
Access to Healthcare Facilities and Women’s Healthcare Requirements in Urban Areas: A Case Study of Beijing

Abstract
1. Introduction
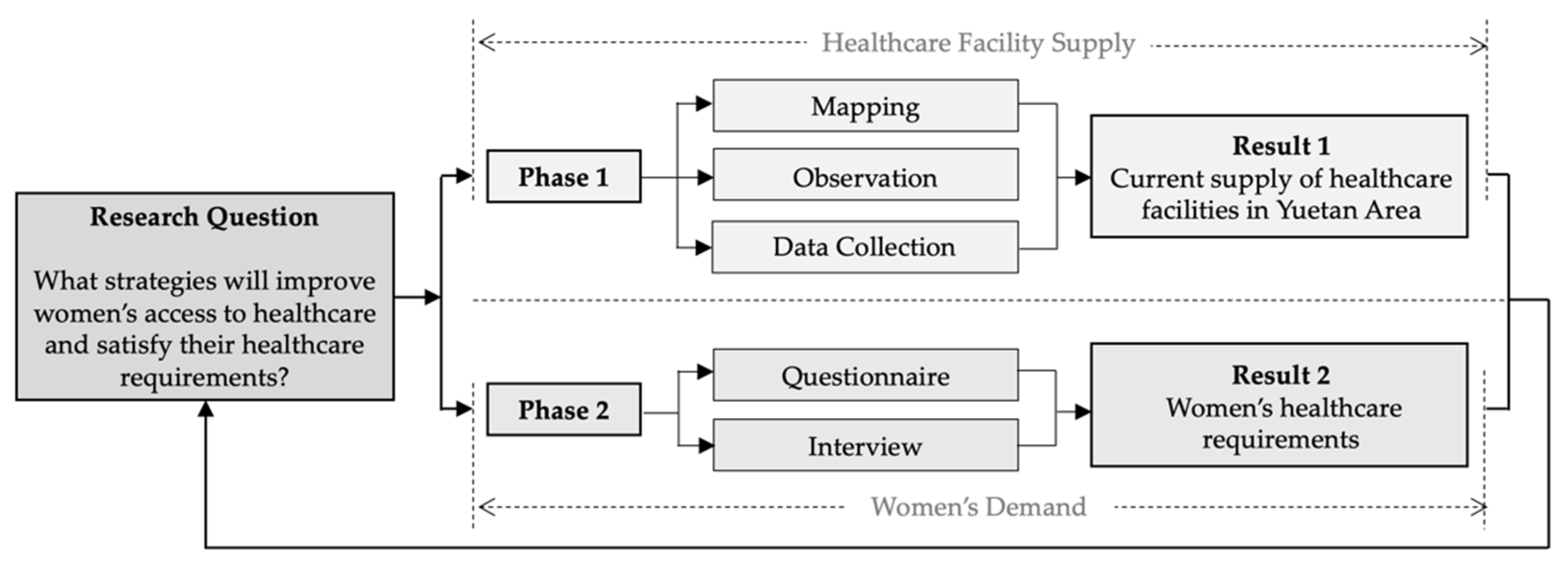
2. Materials and Methods
2.1. Mapping, Observation and Data Collection
2.2. Questionnaire and Interview
3. Results and Discussion
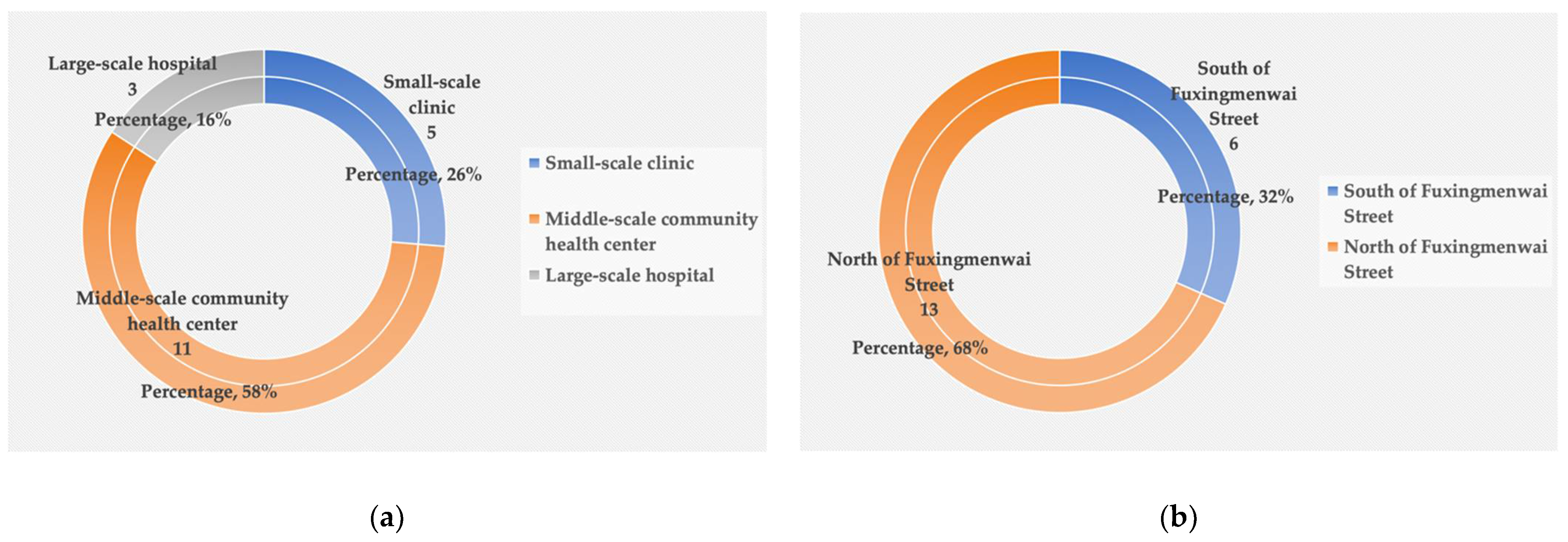
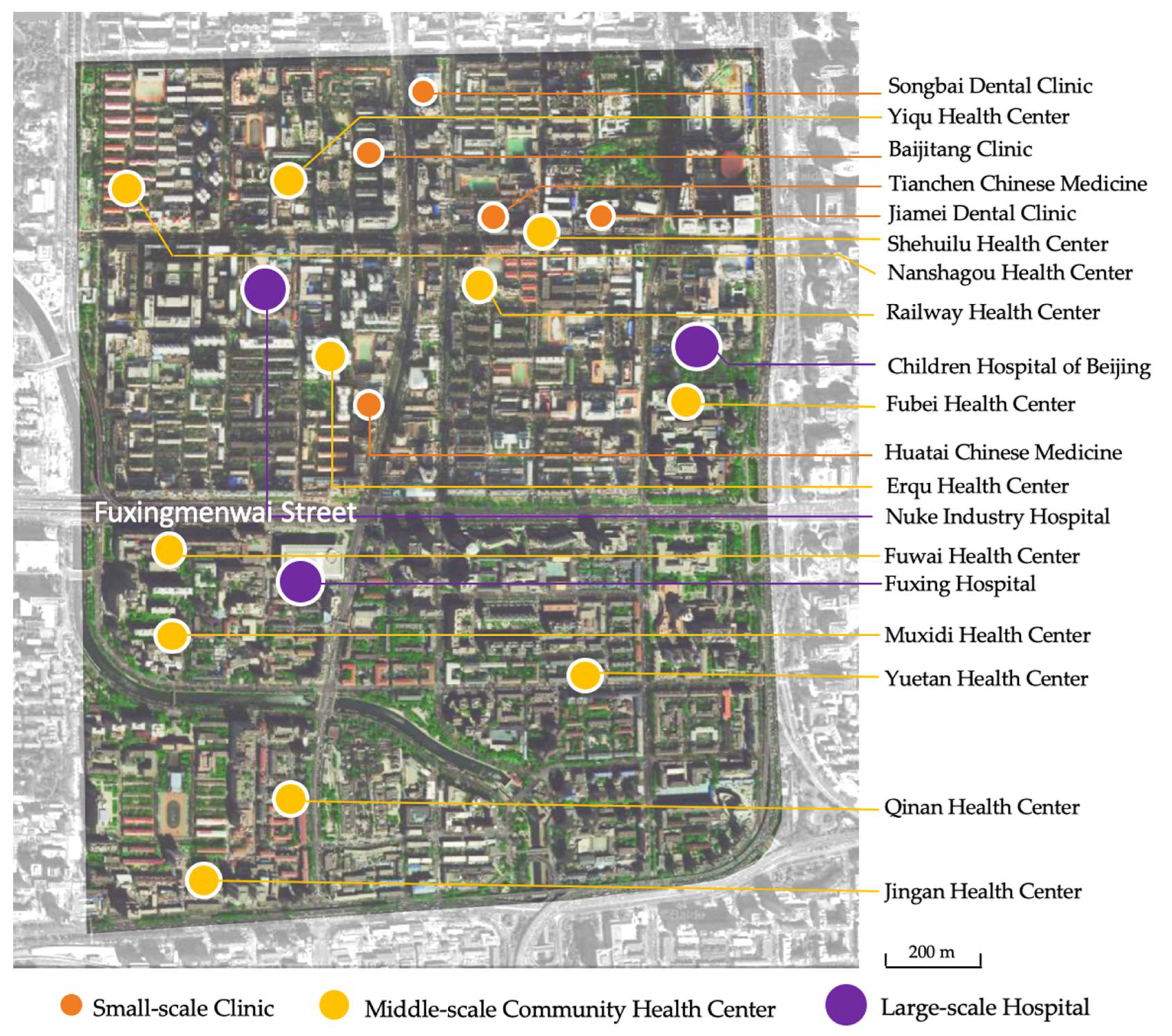
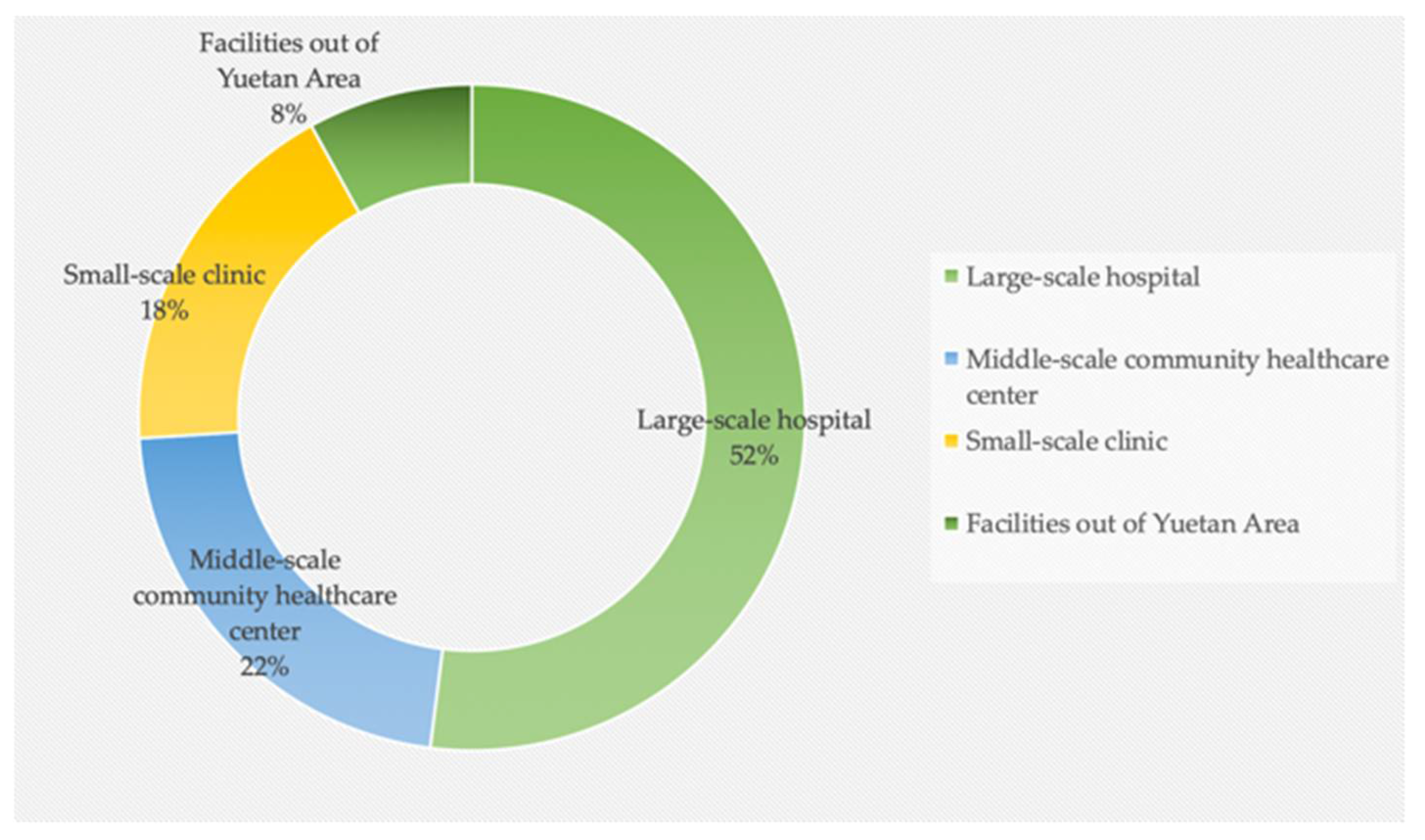
3.1. Current Healthcare Facility Supply in Yuetan Area
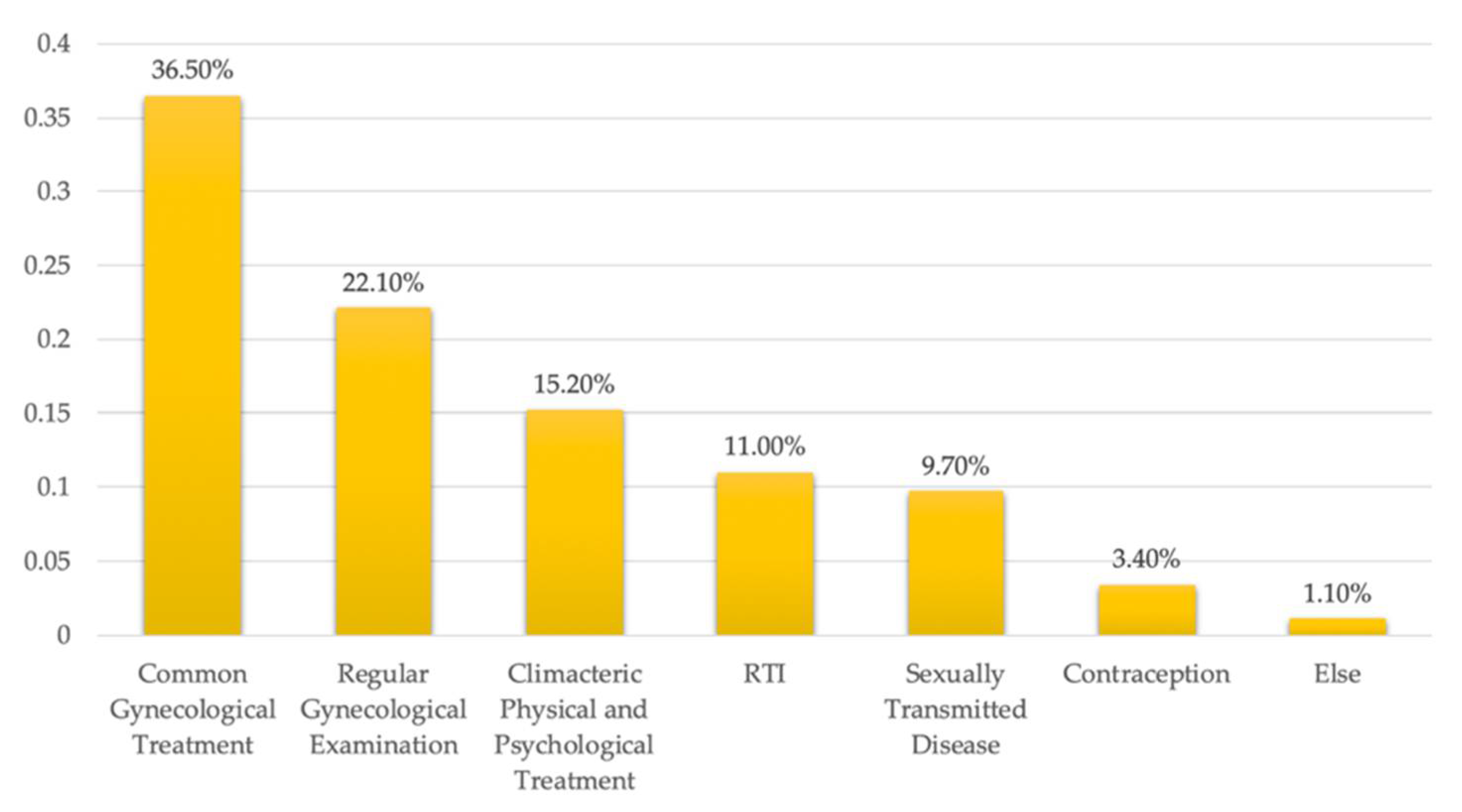
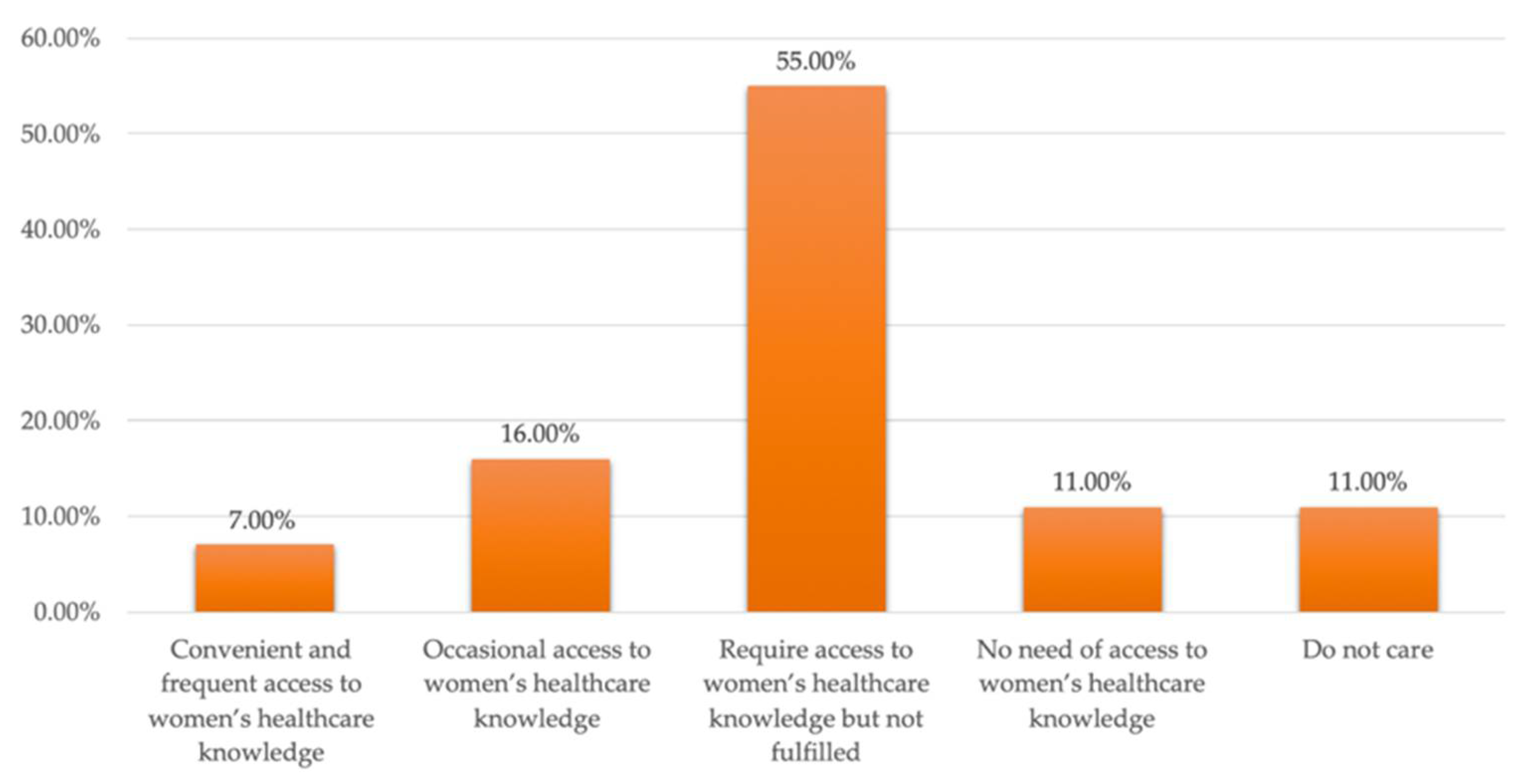
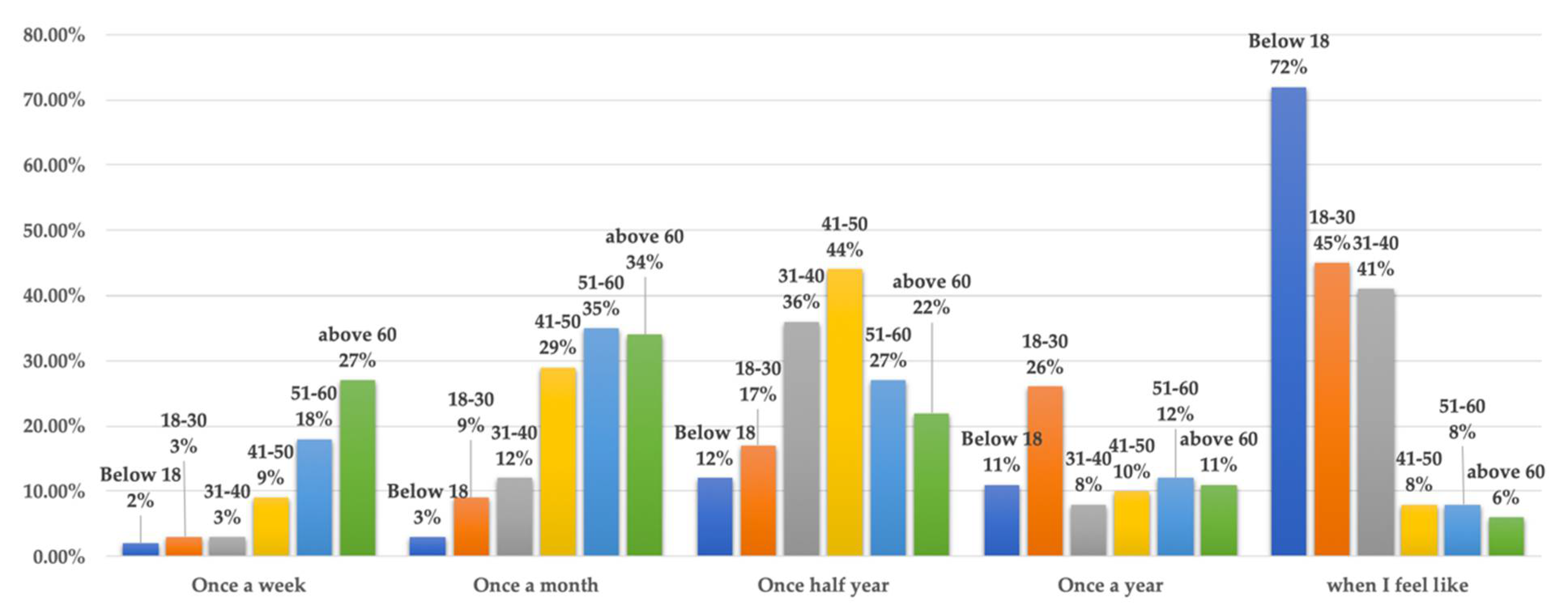
3.2. Women’s Healthcare Requirements
4. Strategies to Improve Healthcare Facilities’ Accessibility
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lawrence, R.; Fudge, C. Healthy Cities in a Global and Regional Context. Health Promot. Int. 2009, 24, i11–i18. [Google Scholar] [CrossRef] [PubMed][Green Version]
- World Health Organization. The Ottawa Charter for Health Promotion; World Health Organization: Ottawa, ON, Canada, 1986. [Google Scholar]
- World Health Organization Regional Office for Europe. Implementation Framework for Phase VII (2019–2024) of the WHO European Healthy Cities Network: Goals, Requirements and Strategic Approaches; World Health Organization: København, Denmark, 2019. [Google Scholar]
- Tsouros, A.D. World Health Organization Healthy Cities Project: A Project Becomes a Movement: Review of Progress 1987 to 1990; Sogess: Milano, Italy, 1991. [Google Scholar]
- Draper, R. WHO Healthy Cities Project: Review of the First Five Years (1987–1992): A Working Tool and A Reference Framework for Evaluating the Project; World Health Organization Regional Office for Europe: København, Denmark, 1993. [Google Scholar]
- Zhang, Y.; Liu, C. Parametric Modeling for Form-Based Planning in Dense Urban Environments. Sustainability 2019, 20, 5678. [Google Scholar] [CrossRef]
- Figueras, J.; Mckee, M. Health Systems, Health, Wealth and Social Well-being: Assessing the Case For Investing In Health Systems; Open University Press: Berkshire, UK, 2012. [Google Scholar]
- Aliyu, K. Spatial Distribution of Public Health Care Facilities in Gombe LGA BY. Bachelor’s Thesis, Gombe State University, Gombe, Nigeria, October 2019. [Google Scholar]
- Ogundare, E.I. Healthcare Delivery is a Success in Oyo State. Dly. Sketch 1982, 27, 7. [Google Scholar]
- Sanni, L. Distribution Pattern of Healthcare Facilities in Osun State, Nigeria. Ethiop. J. Environ. Stud. Manag. 2010, 3, 65–76. [Google Scholar] [CrossRef][Green Version]
- Luo, W. Using a GIS-based Floating Catchment Method to Assess Areas with Shortage of Physicians. Health Place 2004, 10, 1–11. [Google Scholar] [CrossRef]
- World Health Organization. Density of Hospitals. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3361 (accessed on 12 October 2021).
- World Health Organization. Hospital Beds per 1000 Population. Available online: https://www.who.int/data/gho/indicator-metadata-registry/imr-details/3119 (accessed on 12 October 2021).
- Shanosky, N.; McDermott, D.; Kurani, N. How Do U.S. Healthcare Resources Compare to Other Countries? Available online: https://www.healthsystemtracker.org/chart-collection/u-s-health-care-resources-compare-countries/ (accessed on 12 August 2020).
- Ujoh, F.; Kwaghsende, F. Analysis of the Spatial Distribution of Health Facilities in Benue State. Niger. Sci. Acad. Publ. 2014, 4, 210–218. [Google Scholar] [CrossRef]
- Ahmadi-Javid, A.; Seyedi, P.; Syam, S.S. A Survey of Healthcare Facility Location. Comput. Oper. Res. 2017, 79, 223–263. [Google Scholar] [CrossRef]
- World Health Organization. The Urban Health Crisis: Strategies for Health for All in the Face of Rapid Urbanization; WHO Library Cataloguing in Publication Data: Geneva, Switzerland, 1993. [Google Scholar]
- Vearey, J.; Luginaah, I.; Magitta, N.F.; Shilla, D.J.; Oni, T. Urban Health in Africa: A Critical Global Public Health Priority. BMC Public Health 2019, 19, 340. [Google Scholar] [CrossRef] [PubMed]
- Aliyu, A.A.; Amada, L. Urbanization, Cities, and Health: The Challenges to Nigeria—A Review. Ann. Afr. Med. 2017, 16, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Chassin, M.R. Is Health Care ready for Six Sigma Quality? Milbank Q. 1998, 76, 565–591. [Google Scholar] [CrossRef] [PubMed]
- Chassin, M.R.; Galvin, R.W. The Urgent Need to Improve Health Aare Quality. J. Am. Med Assoc. 1998, 280, 1000–1005. [Google Scholar] [CrossRef] [PubMed]
- Greiner, A.C.; Knebel, E. Health Professions Education: A Bridge to Quality; National Academies Press: Washington, DC, USA, 2003. [Google Scholar]
- Zhang, Y.; Chen, G.; He, Y.; Jiang, X.; Xue, C. Social Interaction in Public Spaces and Well-Being among Elderly Women: Towards Age-Friendly Urban Environments. Int. J. Environ. Res. Public Health 2022, 19, 746. [Google Scholar] [CrossRef] [PubMed]
- Kiesel, L. Women and Pain: Disparities in Experience and Treatment. Available online: https://www.health.harvard.edu/blog/women-and-pain-disparities-in-experience-and-treatment-2017100912562 (accessed on 9 October 2017).
- Long, M.; Frederiksen, B.; Ranji, U.; Salganicoff, A. Women’s Health Care Utilization and Costs: Findings from the 2020 KFF Women’s Health Survey. Available online: https://www.kff.org/womens-health-policy/issue-brief/womens-health-care-utilization-and-costs-findings-from-the-2020-kff-womens-health-survey/ (accessed on 21 April 2021).
- Chen, G.; Liu, L.; Yu, J. A Comparative Study on Strength between American College Male and Female Students in Caucasian and Asian Populations. Sport Sci. Rev. 2012, 21, 153–165. [Google Scholar] [CrossRef]
- Ventura Orthopedics. Available online: https://venturaortho.com/do-people-really-shrink-with-age/ (accessed on 29 October 2021).
- Wheeler, J.B.; Foreman, M.; Rueschhoff, A. Improving Women’s Health Challenges, Access and Prevention. Available online: https://www.ncsl.org/research/health/improving-womens-health-2013.aspx (accessed on 31 December 2013).
- Barton, H.; Tsurou, C. Healthy Urban Planning; Spon Press: London, UK, 2000. [Google Scholar]
- MedilinePlus, Women’s Health. Available online: https://medlineplus.gov/ency/article/007458.htm (accessed on 1 August 2021).
- Carmel, S. Health and Well-Being in Late Life: Gender Differences Worldwide. Front. Med. 2019, 6, 218. [Google Scholar] [CrossRef] [PubMed]
- Wang, L. An Analysis on Elderly Women and Social Service Demands. J. China Women’s Univ. 2016, 28, 47–54. [Google Scholar] [CrossRef]
- Safran, D.G.; Rogers, W.H.; Tarlov, A.R.; McHorney, C.A.; Ware, J.E., Jr. Gender Differences in Medical Treatment: The Case of Physician–Prescribed Activity Restrictions. Soc. Sci Med. 1997, 45, 711–722. [Google Scholar] [CrossRef]
- Beijing Municipal Bureau of Statistics. Beijing Municipal Bureau of Statistics and NBS Survey Office in Beijing. Available online: http://nj.tjj.beijing.gov.cn/nj/main/2019-tjnj/zk/indexeh.htm (accessed on 24 January 2019).
- Bhasin, H. Observation Methods–Definition, Types, Examples, Advantages. Available online: https://www.marketing91.com/observation-method/ (accessed on 5 March 2020).
- Kabir, S.M.S. Methods of Data Collection; Zenodo: Mayrin, Switzerland, 2018. [Google Scholar] [CrossRef]
- QuetionPro. Questionnaires: The Ultimate Guide, Samples & Examples. Available online: https://www.questionpro.com/blog/what-is-a-questionnaire/ (accessed on 1 January 2022).
- Merriam Webster Dictionary, Dictionary Definition. Available online: https://www.merriam-webster.com/dictionary/interview (accessed on 16 February 2016).
- Ni, J. Spatial Distribution Characteristics of Healthcare Facilities in Nanjing: Network Point Pattern Analysis and Correlation Analysis. Int. J. Environ. Res. Public Health 2016, 13, 833. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Age-Friendly Cities: A Guide; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Office of the Victorian Government Architect. The Case for Good Design: Healthcare. Available online: https://www.ovga.vic.gov.au/case-good-design-healthcare-guide-government (accessed on 16 January 2022).
- University of Washington. How to Make Healthcare Accessible for All. Aging Well with a Physical Disability Factsheet Series. Available online: https://agerrtc.washington.edu/info/factsheets/healthaccess#improveaccess (accessed on 31 December 2017).
- Harvard University. Women and Health Initiative. Available online: https://www.hsph.harvard.edu/women-and-health-initiative/projects/ (accessed on 16 January 2022).
- Bhatt, J.D.; Bathija, P. Ensuring Access to Quality Health Care in Vulnerable Communities. Acad. Med. 2018, 93, 1271–1275. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine. Health-Care Utilization as a Proxy in Disability Determination; National Academies Press: Washington, DC, USA, 2018. [Google Scholar]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Name | Area (m2) | Service Targets | ||
|---|---|---|---|---|---|
| Community Area (km2) | Households | Population | |||
| 1 | Yuetan Health Center | 2380 | 1.19 | 19,630 | 33,528 |
| 2 | Yiqu Health Center | 840 | 0.71 | 5860 | 21,474 |
| 3 | Erqu Health Center | 259 | 0.49 | 4056 | 13,562 |
| 4 | Muxidi Health Center | 689 | 0.42 | 3584 | 15,290 |
| 5 | Fuwai Health Center | 120 | |||
| 6 | Shehuilu Health Center | 183 | 0.28 | 3983 | 12,441 |
| 7 | Nanshagou Health Center | 120 | 0.1 | 474 | 1292 |
| 8 | Fubei Health Center | 360 | 0.61 | 4611 | 17,029 |
| 9 | Jingan Health Center | 224 | 0.16 | 2584 | 7196 |
| 10 | Qinan Health Center | 160 | |||
| 11 | Railway Health Center | 800 | 0.15 | 3623 | 11,626 |
| total | 6135 | 4.11 | 48,405 | 121,812 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y. Access to Healthcare Facilities and Women’s Healthcare Requirements in Urban Areas: A Case Study of Beijing. Int. J. Environ. Res. Public Health 2022, 19, 3709. https://doi.org/10.3390/ijerph19063709
Zhang Y. Access to Healthcare Facilities and Women’s Healthcare Requirements in Urban Areas: A Case Study of Beijing. International Journal of Environmental Research and Public Health. 2022; 19(6):3709. https://doi.org/10.3390/ijerph19063709
Chicago/Turabian StyleZhang, Yingyi. 2022. "Access to Healthcare Facilities and Women’s Healthcare Requirements in Urban Areas: A Case Study of Beijing" International Journal of Environmental Research and Public Health 19, no. 6: 3709. https://doi.org/10.3390/ijerph19063709
APA StyleZhang, Y. (2022). Access to Healthcare Facilities and Women’s Healthcare Requirements in Urban Areas: A Case Study of Beijing. International Journal of Environmental Research and Public Health, 19(6), 3709. https://doi.org/10.3390/ijerph19063709