
Towards a Better Understanding of the Factors Associated with Distress in Elderly Cancer Patients: A Systematic Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Literature Search
2.3. Extraction and Synthesis Strategy
2.4. Quality Appraisal
3. Results
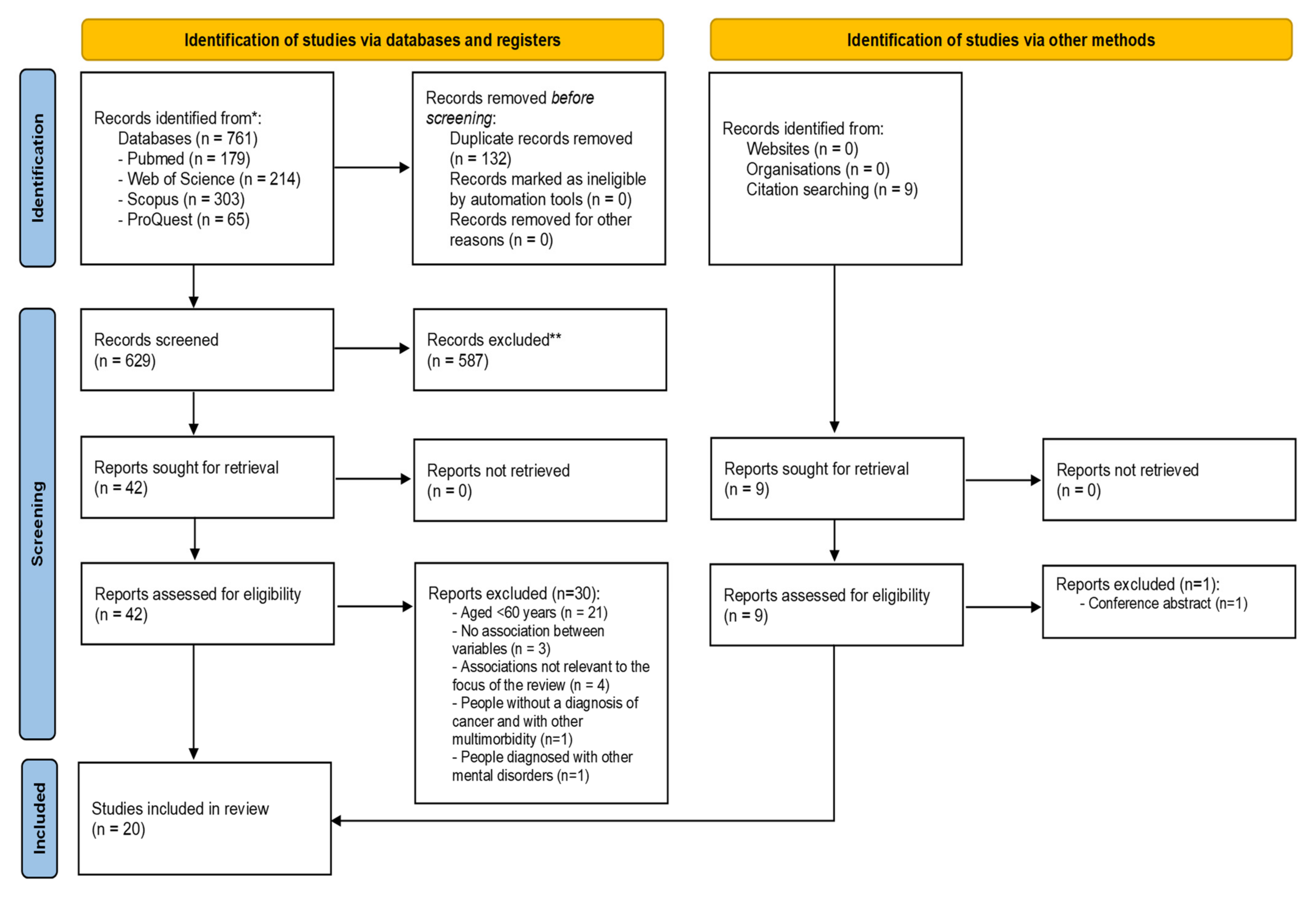
3.1. Search Results
3.2. Study Characteristics
3.3. Measures
3.4. Factors Affecting Psychological Distress
3.4.1. Sociodemographic Factors and Distress
3.4.2. Clinical Factors and Distress
3.4.3. Psychosocial Factors and Distress
3.5. Study Quality Assessment
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations in Western Europe. Available online: https://unric.org/pt/envelhecimento/ (accessed on 2 December 2021).
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- World Health Organization. Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 2 December 2021).
- Cancer Tomorrow. Available online: https://gco.iarc.fr/tomorrow/en (accessed on 19 December 2021).
- Blank, T.O.; Bellizzi, K.M. A gerontologic perspective on cancer and aging. Cancer 2008, 112, 2569–2576. [Google Scholar] [CrossRef] [PubMed]
- Dale, W.; Mohile, S.G.; Eldadah, B.A.; Trimble, E.L.; Schilsky, R.L.; Cohen, H.J.; Muss, H.B.; Schmader, K.E.; Ferrell, B.; Extermann, M.; et al. Biological, Clinical, and Psychosocial Correlates at the Interface of Cancer and Aging Research. J. Natl. Cancer Inst. 2012, 104, 581–589. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Surbone, A.; Kagawa-Singer, M.; Terret, C.; Baider, L. The illness trajectory of elderly cancer patients across cultures: SIOG position paper. Ann. Oncol. 2007, 18, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Hurria, A.; Levit, L.A.; Dale, W.; Mohile, S.G.; Muss, H.B.; Fehrenbacher, L.; Magnuson, A.; Lichtman, S.; Bruinooge, S.S.; Soto-Perez-De-Celis, E.; et al. Improving the Evidence Base for Treating Older Adults With Cancer: American Society of Clinical Oncology Statement. J. Clin. Oncol. 2015, 33, 3826–3833. [Google Scholar] [CrossRef]
- Beekman, A.T.F.; Copeland, J.R.; Prince, M.J. Review of community prevalence of depression in later life. Br. J. Psychiatry 1999, 174, 307–311. [Google Scholar] [CrossRef]
- Bryant, C.; Jackson, H.; Ames, D. The prevalence of anxiety in older adults: Methodological issues and a review of the literature. J. Affect. Disord. 2008, 109, 233–250. [Google Scholar] [CrossRef]
- Alici, Y.; Weiss, T.; Holland, J.C.; Nelson, C.; Roth, A. Common psychiatric problems in older patients with cancer: Report of one-year experience of a psychiatry outpatient clinic. J. Geriatr. Oncol. 2011, 2, 137–141. [Google Scholar] [CrossRef]
- Kurtz, M.E.; Kurtz, J.C.; Stommel, M.; Given, C.W.; Given, B. Physical Functioning and Depression Among Older Persons with Cancer. Cancer Pr. 2001, 9, 11–18. [Google Scholar] [CrossRef]
- Weinberger, M.I.; Roth, A.J.; Nelson, C.J. Untangling the Complexities of Depression Diagnosis in Older Cancer Patients. Oncologist 2009, 14, 60–66. [Google Scholar] [CrossRef]
- Husain, M.; Rush, A.J.; Sackeim, H.A.; Wisniewski, S.R.; Mcclintock, S.M.; Craven, N.; Holiner, J.; Mitchell, J.R.; Balasubramani, G.; Hauger, R. Age-Related Characteristics of a Depression: A Preliminary STAR*D Report. Am. J. Geriatr. Psychiatry 2005, 13, 852–860. [Google Scholar] [CrossRef]
- Stark, D.P.H.; House, A. Review: Anxiety in cancer patients. Br. J. Cancer 2000, 83, 1261–1267. [Google Scholar] [CrossRef]
- Roth, A.J.; Greenstein, M.; Wiesel, T.W.; Schulberg, S. Depressive Spectrum Disorders and Grief. In Geriatric Psycho-Oncology; Holland, J.C., Wiesel, T.W., Nelson, C.J., Roth, A.J., Alici, Y., Eds.; Oxford University Press (OUP): Oxford, UK, 2014; pp. 59–68. [Google Scholar]
- Roth, A.J.; Modi, R. Psychiatric issues in older cancer patients. Crit. Rev. Oncol. 2003, 48, 185–197. [Google Scholar] [CrossRef]
- Prieto, J.M.; Blanch, J.; Atala, J.; Carreras, E.; Rovira, M.; Cirera, E.; Gastó, C. Psychiatric Morbidity and Impact on Hospital Length of Stay Among Hematologic Cancer Patients Receiving Stem-Cell Transplantation. J. Clin. Oncol. 2002, 20, 1907–1917. [Google Scholar] [CrossRef]
- Brothers, B.M.; Andersen, B.L. Hopelessness as a predictor of depressive symptoms for breast cancer patients coping with recurrence. Psycho-Oncology 2008, 18, 267–275. [Google Scholar] [CrossRef]
- Hjerl, K.; Andersen, E.W.; Keiding, N.; Mouridsen, H.T.; Mortensen, P.B.; Jørgensen, T. Depression as a Prognostic Factor for Breast Cancer Mortality. J. Psychosom. Res. 2003, 44, 24–30. [Google Scholar] [CrossRef]
- Reich, M.; Lesur, A.; Perdrizet-Chevallier, C. Depression, quality of life and breast cancer: A review of the literature. Breast Cancer Res. Treat. 2007, 110, 9–17. [Google Scholar] [CrossRef]
- Niedzwiedz, C.L.; Knifton, L.; Robb, K.A.; Katikireddi, S.V.; Smith, D.J. Depression and anxiety among people living with and beyond cancer: A growing clinical and research priority. BMC Cancer 2019, 19, 943. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef]
- Joanna Briggs Institute. Checklist for Analytical Cross Sectional Studies; Joanna Briggs Institute: Adelaide, Australia, 2020. [Google Scholar]
- Joanna Briggs Institute. Checklist for Cohort Studies; Joanna Briggs Institute: Adelaide, Australia, 2020. [Google Scholar]
- Baeza-Velasco, C.; Baguet, F.; Allart, P.; Aguerre, C.; Sultan, S.; Ninot, G.; Soubeyran, P.; Cousson-Gelie, F. Major depressive disorder and associated factors in elderly patients with Non-Hodgkin’s Lymphoma. Health Psychol. Behav. Med. 2017, 5, 57–65. [Google Scholar] [CrossRef][Green Version]
- Alwhaibi, M.; Sambamoorthi, U.; Madhavan, S.; Bias, T.; Kelly, K.; Walkup, J. Cancer Type and Risk of Newly Diagnosed Depression Among Elderly Medicare Beneficiaries With Incident Breast, Colorectal, and Prostate Cancers. J. Natl. Compr. Cancer Netw. 2016, 15, 46–55. [Google Scholar] [CrossRef]
- Meier, C.; Taubenheim, S.; Lordick, F.; Mehnert-Theuerkauf, A.; Götze, H. Depression and anxiety in older patients with hematological cancer (70+)—Geriatric, Social, Cancer- and Treatment-Related Associations. J. Geriatr. Oncol. 2019, 11, 828–835. [Google Scholar] [CrossRef]
- Wiesel, T.R.W.; Nelson, C.J.; Tew, W.P.; Hardt, M.; Mohile, S.G.; Owusu, C.; Klepin, H.D.; Gross, C.P.; Gajra, A.; Lichtman, S.M.; et al. The relationship between age, anxiety, and depression in older adults with cancer. Psycho-Oncology 2015, 24, 712–717. [Google Scholar] [CrossRef]
- Klapheke, A.K.; Keegan, T.H.; Ruskin, R.; Cress, R.D. Depressive symptoms and health-related quality of life in older women with gynecologic Cancers. J. Geriatr. Oncol. 2020, 11, 820–827. [Google Scholar] [CrossRef]
- Rost, K.; Burnam, M.A.; Smith, G.R. Development of Screeners for Depressive Disorders and Substance Disorder History. Med. Care 1993, 31, 189–200. [Google Scholar] [CrossRef]
- Goldzweig, G.; Baider, L.; Rottenberg, Y.; Andritsch, E.; Jacobs, J.M. Is age a risk factor for depression among the oldest old with cancer? J. Geriatr. Oncol. 2018, 9, 476–481. [Google Scholar] [CrossRef]
- Hong, J.-F.; Zhang, W.; Song, Y.-X.; Xie, L.-F.; Wang, W.-L. Psychological distress in elderly cancer patients. Int. J. Nurs. Sci. 2015, 2, 23–27. [Google Scholar] [CrossRef]
- Duc, S.; Rainfray, M.; Soubeyran, P.-L.; Fonck, M.; Blanc, J.F.; Ceccaldi, J.; Cany, L.; Brouste, V.; Mathoulin-Pélissier, S. Predictive factors of depressive symptoms of elderly patients with cancer receiving first-line chemotherapy. Psycho-Oncology 2016, 26, 15–21. [Google Scholar] [CrossRef]
- Malak, M.Z.; Tawalbeh, L.I.; Al-Amer, R.M. Depressive Symptoms among Older Jordanian Patients with Cancer Undergoing Treatment. Clin. Gerontol. 2020, 44, 133–142. [Google Scholar] [CrossRef]
- Deimling, G.T.; Albitz, C.; Monnin, K.; Pappada, H.T.R.; Nalepa, E.; Boehm, M.L.; Mitchell, C. Personality and psychological distress among older adult, long-term cancer survivors. J. Psychosoc. Oncol. 2016, 35, 17–31. [Google Scholar] [CrossRef]
- Ladaninejad, S.; Ilali, E.; Mousavinasab, N.; Taraghi, Z. The Relationship between Depressive Symptoms and Demographic-Medical Characteristics among Elder People with Cancer. Asia-Pac. J. Oncol. Nurs. 2019, 6, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Deimling, G.T.; Brown, S.P.; Albitz, C.; Burant, C.J.; Mallick, N. The relative importance of cancer-related and general health worries and distress among older adult, long-term cancer survivors. Psycho-Oncology 2015, 26, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Soto-Perez-De-Celis, M.E.; Sun, C.; Tew, W.P.; Mohile, S.G.; Gajra, A.; Klepin, H.D.; Owusu, C.; Gross, C.P.; Muss, H.B.; Lichtman, S.M.; et al. Association between patient-reported hearing and visual impairments and functional, psychological, and cognitive status among older adults with cancer. Cancer 2018, 124, 3249–3256. [Google Scholar] [CrossRef] [PubMed]
- Canoui-Poitrine, F.; Reinald, N.; Laurent, M.; Guery, E.; Caillet, P.; David, J.-P.; Tournigand, C.; Lagrange, J.-L.; Bastuji-Garin, S.; Lemogne, C.; et al. Geriatric assessment findings independently associated with clinical depression in 1092 older patients with cancer: The ELCAPA Cohort Study. Psycho-Oncology 2016, 25, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Clark, C.J.; Fino, N.F.; Liang, J.H.; Hiller, D.; Bohl, J. Depressive symptoms in older long-term colorectal cancer survivors: A population-based analysis using the SEER-Medicare healthcare outcomes survey. Support. Care Cancer 2016, 24, 3907–3914. [Google Scholar] [CrossRef]
- Solvik, E.; Ytrehus, S.; Utne, I.; Grov, E.K. Pain, fatigue, anxiety and depression in older home-dwelling people with cancer. Nurs. Open 2019, 7, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Atag, E.; Mutlay, F.; Soysal, P.; Semiz, H.S.; Kazaz, S.N.; Keser, M.; Ellidokuz, H.; Karaoglu, A. Prevalence of depressive symptoms in elderly cancer patients receiving chemotherapy and influencing factors. Psychogeriatrics 2018, 18, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Goldzweig, G.; Baider, L.; Andritsch, E.; Pfeffer, R.; Rottenberg, Y. A Dialogue of Depression and Hope: Elderly Patients Diagnosed with Cancer and Their Spousal Caregivers. J. Cancer Educ. 2017, 32, 549–555. [Google Scholar] [CrossRef]
- Okumura, M.; Inoue, T.; Melinda, G.; Saito, T.; Fukuta, A.; Makiura, D.; Inoue, J.; Sakai, Y.; Ono, R. Social frailty as a risk factor for new-onset depressive symptoms at one year post-surgery in older patients with gastrointestinal cancer. J. Geriatr. Oncol. 2020, 11, 904–907. [Google Scholar] [CrossRef]
- Oserowsky, A.; Anwar, T.; Lough, C.; Golzy, M.; Murray, K.S. The Significant Role of Depression in Elderly Patients with Bladder Cancer. Eur. Urol. Open Sci. 2021, 33, 11–18. [Google Scholar] [CrossRef]
- Maier, A.; Riedel-Heller, S.G.; Pabst, A.; Luppa, M. Risk factors and protective factors of depression in older people 65+. A systematic review. PLoS ONE 2021, 16, e0251326. [Google Scholar] [CrossRef]
- Massie, M.J. Prevalence of Depression in Patients with Cancer. J. Natl. Cancer Inst. Monogr. 2004, 2004, 57–71. [Google Scholar] [CrossRef]
- Parpa, E.; Tsilika, E.; Gennimata, V.; Mystakidou, K. Elderly cancer patients’ psychopathology: A systematic review. Arch. Gerontol. Geriatr. 2015, 60, 9–15. [Google Scholar] [CrossRef]


{kind=link}
| Ref ID | Author (Year) | Country | Study Design | Sample Size (N) | Cancer Type | Mean Age | % Female | Distress Measures | Main Factors | Main Results |
|---|---|---|---|---|---|---|---|---|---|---|
| [28] | Meier et al. (2020) | Germany | Cross-sectional study | N = 425 | Hematological | 75.7 (4.2) | 38.4% | General Anxiety Disorder (GAD-7) Patient Health Questionnaire (PHQ-9) | Gender, age, partnership, education, type of cancer, disease condition, treatment, malnutrition, polypharmacy, tendency to fall, limited mobility, care level, self-perceived social support, social isolation, quality of life (QoL). | - ↓ mobility, need for care, comorbidity, ongoing chemotherapy, lack of partnership and ↓QoL were associated with ↑ depression. ↓ social interaction, cognitive and emotional functioning, poor nutrition, and comorbidity was associated with ↑ anxiety. |
| [27] | Alwhaibi et al. (2017) | USA | Retrospective Cohort Study | N = 53,821 | Breast, colorectal, prostate | Age groups (66–69 y, n = 14,007), (70–74 y, n = 15,791), (75–79 y, n = 11,276), (≥80 y, n = 2747) | 48.9% | International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) | Cancer type, stage at cancer diagnosis, treatment, gender. | - Women with colorectal cancer (CRC) compared with men with CRC; women with CRC compared with those with breast cancer, and among men with CRC compared with those with prostate cancer; and survivors diagnosed at an advanced stage were associated ↑ % diagnosis depression. |
| [29] | Wiesel et al. (2015) | USA | Cross sectional- study | N = 500 | Lung, gastrointestinal, gynaecological, breast, genitourinary and others. | 73.1 (6.18) | 56.2% | Hospital Anxiety and Depression Scale (HADS) | Age, gender, education, cancer type, stage of disease, comorbidities, social support. | - ↑ age, ↑ social support, ↓ number of comorbidities were associated ↓ anxiety. - ↓ social support, ↑ number of comorbidities, and advanced stage were associated with ↑ depression. |
| [26] | Baeza-Velasc et al. (2017) | France | Cross sectional-study | N = 42 | Non-Hodgkin’s lymphoma | 81.6 (4.2) | 52.4% | Mini-international neuropsychiatric interview (MINI) | Gender, age, marital status, number of children, schooling, geographical area, stage, comorbidities, No of drugs, malnutrition, performance status, fatigue, history of depression, cognitive status coping strategies, perception of social support, conflict, depth, global health status and global QoL. | - ↓ self-perceived ↓ performance status, ↑ fatigue and history of depression were associated a patients with Major of Depressive Disorder (MDD). |
| [30] | Klapheke et al. (2019) | USA | Cross-sectional study | N = 11,862 | Gynecologic | age all cancer = 74.8 (6.5), age no cancer = 75.3 (7.0). | 100% | Algorithm by Rost et al. [31] and responses to questions from the Diagnostic Interview Schedule in the MHOS. - Veterans RAND 12-item Health Survey (VR-12) | Age, race, education level, marital status, income, region, cancer site, comorbidities, stage at diagnosis, Activitie Daily Living (ADLs), time since diagnosis, health-related quality of life. | - ↑ age was associated with ↓ depressive symptoms. - later stage diagnosis, cardiovascular disease, stroke, sciatica, impairment in ADL, ↓ physical and mental measures of HRQOL were associated ↑ depressive symptoms. |
| [32] | Goldzweig et al. (2018) | Israel | Cross-sectional study | N = 243 | Lung, prostate, breast, colorectal, melanoma, other | 77.53 (9.29) | 35.8% | Geriatric Depression Scale (GDS-5) Distress thermometer (1 item) | Age, gender, time of diagnosis, stage of cancer, performance status, comorbidity treatment, social support. | - ↑ age was associated ↑ depression levels and distress. |
| [33] | Hong et al. (2015) | China | Cross-sectional study | N = 153 | Digestive, respiratory, breast, urogenital system, others | 67.2 (6.01) | 39.2% | Distress thermometer | Gender, marital status, education, income, disease site of cancer, treatment. | - married, ↑ education, ↑ monthly income had ↓ distress. |
| [34] | Duc et al. (2017) | France | Prospective cohort study | N = 260 | Colon, stomach, pancreas, non-Hodgkin´s lymphoma, prostate, ovary, bladder, lung, unknown primary origin | 77.6 (4.8) | 44.6% | GDS-15 | Age, gender, live alone, education, marital status, cancer site, performance, advanced disease, treatment, ADLs, Instrumental Activities of Daily Living (IADLs), cognitive status, nutritional status, fall risk. | - Depressive symptoms at baseline, and malnutrition was associated ↑ risk of depression. - Effective chemotherapy was associated with a ↓ risk of depression. |
| [35] | Malak et al. (2020) | Jordan | Cross-sectional study | N = 150 | Undefined | 64.33 (3.46) | 42% | HADS | Age, educational level, duration of cancer treatment, type of treatment, health insurance, hope, anxiety. | - ↓ Duration of treatment, ↓ hope, and ↑ anxiety were the predictors of ↑ depression. |
| [36] | Deimling, et al. (2017) | USA | Cross sectional study | N = 275 | Breast, prostate | 73.18 (7.18) | 58.2% | Center for Epidemiologic Studies Depression Scale (CES-D) | Age, gender, race, personality, type, stage at diagnosis, years since diagnosis, No of treatments, No of symptoms, No of symptoms attributed to cancer, No of health conditions, functional difficulties, cancer-related health insurance. | - Neuroticism, conscientiousness, agreeableness were significant predictors of depression. |
| [37] | Ladaninejad et al. (2019) | Iran | Cross-sectional study | N = 200 | Colon, esophageal, breast, prostate, lung; head and neck, gastric | 67.82 (6.73) | 51% | GDS | Gender, marital status, living with, frequency of contact with children, education, income, type of underlying disease, type of cancer, stage of cancer, metastasis, pain, nausea, vomiting, shortness of breath, hair loss, frequency of chemotherapy, ADLs, cognitive status, perceived social support. | - Single patients and patients with colon cancer had ↓ depression. - Widowed, elderly, ↓ income, with diabetes and respiratory diseases had a ↑ depression. |
| [38] | Deimling et al. (2017) | USA | Cross sectional design | N = 245 | Breast, prostate, colorectal | 75.9 | 63% | CES-D Profile of Mood States (POMS) | Age, type of cancer, years since diagnosis, comorbidities, functional difficulties, current cancer and non cancer symptoms, worry dimensions, psychological distress. | Symptoms not attributed to cancer, functional difficulties, No of comorbidities are relatively strong correlates of depression and anxiety. |
| [39] | Soto-Perez-de-Celis et al. (2015) | USA | Prospective study | N = 750 | Lung, gastrointestinal, breast, gynecological and others | 72 (median) | 44% | HADS | Sensory impairments | Sensory impairments were associated with depression and anxiety. |
| [40] | Canoui-Poitrine et al. (2015) | France | Cross-sectional study | N = 1092 | Ovarian and endometrial, esophagus, prostate, urinary, colorectal, breast, skin, unknown primary, hematological, stomach, lung, pancreas, and others | 80.4 (5.7) | 48.8% | Semi-structured interview was designed to identify eight of nine symptoms of diagnostic and Statistical Manual of Mental Disorders—IV (DSM-IV) criteria for a major depressive | Age, gender, living alone, with inpatient status, metastasis, mobility, functional status, pain, malnutrition, cognitive impairment, comorbidities, No of nonantidepressant drugs, polypharmacy, social support. | Inpatient status, inadequate social support, impaired mobility, cognitive impairment, polypharmacy, and cancer-related pain were associated depression. |
| [41] | Clark et al. (2016) | USA | Retrospective cohort study | N = 1785 | Colorectal | 78 (7) | 51% | Depression was defined as an affirmative answer to at least one of the three depression screening questions;—VR-12. | Age, race, gender, education, income, homeownership, marital status, tumor size, stage, and radiation therapy, No of months from CRC diagnosis to survey, No of comorbidities, impairment ADLs, age per 10 years) | Nonwhite race, ↓ income, comorbidities, impairment in ADLs were associated with depression. |
| [42] | Solvik et al. (2020) | Norway | Cross-sectional study | N = 174 | Breast, prostate, lymphoma, lung, colon, brain, rectal, bladder, ovarian and others | 77.4 (7.1) | 41% | Edmonton Symptom Assessment System Revised (ESAS-r) | Age, civil status, education, type of cancer, time since diagnosis, ongoing treatment, functional level, body mass index, fatigue, anxiety. | - ↑ pain was associated with higher scores of fatigues and anxiety and the women reported higher levels the anxiety and depression. - strong correlation between anxiety and depression. |
| [43] | Atag et al. (2018) | Turkey | Prospective study | N = 170 | Lung, gastrointestinal, breast, gynaecologic, genitourinary and other | 71.19 (5.03) | 47.1% | GDS | Age, gender, marital status); awareness of disease, stage, No of comorbidities, pain, time since diagnosis operated due to cancer, radiotherapy, social support. | - ↑ pain in patients with depressive symptoms. |
| [44] | Goldzweig et al. (2017) | Israel | Cross-sectional design | N = 90 | Prostate, lung, colorectal, breast | Patients 90.49 (2.40); Spouses 84.96 (9.87) | Patients = 55.6%; Spouses = 44.4%; | GDS Distress thermometer—1 item | Age of the patient, age of the caregiver, comorbidity, treatment, social support, hope | - ↑ patient´s age and ↓ the patient´s hope being cured were predictors of distress. |
| [45] | Okumura et al. (2020) | Japan | Cohort study | N = 48 | Gastrointestinal | 71 | 33% | GDS | Age, gender, marital history, level of education, depression at baseline, clinical stage, cancer type, performance status, complication, postoperative, adjuvant therapy, social frailty. | - Preoperative social frailty was associated with new-onset depressive symptoms. |
| [46] | Oserowskyet al. (2021) | USA | Retrospective cohort study | N = 5787 | Bladder | 77.4 (6.8) | 24% | Affirmative answer to at least one of the three depression screening questions;—VR-12. | Age, race, gender, education, income, marital status, smoking status, and homeownership, cancer stage, ADLs, self-reported comorbidities, general health. | - ↑Age, married, higher education were associated with a ↓ depression. General health, nonwhite race, income <$30,000, difficulties with ADL, stroke, muscular disease, and urinary issues were predictors of depression. |
| Criteria/Studies | [43] | [26] | [40] | [36] | [38] | [44] | [32] | [33] | [30] | [37] | [35] | [28] | [42] | [39] | [29] |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Inclusion criteria clearly defined | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Detailed description of subjects and setting | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Exposure measured in a valid and reliable way | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Objective criteria for measurement of the condition | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Confounding factors identified | No | No | Yes | Yes | No | No | Yes | No | Yes | Yes | No | Yes | No | Yes | Yes |
| Strategies for dealing with confounders | No | No | Yes | Yes | No | No | Yes | No | Yes | No | No | Yes | No | Yes | Yes |
| Results measured in a valid and reliable way | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | Yes |
| Appropriate statistical analysis | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Cohort Studies | [45] | [27] | [34] | [41] | [46] |
|---|---|---|---|---|---|
| Two groups similar and recruited from the same population | Yes | Yes | Yes | Yes | Yes |
| Exposures measured similarly to assign people to both exposed and unexposed groups | Yes | Yes | Yes | Yes | Yes |
| Exposure measured in a valid and reliable way | Yes | Yes | Yes | Yes | Yes |
| Objective criteria for measurement of the condition | Yes | Yes | Yes | Yes | Yes |
| Confounding factors identified | Yes | Yes | Yes | Yes | Yes |
| Strategies for dealing with confounders | Unclear | Yes | Yes | Yes | Yes |
| Participants free of the outcome at the start of the study | Yes | Yes | No | Unclear | Unclear |
| Outcomes measured in a valid and reliable way | Yes | Yes | Yes | Yes | Yes |
| The follow up time reported and sufficient to be long enough for outcomes to occur | Yes | Yes | Yes | Yes | Yes |
| Complete follow-up or presentation of the reasons for the loss of follow-up | Yes | Yes | Yes | Unclear | Unclear |
| Strategies to address incomplete follow up utilized | Yes | Yes | Yes | Unclear | Unclear |
| Appropriate statistical analysis | Yes | Yes | Yes | Yes | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, S.; Bártolo, A.; Santos, I.M.; Pereira, A.; Monteiro, S. Towards a Better Understanding of the Factors Associated with Distress in Elderly Cancer Patients: A Systematic Review. Int. J. Environ. Res. Public Health 2022, 19, 3424. https://doi.org/10.3390/ijerph19063424
Silva S, Bártolo A, Santos IM, Pereira A, Monteiro S. Towards a Better Understanding of the Factors Associated with Distress in Elderly Cancer Patients: A Systematic Review. International Journal of Environmental Research and Public Health. 2022; 19(6):3424. https://doi.org/10.3390/ijerph19063424
Chicago/Turabian StyleSilva, Sandra, Ana Bártolo, Isabel M. Santos, Anabela Pereira, and Sara Monteiro. 2022. "Towards a Better Understanding of the Factors Associated with Distress in Elderly Cancer Patients: A Systematic Review" International Journal of Environmental Research and Public Health 19, no. 6: 3424. https://doi.org/10.3390/ijerph19063424
APA StyleSilva, S., Bártolo, A., Santos, I. M., Pereira, A., & Monteiro, S. (2022). Towards a Better Understanding of the Factors Associated with Distress in Elderly Cancer Patients: A Systematic Review. International Journal of Environmental Research and Public Health, 19(6), 3424. https://doi.org/10.3390/ijerph19063424