed]
- Lam, S.; Tammemagi, M. Contemporary issues in the implementation of lung cancer screening. Eur. Resp. Rev. 2021, 30, 200288. [Google Scholar] [CrossRef] [PubMed]
- Kaaks, R.; Delorme, S. Lung cancer screening by low-dose computed tomography–Part 1: Expected benefits, possible harms, and criteria for eligibility and population targeting. RoFo 2021, 193, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Oudkerk, M.; Liu, S.Y.; Heuvelmans, M.A.; Walter, J.E.; Field, J.K. Lung cancer LDCT screening and mortality reduction-evidence, pitfalls and future perspectives. Nat. Rev. Clin. Oncol. 2021, 18, 135–151. [Google Scholar] [CrossRef]
- Chawla, N.V.; Bowyer, K.W.; Hall, L.O.; Kegelmeyer, W.P. SMOTE: Synthetic minority oversampling technique. J. Artif. Intellig. Res. 2002, 16, 321–357. [Google Scholar] [CrossRef]
- Hoerl, A.E.; Kennard, R.W. Ridge regression: Biased estimation for nonorthogonal problems. Technometrics 1970, 12, 55–67. [Google Scholar] [CrossRef]
- Tibshirani, R. Regression shrinkage and selection via the lasso. J. Roy. Stat. Soc. B Met. 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Zou, H.; Hastie, T. Regularization and variable selection via the elastic net. J. R. Stat. Soc. B 2005, 67, 301–320. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.; Lee, H.Y.; Park, H.; Schiebler, M.L.; van Beek, E.J.R.; Ohno, Y.; Seo, J.B.; Leung, A. Radiomics and its emerging role in lung cancer research, imaging biomarkers and clinical management: State of the art. Eur. J. Radiol. 2017, 86, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Naidich, D.P.; Bankier, A.A.; MacMahon, H.; Schaefer-Prokop, C.M.; Pistolesi, M.; Goo, J.M.; Macchiarini, P.; Crapo, J.D.; Herold, C.J.; Austin, J.H.; et al. Recommendations for the management of subsolid pulmonary nodules detected at CT: A statement from the Fleischner Society. Radiology 2013, 266, 304–317. [Google Scholar] [CrossRef] [PubMed]
- Firmino, M.; Angelo, G.; Morais, H.; Dantas, M.R.; Valentim, R. Computer-aided detection (CADe) and diagnosis (CADx) system for lung cancer with likelihood of malignancy. BioMed. Eng. OnLine 2016, 15, 2. [Google Scholar] [CrossRef] [Green Version]
- Erasmus, J.J.; Connolly, J.E.; McAdams, H.P.; Roggli, V.L. Solitary pulmonary nodules: Part I. Morphologic evaluation for differentiation of benign and malignant lesions. Radiographics 2000, 20, 43–58. [Google Scholar] [CrossRef]
- Brenner, D.R.; McLaughlin, J.R.; Hung, R.J. Previous lung diseases and lung cancer risk: A systematic review and meta-analysis. PLoS ONE 2011, 6, e17479. [Google Scholar] [CrossRef]
- Lee, J.Y.; Jeon, I.; Lee, J.M.; Yoon, J.M.; Park, S.M. Diabetes mellitus as an independent risk factor for lung cancer: A meta-analysis of observational studies. Eur. J. Cancer 2013, 49, 2411–2423. [Google Scholar] [CrossRef]
- Wang, W.; Xu, D.; Wang, B.; Yan, S.; Wang, X.; Yin, Y.; Wang, X.; Sun, B.; Sun, X. Increased risk of cancer in relation to gout: A Review of three prospective cohort studies with 50,358 subjects. Mediat. Inflamm. 2015, 2015, 680853. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.S.; Myung, J.; Lee, H.A.; Hong, S.; Lee, C.K.; Yoo, B.; Oh, J.S.; Kim, Y.G. Risk of cancer in middle-aged patients with gout: A nationwide population-based study in Korea. J. Rheumatol. 2021, 48, 1465–1471. [Google Scholar] [CrossRef]
- Zhou, F.; Zhou, C. Lung cancer in never smokers—The East Asian experience. Transl. Lung Cancer Res. 2018, 7, 450. [Google Scholar] [CrossRef]
- Shi, Y.; Au, J.S.K.; Thongprasert, S.; Srinivasan, S.; Tsai, C.M.; Khoa, M.T.; Heeroma, K.; Itoh, Y.; Cornelio, G.; Yang, P.C. A prospective, molecular epidemiology study of EGFR mutations in Asian patients with advanced non–small-cell lung cancer of adenocarcinoma histology (PIONEER). J. Thorac. Oncol. 2014, 9, 154–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitsudomi, T. Molecular epidemiology of lung cancer and geographic variations with special reference to EGFR mutations. Transl. Lung Cancer Res. 2014, 3, 205. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Coding | Description |
|---|---|---|
| Gender | 0/1 | Female/male |
| Smoke | 0/1 | Non-smoking/smoking |
| PTB | 0/1 | Tuberculosis (TB), old TB, or tuberculous pleurisy |
| Lung radiation | 0/1 | Radiation exposure to lung |
| Asthma | 0/1 | Asthma record |
| COPD | 0/1 | Chronic obstructive pulmonary disease, chronic bronchitis, or emphysema |
| Myoma | 0/1 | Myoma record |
| Diabetes | 0/1 | Diabetes record |
| Hypertension | 0/1 | Hypertension record |
| CVA | 0/1 | Cerebrovascular accident |
| Gout | 0/1 | Gout, hyperuricemia |
| Liver | 0/1 | Diseases related to liver |
| Cardiovascular disease | 0/1 | Diseases related to heart or blood vessels, such as arrhythmia, atrial fibrillation (AF), valvular cardiac valve disease, peripheral arterial occlusive disease (PAOD), and dyslipidemia, and hyperlipidemia. |
| Digestive system | 0/1 | Diseases related to digestive system, such as colorectal polyp, gastric ulcer (GU), gastroesophageal reflux disease (GERD), and anus polyp. |
| Urinary system | 0/1 | Diseases related to urinary system, such as penile tumors, benign prostatic hyperplasia (BPH), ureteral stone, renal stone, and nephrectomy. |
| Thyroid | 0/1 | Diseases related to thyroid, such as thyroid tumor, hypothyroidism, thyroid nodule, thyroidectomy, and goiter. |
| Other cancer | 0/1 | Cancer record other than lung cancer |
| Family lung cancer | 0/1 | Family history of lung cancer |
| Age | age at visit (years) | |
| BMI | Body mass index (BMI) (kg/m2) | |
| BUN | Blood urea nitrogen (BUN) (mg/dL) | |
| Creatinine | Creatinine (mg/dL) | |
| ALT | Alanine aminotransferase (ALT) (IU/L) | |
| HGB | Hemoglobin (HGB) (g/dL) | |
| WBC | White blood cell count (SBC) (103/μL) | |
| Platelet | Platelet (103/μL) |
| Variable | Coding | Description |
|---|---|---|
| Count | Total nodule counts | |
| Diameter | The diameter of the maximum nodule (cm) | |
| GGO | 0/1 | Presence of ground-glass opacity (GGO) |
| Solid | 0/1 | Presence of solid nodule |
| Part Solid | 0/1 | Presence of partial solid nodule |
| Upper | 0/1 | Presence of nodule at middle lobe |
| Middle | 0/1 | Presence of nodule at upper lobe |
| Lower | 0/1 | Presence of nodule at lower lobe |
| Spiculated | 0/1 | Presence of spiculation feature |
| Fibrotic | 0/1 | Presence of fibrotic pattern |
| Mosaic | 0/1 | Presence of mosaic pattern |
| Calcified | 0/1 | Presence of calcification pattern |
| Pneumothorax | 0/1 | Presence of pneumothorax |
| Pleural Effusion | 0/1 | Presence of pleural effusion |
| Variable | Non-Cancer | Cancer | p-Value |
|---|---|---|---|
| Count | 3.08 (2.50) | 1.57 (1.39) | 0.000 |
| Diameter | 1.48 (1.64) | 1.67 (0.83) | 0.003 |
| Age a | 56.58 (9.86) | 61.33 (11.11) | 0.026 |
| BMI a | 24.29 (3.28) | 24.19 (3.24) | 0.877 |
| BUN | 15.41 (4.85) | 18.35 (10.36) | 0.094 |
| Creatinine | 0.93 (0.79) | 1.08 (1.50) | 0.484 |
| ALT | 22.08 (8.92) | 23.61 (18.11) | 0.639 |
| HGB a | 13.32 (1.27) | 13.29 (1.66) | 0.926 |
| WBC a | 6.29 (1.50) | 6.61 (1.90) | 0.372 |
| Platelet a | 221.58 (47.05) | 219.8 (50.95) | 0.855 |
| Variable | Non-Cancer | Cancer | p-Value |
|---|---|---|---|
| Gender a | 0.554 | ||
| Female | 58.33 | 52.58 | |
| Male | 41.67 | 47.42 | |
| Smoke a | 33.33 | 31.96 | 0.880 |
| PTB | 0.00 | 6.19 | 0.190 |
| Lung radiation | 0.00 | 1.03 | 1.000 |
| Asthma | 2.78 | 2.06 | 1.000 |
| COPD | 8.33 | 16.49 | 0.278 |
| Myoma | 0.00 | 1.03 | 1.000 |
| Diabetes | 8.33 | 16.49 | 0.278 |
| Hypertension a | 27.78 | 38.14 | 0.266 |
| CVA | 0.00 | 3.09 | 0.563 |
| Gout | 0.00 | 3.09 | 0.563 |
| Liver | 5.56 | 1.03 | 0.178 |
| Cardiovascular disease a | 22.22 | 17.53 | 0.538 |
| Digestive System | 11.11 | 1.03 | 0.019 |
| Urinary System | 8.33 | 12.37 | 0.759 |
| Thyroid | 11.11 | 4.12 | 0.211 |
| Other Cancer | 5.56 | 14.43 | 0.233 |
| Family lung cancer | 2.78 | 2.06 | 1.000 |
| GGO a | 27.78 | 32.99 | 0.566 |
| Solid | 91.67 | 76.29 | 0.052 |
| Part Solid | 2.78 | 11.34 | 0.179 |
| Upper a | 80.56 | 69.07 | 0.189 |
| Middle a | 30.56 | 9.28 | 0.002 |
| Lower a | 63.89 | 52.58 | 0.243 |
| Spiculated | 0.00 | 29.90 | 0.000 |
| Fibrotic | 11.11 | 15.46 | 0.781 |
| Mosaic | 2.78 | 1.03 | 0.470 |
| Calcified | 11.11 | 9.28 | 0.748 |
| Pneumothorax | 0.00 | 1.03 | 1.000 |
| Pleural Effusion | 2.78 | 6.19 | 0.674 |
| Average of 5-Fold Cross Validation | ||||
|---|---|---|---|---|
| Lasso | Ridge | Elastic Net | Best Model (α = 1, λ = 0.037) | |
| Accuracy | 0.72 | 0.73 | 0.73 | 0.89 |
| Sensitivity | 0.75 | 0.78 | 0.75 | 0.85 |
| Specificity | 0.64 | 0.58 | 0.67 | 1.00 |
| Precision | 0.84 | 0.83 | 0.86 | 1.00 |
| F1-measure | 0.79 | 0.80 | 0.80 | 0.92 |
| G-mean | 0.68 | 0.67 | 0.70 | 0.92 |
| AUC | 0.78 | 0.77 | 0.77 | 0.93 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, H.-T.; Wang, P.-H.; Chen, W.-F.; Lin, C.-J. Risk Assessment of Early Lung Cancer with LDCT and Health Examinations. Int. J. Environ. Res. Public Health 2022, 19, 4633. https://doi.org/10.3390/ijerph19084633
Chang H-T, Wang P-H, Chen W-F, Lin C-J. Risk Assessment of Early Lung Cancer with LDCT and Health Examinations. International Journal of Environmental Research and Public Health. 2022; 19(8):4633. https://doi.org/10.3390/ijerph19084633
Chicago/Turabian StyleChang, Hou-Tai, Ping-Huai Wang, Wei-Fang Chen, and Chen-Ju Lin. 2022. "Risk Assessment of Early Lung Cancer with LDCT and Health Examinations" International Journal of Environmental Research and Public Health 19, no. 8: 4633. https://doi.org/10.3390/ijerph19084633
APA StyleChang, H.-T., Wang, P.-H., Chen, W.-F., & Lin, C.-J. (2022). Risk Assessment of Early Lung Cancer with LDCT and Health Examinations. International Journal of Environmental Research and Public Health, 19(8), 4633. https://doi.org/10.3390/ijerph19084633