
Sexual Assault Is the Biggest Risk Factor for Violence against Women in Taiwan—A Nationwide Population Cohort Study from 2000 to 2015

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
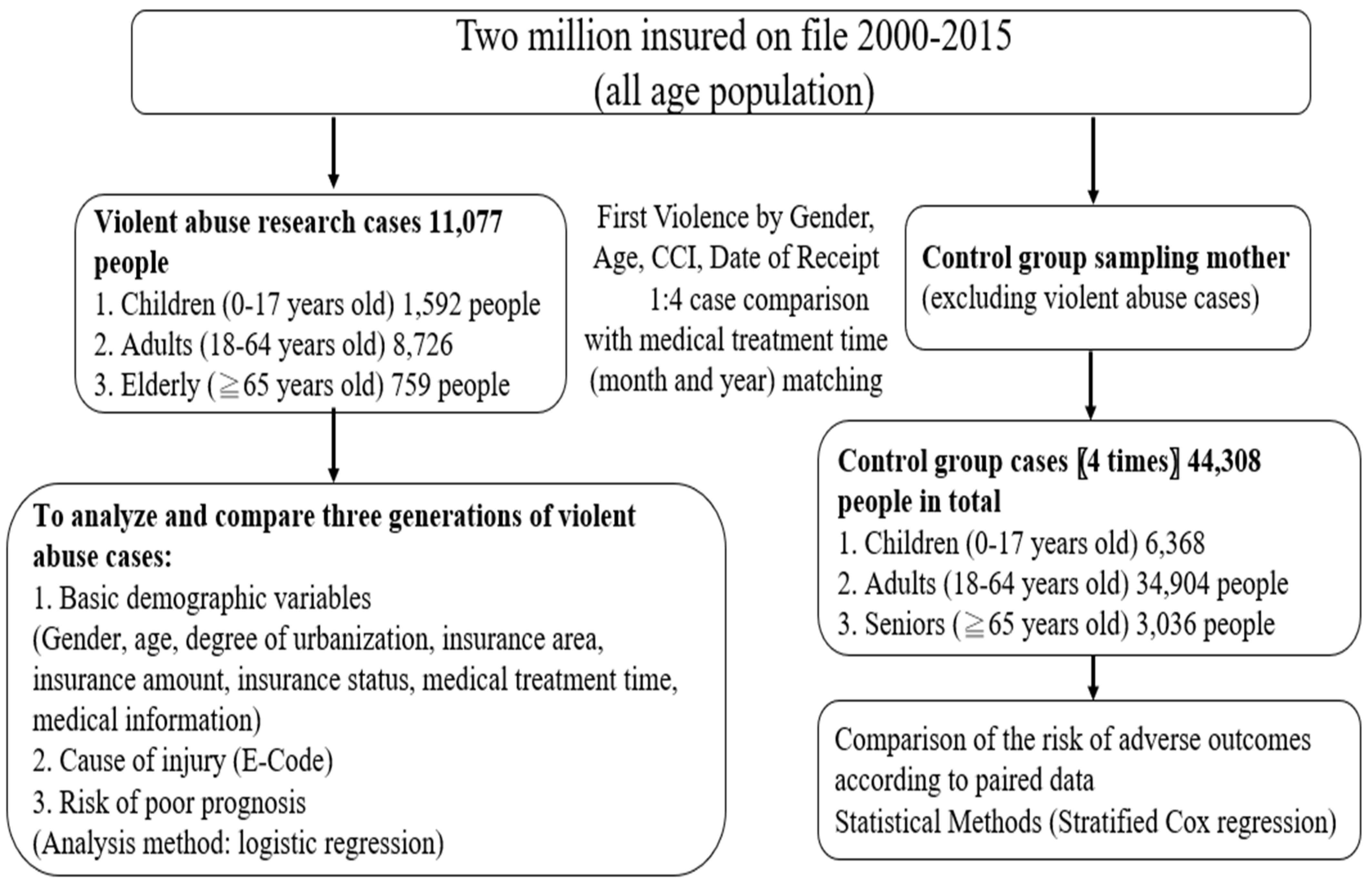
2.1. Data Source
2.2. Participants
2.3. Statistical Analysis
3. Results
4. Discussion
4.1. Importance of This Study
4.2. Cause of High Risk of Sexual Assault among High School Girls
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
| E-Code | Description |
| E960 | *Fight, brawl, rape |
| E960.0 | Unarmed fight or brawl |
| E960.1 | Rape |
| E961 | Assault by corrosive or caustic substance, except poisoning |
| E962 | *Assault by poisoning |
| E962.0 | Assault by drugs and medicinal substances |
| E962.1 | Assault by other solid and liquid substances |
| E962.2 | Assault by other gases and vapors |
| E962.9 | Assault by unspecified poisoning |
| E963 | Assault by hanging and strangulation |
| E964 | Assault by submersion (drowning) |
| E965 | *Assault by firearms and explosives |
| E965.0 | Assault by handgun |
| E965.1 | Assault by shotgun |
| E965.2 | Assault by hunting rifle |
| E965.3 | Assault by military firearms |
| E965.4 | Assault by other and unspecified firearm |
| E965.5 | Assault by antipersonnel bomb |
| E965.6 | Assault by gasoline bomb |
| E965.7 | Assault by letter bomb |
| E965.8 | Assault by another specified explosive |
| E965.9 | Assault by unspecified explosive |
| E966 | Assault by cutting and piercing instrument |
| ®E967 | *Perpetrator child and adult abuse |
| ®E967.0 | Perpetrator child and adult abuse by father, stepfather or boyfriend |
| E967.1 | Perpetrator child and adult abuse by another specified person |
| E967.2 | Perpetrator child and adult abuse by mother, stepmother or girlfriend |
| E967.3 | Perpetrator child and adult abuse by spouse or partner |
| E967.4 | Perpetrator child and adult abuse by child |
| E967.5 | Perpetrator child and adult abuse by sibling |
| E967.6 | Perpetrator child and adult abuse by grandparent |
| E967.7 | Perpetrator child and adult abuse by other relative |
| E967.8 | Perpetrator child and adult abuse by non- related caregiver |
| E967.9 | Perpetrator child and adult abuse by unspecified person |
| E968 | *Assault by other and unspecified means |
| E968.0 | Assault by fire |
| E968.1 | Assault by pushing from a high place |
| E968.2 | Assault by striking by blunt or thrown object |
| E968.3 | Assault by hot liquid |
| E968.4 | Assault by criminal neglect |
| E968.5 | Assault by transport vehicle |
| E968.6 | Assault by air gun |
| E968.7 | Assault by human bite |
| E968.8 | Assault by other specified means |
| E968.9 | Assault by unspecified means |
| E969 | Late effects of injury purposely inflicted by another person |
References
- World Health Organization. Violence Against. 2021. wome.Retrieved. Available online: https://www.who.int/news-room/fact-sheets/detail/violence-against-women (accessed on 16 October 2021).
- Schmitt, S.; Robjant, K.; Elbert, T.; Koebach, A. To add insult to injury: Stigmatization reinforces the trauma of rape survivors—Findings from the DR Congo. SSM Popul. Health 2021, 13, 100719. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guidelines for Medico-Legal Care of Victims of Sexual Violence; World Health Organization: Geneva, Switzerland, 2003.
- Das, T.; Basu Roy, D.T. More than individual factors; is there any contextual effect of unemployment, poverty and literacy on the domestic spousal violence against women? A multilevel analysis on Indian context. SSM Popul. Health 2020, 12, 100691. [Google Scholar] [CrossRef] [PubMed]
- Hammarström, S.; Alehagen, S.; Kilander, H. Violence and Sexual Risk Taking Reported by Young People at Swedish Youth Clinics. 2022. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8788656/ (accessed on 11 March 2022).
- Ajayi, A.I.; Mudefi, E.; Owolabi, E.O. Prevalence and correlates of sexual violence among adolescent girls and young women: Findings from a cross-sectional study in a South African university. BMC Women’s Health 2021, 21, 299. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, A.; Zahediasl, S. Normality tests for statistical analysis: A guide for non-statisticians. Int. J. Endocrinol. Metab. 2012, 10, 486–489. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oram, S.; Khalifeh, H.; Howard, L.M. Violence against women and mental health. Lancet. Psychiatry 2017, 4, 159–170. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Child Maltreatment. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/child-maltreatment (accessed on 11 March 2022).
- Arnarsson, A.M.; Gisladottir, K.H.; Jonsson, S.H. The prevalence of sexual abuse and sexual assault against Icelandic adolescents. Laeknabladid 2016, 102, 289–295. [Google Scholar]
- Mohler-Kuo, M.; Landolt, M.A.; Maier, T.; Meidert, U.; Schönbucher, V.; Schnyder, U. Child sexual abuse revisited: A population-based cross-sectional study among Swiss adolescents. J. Adolesc. Health 2014, 54, 304–311.e1. [Google Scholar] [CrossRef] [Green Version]
- Priebe, G.; Svedin, C.G. Child sexual abuse is largely hidden from the adult society: An epidemiological study of adolescents’ disclosures. Child Abus. Negl. 2008, 32, 1095–1108. [Google Scholar] [CrossRef]
- Coley, R.L.; Sims, J.; Dearing, E.; Spielvogel, B. Locating economic risks for adolescent mental and behavioral health: Poverty and affluence in families, neighborhoods, and schools. Child Dev. 2018, 89, 360–369. [Google Scholar] [CrossRef] [Green Version]
- Lund, T.J.; Dearing, E.; Zachrisson, H.D. Is affluence a risk for adolescents in Norway? J. Res. Adolesc. 2017, 27, 628–643. [Google Scholar] [CrossRef] [Green Version]
- Torsheim, T.; Nygren, J.M.; Rasmussen, M.; Arnarsson, A.M.; Bendtsen, P.; Schnohr, C.W.; Nielsen, L.; Nyholm, M. Social inequalities in self-rated health: A comparative cross-national study among 32,560 Nordic adolescents. Scand. J. Public Health 2018, 46, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Inchley, J.; Currie, D. Growing up unequal: Gender and socioeconomic differences in young people’s health and well-being. In Health Behaviour in Schoolaged Children (HBSC) Study: International Report from the 2013/2014 Survey; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Elgar, F.J.; Pförtner, T.K.; Moor, I.; De Clercq, B.; Stevens, G.W.; Currie, C. Socioeconomic inequalities in adolescent health 2002-2010: A time-series analysis of 34 countries participating in the Health Behaviour in School-aged Children study. Lancet 2015, 385, 2088–2095. [Google Scholar] [CrossRef] [Green Version]
- Runarsdottir, E.; Smith, E.; Arnarsson, A. The effects of gender and family wealth on sexual abuse of adolescents. Int. J. Environ. Res. Public Health 2019, 16, 1788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sedlak, A.J.; Mettenburg, J.; Basena, M.; Peta, I.; McPherson, K.; Greene, A.; Li, S. Fourth National Incidence Study of Child Abuse and Neglect; US Department of Health and Human Services: Washington, DC, USA, 2010; Volume 9, (NIS-4).
- Lee, C.; Coe, C.L.; Ryff, C.D. Social disadvantage, severe child abuse, and biological profiles in adulthood. J. Health Soc. Behav. 2017, 58, 371–386. [Google Scholar] [CrossRef]
- Matta Oshima, K.M.; Jonson-Reid, M.; Seay, K.D. The influence of childhood sexual abuse on adolescent outcomes: The roles of gender, poverty, and revictimization. J. Child Sex. Abus. 2014, 23, 367–386. [Google Scholar] [CrossRef] [Green Version]
- Mendelson, T.; Kubzansky, L.D.; Datta, G.D.; Buka, S.L. Relation of female gender and low socioeconomic status to internalizing symptoms among adolescents: A case of double jeopardy? Soc. Sci. Med. 2008, 66, 1284–1296. [Google Scholar] [CrossRef]
- Skinner, T. POLICY BRIEF: Strategies to Support Migrant Victim-Survivors of Domestic Abuse; Department of Social & Policy Sciences Centre for Analysis of SOCIAL Policy (CASP): Bath, UK, 2021; Available online: https://researchportal.bath.ac.uk/en/publications/policy-brief-strategies-to-support-migrant-victim-survivors-of-do (accessed on 16 September 2021).
- Sapp, M.V.; Vandeven, A.M. Update on childhood sexual abuse. Curr. Opin. Pediatrics 2005, 17, 258–264. [Google Scholar] [CrossRef]
- Hébert, M.; Moreau, C.; Blais, M.; Lavoie, F.; Guerrier, M. Child sexual abuse as a risk factor for teen dating violence: Findings from a representative sample of Quebec youth. J. Child Adolesc. Trauma 2017, 10, 51–61. [Google Scholar] [CrossRef]
- Casteel, C.; Martin, S.L.; Smith, J.B.; Gurka, K.K.; Kupper, L.L. National study of physical and sexual assault among women with disabilities. Inj. Prev. 2008, 14, 87–90. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Violence Prevention; Chan, H.C.M., Fedotov, Y., Eds.; World Health Organization: Geneva, Switzerland, 2014.
- Fuller-Thomson, E.; Agbeyaka, S. A trio of risk factors for childhood sexual abuse: Investigating exposure to parental domestic violence, parental addiction, and parental mental illness as correlates of childhood sexual abuse. Soc. Work 2020, 65, 266–277. [Google Scholar] [CrossRef]
- Zhang, X.; Wu, G. Review and Prospect of Gender-Based Violence Prevention and Control in Taiwan. 2016. Available online: https://cdj.sfaa.gov.tw/Journal/Content?gno=6906 (accessed on 11 March 2022).
- Ministry of Health and Welfare. Domestic Violence Prevention Act. 2021. Available online: https://law.moj.gov.tw/LawClass/LawAll.aspx?PCode=D0050071 (accessed on 15 September 2021).
- Mathews, B.; Collin-Vézina, D. Child sexual abuse: Toward a conceptual model and definition. Trauma Violence Abus. 2019, 20, 131–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blake, M.T.; Drezett, J.; Vertamatti, M.A.; Adami, F.; Valenti, V.E.; Paiva, A.C.; Viana, J.M.; Pedroso, D.; De Abreu, L.C. Characteristics of sexual violence against adolescent girls and adult women. BMC Women’s Health 2014, 14, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Öberg, M.; Skalkidou, A.; Heimer, G.; Lucas, S. Sexual violence against women in Sweden: Associations with combined childhood violence and sociodemographic factors. Scand. J. Public Health 2021, 49, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare Department of Protection Services. Cross-Statistical Statistics on Age and Gender of Victims in Sexual Assault Cases. 2021. Available online: https://dep.mohw.gov.tw/DOPS/cp-1303-59309-105.html (accessed on 11 October 2021).
- Lesuer, W. An international study of the contextual effects of gender inequality on intimate partner sexual violence against women students. Fem. Criminol. 2020, 15, 97–118. [Google Scholar] [CrossRef]
- Sanday, P.R. The socio-cultural context of rape: A cross-cultural study. J. Soc. Issues 1981, 37, 5–27. [Google Scholar] [CrossRef]
- Cohen, L.E.; Felson, M. Social change and crime rate trends: A routine activity approach. Am. Sociol. Rev. 1979, 44, 588–608. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC). International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). 2021. Available online: https://www.cdc.gov/nchs/icd/icd9cm.htm (accessed on 11 March 2022).


{kind=link}
| Cause of Injury (E-Code E960–E969) ‡ | Children and Adolescents (n = 1592) | Adult (n = 8726) | Elderly (n = 759) | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | p | |
| Grapple, fighting, sexual assault (E960) | 659 | 41.4 | 3265 | 37.4 | 183 | 24.1 | <0.0001 ** |
| Unarmed combat or fighting (E960.0) | 315 | 19.8 | 2877 | 33.0 | 173 | 22.8 | <0.0001 ** |
| Sexual Assault (E960.1) | 301 | 18.9 | 217 | 2.5 | 0 | 0.0 | <0.0001 ** |
| Damage from cutting tools (E966) | 94 | 5.9 | 803 | 9.2 | 57 | 7.5 | <0.0001 ** |
| Persecuted and abused children and adults (E967) | 73 | 4.6 | 550 | 6.3 | 43 | 5.7 | 0.0273 * |
| Persecuted by father, stepfather, or boyfriend (E967.0) | 16 | 1.0 | 22 | 0.3 | 0 | 0.0 | <0.0001 ** |
| Persecuted by spouse or partner (E967.3) | 0 | 0.0 | 232 | 2.7 | 8 | 1.1 | <0.0001 ** |
| Persecuted by others (E967.1, E967.2, E967.4–E967.9) | 56 | 3.5 | 293 | 3.4 | 35 | 4.6 | 0.1927 |
| Wounded by blunt object or dropped object (E968.2) | 95 | 6.0 | 705 | 8.1 | 46 | 6.1 | 0.0034 ** |
| Harmed by other means (E961–E965, E968.0, E968.1, E968.3–E968.7) | 475 | 29.8 | 3447 | 39.5 | 382 | 50.3 | <0.0001 ** |
| Cause of Injury (E-Code E960–E969) ‡ | Children and Adolescents (n = 759) | Adult (n = 2873) | The Elderly (n = 282) | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | p | |
| Grapple, fighting, and sexual assault (E960) | 357 | 47.0 | 981 | 34.1 | 58 | 20.6 | <0.0001 ** |
| Unarmed combat or fighting (E960.0) | 42 | 5.5 | 705 | 24.5 | 52 | 18.4 | <0.0001 ** |
| Sexual Assault (E960.1) | 295 | 38.9 | 212 | 7.4 | 0 | 0.0 | <0.0001 ** |
| Damage from cutting tools (E966) | 17 | 2.2 | 147 | 5.1 | 17 | 6.0 | 0.0018 ** |
| Persecuted and abused children and adults (E967) | 31 | 4.1 | 357 | 12.4 | 18 | 6.4 | <0.0001 ** |
| Persecuted by father, stepfather, or boyfriend (E967.0) | 6 | 0.8 | 16 | 0.6 | 0 | 0.0 | 0.3160 |
| Persecuted by spouse or partner (E967.3) | 0 | 0.0 | 206 | 7.2 | 5 | 1.8 | <0.0001 ** |
| Persecuted by others (E967.1, E967.2, E967.4–E967.9) | 24 | 3.2 | 132 | 4.6 | 13 | 4.6 | 0.2182 |
| Wounded by blunt object or dropped object (E968.2) | 12 | 1.6 | 113 | 3.9 | 17 | 6.0 | 0.0007 ** |
| Harmed by other means (E961–E965, E968.0, E968.1, E968.3–E968.7) | 100 | 13.2 | 885 | 30.8 | 141 | 50.0 | <0.0001 ** |
| Demographic Variables | Sexually Assaulted | Other Reasons | ||||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | p a | OR (95% CI) | p b | ||
| Age (years) | <12 | 17 | 3.4 | 66 | 2.1 | <0.0001 ** | 1.000 | |
| 12–17 | 278 | 54.8 | 398 | 12.7 | 2.71 (1.56–4.72) | 0.0004 ** | ||
| 18–23 | 97 | 19.1 | 331 | 10.6 | 1.14 (0.64–2.03) | 0.6623 | ||
| 24–44 | 93 | 18.3 | 1480 | 47.4 | 0.24 (0.14–0.43) | <0.0001 ** | ||
| 45–64 | 22 | 4.3 | 850 | 27.2 | 0.10 (0.05–0.20) | <0.0001 ** | ||
| Age Group | OR (95% CI) | p |
|---|---|---|
| Senior age vs. Junior age | 2.50 (1.37–4.55) | 0.0030 ** |
| Children and Adolescents vs. The Elderly | 11.4 (7.07–18.4) | <0.0001 ** |
| Adult vs. The Elderly | 2.51 (1.57–4.01) | 0.0001 ** |
| Occupation of the Person or the Health Care Dependent | Girls vs. Adult Women | |
|---|---|---|
| OR (95% CI) | p | |
| Public insurance | 1.00 | |
| Labor insurance | 4.87 (1.31–18.13) | 0.0184 * |
| Farmer | 4.44 (1.04–19.01) | 0.0443 * |
| Member of Water Conservancy and Fisheries Association | 5.93 (1.29–27.28) | 0.0224 * |
| Low-income households | 10.74 (2.42–47.72) | 0.0018 ** |
| Community insured population | 3.91 (1.04–14.79) | 0.0443 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chwo, M.-J.; Huang, S.-H.; Huang, Y.-C.; Lin, I.-J.; Yu, C.-P.; Chung, C.-H.; Chien, W.-C.; Sun, C.-A.; Wu, G.-J. Sexual Assault Is the Biggest Risk Factor for Violence against Women in Taiwan—A Nationwide Population Cohort Study from 2000 to 2015. Int. J. Environ. Res. Public Health 2022, 19, 3473. https://doi.org/10.3390/ijerph19063473
Chwo M-J, Huang S-H, Huang Y-C, Lin I-J, Yu C-P, Chung C-H, Chien W-C, Sun C-A, Wu G-J. Sexual Assault Is the Biggest Risk Factor for Violence against Women in Taiwan—A Nationwide Population Cohort Study from 2000 to 2015. International Journal of Environmental Research and Public Health. 2022; 19(6):3473. https://doi.org/10.3390/ijerph19063473
Chicago/Turabian StyleChwo, Miao-Ju, Shi-Hao Huang, Yao-Ching Huang, Iau-Jin Lin, Chia-Peng Yu, Chi-Hsiang Chung, Wu-Chien Chien, Chien-An Sun, and Gwo-Jang Wu. 2022. "Sexual Assault Is the Biggest Risk Factor for Violence against Women in Taiwan—A Nationwide Population Cohort Study from 2000 to 2015" International Journal of Environmental Research and Public Health 19, no. 6: 3473. https://doi.org/10.3390/ijerph19063473
APA StyleChwo, M.-J., Huang, S.-H., Huang, Y.-C., Lin, I.-J., Yu, C.-P., Chung, C.-H., Chien, W.-C., Sun, C.-A., & Wu, G.-J. (2022). Sexual Assault Is the Biggest Risk Factor for Violence against Women in Taiwan—A Nationwide Population Cohort Study from 2000 to 2015. International Journal of Environmental Research and Public Health, 19(6), 3473. https://doi.org/10.3390/ijerph19063473