
Awareness and Perceptions among Members of a Japanese Cancer Patient Advocacy Group Concerning the Financial Relationships between the Pharmaceutical Industry and Physicians

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
Study Aims
2. Methods
2.1. Study Setting, Design, and Respondents
2.2. Data Collection
2.3. Survey Sheet
2.4. Data Analysis
2.5. Ethics Approval
3. Results
3.1. Respondents
3.2. Quantitative Findings
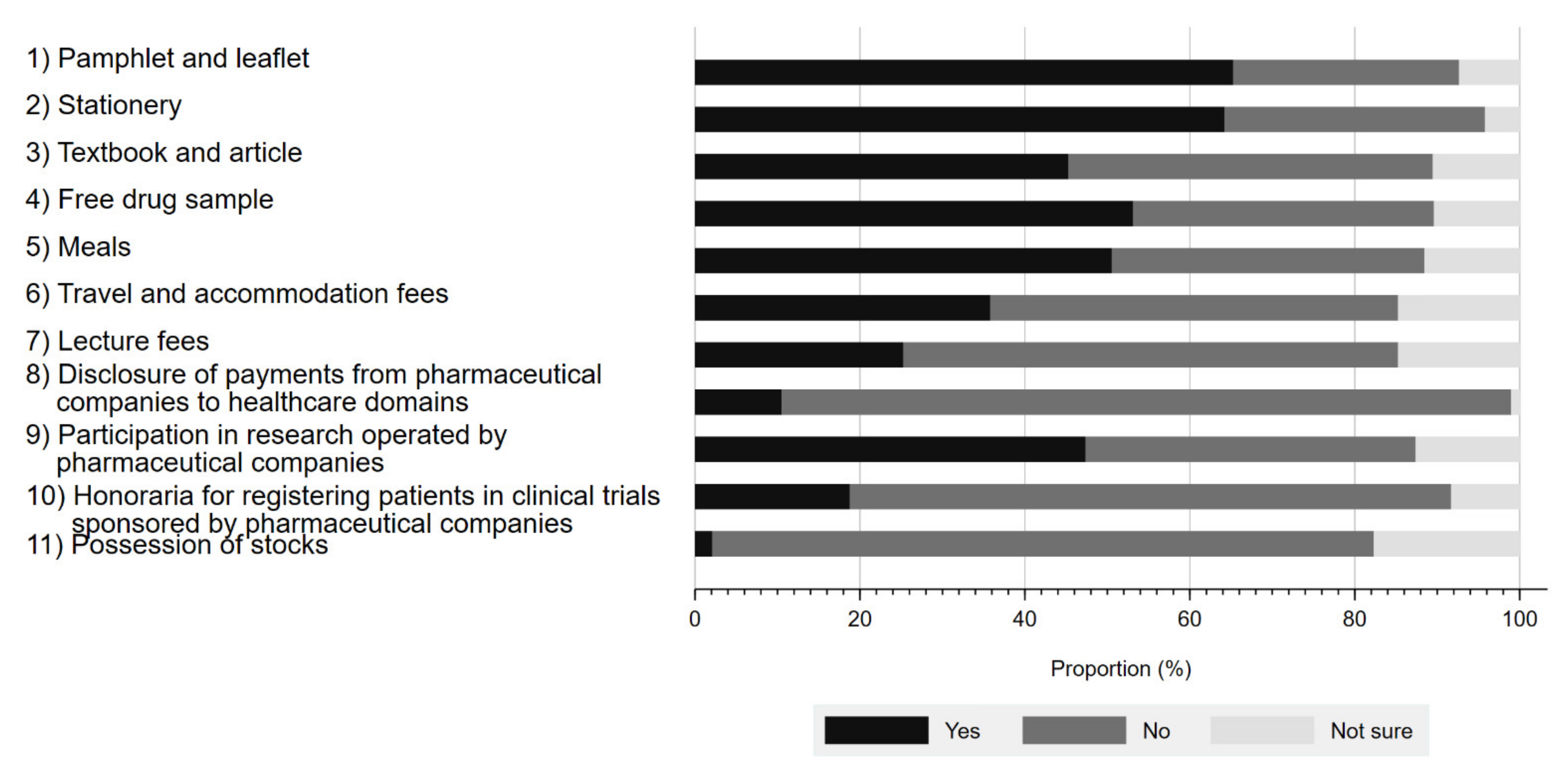
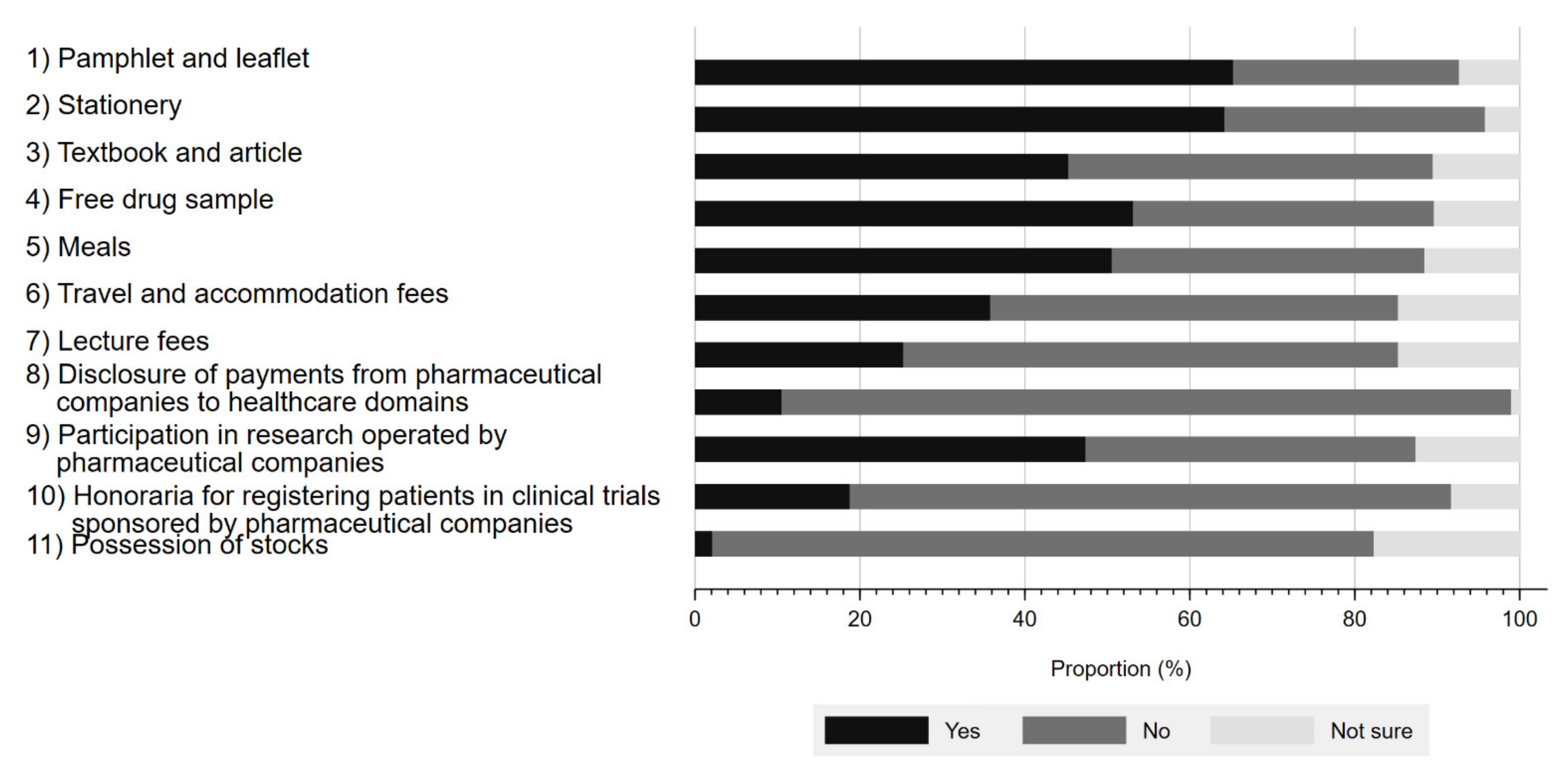
3.2.1. Awareness of Physician–Pharma Interactions
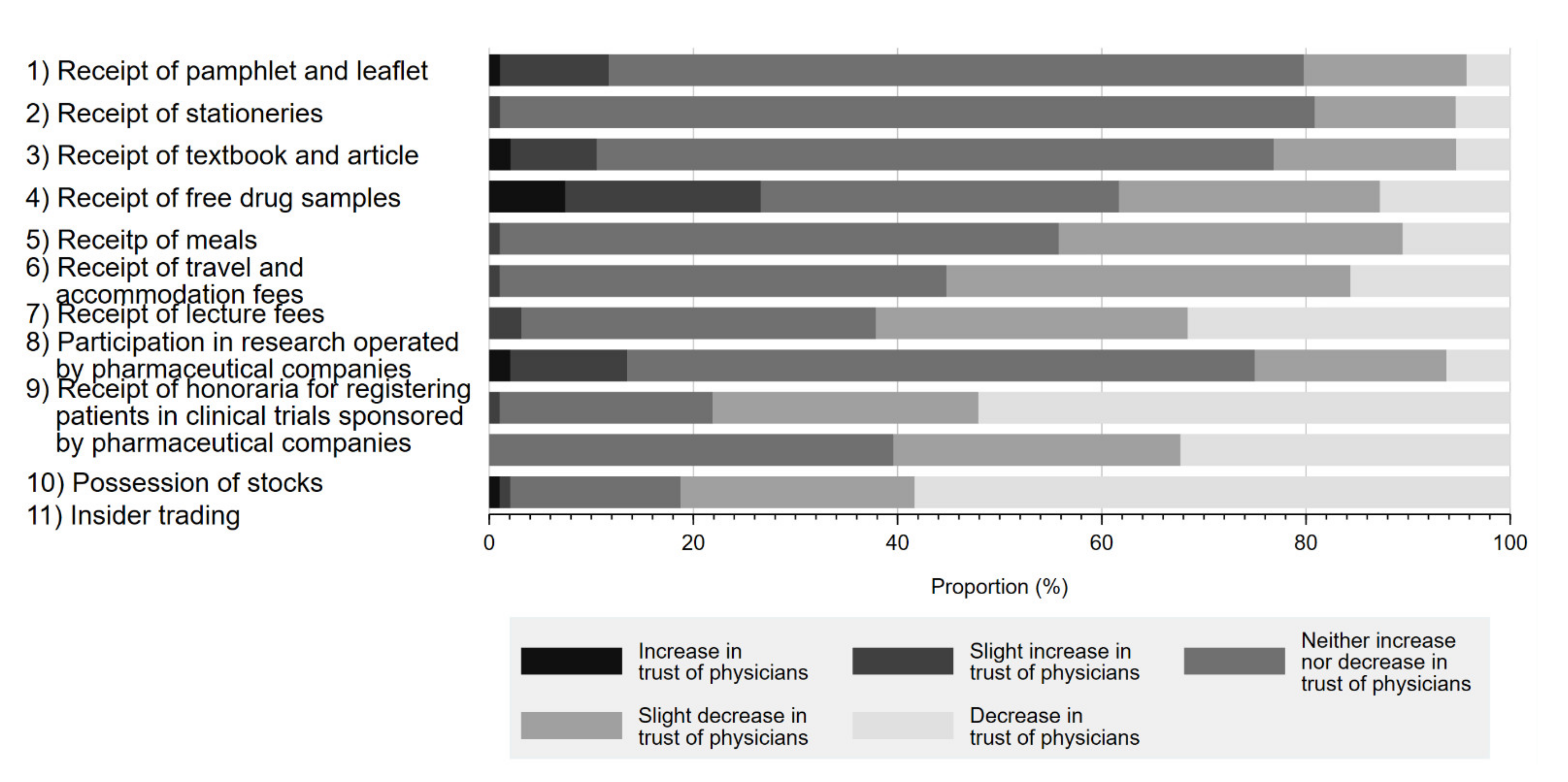
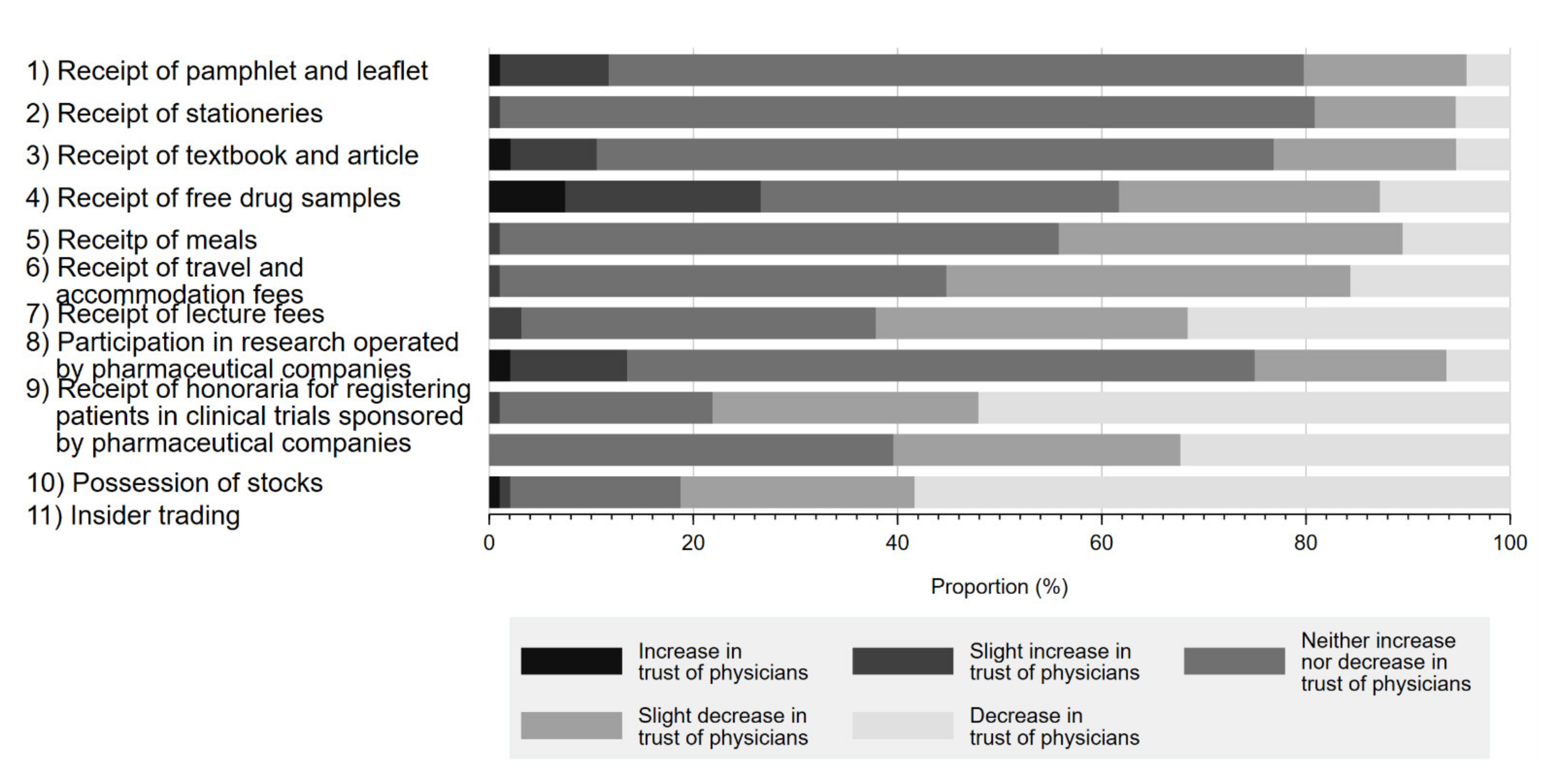
3.2.2. Influence of Physician–Pharma Interactions on Trust in Physicians
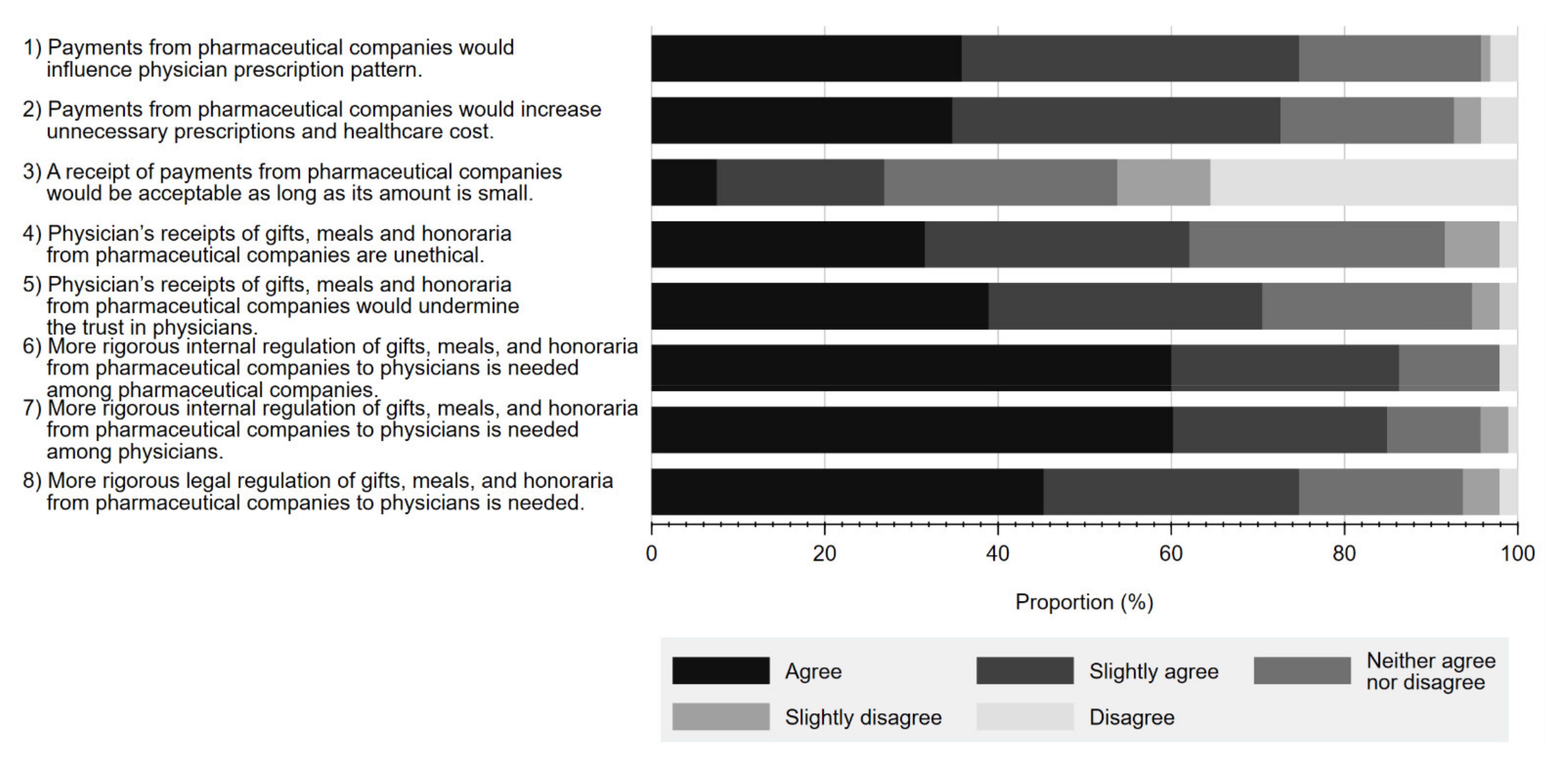
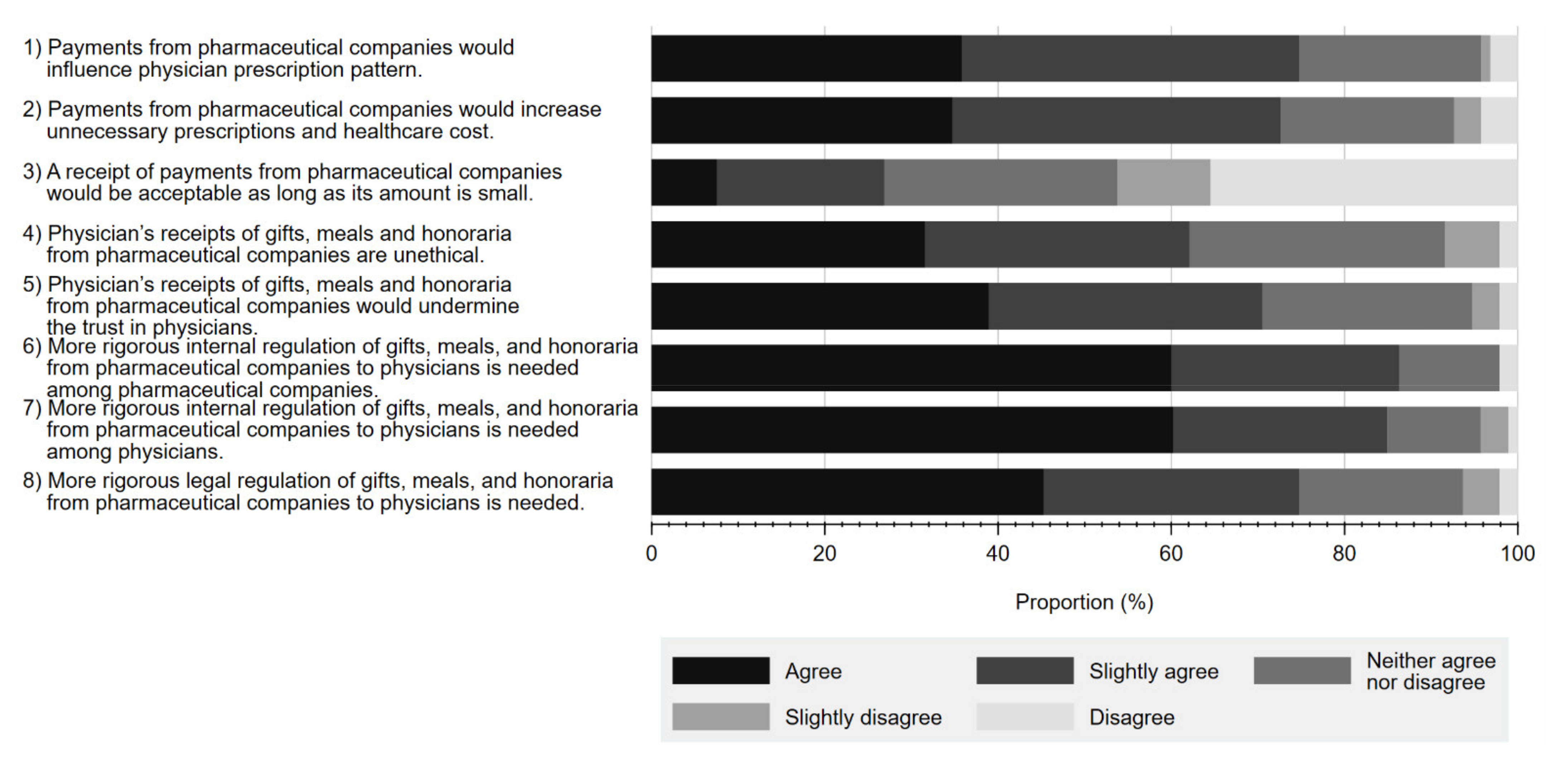
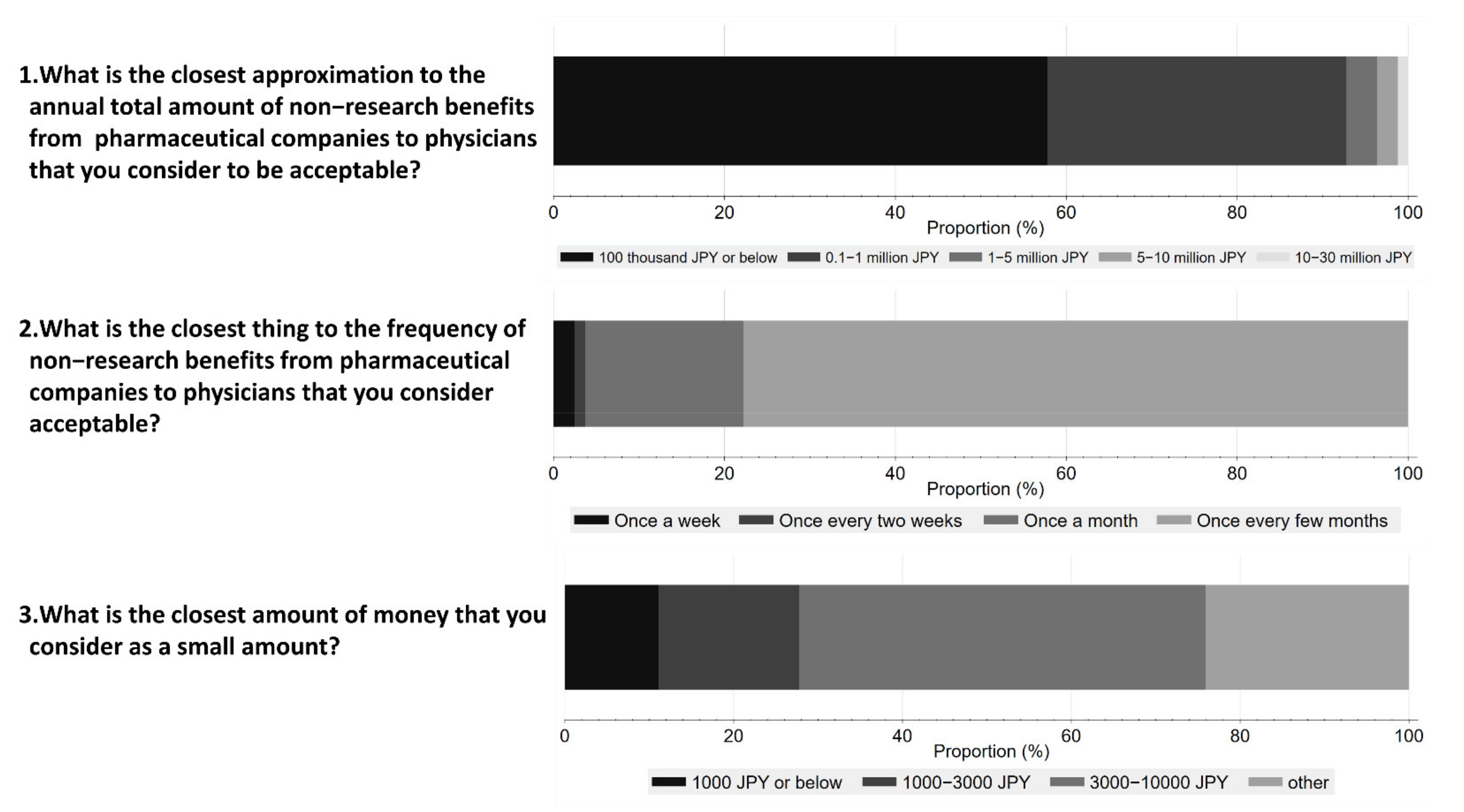
3.2.3. Perception on Physician–Pharma Interactions
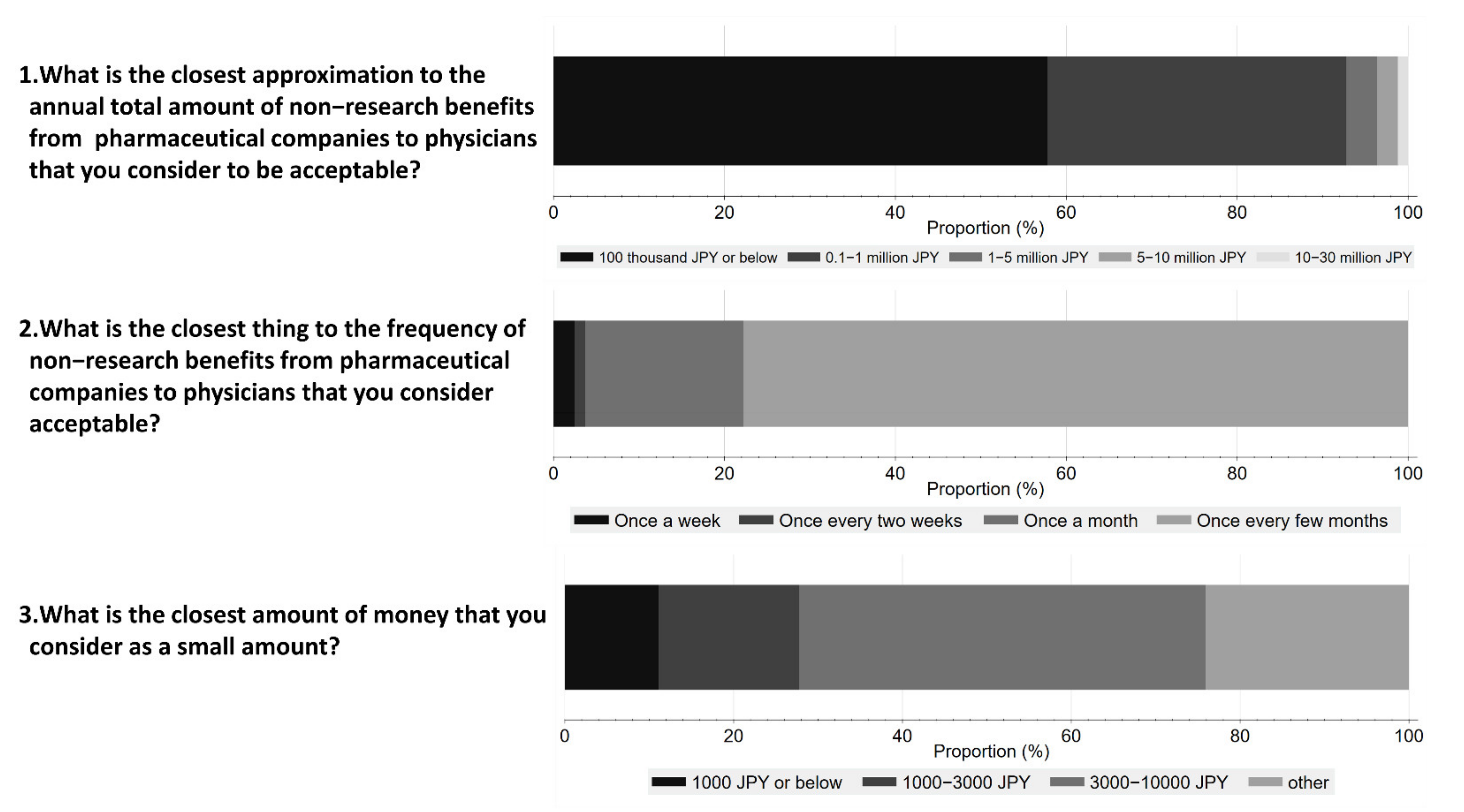
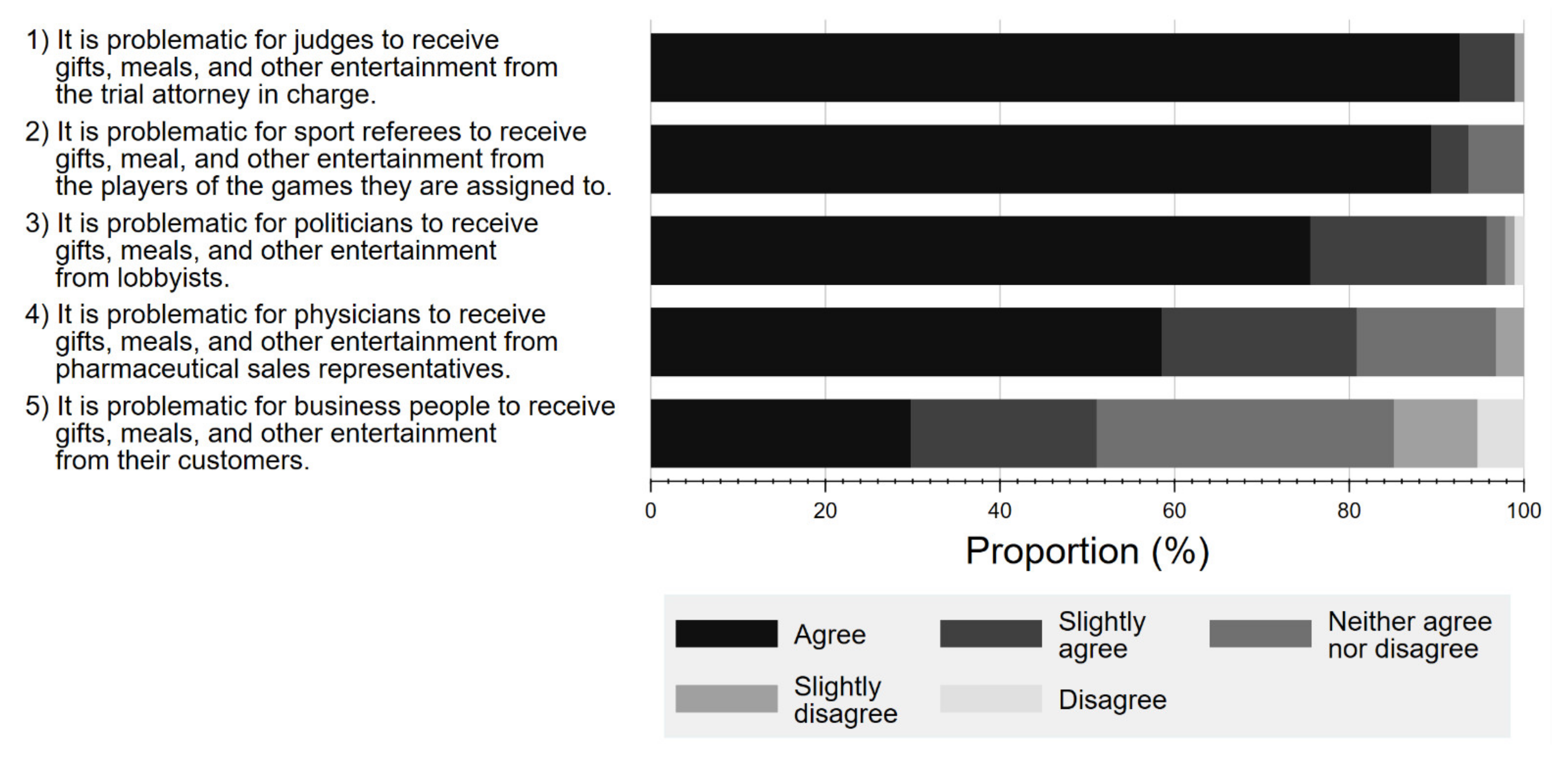
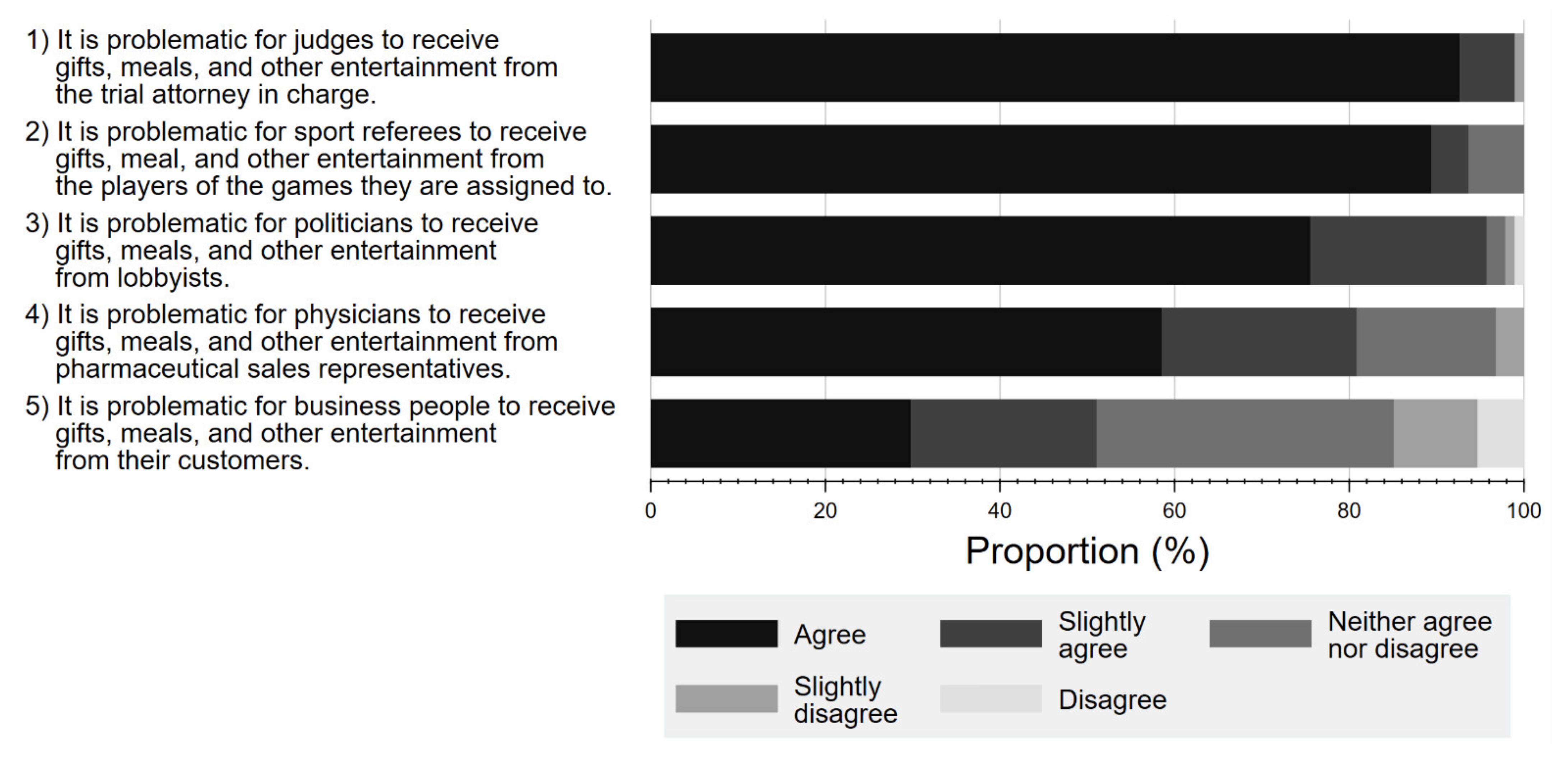
3.2.4. Attitude towards Various Professional FCOI
3.3. Qualitative Findings of Open-Ended Responses
- Theme 1: Perception towards the FCOI
- Theme 2: Concerns about the respondent’s treatment
- Theme 3: Reasons of physician–Pharma interactions
- Theme 4: Possible solutions from the patient perspective
4. Discussion
4.1. RQ1. Awareness of Physician–Pharma Interactions
4.2. RQ2. Impacts of Physician–Pharma Interactions on Trust in Physicians
4.3. RQ3. Perception on Physician–Pharma Interactions
5. Clinical Implementation
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- Ozaki, A.; Saito, H.; Senoo, Y.; Sawano, T.; Shimada, Y.; Kobashi, Y.; Yamamoto, K.; Suzuki, Y.; Tanimoto, T. Overview and transparency of non-research payments to healthcare organizations and healthcare professionals from pharmaceutical companies in Japan: Analysis of payment data in 2016. Health Policy 2020, 124, 727–735. [Google Scholar] [CrossRef] [PubMed]
- Fickweiler, F.; Fickweiler, W.; Urbach, E. Interactions between physicians and the pharmaceutical industry generally and sales representatives specifically and their association with physicians’ attitudes and prescribing habits: A systematic review. Br. Med. J. Open 2017, 7, e016408. [Google Scholar] [CrossRef] [Green Version]
- Ozieranski, P.; Csanadi, M.; Rickard, E.; Tchilingirian, J.; Mulinari, S. Analysis of Pharmaceutical Industry Payments to UK Health Care Organizations in 2015. JAMA Netw. Open 2019, 2, e196253. [Google Scholar] [CrossRef] [PubMed]
- Goupil, B.; Balusson, F.; Naudet, F.; Esvan, M.; Bastian, B.; Chapron, A.; Frouard, P. Association between gifts from pharmaceutical companies to French general practitioners and their drug prescribing patterns in 2016: Retrospective study using the French Transparency in Healthcare and National Health Data System databases. Br. Med. J. 2019, 367, l6015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brax, H.; Fadlallah, R.; Al-Khaled, L.; Kahale, L.A.; Nas, H.; El-Jardali, F.; Akl, E.A. Association between physicians’ interaction with pharmaceutical companies and their clinical practices: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0175493. [Google Scholar] [CrossRef] [PubMed]
- What Is Patient-Centered Care? NEJM Catalyst. 2017. Available online: https://catalyst.nejm.org/doi/full/10.1056/CAT.17.0559 (accessed on 10 March 2022).
- Institute of Medicine. Conflict of Interest in Medical Research, Education, and Practice; The National Academies Press: Washington, DC, USA, 2009; p. 436. [Google Scholar]
- Moynihan, R.; Bero, L.; Hill, S.; Johansson, M.; Lexchin, J.; Macdonald, H.; Mintzes, B.; Pearson, C.; Rodwin, M.A.; Stavdal, A.; et al. Pathways to independence: Towards producing and using trustworthy evidence. Br. Med. J. 2019, 367, l6576. [Google Scholar] [CrossRef] [Green Version]
- Kanter, G.P.; Loewenstein, G. Evaluating Open Payments. JAMA 2019, 322, 401. [Google Scholar] [CrossRef]
- Santhakumar, S.; Adashi, E.Y. The Physician Payment Sunshine Act: Testing the Value of Transparency. JAMA 2015, 313, 23–24. [Google Scholar] [CrossRef] [PubMed]
- Stein, G.E.; Kamler, J.J.; Chang, J.S. Ophthalmology Patient Perceptions of Open Payments Information. JAMA Ophthalmol. 2018, 136, 1375–1381. [Google Scholar] [CrossRef] [Green Version]
- Stoll, M.; Hubenschmid, L.; Koch, C.; Lieb, K. Voluntary disclosures of payments from pharmaceutical companies to healthcare professionals in Germany: A descriptive study of disclosures in 2015 and 2016. Br. Med. J. Open 2020, 10, e037395. [Google Scholar] [CrossRef]
- Napierala, H.; Schäfer, L.; Schott, G.; Schurig, N.; Lempert, T. Management of financial conflicts of interests in clinical practice guidelines in Germany: Results from the public database GuidelineWatch. BMC Med. Ethics 2018, 19, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mulinari, S.; Ozieranski, P. Disclosure of payments by pharmaceutical companies to healthcare professionals in the UK: Analysis of the Association of the British Pharmaceutical Industry’s Disclosure UK database, 2015 and 2016 cohorts. Br. Med. J. Open 2018, 8, e023094. [Google Scholar] [CrossRef] [PubMed]
- Adlington, K.; Godlee, F. Disclosure UK: Transparency should no longer be an optional extra. Br. Med. J. 2016, 354, i3730. [Google Scholar] [CrossRef] [PubMed]
- Ozieranski, P.; Rickard, E.; Mulinari, S. Exposing drug industry funding of UK patient organizations. Br. Med. J. 2019, 365, l1806. [Google Scholar] [CrossRef] [Green Version]
- Medicines Australia. Transparency Reporting. Available online: https://www.disclosureaustralia.com.au/search/ (accessed on 28 October 2020).
- Pokorny, A.M.J.; Bero, L.A.; Moynihan, R.; Mintzes, B.J. Industry payments to Australian medical oncologists and clinical haematologists: A cross-sectional analysis of publicly available disclosures. Intern. Med. J. 2020, 51, 1816–1824. [Google Scholar] [CrossRef]
- Sawano, T.; Ozaki, A.; Saito, H.; Shimada, Y.; Tanimoto, T. Pharmaceutical Company Payments to Japanese Government Drug Regulation Committee Members. Clin. Pharmacol. Ther. 2020, 108, 1049–1054. [Google Scholar] [CrossRef]
- Murayama, A.; Ozaki, A.; Saito, H.; Sawano, T.; Shimada, Y.; Yamamoto, K.; Suzuki, Y.; Tanimoto, T. Pharmaceutical company payments to dermatology Clinical Practice Guideline authors in Japan. PLoS ONE 2020, 15, e0239610. [Google Scholar] [CrossRef]
- Kanter, G.P.; Carpenter, D.; Lehmann, L.; Mello, M.M. Effect of the public disclosure of industry payments information on patients: Results from a population-based natural experiment. Br. Med. J. Open 2019, 9, e024020. [Google Scholar] [CrossRef] [Green Version]
- Hampson, L.A.; Agrawal, M.; Joffe, S.; Gross, C.P.; Verter, J.; Emanuel, E.J. Patients’ Views on Financial Conflicts of Interest in Cancer Research Trials. N. Engl. J. Med. 2006, 355, 2330–2337. [Google Scholar] [CrossRef]
- Pham-Kanter, G.; Mello, M.M.; Lehmann, L.S.; Campbell, E.G.; Carpenter, D. Public Awareness of and Contact with Physicians Who Receive Industry Payments: A National Survey. J. Gen. Intern. Med. 2017, 32, 767–774. [Google Scholar] [CrossRef]
- Kanter, G.P.; Carpenter, D.; Lehmann, L.S.; Mello, M.M. US Nationwide Disclosure of Industry Payments and Public Trust in Physicians. JAMA Netw. Open 2019, 2, e191947. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayyar, B.V.; Arora, S.; O’Kennedy, R. Coming-of-Age of Antibodies in Cancer Therapeutics. Trends Pharmacol. Sci. 2016, 37, 1009–1028. [Google Scholar] [CrossRef] [PubMed]
- Lagassé, H.A.D.; Alexaki, A.; Simhadri, V.L.; Katagiri, N.H.; Jankowski, W.; Sauna, Z.E.; Kimchi-Sarfaty, C. Recent advances in (therapeutic protein) drug development. F1000Research 2017, 6, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tay-Teo, K.; Ilbawi, A.; Hill, S.R. Comparison of Sales Income and Research and Development Costs for FDA-Approved Cancer Drugs Sold by Originator Drug Companies. JAMA Netw. Open 2019, 2, e186875. [Google Scholar] [CrossRef] [PubMed]
- Aitken, M.; Kleinrock, M.; Simorellis, A.; Nass, D. The Global Use of Medicine in 2019 and Outlook to 2023; IQVIA: Durham, NC, USA, 2019. [Google Scholar]
- Fuji Keizai Management Co. Ltd. Ethical Pharmaceutical Data Book 2018–2019; Fuji Keizai Management Co. Ltd.: Tokyo, Japan, 2019. [Google Scholar]
- Japan Pharmaceutical Manufacturers Association. Transparency Guideline for the Relation between Corporate Activities and Medical Institutions. Available online: http://www.jpma.or.jp/english/policies_guidelines/transparency_guideline.html (accessed on 14 December 2020). (In Japanese).
- Tansa; Medical Governance Research Institute. Money for Docs Database. Available online: https://db.tansajp.org/en (accessed on 22 September 2021).
- Saito, H.; Ozaki, A.; Kobayashi, Y.; Sawano, T.; Tanimoto, T. Pharmaceutical Company Payments to Executive Board Members of Professional Medical Associations in Japan. JAMA Intern. Med. 2019, 179, 578–580. [Google Scholar] [CrossRef]
- Ozaki, A.; Saito, H.; Onoue, Y.; Sawano, T.; Shimada, Y.; Somekawa, Y.; Tsuji, A.; Tanimoto, T. Pharmaceutical payments to certified oncology specialists in Japan in 2016: A retrospective observational cross-sectional analysis. Br. Med. J. Open 2019, 9, e028805. [Google Scholar] [CrossRef] [Green Version]
- Saito, H.; Ozaki, A.; Sawano, T.; Shimada, Y.; Tanimoto, T. Evaluation of Pharmaceutical Company Payments and Conflict of Interest Disclosures Among Oncology Clinical Practice Guideline Authors in Japan. JAMA Netw. Open 2019, 2, e192834. [Google Scholar] [CrossRef]
- Hillen, M.A.; Medendorp, N.M.; Daams, J.G.; Smets, E.M. Patient-Driven Second Opinions in Oncology: A Systematic Review. Oncologist 2017, 22, 1197–1211. [Google Scholar] [CrossRef] [Green Version]
- Ammous, A.; Eddine, S.B.Z.; Dani, A.; Dbaibou, J.; El-Asmar, J.M.; Sadder, L.; Akl, E.A. Awareness and attitudes of the Lebanese population with regard to physician–pharmaceutical company interaction: A survey study. Br. Med. J. Open 2017, 7, e013041. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Center, Center for Cancer Control and Information Services. Summary Report of Hospital-Based Cancer Registry in 2018; National Cancer Center: Tokyo, Japan, 2018.
- Hulin, C.; Netemeyer, R.; Cudeck, R. Can a Reliability Coefficient Be Too High? J. Consum. Psychol. 2001, 10, 55–58. [Google Scholar]
- Green, M.J.; Masters, R.; James, B.; Simmons, B.; Lehman, E. Do gifts from the pharmaceutical industry affect trust in physicians? Fam. Med. 2012, 44, 325–331. [Google Scholar] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Hori, M.; Matsuda, T.; Shibata, A.; Katanoda, K.; Sobue, T.; Nishimoto, H. Cancer incidence and incidence rates in Japan in 2009: A study of 32 population-based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn. J. Clin. Oncol. 2015, 45, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Fadlallah, R.; Nas, H.; Naamani, D.; El-Jardali, F.; Hammoura, I.; Al-Khaled, L.; Brax, H.; Kahale, L.; Akl, E.A. Knowledge, Beliefs and Attitudes of Patients and the General Public towards the Interactions of Physicians with the Pharmaceutical and the Device Industry: A Systematic Review. PLoS ONE 2016, 11, e0160540. [Google Scholar] [CrossRef] [Green Version]
- Lopez, J.; Naved, B.A.; Pradeep, T.; Pineault, K.; Purvis, T.; Macmillan, A.; Slezak, S.; May, J.W.J.; Dorafshar, A.H. What Do Plastic Surgery Patients Think of Financial Conflicts of Interest and the Sunshine Act? Ann. Plast. Surg. 2019, 82, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Jastifer, J.; Roberts, S. Patients’ Awareness of and Attitudes toward Gifts from Pharmaceutical Companies to Physicians. Int. J. Health Serv. 2009, 39, 405–414. [Google Scholar] [CrossRef]
- Sawano, T.; Ozaki, A.; Saito, H.; Shimada, Y.; Tanimoto, T. Payments from Pharmaceutical Companies to Authors Involved in the Valsartan Scandal in Japan. JAMA Netw. Open 2019, 2, e193817. [Google Scholar] [CrossRef] [Green Version]
- Blake, R.L.; Early, E.K. Patients’ attitudes about gifts to physicians from pharmaceutical companies. J. Am. Board Fam. Pract. 1995, 8, 457–464. [Google Scholar]
- Mainous, A.G., 3rd; Hueston, W.J.; Rich, E.C. Patient perceptions of physician acceptance of gifts from the pharmaceutical industry. Arch. Fam. Med. 1995, 4, 335–339. [Google Scholar] [CrossRef]
- Saito, H.; Ozaki, A.; Sawano, T.; Shimada, Y.; Yamamoto, K.; Suzuki, Y.; Tanimoto, T. Pharmaceutical Company Payments to the Professors of Orthopaedic Surgery Departments in Japan. J. Bone Jt. Surg. 2020, 102, e39. [Google Scholar] [CrossRef] [PubMed]
- Saito, H.; Tani, Y.; Ozaki, A.; Sawano, T.; Shimada, Y.; Yamamoto, K.; Tanimoto, T. Financial ties between authors of the clinical practice guidelines and pharmaceutical companies: An example from Japan. Clin. Microbiol. Infect. 2019, 25, 1304–1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harada, K.; Ozaki, A.; Saito, H.; Sawano, T.; Yamamoto, K.; Murayama, A.; Senoo, Y.; Tanimoto, T. Financial payments made by pharmaceutical companies to the authors of Japanese hematology clinical practice guidelines between 2016 and 2017. Health Policy 2020, 125, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.G.; DiPaola, C.P.; Noonan, V.K.; Bailey, C.; Dvorak, M.F.S. Physician-industry conflict of interest: Public opinion regarding industry-sponsored research. J. Neurosurg. Spine 2012, 17, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiPaola, C.P.; Dea, N.; Noonan, V.K.; Bailey, C.S.; Dvorak, M.F.; Fisher, C.G. Surgeon-industry conflict of interest: Survey of North Americans’ opinions regarding surgeons consulting with industry. Spine J. 2014, 14, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Melander, H.; Ahlqvist-Rastad, J.; Meijer, G.; Beermann, B. Evidence b(i)ased medicine—Selective reporting from studies sponsored by pharmaceutical industry: Review of studies in new drug applications. Br. Med. J. 2003, 326, 1171–1173. [Google Scholar] [CrossRef] [Green Version]
- Lexchin, J.; Bero, L.; Djulbegovic, B.; Clark, O. Pharmaceutical industry sponsorship and research outcome and quality: Systematic review. Br. Med. J. 2003, 326, 1167–1170. [Google Scholar] [CrossRef] [Green Version]
- Mullard, A. Mediator scandal rocks French medical community. Lancet 2011, 377, 890–892. [Google Scholar] [CrossRef]
- Holbrook, A.; Lexchin, J.; Pullenayegum, E.; Campbell, C.; Marlow, B.; Troyan, S.; Weijer, C.; Blackmer, J.; Brazil, K.; Willison, D. What do Canadians think about physician-pharmaceutical industry interactions? Health Policy 2013, 112, 255–263. [Google Scholar] [CrossRef]
- Niforatos, J.D.; Chaitoff, A.; Mercer, M.B.; Yu, P.-C.; Rose, S.L. Association Between Public Trust and Provider Specialty Among Physicians with Financial Conflicts of Interest. Mayo Clin. Proc. 2019, 94, 2467–2475. [Google Scholar] [CrossRef]
- Gidman, W.; Ward, P.; McGregor, L. Understanding public trust in services provided by community pharmacists relative to those provided by general practitioners: A qualitative study. Br. Med. J. Open 2012, 2, e000939. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ward, P.; Coates, A. ‘We shed tears, but there is no one there to wipe them up for us’: Narratives of (mis)trust in a materially deprived community. Health 2006, 10, 283–301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, M.A.; Dugan, E.; Zheng, B.; Mishra, A.K. Trust in Physicians and Medical Institutions: What Is It, Can It Be Measured, and Does It Matter? Milbank Q. 2001, 79, 613–639. [Google Scholar] [CrossRef] [Green Version]
- Luhmann, N. Trust: A Mechanism for the Reduction of Social Complexity. Trust and Power. In Two Works by Niklas Luhmann; John Wiley & Sons: Hoboken, NJ, USA, 1979; pp. 1–103. [Google Scholar]
- Benedict, R. The Chrysanthemum and the Sword: Patterns of Japanese Culture; Houghton Mifflin Harcourt: Boston, MA, USA, 1946. [Google Scholar]
- Yanagida, K. A Vulgar Man’s View of Life (What Ruth Benedict’s The Chrysanthemum and the Sword offers). Jpn. J. Ethnol. 1950, 14, 290–297. [Google Scholar]
- Yamamoto, K.; Murayama, A.; Ozaki, A.; Saito, H.; Sawano, T.; Tanimoto, T. Financial conflicts of interest between pharmaceutical companies and the authors of urology clinical practice guidelines in Japan. Int. Urogynecol. J. 2021, 32, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Fudman, D.; Feuerstein, J.D. The Call for Greater Transparency in Conflicts of Interest. JAMA Netw. Open 2018, 1, e186342. [Google Scholar] [CrossRef]
- Spurling, G.K.; Mansfield, P.R.; Montgomery, B.D.; Lexchin, J.; Doust, J.; Othman, N.; Vitry, A.I. Information from pharmaceutical companies and the quality, quantity, and cost of physicians’ prescribing: A systematic review. PLoS Med. 2010, 7, e1000352. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, A.P.; Trivedi, N.U.; Gennarelli, R.L.; Chimonas, S.; Tabatabai, S.M.; Goldberg, J.; Diaz, L.A., Jr.; Korenstein, D. Are Financial Payments from the Pharmaceutical Industry Associated WITH Physician Prescribing?: A Systematic Review. Ann. Intern. Med. 2020, 174, 353–361. [Google Scholar] [CrossRef]
- Wen, L. Patients can’t trust doctors’ advice if we hide our financial connections with drug companies. Br. Med. J. 2014, 348, g167. [Google Scholar] [CrossRef]
- Tattersall, M.H.; Dimoska, A.; Gan, K. Patients expect transparency in doctors’ relationships with the pharmaceutical industry. Med. J. Aust. 2009, 190, 65–68. [Google Scholar] [CrossRef]
- Edwards, D.; Ballantyne, A. Patient awareness and concern regarding pharmaceutical manufacturer interactions with doctors. Intern. Med. J. 2009, 39, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Pham-Kanter, G. Act II of the Sunshine Act. PLoS Med. 2014, 11, e1001754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozaki, A.; Murayama, A.; Saito, H.; Sawano, T.; Harada, K.; Senoo, Y.; Yamamoto, K.; Tanimoto, T. Transparency Is Not Enough: How Can We Improve the Management of Financial Conflicts of Interest between Pharma and Healthcare Sectors? Clin. Pharmacol. Ther. 2020, 110, 289–291. [Google Scholar] [CrossRef] [PubMed]
- Moynihan, R.; Fabbri, A.; Parker, L.; Bero, L. Mixed methods evaluation of workshops for citizen health advocates about financial conflicts of interests in healthcare. Br. Med. J. Open 2020, 10, e034195. [Google Scholar] [CrossRef]
- ABIM Foundation. American Board of Internal Medicine. Medical professionalism in the new millennium: A physician charter. Ann. Intern. Med. 2002, 136, 243–246. [Google Scholar] [CrossRef]
- Saito, S.; Maeno, T.; Miyata, Y.; Maeno, T. Medical students’ attitudes toward interactions with the pharmaceutical industry: A national survey in Japan. BMC Med. Educ. 2018, 18, 286. [Google Scholar] [CrossRef] [Green Version]
- Evans, D.V.; Desnick, L.; Keys, T. Pharma Exposure Occurs Early in Training and More Often in Rural Clinical Sites. Acad. Med. 2016, 91, 9. [Google Scholar] [CrossRef]
- Fitz, M.M.; Homan, D.; Reddy, S.; Griffith, C.H.; Baker, E.; Simpson, K.P. The Hidden Curriculum: Medical Students’ Changing Opinions toward the Pharmaceutical Industry. Acad. Med. 2007, 82, S1–S3. [Google Scholar] [CrossRef]
- Saito, S.; Mukohara, K.; Bito, S. Japanese Practicing Physicians’ Relationships with Pharmaceutical Representatives: A National Survey. PLoS ONE 2010, 5, e12193. [Google Scholar] [CrossRef]
- Cain, D.M.; Detsky, A.S. Everyone’s a Little Bit Biased (Even Physicians). JAMA 2008, 299, 2893–2895. [Google Scholar] [CrossRef]
- Lea, D.; Spigset, O.; Slørdal, L. Norwegian medical students’ attitudes towards the pharmaceutical industry. Eur. J. Clin. Pharmacol. 2010, 66, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Iezzoni, L.I.; Rao, S.R.; Desroches, C.M.; Vogeli, C.; Campbell, E.G. Survey Shows That At Least Some Physicians Are Not Always Open or Honest with Patients. Health Aff. 2012, 31, 383–391. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Maeno, T.; Miyata, Y.; Maeno, T. Follow-up survey of Japanese medical students’ interactions with the pharmaceutical industry. PLoS ONE 2018, 13, e0206543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montastruc, F.; Moulis, G.; Palmaro, A.; Gardette, V.; Durrieu, G.; Montastruc, J.-L. Interactions between Medical Residents and Drug Companies: A National Survey after the Mediator® Affair. PLoS ONE 2014, 9, e104828. [Google Scholar] [CrossRef]
- Hodges, B. Interactions with the pharmaceutical industry: Experiences and attitudes of psychiatry residents, interns and clerks. Can. Med. Assoc. J. 1995, 153, 553–559. [Google Scholar]
- Inoue, K.; Figueroa, J.F.; Orav, E.J.; Tsugawa, Y. Association between industry payments for opioid products and physicians’ prescription of opioids: Observational study with propensity-score matching. J. Epidemiol. Community Health 2020, 74, 647–654. [Google Scholar] [CrossRef]
- Civaner, M.M. A follow-up study on the effects of an educational intervention against pharmaceutical promotion. PLoS ONE 2020, 15, e0240713. [Google Scholar] [CrossRef]
- Austad, K.; Avorn, J.; Kesselheim, A.S. Medical Students’ Exposure to and Attitudes about the Pharmaceutical Industry: A Systematic Review. PLoS Med. 2011, 8, e1001037. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | |
|---|---|
| Gender, N (%) | |
| Male | 63 (67.7) |
| Female | 30 (32.3) |
| Missing | 3 |
| Age category, N (%) | |
| ≦60 | 15 (16.0) |
| 61–70 | 30 (31.9) |
| 71–80 | 38 (40.4) |
| 81–90 | 11 (11.7) |
| Missing | 2 |
| Annual family income, N (%) | |
| <JPY 2 million (<USD 18,349) | 6 (7.0) |
| JPY 2–4 million (USD 18,349–36,697) | 40 (46.5) |
| JPY 4–6 million (USD 36,697–55,046) | 14 (16.3) |
| JPY 6–8 million (USD 55,046–73,394) | 12 (14.0) |
| JPY 8–10 million (USD 73,394–91,743) | 5 (5.8) |
| >JPY 10 million (>USD 91,743) | 9 (10.5) |
| Missing | 10 |
| Type of business, N (%) | |
| Unemployed | 52 (55.9) |
| Self-employed | 15 (16.1) |
| Full-time job | 11 (11.8) |
| Part-time job | 7 (7.5) |
| Other | 8 (8.6) |
| Missing | 3 |
| Educational background, N (%) | |
| Less than high school graduate | 1 (1.1) |
| High school graduate | 27 (29.0) |
| Associate degree or diploma | 15 (16.1) |
| Bachelor’s degree or more (bachelor, master, and doctoral degree) | 50 (53.8) |
| Missing | 3 |
| Type of cancer, N (%) | |
| Not cancer patient | 20 (22.5) |
| Prostate cancer | 24 (27.0) |
| Lung cancer | 5 (5.6) |
| Breast cancer | 5 (5.6) |
| Colorectal cancer | 4 (4.5) |
| Gastric cancer | 4 (4.5) |
| Other type of cancer | 27 (30.3) |
| Missing | 7 |
| Cancer’s stage, N (%) * | |
| Stage 1 | 23 (35.9) |
| Stage 2 | 16 (25.0) |
| Stage 3 | 10 (15.6) |
| Stage 4 | 5 (7.7) |
| Unclear | 10 (15.6) |
| Missing | 5 |
| Year of diagnosis, N (%) * | |
| 2018 | 4 (5.8) |
| 2017 | 6 (8.7) |
| 2016 | 3 (4.4) |
| 2015 | 4 (5.8) |
| Before 2015 | 52 (75.4) |
| Hospital, N (%) * | |
| Cancer hospital | 20 (29.4) |
| National university | 9 (13.2) |
| Private university | 9 (13.2) |
| National municipal hospital | 10 (14.7) |
| Private municipal hospital | 11 (16.2) |
| Other hospital | 9 (13.2) |
| Missing | 1 |
| Previous cancer recurrence * | |
| Yes | 13 (20.0) |
| No | 47 (72.3) |
| Not clear | 5 (7.7) |
| Missing | 4 |
| Count of previous cancer reoccurrence, N (%) | |
| 1 | 6 (42.9) |
| 2 | 2 (14.3) |
| 3 | 1 (7.1) |
| 6 | 1 (7.1) |
| 7 | 1 (7.1) |
| 10 | 1 (7.1) |
| Unknown | 2 (14.3) |
| Treatment which you have ever had, N (%) *, ** | |
| Anticancer drug | 22 (16.5) |
| Molecularly targeted drug | 5 (3.8) |
| Hormone therapy | 23 (17.3) |
| Radiation therapy | 37 (27.8) |
| Surgery | 39 (29.3) |
| Other | 4 (3.0) |
| Never | 3 (2.3) |
| Treatment which you have now, N (%) *, ** | |
| Anticancer drug | 2 (2.9) |
| Molecularly targeted drug | 2 (2.9) |
| Hormone therapy | 10 (14.5) |
| Radiation therapy | 2 (2.9) |
| Other | 11 (15.9) |
| Not having | 42 (60.9) |
| Variables | Number (%) | p-Value | |
|---|---|---|---|
| Aware | Unaware or Not Sure | ||
| Gender | |||
| Male | 49 (77.8) | 14 (22.2) | 0.053 |
| Female | 28 (93.3) | 2 (6.7) | |
| Age category | |||
| ≤60 | 13 (86.7) | 2 (13.3) | 0.879 |
| 61–70 | 24 (80.0) | 6 (20.0) | |
| ≥71 | 39 (79.6) | 10 (20.4) | |
| Income | |||
| Lower income (<JPY 4 million (<USD 36,697)) | 39 (84.8) | 7 (15.2) | 0.129 |
| Higher income (≥JPY 4 million (≥USD 36,697)) | 29 (72.5) | 11 (27.5) | |
| Job | |||
| Employed | 30 (81.1) | 7 (18.9) | 0.576 |
| Unemployed | 45 (80.4) | 11 (19.6) | |
| Education | |||
| High school graduate or less | 21 (75.0) | 7 (25.0) | 0.264 |
| Associate degree or more | 54 (83.1) | 11 (16.9) | |
| Cancer | |||
| Non-cancer respondents | 17 (85.0) | 3 (15.0) | 0.433 |
| Cancer patients | 55 (79.7) | 14 (20.3) | |
| Cancer stage 1 | |||
| 1 | 17 (73.9) | 6 (26.1) | 0.287 |
| 2–4 | 26 (83.9) | 5 (16.1) | |
| Year 1 | |||
| 2015–2018 | 15 (88.2) | 2 (11.8) | 0.320 |
| Before 2015 | 41 (78.9) | 11 (21.1) | |
| Hospital 1 | |||
| Other hospitals | 24 (80.0) | 6 (20.0) | 0.555 |
| Cancer special hospitals | 31 (81.6) | 7 (18.4) | |
| Previous cancer recurrence 1 | |||
| No or other | 41 (78.9) | 11 (21.1) | 0.246 |
| Yes | 12 (92.3) | 1 (7.7) | |
| Experience with pharmacotherapy 1 | |||
| No | 19 (73.1) | 7 (26.9) | 0.145 |
| Yes | 33 (86.8) | 5 (13.2) | |
| Experience with radiotherapy 1 | |||
| No | 23 (85.2) | 4 (14.8) | 0.447 |
| Yes | 29 (80.6) | 7 (19.4) | |
| Previous surgical treatment 1 | |||
| No | 22 (75.9) | 7 (25.1) | 0.292 |
| Yes | 32 (84.2) | 6 (15.8) | |
| Variables | Odds Ratio (95% Confidence Interval) | p-Value |
|---|---|---|
| Gender | ||
| Male | Ref. | |
| Female | 4.00 (0.85–18.90) | 0.080 |
| Age category | ||
| ≤60 | Ref. | |
| 61–70 | 0.62 (0.11–3.49) | 0.584 |
| ≥71 | 0.60 (0.12–3.10) | 0.542 |
| Income | ||
| Lower income (<JPY 4 million) | Ref. | |
| Higher income (≥JPY 4 million) | 0.47 (0.16–1.37) | 0.168 |
| Job | ||
| Employed | Ref. | |
| Unemployed | 0.95 (0.33–2.74) | 0.931 |
| Education | ||
| High school graduate or less | Ref. | |
| Associate degree or more | 1.64 (0.56–4.79) | 0.369 |
| Cancer | ||
| Non-cancer respondents | Ref. | |
| Cancer patients | 0.69 (0.18–2.70) | 0.598 |
| Cancer stage 1 | ||
| 1 | Ref. | |
| 2–4 | 1.84 (0.48–6.97) | 0.373 |
| Year 1 | ||
| 2015–2018 | Ref. | |
| Before 2015 | 0.50 (0.10–2.51) | 0.397 |
| Hospital 1 | ||
| Other hospitals | Ref. | |
| Cancer special hospitals | 1.11 (0.33–3.73) | 0.869 |
| Previous cancer recurrence 1 | ||
| No or other | Ref. | |
| Yes | 3.22 (0.38–27.52) | 0.286 |
| Experience with pharmacotherapy 1 | ||
| No | Ref. | |
| Yes | 2.43 (0.68–8.74) | 0.173 |
| Experience with radiotherapy 1 | ||
| No | Ref. | |
| Yes | 0.72 (0.19–2.76) | 0.633 |
| Previous surgical treatment 1 | ||
| No | Ref. | |
| Yes | 1.70 (0.50–5.74) | 0.395 |
| Variables | Number (%) | p-Value | |
|---|---|---|---|
| Decrease Trust | Other | ||
| Gender | |||
| Male | 55 (87.3) | 8 (12.7) | 0.157 |
| Female | 28 (96.6) | 1 (3.4) | |
| Age category | |||
| ≤60 | 14 (93.3) | 1 (6.7) | 0.550 |
| 61–70 | 26 (89.7) | 3 (10.3) | |
| ≥71 | 44 (89.8) | 5 (10.2) | |
| Income | |||
| Lower income (<JPY 4 million) | 41 (89.1) | 5 (10.9) | 0.590 |
| Higher income (≥JPY 4 million) | 36 (90.0) | 4 (10.0) | |
| Job | |||
| Employed | 33 (98.2) | 4 (10.8) | 0.515 |
| Unemployed | 51 (91.1) | 5 (8.9) | |
| Education | |||
| High school graduate or less | 23 (82.1) | 5 (17.7) | 0.089 |
| Associate degree or more | 61 (93.9) | 4 (6.1) | |
| Cancer | |||
| Non-cancer respondents | 19 (95.0) | 1 (5.0) | 0.424 |
| Cancer patients | 62 (89.9) | 7 (10.1) | |
| Cancer stage 1 | |||
| 1 | 22 (95.7) | 1 (4.3) | 0.283 |
| 2–4 | 27 (87.1) | 4 (12.9) | |
| Year 1 | |||
| 2015–2018 | 14 (82.4) | 3 (17.6) | 0.316 |
| Before 2015 | 46 (90.2) | 5 (9.8) | |
| Hospital 1 | |||
| Other hospitals | 26 (89.7) | 3 (10.3) | 0.517 |
| Cancer special hospitals | 33 (86.8) | 5 (13.2) | |
| Previous cancer recurrence 1 | |||
| No or other | 47 (90.4) | 5 (9.6) | 0.428 |
| Yes | 11 (84.6) | 2 (15.4) | |
| Experience with pharmacotherapy 1 | |||
| No | 24 (92.3) | 2 (7.7) | 0.398 |
| Yes | 33 (86.8) | 5 (13.2) | |
| Experience with radiotherapy 1 | |||
| No | 25 (92.6) | 2 (7.4) | 0.349 |
| Yes | 31 (86.1) | 5 (13.9) | |
| Experience with surgical treatment 1 | |||
| No | 24 (82.8) | 5 (17.2) | 0.119 |
| Yes | 36 (94.7) | 2 (5.3) | |
| Variables | Odds Ratio (95% Confidence Interval) | p-Value |
|---|---|---|
| Gender | ||
| Male | Ref. | |
| Female | 4.07 (0.48–34.21) | 0.185 |
| Age category | ||
| ≤60 | Ref. | |
| 61–70 | 0.62 (0.059–6.52) | 0.713 |
| ≥71 | 0.63 (0.068–5.84) | 0.683 |
| Income | ||
| Lower income (<JPY 4 million) | Ref. | |
| Higher income (≥JPY 4 million) | 1.10 (0.27–4.40) | 0.895 |
| Job | ||
| Employed | Ref. | |
| Unemployed | 1.24 (0.31–4.94) | 0.764 |
| Education | ||
| High school graduate or less | Ref. | |
| Associate degree or more | 3.32 (0.82–13.44) | 0.093 |
| Cancer | ||
| Non-cancer respondents | Ref. | |
| Cancer patients | 0.47 (0.054–4.03) | 0.488 |
| Cancer stage 1 | ||
| 1 | Ref. | |
| 2–4 | 0.31 (0.032–2.95) | 0.306 |
| Year 1 | ||
| 2015–2018 | Ref. | |
| Before 2015 | 1.97 (0.42–9.30) | 0.376 |
| Hospital 1 | ||
| Other hospitals | Ref. | |
| Cancer special hospitals | 0.76 (0.17–3.48) | 0.689 |
| Previous cancer recurrence 1 | ||
| No or other | Ref. | |
| Yes | 0.59 (0.10–3.42) | 0.552 |
| Experience with pharmacotherapy 1 | ||
| No | Ref. | |
| Yes | 0.55 (0.098–3.08) | 0.496 |
| Experience with radiotherapy 1 | ||
| No | Ref. | |
| Yes | 0.50 (0.089–2.78) | 0.425 |
| Experience with surgical treatment 1 | ||
| No | Ref. | |
| Yes | 3.75 (0.67–20.93) | 0.132 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Murayama, A.; Senoo, Y.; Harada, K.; Kotera, Y.; Saito, H.; Sawano, T.; Suzuki, Y.; Tanimoto, T.; Ozaki, A. Awareness and Perceptions among Members of a Japanese Cancer Patient Advocacy Group Concerning the Financial Relationships between the Pharmaceutical Industry and Physicians. Int. J. Environ. Res. Public Health 2022, 19, 3478. https://doi.org/10.3390/ijerph19063478
Murayama A, Senoo Y, Harada K, Kotera Y, Saito H, Sawano T, Suzuki Y, Tanimoto T, Ozaki A. Awareness and Perceptions among Members of a Japanese Cancer Patient Advocacy Group Concerning the Financial Relationships between the Pharmaceutical Industry and Physicians. International Journal of Environmental Research and Public Health. 2022; 19(6):3478. https://doi.org/10.3390/ijerph19063478
Chicago/Turabian StyleMurayama, Anju, Yuki Senoo, Kayo Harada, Yasuhiro Kotera, Hiroaki Saito, Toyoaki Sawano, Yosuke Suzuki, Tetsuya Tanimoto, and Akihiko Ozaki. 2022. "Awareness and Perceptions among Members of a Japanese Cancer Patient Advocacy Group Concerning the Financial Relationships between the Pharmaceutical Industry and Physicians" International Journal of Environmental Research and Public Health 19, no. 6: 3478. https://doi.org/10.3390/ijerph19063478
APA StyleMurayama, A., Senoo, Y., Harada, K., Kotera, Y., Saito, H., Sawano, T., Suzuki, Y., Tanimoto, T., & Ozaki, A. (2022). Awareness and Perceptions among Members of a Japanese Cancer Patient Advocacy Group Concerning the Financial Relationships between the Pharmaceutical Industry and Physicians. International Journal of Environmental Research and Public Health, 19(6), 3478. https://doi.org/10.3390/ijerph19063478