
Workplace Factors, Burnout Signs, and Clinical Mental Health Symptoms among Mental Health Workers in Lombardy and Quebec during the First Wave of COVID-19

 ,
,  , and
, and
Abstract
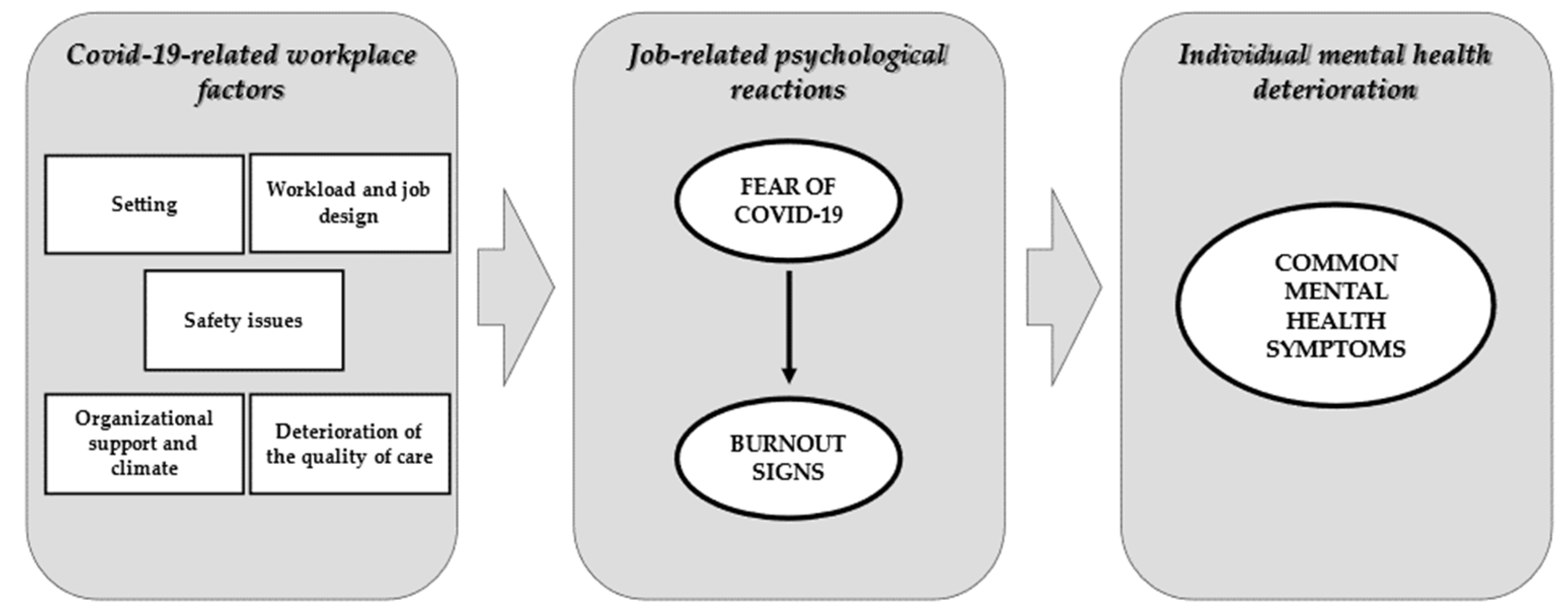
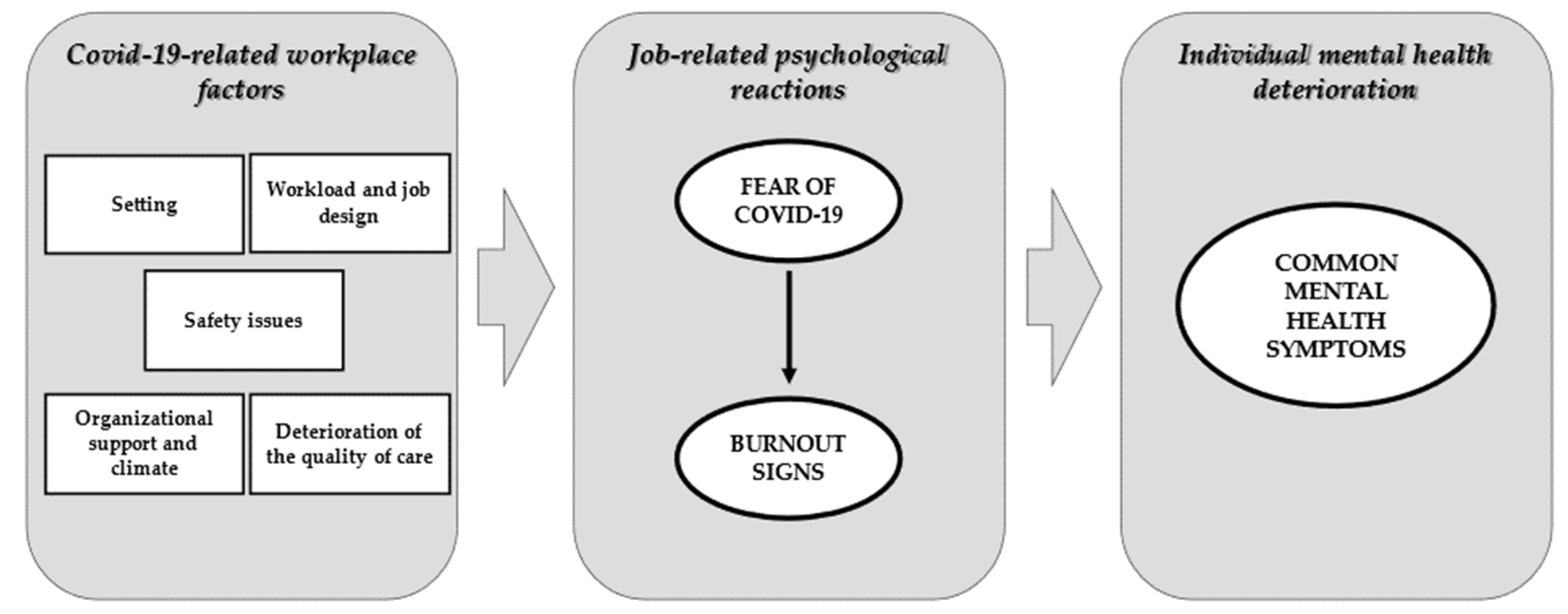
:1. Introduction
2. Materials and Methods
2.1. Design and Data Collection
2.2. Instruments
2.3. Data Analysis
3. Results
3.1. Participants’ Characteristics
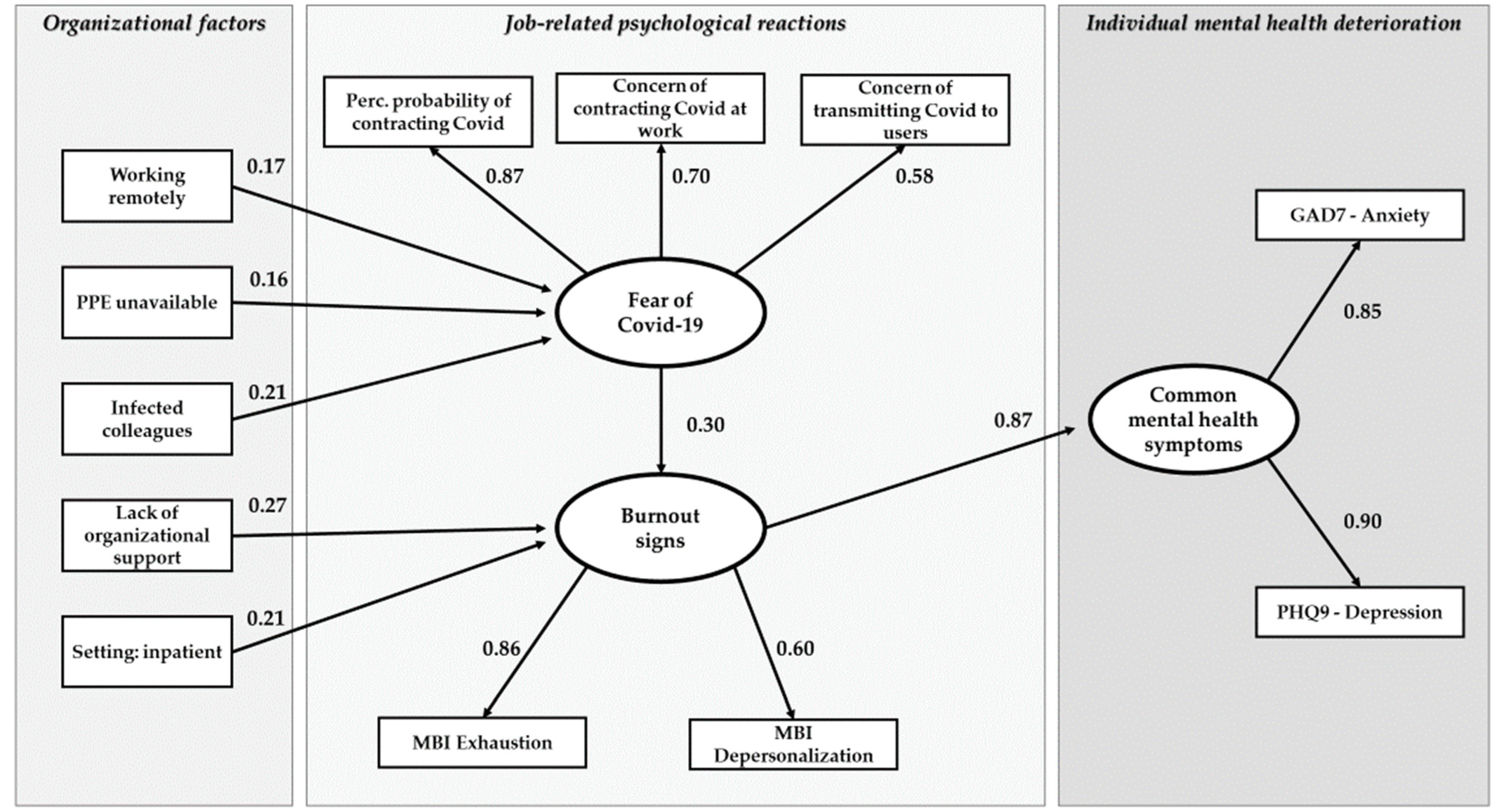
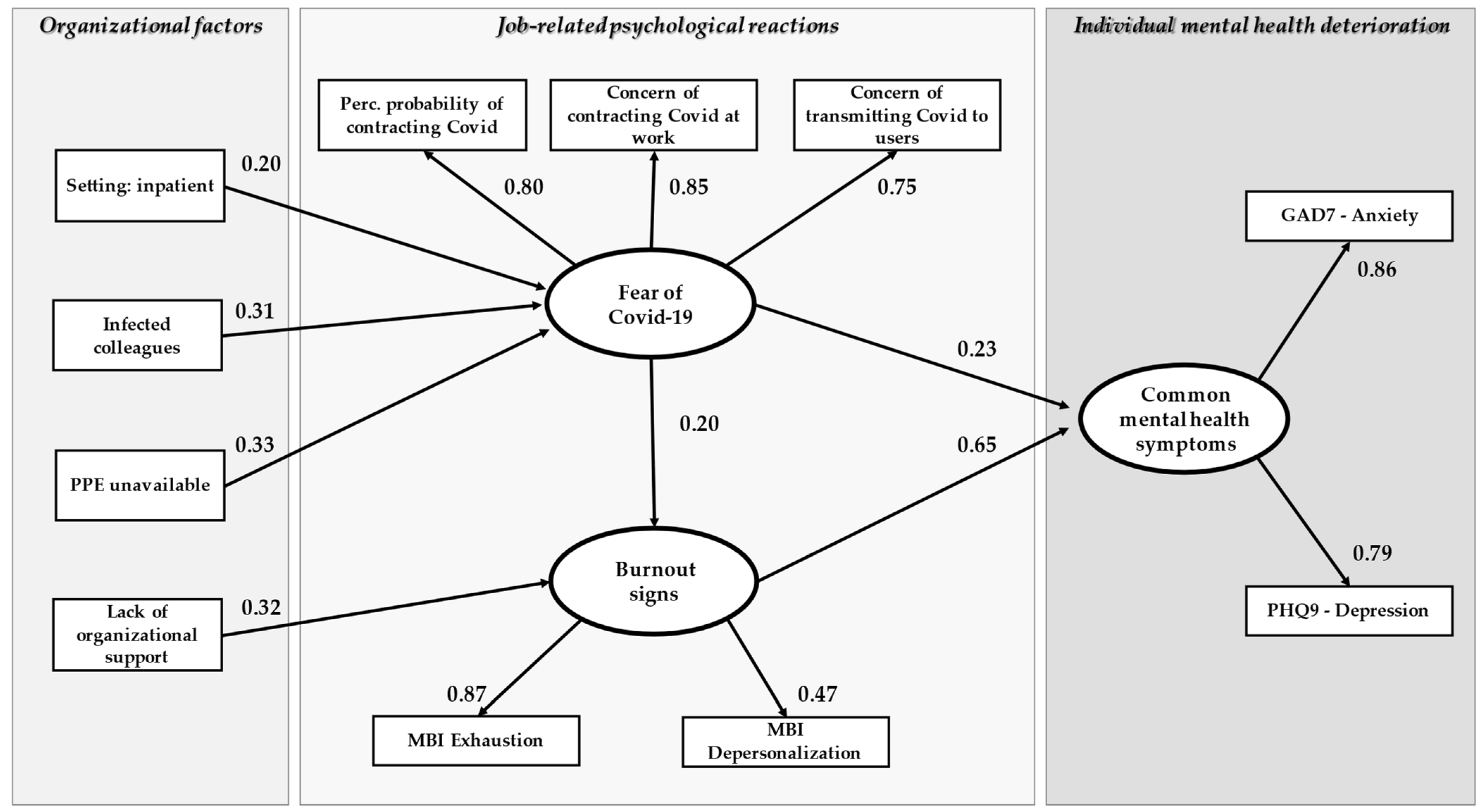
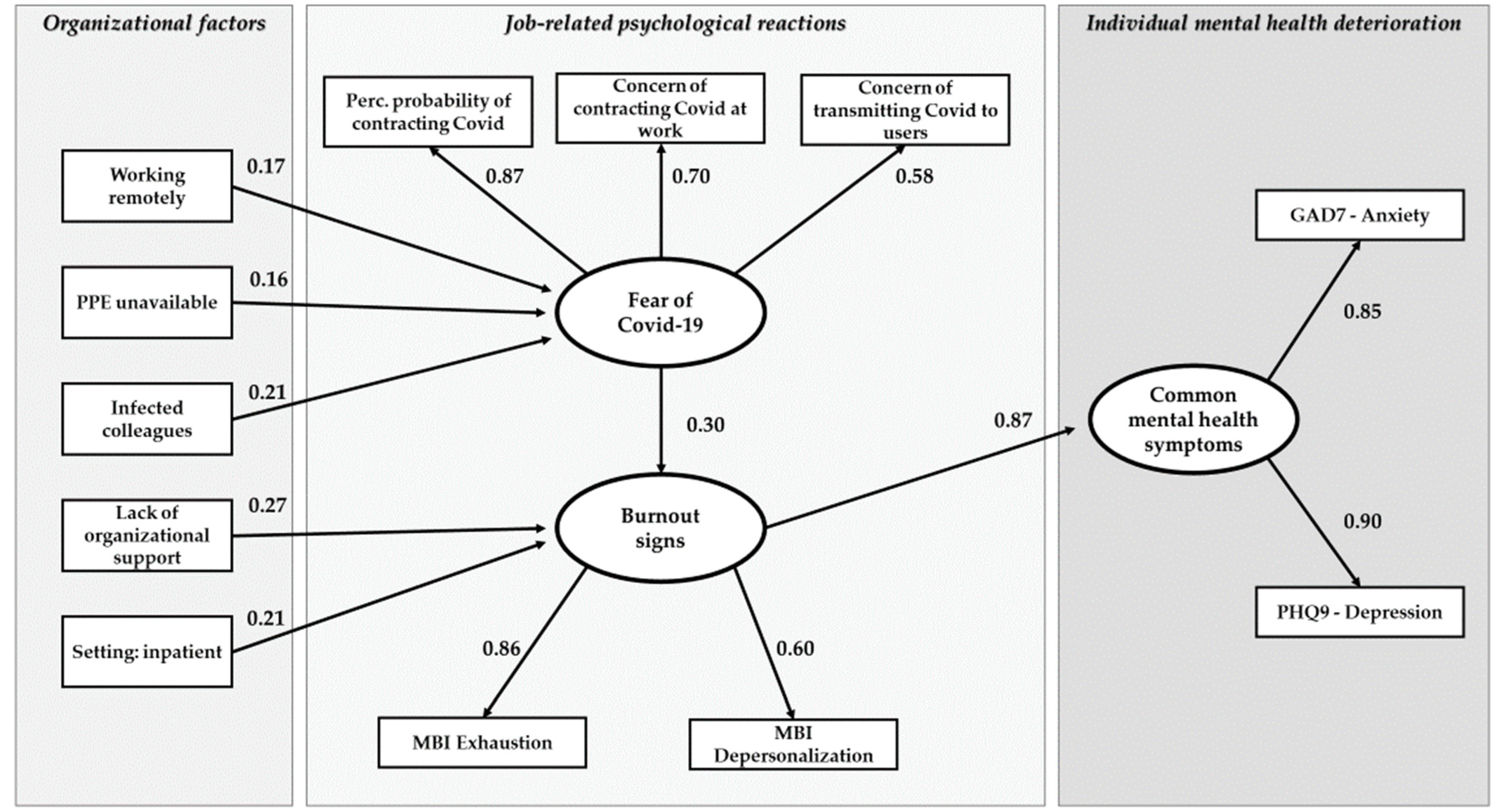
3.2. Path Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raphael, J.; Winter, R.; Berry, K. Adapting practice in mental healthcare settings during the COVID-19 pandemic and other contagions: Systematic review. BJPsych Open 2021, 7, e62. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, A.; Demartini, B.; Cavallotti, S.; Gambini, O. Mental health services in Italy during the COVID-19 outbreak. Lancet Psych. 2020, 7, 385–387. [Google Scholar] [CrossRef]
- Percudani, M.; Corradin, M.; Moreno, M.; Indelicato, A.; Vita, A. Mental health services in Lombardy during COVID-19 outbreak. Psychiatry Res. 2020, 288, 112980. [Google Scholar] [CrossRef]
- Carpiniello, B.; Tusconi, M.; di Sciascio, G.; Enrico, Z.; Di Giannantonio, M. Mental health services in Italy during the COVID-19 pandemic. Psychiatry Clin. Neurosci. 2020, 74, 442–443. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, F.; Vallarino, M.; Cavallini, E.; Barbato, A.; Brousseau-Paradis, C.; De Benedictis, L.; Lesage, A. The Early Impact of the COVID-19 Emergency on Mental Health Workers: A Survey in Lombardy, Italy. Int. J. Environ. Res. Public Health 2020, 17, 8615. [Google Scholar] [CrossRef] [PubMed]
- Haesebaert, F.; Haesebaert, J.; Zante, E.; Franck, N. Who maintains good mental health in a locked-down country? A French nationwide online survey of 11,391 participants. Health Place 2020, 11, 66. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.M.; Sultana, A.; Purohit, N. Mental health outcomes of quarantine and isolation for infection prevention: A systematic umbrella review of the global evidence. Epidemiol. Health 2020, 42, e2020038. [Google Scholar] [CrossRef]
- Tsonis, O.; Diakaki, K.; Gkrozou, F.; Papadaki, A.; Dimitriou, E.; Paraskevaidis, M.; Siafaka, V. Psychological burden of COVID-19 health crisis on health professionals and interventions to minimize the effect: What has history already taught us? Riv. Psichiatr. 2021, 56, 57–63. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Lluch, C.; Galiana, L.; Doménech, P.; Sansó, N. The Impact of the COVID-19 Pandemic on Burnout, Compassion Fatigue, and Compassion Satisfaction in Healthcare Personnel: A Systematic Review of the Literature Published during the First Year of the Pandemic. Healthcare 2022, 10, 364. [Google Scholar] [CrossRef]
- Roberts, R.; Wong, A.; Jenkins, S.; Neher, A.; Sutton, C.; O’Meara, P.; Frost, M.; Bamberry, L.; Dwivedi, A. Mental health and well-being impacts of COVID-19 on rural paramedics, police, community nurses and child protection workers. Aust. J. Rural Health 2021, 29, 753–767. [Google Scholar] [CrossRef] [PubMed]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare staff wellbeing, burnout, and patient safety: A systematic review. PLoS ONE 2016, 11, e0159015. [Google Scholar] [CrossRef] [PubMed]
- Aronsson, G.; Theorell, T.; Grape, T.; Hammarström, A.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Träskman-Bendz, L.; Hall, C. A systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health 2017, 17, 264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leiter, M.P.; Harvie, P.L. Burnout among mental health workers: A review and a research agenda. Int. J. Soc. Psychiatry 1996, 42, 90–101. [Google Scholar] [CrossRef]
- Morse, G.; Salyers, M.P.; Rollins, A.L.; Monroe-DeVita, M.; Pfahler, C. Burnout in mental health services: A review of the problem and its remediation. Adm. Policy Ment. Health 2012, 39, 341–352. [Google Scholar] [CrossRef] [Green Version]
- Naldi, A.; Vallelonga, F.; Di Liberto, A.; Cavallo, R.; Agnesone, M.; Gonella, M.; Leombruni, P. COVID-19 pandemic-related anxiety, distress and burnout: Prevalence and associated factors in healthcare workers of north-west italy. BJPsych Open 2021, 7, 9. [Google Scholar] [CrossRef]
- Fiabane, E.; Gabanelli, P.; La Rovere, M.T.; Tremoli, E.; Pistarini, C.; Gorini, A. Psychological and work-related factors associated with emotional exhaustion among healthcare professionals during the COVID-19 outbreak in Italian hospitals. Nurs. Health Sci. 2021, 23, 670–675. [Google Scholar] [CrossRef]
- Foye, U.; Dalton-Locke, C.; Harju-Seppänen, J.; Lane, R.; Beames, L.; Vera San Juan, N.; Simpson, A. How has COVID-19 affected mental health nurses and the delivery of mental health nursing care in the UK? results of a mixed-methods study. J. Psychiatr. Ment. Health Nurs. 2021, 28, 126–137. [Google Scholar] [CrossRef]
- Sklar, M.; Ehrhart, M.G.; Aarons, G.A. COVID-related work changes, burnout, and turnover intentions in mental health providers: A moderated mediation analysis. Psychiatr. Rehabil. J. 2021, 44, 219–228. [Google Scholar] [CrossRef]
- Johnson, S.; Dalton-Locke, C.; Vera San Juan, N.; Foye, U.; Oram, S.; Papamichail, A.; Landau, S.; Olive, R.R.; Jeynes, T.; Shah, P.; et al. Impact on mental health care and on mental health service users of the COVID-19 pandemic: A mixed methods survey of UK mental health care staff. Soc. Psychiatry 2021, 56, 25–37. [Google Scholar] [CrossRef]
- Islam, M.; George, P.; Sankaran, S.; Janet Leu, S.H.; Kit, T. Impact of COVID-19 on the mental health of healthcare workers in different regions of the world. BJPsych Open 2021, 7, S258–S259. [Google Scholar] [CrossRef]
- Pappa, S.; Barnett, J.; Berges, I.; Sakkas, N. Tired, worried and burned out, but still resilient: A cross-sectional study of mental health workers in the UK during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4457. [Google Scholar] [CrossRef] [PubMed]
- De los Santos, J.A.A.; Labrague, L.J. The impact of fear of COVID-19 on job stress, and turnover intentions of frontline nurses in the community: A cross-sectional study in the Philippines. Traumat. Int. J. 2021, 27, 52–59. [Google Scholar] [CrossRef]
- Cawcutt, K.A.; Starlin, R.; Rupp, M.E. Fighting fear in healthcare workers during the COVID-19 pandemic. Infect Control Hosp. Epidemiol. 2020, 41, 1192–1193. [Google Scholar] [CrossRef]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; WU, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. 2020, 3, e203976. [Google Scholar] [CrossRef]
- Arnetz, J.E.; Goetz, C.M.; Sudan, S.; Arble, E.; Janisse, J.; Arnetz, B.B. Personal protective equipment and mental health symptoms among nurses during the COVID-19 pandemic. J. Occup. Environ. Med. 2020, 62, 892–897. [Google Scholar] [CrossRef]
- Kameg, B.N.; Fradkin, D.; Lee, H.; Mitchell, A. Mental wellness among psychiatric-mental health nurses during the COVID-19 pandemic. Arch. Psychiatr. Nurs. 2021, 35, 401–406. [Google Scholar] [CrossRef]
- Tam, C.C.; Sun, S.; Yang, X.; Li, X.; Zhou, Y.; Shen, Z. Psychological distress among hiv healthcare providers during the COVID-19 pandemic in china: Mediating roles of institutional support and resilience. AIDS Behav. 2020, 25, 9–17. [Google Scholar] [CrossRef]
- Bianchi, R.; Schonfeld, I.S.; Laurent, E. Is burnout separable from depression in cluster analysis? A longitudinal study. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 1005–1011. [Google Scholar] [CrossRef] [Green Version]
- Tokac, U.; Razon, S. Nursing professionals’ mental well-being and workplace impairment during the COVID-19 crisis: A Network analysis. J. Nurs. Manag. 2021, 29, 1653–1659. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Sirigatti, S.; Stefanile, C. Per una scala di misurazione del burnout. Boll. Psicol. Appl. 1988, 187, 29–32. [Google Scholar]
- Sirigatti, S.; Stefanile, C. Adattamento e taratura per l’Italia. In MBI Maslach Burnout Inventory; Maslach, C., Jackson, S.E., Eds.; Organizzazioni Speciali: Firenze, Italy, 1993; pp. 33–42. [Google Scholar]
- Dion, G.; Tessier, R. Validation de la traduction de l’inventaire d’épuisement professionnel de Maslach et Jackson. Can. J. Behav. Sci. 1994, 26, 210–227. [Google Scholar] [CrossRef] [Green Version]
- Maslach, C.; Leiter, M.P. Early predictors of job burnout and engagement. J. Appl. Psychol. 2008, 93, 498–512. [Google Scholar] [CrossRef] [Green Version]
- Schaufeli, W.B.; Taris, T.W. The conceptualization and measurement of burnout: Common ground and worlds apart. Work. Stress 2005, 19, 256–262. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Yorck Herzberg, P. Validation and standardization of the generalized anxiety disorder screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef]
- Mogesie, N.; Mekonnen, T.; Mengesha, B.; Gebyaw, B.; Erkihun, T. Prevalence of anxiety, depression, and psychological distress among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Int. J. Soc. Psychiatry 2021, 11, 892–906. [Google Scholar]
- Pandémie, Bien-Étre Émotionnel et Santé Mentale. Available online: https://www.inspq.qc.ca/sites/default/files/publications/3083-bien-etre-emotionnel-sante-mentale-COVID19.pdf (accessed on 17 February 2021).
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Janet, B.W. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [Green Version]
- Gilbody, S.; Richards, D.; Barkham, M. Diagnosing depression in primary care using self-completed instruments: A UK validation of the PHQ-9 and CORE-OM. Br. J. Gen. Pract. 2007, 57, 650–652. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria versus New Alternatives. Struct. Equ. Model. Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Steiger, J.H. Structural model evaluation and modification: An interval estimation approach. Multivar. Behav. Res. 1990, 25, 173–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maslach, C.; Leiter, M.P. Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry 2016, 15, 103–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, A.E.; Albanese, B.J.; Shapiro, N.M.; Aarons, G.A. The roles of individual and organizational factors in burnout among community-based mental health service providers. Psychol. Serv. 2014, 11, 41–49. [Google Scholar] [CrossRef] [Green Version]
- Bakker, A.B.; Costa, P.L. Chronic job burnout and daily functioning: Atheoretical analysis. Burn. Res. 2014, 1, 112–119. [Google Scholar] [CrossRef] [Green Version]
- Erbiçer, E.S.; Metin, A.; Çetinkaya, A.; Şen, S. The relationship between fear of COVID-19 and depression, anxiety, and stress: A meta-analysis. Eur. Psychol. 2021, 26, 323–333. [Google Scholar] [CrossRef]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Job burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [Green Version]
- Demerouti, E.; Bakker, A.B.; Nachreiner, F.; Schaufeli, W.B. The job demands-resources model of burnout. J. Appl. Soc. Psychol. 2001, 86, 499–512. [Google Scholar] [CrossRef]
- Hennein, R.; Lowe, S. A hybrid inductive-abductive analysis of health workers’ experiences and wellbeing during the COVID-19 pandemic in the United States. PLoS ONE 2020, 15, e0240646. [Google Scholar] [CrossRef]
- Dufour, M.; Bergeron, N.; Rabasa, A.; Guay, S.; Geoffrion, S. Assessment of psychological distress in health-care workers during and after the first wave of COVID-19: A canadian longitudinal study: Évaluation de la détresse psychologique chez les travailleurs de la santé durant et après la première vague de la COVID-19: Une étude longitudinale canadienne. Can. J. Psychiatry 2021, 7067437211025217. [Google Scholar] [CrossRef]
- Magliano, L.; Bonavigo, T.; Battiston, C.; Oretti, A.; Accardo, R.; D’Ambrosi, G.; Affuso, G.; Pascolo-Fabrici, E. Views of mental health professionals on positive changes in service practices and staff-user relationships after one year of COVID-19 pandemic in Italy. J. Psychos. Rehab. Mental Health 2021, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Rapisarda, F.; Corbière, M.; Lesage, A.D.; De Benedictis, L.; Pelletier, J.F.; Felx, A.; Miglioretti, M. Development and validation of the mental health professional culture inventory. Epidemiol. Psychiatr. Sci. 2019, 29, 1–9. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Variables | Lombardy n = 212 | Quebec n = 184 |
|---|---|---|
| Sex | ||
| Female | 161 (75.9%) | 138 (75.0%) |
| Age | ||
| Mean, sd * | 44.4 (12.2) | 41.8 (11.1) |
| Professional Role ** | ||
| Rehabilitation counselor | 62 (29.2%) | 39 (21.2%) |
| Psychologist | 59 (27.8%) | 14 (7.6%) |
| Nurse | 22 (10.4%) | 42 (22.8%) |
| Medical Doctor | 22 (10.4%) | 15 (8.2%) |
| Social Worker | 14 (6.6%) | 43 (23.4%) |
| Peer Supporter | 15 (7.1%) | 0 (0.0%) |
| Manger or Administration Officer | 7 (3.3%) | 17 (9.2%) |
| Other | 11 (5.2%) | 13 (7.1%) |
| Setting | ||
| Outpatient | 122 (57.5%) | 110 (59.8%) |
| Inpatient | 73 (34.4%) | 74 (40.2%) |
| Availability of PPE * | ||
| Always available or not necessary | 192 (90.6%) | 145 (78.8%) |
| Sometimes unavailable | 20 (9.4%) | 39 (21.2%) |
| Did any of your colleagues get COVID-19? | ||
| Yes | 117 (55.2%) | 119 (64.7%) |
| Did any of your users/clients get COVID-19 | ||
| Yes | 107 (50.5%) | 109 (50.2%) |
| Have you been working remotely only? | ||
| Yes ** | 68 (32.1%) | 22 (12.0%) |
| Did workload increase during COVID-19 pandemic? | ||
| Yes ** | 43 (20.5%) | 85 (46.2%) |
| Variables | Lombardy n = 212 | Quebec n = 184 |
|---|---|---|
| Fear of contagion | ||
| Perceived risk of contracting COVID-19 at work a | 1.6 (0.7) | 1.5 (0.6) |
| Concern of contracting COVID-19 at work b * | 1.1 (0.9) | 1.3 (0.7) |
| Maslach Burnout Inventory | ||
| Staff above the “moderate emotional exhaustion” cut off | 45 (21.2%) | 52 (28.3%) |
| Staff above the “severe emotional exhaustion” cut off | 36 (17.0%) | 66 (33.0%) |
| Staff above the “moderate depersonalization” cut off | 41 (21.1%) | 49 (26.6%) |
| Staff above the “severe depersonalization” cut off | 46 (23.7%) | 52 (28.3%) |
| Common mental health symptoms | ||
| GAD7 (anxiety symptoms), mean score (SD) | 5.1 (3.4) | 4.9 (4.4) |
| Staff above the “moderate anxiety” cut off | 28 (13.2%) | 31 (16.9%) |
| Staff above the “severe anxiety” cut off | 3 (1.4%) | 7 (3.8%) |
| PHQ9 (depression symptoms), mean score (SD) | 4.8 (2.9) | 5.5 (4.5) |
| Staff above the “moderate depression” cut off | 15 (7.0%) | 32 (15.3%) |
| Staff above the “severe depression” cut off | 2 (0.9%) | 8 (2.3%) |
| Self-reported narratives of work-related difficulties | ||
| Changes in workload and tasks ** | 61 (30.4%) | 78 (42.6%) |
| Perceived lack of organizational support ** | 41 (20.1%) | 68 (37.1%) |
| Pandemic context reduced the quality of mental health care ** | 87 (42.9%) | 39 (21.3%) |
| Emotional distress | 27 (13.4%) | 35 (18.8%) |
| Difficulties in respecting safety norms * | 12 (5.8%) | 22 (11.9%) |
| Lack of support from colleagues | 14 (6.8%) | 14 (7.4%) |
| Work-life balance | 14 (6.8%) | 5 (2.5%) |
| Lombardy | Quebec | |||||||
|---|---|---|---|---|---|---|---|---|
| Regression Parameter | Std. Estimate | Std. Err | z | p | Std. Estimate | Std. Err | z | p |
| Determinants of FCC | ||||||||
| LPPE → FCC | 0.33 | 0.06 | 5.28 | <0.01 | 0.16 | 0.08 | 2.08 | 0.03 |
| Inf Coll → FCC | 0.31 | 0.06 | 4.83 | <0.01 | 0.22 | 0.08 | 2.75 | <0.01 |
| Setting → FCC | 0.20 | 0.07 | 2.85 | <0.01 | Not included in the model | |||
| Work rem → FCC | Not included in the model | 0.17 | 0.08 | 2.14 | 0.03 | |||
| Determinants of BS | ||||||||
| FCC → BS | 0.19 | 0.08 | 2.37 | 0.02 | 0.30 | 0.08 | 3.68 | <0.01 |
| LOS → BS | 0.32 | 0.07 | 4.50 | <0.01 | 0.27 | 0.07 | 3.67 | <0.01 |
| Setting (inpatient) → BS | Not included in the model | 0.21 | 0.07 | 2.87 | <0.01 | |||
| Determinants of CMHS | ||||||||
| FCC →CMHS | 0.24 | 0.07 | 3.36 | <0.01 | Not included in the model | |||
| BS →CMHS | 0.64 | 0.08 | 8.45 | <0.01 | 0.87 | 0.04 | 21.20 | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rapisarda, F.; Vallarino, M.; Brousseau-Paradis, C.; Benedictis, L.D.; Corbière, M.; Villotti, P.; Cavallini, E.; Briand, C.; Cailhol, L.; Lesage, A. Workplace Factors, Burnout Signs, and Clinical Mental Health Symptoms among Mental Health Workers in Lombardy and Quebec during the First Wave of COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 3806. https://doi.org/10.3390/ijerph19073806
Rapisarda F, Vallarino M, Brousseau-Paradis C, Benedictis LD, Corbière M, Villotti P, Cavallini E, Briand C, Cailhol L, Lesage A. Workplace Factors, Burnout Signs, and Clinical Mental Health Symptoms among Mental Health Workers in Lombardy and Quebec during the First Wave of COVID-19. International Journal of Environmental Research and Public Health. 2022; 19(7):3806. https://doi.org/10.3390/ijerph19073806
Chicago/Turabian StyleRapisarda, Filippo, Martine Vallarino, Camille Brousseau-Paradis, Luigi De Benedictis, Marc Corbière, Patrizia Villotti, Elena Cavallini, Catherine Briand, Lionel Cailhol, and Alain Lesage. 2022. "Workplace Factors, Burnout Signs, and Clinical Mental Health Symptoms among Mental Health Workers in Lombardy and Quebec during the First Wave of COVID-19" International Journal of Environmental Research and Public Health 19, no. 7: 3806. https://doi.org/10.3390/ijerph19073806
APA StyleRapisarda, F., Vallarino, M., Brousseau-Paradis, C., Benedictis, L. D., Corbière, M., Villotti, P., Cavallini, E., Briand, C., Cailhol, L., & Lesage, A. (2022). Workplace Factors, Burnout Signs, and Clinical Mental Health Symptoms among Mental Health Workers in Lombardy and Quebec during the First Wave of COVID-19. International Journal of Environmental Research and Public Health, 19(7), 3806. https://doi.org/10.3390/ijerph19073806