
Prevalence of Adverse Childhood Experiences in Students with Emotional and Behavioral Disorders in Special Education Schools from a Multi-Informant Perspective

 , ,
, ,
Abstract
1. Introduction
1.1. Students with EBD in Special Education
1.2. Adverse Childhood Experiences
1.3. Adverse Childhood Experience in Students with EBD in SE
1.4. The Present Study
2. Materials and Methods
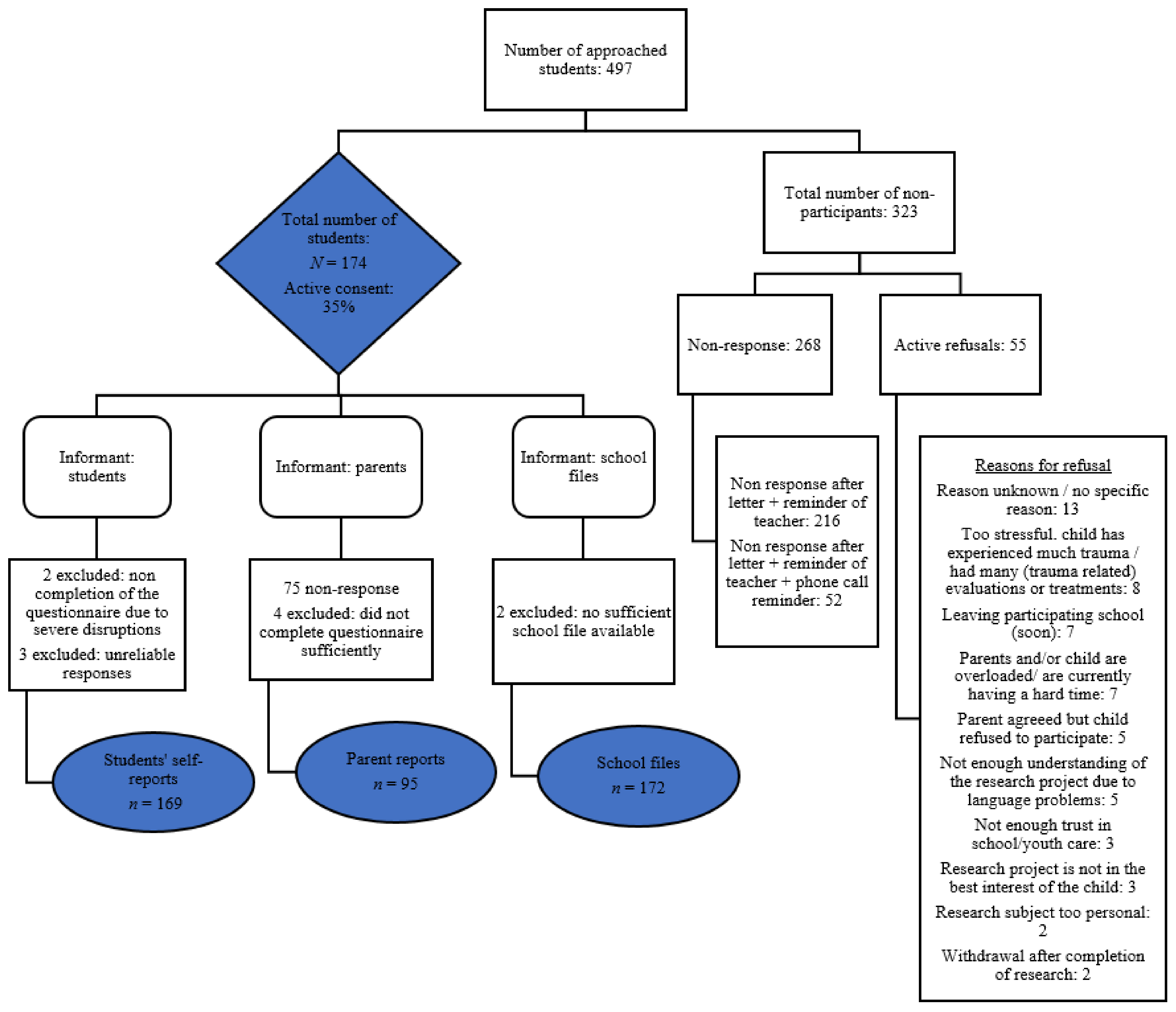
2.1. Sample
2.2. Design and Procedures
2.3. Measures
2.3.1. Measures of Student Self-Reports
2.3.2. Measures of Parent Reports
2.3.3. Measures of School File Reports
2.4. Data Analysis
3. Results
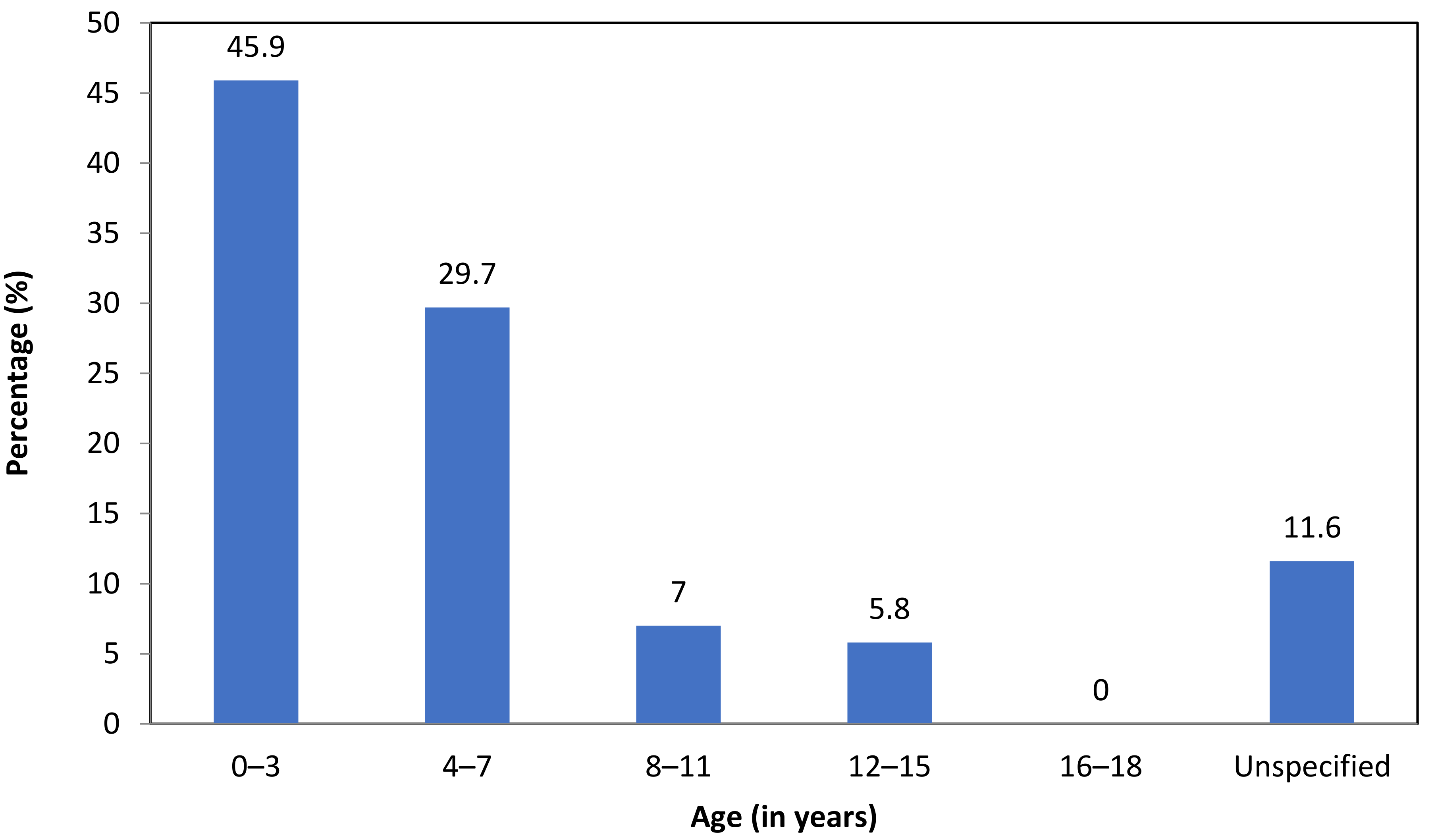
3.1. Prevalence, Type and Timing of ACEs
3.2. Demographic Characteristics, Diagnoses and the Prevalence of ACEs
4. Discussion
4.1. Clinical Implications
4.2. Limitations
4.3. Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| ACEs in the Life Events Checklist (LEC) of the Dutch version of the CAPS-CA for children and adolescents [71] |
| Natural disaster |
| Fire/explosion |
| Traffic accident |
| Other serious accident |
| Exposure to hazardous substances |
| Bullying |
| Physical abuse |
| Physical assault with a weapon |
| Experienced shooting |
| Experienced neighborhood violence or war |
| Emotional abuse |
| Domestic violence |
| Witnessed other people having sex or porn |
| Sexual abuse |
| Forced into doing something (non-sexual) |
| Stalking |
| Police arrest |
| Physical neglect |
| Supervisory neglect |
| Forced to be somewhere |
| Serious illness or close to dying |
| Witnessed other people injured or dead |
| Death of someone close |
| Hurting someone severely |
| Other severe or frightening events |
| ACEs used from the Dutch version of the ACE questionnaire a [73] |
| Parental substance abuse (alcohol and drugs) |
| Parental mental health problems |
| Household (attempted) suicide |
Appendix B
| ACEs | Operationalization [36,37,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,98] |
|---|---|
| Physical/supervisory neglect | A parent(s) or primary caregiver(s) behavior interfered with the child’s care, wearing dirty clothes/bad hygiene/not enough personal space/no safe living space/not enough to eat/no oversight to ensure a child’s safety, forced to take care of themselves. |
| Emotional neglect | A parent(s) or primary caregiver(s) didn’t make the child feel special and loved/the family not being a source of strength, protection and support or the child received little attention. |
| Medical neglect | A parent(s) or primary caregiver(s) failed to recognize or respond to the child’s medical needs: (1) Failure to heed obvious signs of serious illness (2) Not taken to a doctor when needed (3) Failure to follow a physician’s instructions once medical advice was sought. |
| Educational neglect | A parent(s) or primary caregiver(s) failed to send their child to school or a lack of parental involvement in learning. |
| Neglect unspecified | Neglect was reported in the school files without mention of the type of neglect. |
| Physical abuse | The child experienced pushing/beating/grabbing/slapping/kicking or being hit so hard by the parent(s) or primary caregiver(s) that it resulted in marks or injury. |
| Emotional abuse | The child was yelled at/insulted/threatened or put down by the parent(s) or primary caregiver(s). |
| Abuse unspecified | Abuse was reported in the school files without mention of the type of abuse. |
| Sexual abuse | The child was involuntarily touched in a sexual way/forced into any form of sexual contact/forced into watching sexual content. |
| Domestic violence | A household or family member(s) experienced a form of (recurring) violence within the home, either physically, sexually, psychologically or economically. The violence is aimed at someone (e.g., sibling/parent) within the household, also after a divorce), but not at the child directly. |
| Parental separation or divorce | The parents or primary caregivers were (temporarily or permanently) separated or divorced. |
| Parental mental health problems | (1) A parent(s) or primary caregiver(s) had mental health problems (symptoms or disorders) interfering with the child’s care. (2) A parent(s) or primary caregiver(s) ever attempted suicide. |
| Economic hardship | The household experienced frequent financial problems (e.g., debts), problems paying for basic needs such as food or rent/mortgage and/or experienced housing problems. |
| Many (sudden) relocations | The child experienced high frequency in changes of residence/relocations that were unplanned, unpredictable, disruptive and/or led to broken social ties and change(s) in schools. |
| Bad accident or physical illness of a parent | (1) A parent(s) or primary caregiver(s) was hospitalized more than once or had a (serious or life-threatening) chronic and/or somatic illness. (2) A parent(s) or primary caregiver(s) had a bad accident that caused serious injuries. |
| Parental substance abuse | A parent or primary caregiver(s) used excessive alcohol or drugs; the child is exposed to (excessive) substance abuse (alcohol or drugs) within the household. |
| Parental death | The child experienced the death of a parent(s) or primary caregiver(s) prior to 18 years of age. |
| Parental incarceration | A parent(s) or primary caregiver(s) was arrested and kept in detention in jail or prison. |
| Bullying | The child was bullied or experienced hurtful or harmful behavior enacted by one or more perpetrators who were more powerful, carried out repeatedly and over time. |
| Negative school experiences | (1) The child did not receive enough support from the previous school(s) for a successful school career. (2) The child experienced failure for not being able to adapt their behavior to the expectations of the teacher and classroom peers. |
| Victim of neighborhood violence | The child was a victim of or witnessed neighborhood violence such as being pressured/threatened/discriminated against or treated unfairly. |
| Separation from parents | The child was separated from a parent(s) or primary caregiver(s) because of out-of-home-placement/institutional rearing/foster care/orphanage/adoption. |
| Parental absence | (1) The child (temporarily) lost a parent because of divorce/hospitalization/emigration or abandonment. (2) The parent no longer lived with the child and made no effort to see or bond with the child for several months or years. |
| Medical trauma | The child experienced life-threatening or serious illness(es)/prolonged or repeated medical procedures/intensive medical procedures/invasive, stressful or frightening medical treatment/essential complex medicalprocedures during pregnancy, birth or postnatal—in the first days after birth. |
| Other | The child experienced other severe or frightening events, e.g., the death of a sibling, near-drowning. |
Appendix C
| Quality | Operationalization | ||
|---|---|---|---|
| Low | Incomplete school files: at least 50% of the reports for each section of the codebook, with the exception of demographic variables, was missing (reports on the students’ developmental history and school, youth health care and juvenile offending trajectories). | ||
| Moderate | Partially complete school files: at least 50% of the reports for the school and health care trajectories in the codebook were available. When psychological/child psychiatric evaluations have been completed, these reports should be available in the school file. | ||
| High | (Nearly) complete school files: each section of the codebook could be completed based on the (nearly full) presence of all available reports. | ||
| Quality | Primary special education (%) | Secondary special education (%) | Both school types combined (%) |
| n = 113 | n = 60 | n = 172 | |
| Low | 58.4 | 91.5 | 69.8 |
| Moderate | 38.1 | 8.5 | 27.9 |
| High | 3.5 | 0 | 2.3 |
Appendix D
| ACE | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | 23 | 24 | 25 | 26 | 27 | 28 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Natural disaster | – | |||||||||||||||||||||||||||
| 2 Fire/explosion | 0.235 ** | – | ||||||||||||||||||||||||||
| 3 Traffic accident | 0.220 ** | 0.206 ** | – | |||||||||||||||||||||||||
| 4 Other serious accident | 0.083 | 0.040 | 0.320 *** | – | ||||||||||||||||||||||||
| 5 Hazardous substances | 0.028 | 0.019 | −0.087 | 0.078 | – | |||||||||||||||||||||||
| 6 Bullying | 0.062 | 0.105 | 0.138 | 0.182 * | −0.053 | – | ||||||||||||||||||||||
| 7 Physical abuse | 0.134 | 0.178 * | 0.162 * | 0.096 | 0.050 | 0.389 *** | – | |||||||||||||||||||||
| 8 Physical assault with a weapon | 0.076 | 0.263 *** | 0.139 | 0.132 | 0.016 | 0.278 *** | 0.244 ** | – | ||||||||||||||||||||
| 9 Experienced shooting | 0.330 *** | 0.294 *** | 0.263 *** | 0.213 ** | 0.070 | 0.097 | 0.062 | 0.245 ** | – | |||||||||||||||||||
| 10 Experienced war or neighborhood violence | 0.252 ** | 0.188 * | 0.286 *** | 0.160 * | 0.032 | 0.044 | 0.128 | 0.255 *** | 0.264 *** | – | ||||||||||||||||||
| 11 Emotional abuse | 0.054 | 0.028 | 0.250 ** | 0.195 * | 0.079 | 0.261 *** | 0.256 *** | 0.176 * | 0.135 | 0.114 | – | |||||||||||||||||
| 12 Domestic violence | 0.051 | 0.071 | 0.152 * | 0.189 * | 0.049 | 0.265 *** | 0.182 * | 0.220 ** | 0.016 | 0.140 | 0.333 *** | – | ||||||||||||||||
| 13 Witnessed other people having sex or porn | 0.081 | 0.077 | 0.171 * | 0.264 *** | 0.116 | 0.189 * | 0.136 | 0.123 | 0.178 * | 0.185 * | 0.278 *** | 0.199 ** | – | |||||||||||||||
| 14 Sexual abuse | 0.041 | −0.034 | 0.172 * | 0.200 ** | −0.005 | 0.241 ** | 0.178 * | 0.177 * | 0.181 * | 0.172 * | 0.271 *** | 0.206 ** | 0.188 * | – | ||||||||||||||
| 15 Forced into doing something (non-sexual) | 0.094 | 0.060 | 0.194 * | 0.280 *** | 0.205 ** | 0.259 *** | 0.235 ** | 0.191 * | 0.267 *** | 0.137 | 0.192 * | 0.314 *** | 0.150 | 0.382 *** | – | |||||||||||||
| 16 Stalked | 0.183 * | 0.112 | 0.144 | 0.157 * | 0.053 | 0.244 ** | 0.141 | 0.331 *** | 0.227 ** | 0.299 *** | 0.233 ** | 0.220 * | 0.121 | 0.242 ** | 0.164 * | – | ||||||||||||
| 17 Police arrest of a family member | −0.014 | −0.061 | 0.103 | 0.070 | 0.019 | −0.080 | 0.049 | 0.110 | 0.086 | 0.110 | 0.036 | 0.181 * | 0.104 | −0.005 | 0.068 | 0.147 | – | |||||||||||
| 18 Physical neglect | 0.113 | −0.094 | 0.114 | 0.179 * | 0.043 | 0.152 * | 0.050 | 0.072 | 0.308 *** | 0.102 | 0.129 | 0.208 ** | 0.116 | 0.239 ** | 0.335 *** | 0.176 * | 0.152 * | – | ||||||||||
| 19 Supervisory neglect | 0.011 | −0.015 | 0.327 *** | 0.134 | 0.042 | 0.018 | −0.002 | 0.170 * | 0.231 ** | 0.296 *** | 0.046 | 0.164 * | 0.073 | 0.134 | 0.114 | 0.285 *** | −0.005 | 0.114 | – | |||||||||
| 20 Forced to be somewhere | 0.152 | 0.013 | 0.102 | 0.103 | 0.107 | 0.024 | 0.050 | 0.106 | 0.233 ** | 0.110 | 0.034 | 0.029 | 0.155 * | 0.105 | 0.079 | 0.106 | 0.091 | 0.289 *** | 0.185 * | – | ||||||||
| 21 Serious illness or close to dying through severe injury | 0.041 | 0.069 | 0.166 * | 0.114 | 0.219 ** | 0.185 * | 0.194 * | 0.229 ** | 0.160 * | 0.301 *** | 0.115 | 0.219 ** | 0.100 | 0.111 | 0.252 *** | 0.257 *** | 0.173 * | 0.141 | 0.166 * | 0.156 * | – | |||||||
| 22 Witnessed other people injured or dead | 0.100 | 0.116 | 0.197 * | 0.196 * | 0.218 ** | −0.016 | 0.083 | 0.074 | 0.086 | 0.023 | 0.099 | 0.081 | −0.014 | 0.046 | 0.109 | 0.032 | 0.043 | 0.085 | 0.085 | 0.034 | 0.076 | – | ||||||
| 23 Death of someone close | 0.111 | 0.072 | 0.268 *** | 0.099 | 0.109 | 0.080 | 0.072 | 0.055 | 0.109 | 0.026 | 0.171 * | 0.087 | 0.062 | 0.057 | 0.088 | −0.003 | 0.096 | 0.058 | 0.101 | 0.078 | 0.122 | 0.287 *** | – | |||||
| 24 Hurting someone severely | −0.059 | 0.092 | 0.182 * | 0.164 * | 0.010 | 0.148 | 0.169 * | 0.238 ** | 0.034 | 0.116 | 0.430 *** | 0.207 ** | 0.079 | 0.091 | 0.188 * | 0.224 ** | 0.097 | −0.040 | 0.085 | 0.012 | 0.199 ** | 0.097 | 0.158 * | – | ||||
| 25 Other severe or frightening event | 0.100 | 0.137 | 0.225 ** | 0.146 | 0.155 * | 0.167 * | 0.202 ** | 0.254 *** | 0.110 | 0.187 * | 0.259 *** | 0.213 ** | 0.205 ** | 0.169 * | 0.204 ** | 0.118 | 0.042 | 0.096 | 0.252 *** | 0.136 | 0.098 | 0.116 | 0.157 * | 0.246 ** | – | |||
| 26 Parental substance abuse | −0.100 | 0.021 | 0.195 * | 0.148 | 0.000 | 0.110 | 0.127 | 0.016 | 0.006 | 0.021 | 0.256 *** | 0.085 | 0.273 *** | 0.331 *** | 0.197 * | 0.018 | 0.109 | 0.250 ** | −0.080 | 0.042 | 0.060 | 0.056 | 0.082 | −0.006 | 0.184 * | – | ||
| 27 Parental mental health problems | 0.235 ** | 0.017 | 0.110 | 0.056 | 0.058 | 0.159 * | 0.083 | 0.173 * | −0.077 | 0.088 | 0.205 ** | 0.204 ** | 0.161 * | 0.219 ** | 0.192 * | 0.286 *** | 0.066 | 0.210 ** | 0.052 | 0.082 | 0.251 ** | 0.019 | 0.062 | 0.141 | 0.128 | 0.113 | – | |
| 28 Household (attempted) suicide | 0.072 | 0.077 | 0.216 ** | 0.086 | 0.022 | 0.143 | 0.087 | 0.223 ** | 0.178 * | 0.062 | 0.100 | 0.095 | 0.250 ** | 0.116 | 0.093 | 0.121 | 0.045 | 0.304 *** | 0.073 | 0.155 * | 0.100 | 0.104 | 0.107 | 0.034 | 0.205 ** | 0.052 | 0.161 * | – |
Appendix E
| ACE | 1 | 2 | 3 | 4 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 21 | 22 | 23 | 24 | 25 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Natural disaster | – | ||||||||||||||||||||||
| 2 Fire/explosion | 0.095 | – | |||||||||||||||||||||
| 3 Traffic accident | 0.010 | 0.158 | – | ||||||||||||||||||||
| 4 Other serious accident | −0.099 | 0.104 | 0.011 | – | |||||||||||||||||||
| 6 Bullying | −0.054 | −0.022 | 0.029 | −0.042 | – | ||||||||||||||||||
| 7 Physical abuse | 0.182 | 0.073 | 0.187 | 0.110 | 0.339 *** | – | |||||||||||||||||
| 8 Physical assault with a weapon | −0.061 | 0.033 | 0.035 | −0.028 | 0.047 | 0.157 | – | ||||||||||||||||
| 9 Experienced shooting | −0.036 | −0.057 | 0.221 * | 0.079 | 0.087 | −0.029 | – | ||||||||||||||||
| 10 Experienced war or neighborhood violence | −0.045 | −0.063 | 0.008 | −0.099 | 0.012 | −0.036 | 0.342 *** | −0.022 | – | ||||||||||||||
| 11 Emotional abuse | −0.131 | 0.098 | 0.132 | 0.089 | 0.388 *** | 0.416 *** | 0.008 | 0.092 | 0.081 | – | |||||||||||||
| 12 Domestic violence | −0.020 | −0.001 | 0.025 | 0.238 * | 0.206 * | 0.454 *** | 0.083 | −0.067 | 0.094 | 0.483 *** | – | ||||||||||||
| 13 Witnessed other people having sex or porn | 0.061 | 0.050 | −0.157 | −0.028 | 0.108 | 0.157 | 0.229 * | −0.029 | 0.141 | 0.251 * | 0.083 | – | |||||||||||
| 14 Sexual abuse | −0.032 | −0.049 | 0.092 | −0.070 | 0.114 | 0.126 | −0.042 | −0.015 | −0.031 | 0.133 | 0.069 | 0.239 * | – | ||||||||||
| 15 Forced into doing something (non−sexual) | 0.109 | 0.004 | 0.076 | 0.129 | 0.097 | 0.201 | 0.184 | −0.033 | 0.290 ** | 0.216 * | 0.422 *** | 0.184 | 0.203 | – | |||||||||
| 16 Stalked | 0.216 * | 0.098 | 0.132 | 0.038 | 0.161 | 0.071 | 0.141 | −0.022 | 0.217 * | 0.187 | 0.209 * | −0.059 | −0.031 | 0.111 | – | ||||||||
| 17 Police arrest of a family member | −0.084 | 0.087 | 0.088 | 0.150 | 0.136 | 0.169 | 0.134 | −0.040 | 0.393 *** | 0.336 *** | 0.308 ** | 0.256 * | −0.057 | 0.417 *** | 0.235 * | – | |||||||
| 18 Physical neglect | −0.045 | −0.074 | 0.008 | 0.175 | 0.161 | 0.178 | 0.141 | −0.022 | 0.217 * | 0.187 | 0.324 ** | 0.141 | 0.334 *** | 0.290 ** | 0.217 * | 0.235 * | – | ||||||
| 19 Supervisory neglect | −0.032 | −0.051 | 0.093 | −0.069 | 0.113 | 0.124 | 0.239 * | −0.015 | 0.334 *** | 0.131 | 0.227 * | 0.239 * | 0.489 *** | 0.453 *** | 0.334 *** | 0.165 | 0.699 *** | – | |||||
| 21 Serious illness or close to dying through severe injury | −0.066 | 0.265 * | 0.011 | 0.253 * | 0.153 | 0.102 | 0.060 | −0.031 | −0.064 | 0.270 ** | 0.303 ** | 0.205 * | 0.219 * | 0.290 ** | 0.314 * | 0.112 | 0.314 ** | 0.220 * | – | ||||
| 22 Witnessed other people injured or dead | 0.159 | −0.084 | −0.142 | −0.011 | −0.015 | −0.132 | −0.074 | −0.027 | 0.161 | −0.028 | −0.075 | 0.092 | −0.027 | −0.085 | 0.161 | 0.029 | −0.055 | −0.038 | −0.080 | – | |||
| 23 Death of someone close | 0.056 | 0.030 | −0.036 | 0.049 | 0.197 | 0.222 * | −0.045 | −0.078 | −0.049 | 0.187 | 0.139 | 0.124 | 0.045 | −0.094 | 0.061 | 0.041 | −0.049 | −0.111 | 0.088 | 0.263 * | – | ||
| 24 Hurting someone severely | −0.086 | −0.030 | 0.070 | −0.028 | 0.278 ** | 0.025 | 0.122 | −0.041 | 0.374 *** | 0.293 ** | 0.280 ** | 0.005 | −0.059 | 0.290 ** | 0.069 | 0.308 ** | 0.069 | 0.155 | 0.100 | 0.021 | −0.045 | – | |
| 25 Other severe or frightening event | 0.097 | 0.114 | −0.109 | 0.017 | 0.097 | 0.150 | 0.166 | −0.035 | 0.270 ** | 0.236 * | 0.230 * | 0.297 ** | −0.051 | 0.123 | 0.270 ** | 0.282 ** | 0.099 | 0.189 | −0.104 | 0.192 | 0.171 | 0.362 *** | – |
Appendix F
| ACE | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 Physical/supervisory neglect | – | |||||||||||||||||||||
| 2 Psychological neglect | 0.200 ** | – | ||||||||||||||||||||
| 3 Medical neglect | 0.076 | 0.218 ** | – | |||||||||||||||||||
| 4 Educational neglect | 0.054 | 0.160 * | 0.195 ** | – | ||||||||||||||||||
| 5 Physical abuse | 0.191 ** | 0.163 * | 0.107 | 0.184 * | – | |||||||||||||||||
| 6 Emotional abuse | 0.195 * | 0.175 * | 0.062 | 0.173 * | 0.494 *** | – | ||||||||||||||||
| 7 Sexual abuse | 0.050 | 0.007 | 0.061 | −0.070 | 0.102 | 0.080 | – | |||||||||||||||
| 8 Domestic violence | 0.121 | 0.198 ** | 0.306 *** | 0.179 * | 0.246 ** | 0.093 | 0.076 | – | ||||||||||||||
| 9 Parental separation or divorce | 0.111 | 0.104 | −0.003 | 0.053 | 0.074 | 0.017 | −0.122 | 0.290 *** | – | |||||||||||||
| 10 Parental death | −0.101 | −0.046 | 0.075 | −0.066 | −0.104 | −0.040 | −0.052 | −0.083 | −0.213 ** | – | ||||||||||||
| 11 Parental incarceration | 0.037 | −0.034 | 0.092 | 0.046 | 0.034 | −0.028 | 0.084 | 0.188 * | 0.096 | −0.045 | – | |||||||||||
| 12 Parental mental health problems | 0.210 ** | 0.268 *** | 0.045 | 0.058 | 0.175 * | 0.109 | −0.002 | 0.210 ** | 0.148 | 0.018 | 0.040 | – | ||||||||||
| 13 Medical trauma | 0.032 | −0.062 | −0.100 | −0.088 | 0.089 | 0.025 | 0.089 | 0.017 | −0.043 | −0.106 | −0.023 | 0.101 | – | |||||||||
| 14 Bullying | 0.125 | −0.083 | −0.164 * | −0.071 | 0.220 ** | 0.185 * | −0.052 | −0.098 | −0.050 | 0.141 | −0.143 | 0.029 | 0.242 ** | – | ||||||||
| 15 Bad accident or physical illness of a parent | 0.152 * | 0.140 | −0.001 | −0.025 | 0.049 | 0.041 | 0.167 * | 0.071 | −0.045 | −0.102 | 0.060 | 0.223 ** | 0.016 | −0.058 | – | |||||||
| 16 Parental substance abuse | 0.253 *** | 0.213 ** | 0.213 ** | 0.186 * | 0.207 ** | 0.129 | 0.097 | 0.382 *** | 0.187 * | −0.073 | 0.129 | 0.299 *** | 0.092 | −0.064 | 0.104 | – | ||||||
| 17 Economic hardships | 0.274 *** | 0.166 * | 0.056 | 0.114 | 0.236 ** | 0.257 *** | 0.141 | 0.178 * | 0.119 | −0.043 | 0.115 | 0.220 ** | −0.019 | 0.111 | 0.262 *** | 0.075 | – | |||||
| 18 Many (sudden) relocations | 0.075 | 0.168 * | 0.038 | 0.137 | 0.228 ** | 0.033 | 0.162 * | 0.292 *** | 0.062 | 0.040 | 0.286 *** | 0.241 ** | 0.048 | 0.029 | 0.183 * | 0.250 *** | 0.139 | – | ||||
| 19 Parental absence | 0.148 | 0.081 | 0.109 | 0.271 *** | 0.186 * | 0.143 | 0.015 | 0.062 | 0.131 | −0.071 | 0.238 ** | 0.068 | −0.050 | −0.094 | 0.064 | 0.162 * | −0.013 | 0.162 * | – | |||
| 20 Victim of neighborhood violence | −0.137 | −0.098 | −0.075 | −0.057 | −0.073 | −0.094 | −0.045 | −0.054 | 0.007 | −0.042 | −0.039 | −0.069 | 0.072 | −0.064 | 0.080 | −0.063 | −0.096 | −0.089 | −0.061 | – | ||
| 21 Negative school experiences | −0.008 | 0.070 | 0.114 | 0.084 | 0.100 | 0.127 | −0.008 | 0.108 | 0.102 | 0.002 | −0.077 | 0.072 | 0.004 | 0.006 | 0.016 | 0.379 *** | 0.253 *** | −0.036 | 0.003 | 0.026 | – | |
| 22 Separation from parents | 0.155 * | 0.084 | 0.116 | 0.065 | 0.064 | −0.030 | 0.217 ** | 0.251 *** | 0.087 | −0.131 | 0.212 ** | 0.135 | 0.157 * | −0.103 | 0.075 | 0.028 | 0.272 *** | 0.174 * | 0.031 | −0.101 | – |
References
- Crouch, E.; Radcliff, E.; Bennett, K.J.; Brown, M.J.; Hung, P. Examining the relationship between adverse childhood experiences and ADHD diagnosis and severity. Acad. Pediatr. 2021, 21, 1388–1394. [Google Scholar] [CrossRef] [PubMed]
- Liming, K.W.; Grube, W.A. Wellbeing outcomes for children exposed to multiple adverse experiences in early childhood: A systematic review. Child Adolesc. Soc. Work J. 2018, 35, 317–335. [Google Scholar] [CrossRef]
- Nelson, C.A.; Scott, R.D.; Bhutta, Z.A.; Harris, N.B.; Danese, A.; Samara, M. Adversity in childhood is linked to mental and physical health throughout life. BMJ 2020, 371, m3048. [Google Scholar] [CrossRef] [PubMed]
- Offerman, E.C.P.; Asselman, M.W.; Helmond, P.E.; Stams, G.J.; Lindauer, R.J.L. The Prevalence and Type of Adverse Childhood Experiences in Students with Emotional Behavioral Disorders Receiving Special Education: A Systematic Review; Academic Medical Center: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Breeman, L.D. A Special Need for Others: Social Classroom Relationships and Behavioral Problems in Children with Psychiatric Disorders in Special Education. Ph.D. Thesis, Erasmus University Medical Center, Rotterdam, The Netherlands, 2015. [Google Scholar]
- Little, M.; Kobak, R. Emotional security with teachers and children’s stress reactivity: A comparison of special-education and regular-education classrooms. J. Clin. Child. Adolesc. Psychol. 2003, 32, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, B.P.; Bruhn, A.L.; Sutherland, K.S.; Bradshaw, C.P. Progress and priorities in research to improve outcomes for students with or at risk for emotional and behavioral disorders. Behav. Disord. 2019, 44, 85–96. [Google Scholar] [CrossRef]
- Stoutjesdijk, R.; Scholte, E.M.; Swaab, H. Special needs characteristics of children with emotional and behavioral disorders that affect inclusion in regular education. J. Emot. Behav. Disord. 2012, 20, 92–104. [Google Scholar] [CrossRef]
- Zweers, I.; Tick, N.T.; Bijstra, J.O.; van de Schoot, R. How do included and excluded students with SEBD function socially and academically after 1,5 year of special education services? Eur. J. Dev. Psychol. 2020, 17, 317–335. [Google Scholar] [CrossRef]
- Bradley, R.; Doolittle, J.; Bartolotta, R. Building on the data and adding to the discussion: The experiences and outcomes of students with emotional disturbance. J. Behav. Educ. 2008, 17, 4–23. [Google Scholar] [CrossRef]
- O’Connell, M.E.; Boat, T.; Warner, K.E. Preventing Mental, Emotional, and Behavioral Disorders among Young People: Progress and Possibilities; U.N. Charter art. 28, 29; The National Academies Press: Washington, DC, USA, 2009; pp. 17–19. ISBN 978-030-912-674-8. [Google Scholar]
- United Nations. Convention on the Rights of the Child; Treaty Series; United Nations: New York, NY, USA, 1990; p. 3, Article 28, 29. [Google Scholar]
- Kauffman, J.M.; Landrum, T.J. Characteristics of Emotional and Behavioral Disorders of Children and Youth with Disabilities, 11th ed.; Pearson: Upper Saddle River, NJ, USA, 2018; pp. 63–65, 112–125, 149–264. ISBN 978-013-444-990-6. [Google Scholar]
- Stephens, S.A.; Lakin, K.C. Where students with emotional and behavioral disorders go to school. In Issues in Educational Placement: Students with Emotional Behavioral Disorders, 1st ed.; Kauffman, J.M., Lloyd, J.W., Hallahan, D.P., Astuto, T.A., Eds.; Erlbaum: Hillsdale, NJ, USA, 1995; pp. 47–74. ISBN 978-080-581-533-7. [Google Scholar]
- Individuals with Disability Education Act Amendments of 1997. 1997. Available online: https://www.congress.gov/105/plaws/publ17/PLAW-105publ17.pdf (accessed on 30 August 2021).
- McLeskey, J.; Landers, E.; Williamson, P.; Hoppey, D. Are we moving toward educating students with disabilities in less restrictive settings? J. Spec. Educ. 2012, 46, 131–140. [Google Scholar] [CrossRef]
- United Nations Educational, Scientific and Cultural Organization. The Salamanca Statement and Framework for Action on Special Needs Education. In Proceedings of the World Conferenceon Special Needs Education: Access and Quality, Salamanca, Spain, 7–10 June 1994. [Google Scholar]
- Popham, M.; Counts, J.; Ryan, J.B.; Katsiyannis, A. A systematic review of self-regulation strategies to improve academic outcomes of students with EBD. J. Res. Spec. Educ. Needs 2018, 18, 239–253. [Google Scholar] [CrossRef]
- Schoenfeld, N.A.; Janney, D.M. Identification and treatment of anxiety in students with emotional or behavioral disorders: A review of the literature. Educ. Treat. Child 2008, 31, 583–610. [Google Scholar] [CrossRef]
- Wagner, M.; Kutash, K.; Duchnowski, A.J.; Epstein, M.H.; Sumi, W.C. The children and youth we serve: A national picture of the characteristics of students with emotional disturbances receiving special education. J. Emot. Behav. Disord. 2005, 13, 79–96. [Google Scholar] [CrossRef]
- Trout, A.L.; Hagaman, J.; Casey, K.; Reid, R.; Epstein, M.H. The academic status of children and youth in out-of-home care: A review of the literature. Child. Youth Serv. Rev. 2008, 30, 979–994. [Google Scholar] [CrossRef]
- Binsbergen, M.; van Koopman, P.; Lourens, J. In één Hand: Specialistische Jeugdhulp in Het Speciaal Onderwijs (In One Hand: Specialized Youthcare in Special Education (Report No. 1037, Project No. 40795)); Kohnstamm Instituut: Amsterdam, The Netherlands, 2020; ISBN 978-946-321-108-6. [Google Scholar]
- Smeets, E. Speciaal of Apart: Onderzoek Naar de Omvang van Het Speciaal Onderwijs in Nederland en Andere Europese Landen (Special or Different: Research into the Size of Special Education in the Netherlands and Other European Countries (BOPO-Projectnr: 413-06-009)); ITS, Radboud Universiteit: Nijmegen, The Netherlands, 2007; ISBN 978-905-554-333-5. [Google Scholar]
- Zweers, I. “Shape Sorting” Students for Special Education Services? A Study on Placement Choices and Social-Emotional and Academic Functioning of Students with SEBD in Inclusive and Exclusive Settings. Ph.D. Thesis, Utrecht University, Utrecht, The Netherlands, 2018. [Google Scholar]
- Ministerie van Onderwijs, Cultuur en Wetenschap. Rapport: Trends in Passend Onderwijs 2011–2019. Ministry of Education, Culture and Science. Report: Trends in Inclusive Education 2011–2019. 2020. Available online: https://www.rijksoverheid.nl/documenten/rapporten/2018/06/25/trends-in-passend-onderwijs-2014-2017 (accessed on 6 December 2021).
- Nurmi, J. Students’ characteristics and teacher-child relationships in instruction: A meta-analysis. Educ. Res. Rev. 2012, 7, 177–197. [Google Scholar] [CrossRef]
- Ledoux, G.; Waslander, S. Evaluatie Passend Onderwijs: Eindrapport (Evaluation Education That Fits: Final Report (Report No. 1046, Project No. 20689)); Kohnstamm Instituut: Amsterdam, The Netherlands, 2020; ISBN 978-946-321-113-0. [Google Scholar]
- Gilmour, A.F.; Wehby, J.H. The association between teaching students with disabilities and teacher turnover. J. Educ. Psychol. 2020, 112, 1042. [Google Scholar] [CrossRef]
- Nichols, A.S.; LaPlante Sosnowsky, F. Burnout among special education teachers in self-contained cross-categorical classrooms. Teach. Educ. Spec. Educ. 2002, 25, 71–86. [Google Scholar] [CrossRef]
- Singh, K.; Billingsley, B.S. Intent to stay in teaching: Teachers of students with emotional disorders versus other special educators. Remedial Spec. Educ. 1996, 17, 37–47. [Google Scholar] [CrossRef]
- Wisniewski, L.; Gargiulo, R.M. Occupational stress and burnout among special educators: A review of the literature. J. Spec. Educ. 1997, 31, 325–346. [Google Scholar] [CrossRef]
- Rombouts, M.; Scheffers-van Schayck, T.; van Dorsselaer, S.; Kleinjan, M.; Onrust, S.; Monshouwer, K. Het Gebruik van Tabak, Alcohol, Cannabis en Andere Middelen in Het Praktijkonderwijs en Cluster 4-Onderwijs (The Use of Tobacco, Alcohol, Cannabis and Other Substances in Practical Education and EBD); Trimbos-Instituut: Utrecht, The Netherlands, 2020. [Google Scholar]
- Bethell, C.D.; Carle, A.; Hudziak, J.; Gombojav, N.; Powers, K.; Wade, R.; Braveman, P. Methods to assess adverse childhood experiences of children and families: Toward approaches to promote child well-being in policy and practice. Acad. Pediatr. 2017, 17, S51–S69. [Google Scholar] [CrossRef]
- Marsman-Bonekamp, V.A.M. Beyond Disease and Disorder: Exploring the Long-Lasting Impact of Childhood Adversity in Relation to Mental Health. Ph.D. Thesis, Maastricht University, Maastricht, The Netherlands, 2021. [Google Scholar] [CrossRef]
- Asmundson, G.G.J.G.; Afifi, T.O. (Eds.) Adverse Childhood Experiences: Using Evidence to Advance Research, Practice, Policy, and Prevention; Elsevier: London, UK, 2019; pp. 17–31, 35–42, 220–222. ISBN 978-012-816-065-7. [Google Scholar]
- Felitti, V.J.; Anda, R.F.; Nordenberg, D.; Williamson, D.F.; Spitz, A.M.; Edwards, V.; Marks, J.S. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. Am. J. Prev. Med. 1998, 14, 245–258. [Google Scholar] [CrossRef]
- Kalmakis, K.A.; Chandler, G.E. Adverse childhood experiences: Towards a clear conceptual meaning. J. Adv. Nurs. 2013, 70, 1489–1501. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, K.A. Future directions in childhood adversity and youth psychopathology. J. Clin. Child Adolesc. Psychol. 2016, 45, 361–382. [Google Scholar] [CrossRef] [PubMed]
- Clarkson Freeman, P.A. Prevalence and relationship between adverse childhood experiences and child behavior among young children. Infant Ment. Health J. 2014, 35, 544–554. [Google Scholar] [CrossRef] [PubMed]
- Hamby, S.; Elm, J.H.; Howell, K.H.; Merrick, M.T. Recognizing the cumulative burden of childhood adversities transforms science and practice for trauma and resilience. Am. Psychol. 2021, 76, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.; Bellis, M.A.; Hardcastle, K.A.; Sethi, D.; Butchart, A.; Mikton, C.; Jones, L.; Dunne, M.P. The effect of multiple adverse childhood experiences on health: A systematic review and meta-analysis. Lancet Public Health 2017, 2, 356–366. [Google Scholar] [CrossRef]
- Oh, D.L.; Jerman, P.; Marques, S.S.; Koita, K.; Boparai, S.K.P.; Harris, N.B.; Bucci, M. Systematic review of pediatric health outcomes associated with childhood adversity. BMC Pediatr. 2018, 18, 83. [Google Scholar] [CrossRef]
- Carlson, J.S.; Yohannan, J.; Darr, C.L.; Turley, M.R.; Larez, N.A.; Perfect, M.M. Prevalence of adverse childhood experiences in school-aged youth: A systematic review (1990–2015). Int. J. Sch. Educ. Psychol. 2019, 8, 2–23. [Google Scholar] [CrossRef]
- Alisic, E.; Zalta, A.K.; van Wesel, F.; Larsen, S.E.; Hafstad, G.S.; Hassanpour, K.; Smid, G.E. Rates of post-traumatic stress disorder in trauma-exposed children and adolescents: Meta-analysis. Br. J. Psychiatry 2014, 204, 335–340. [Google Scholar] [CrossRef]
- Berg, K.L.; Acharya, K.; Shiu, C.S.; Msall, M.E. Delayed diagnosis and treatment among children with autism who experience adversity. J. Autism Dev. Disord. 2018, 48, 45–54. [Google Scholar] [CrossRef]
- Bosquet Enlow, M.; Egeland, B.; Blood, E.A.; Wright, R.O.; Wright, R.J. Interpersonal trauma exposure and cognitive development in children to age 8 years: A longitudinal study. J. Epidemiol. Community Health 2012, 66, 1005–1010. [Google Scholar] [CrossRef]
- Connor, D.F.; Ford, J.D.; Arnsten, A.F.; Greene, C.A. An update on posttraumatic stress disorder in children and adolescents. Clin. Pediatr. 2015, 54, 517–528. [Google Scholar] [CrossRef] [PubMed]
- Hunt, T.K.A.; Slack, K.S.; Berger, L.M. Adverse childhood experiences and behavioral problems in middle childhood. Child Abuse Negl. 2017, 67, 391–402. [Google Scholar] [CrossRef] [PubMed]
- Kalmakis, K.A.; Chiodo, L.M.; Kent, N.; Meyer, J.S. Adverse childhood experiences, post-traumatic stress disorder symptoms, and self-reported stress among traditional and nontraditional college students. J. Am. Coll. Health 2020, 68, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Kerns, C.M.; Newschaffer, C.J.; Berkowitz, S.; Lee, B.K. Brief report: Examining the association of autism and adverse childhood experiences in the national survey of children’s health: The important role of income and co-occurring mental health conditions. J. Autism Dev. Disord. 2017, 47, 2275–2281. [Google Scholar] [CrossRef] [PubMed]
- Perfect, M.M.; Turley, M.R.; Carlson, J.S.; Yohanna, J.; Saint Gilles, M.P. School-related outcomes of traumatic event exposure and traumatic stress symptoms in students: A systematic review of research from 1990 to 2015. School Ment. Health 2016, 8, 7–43. [Google Scholar] [CrossRef]
- Ploeg, J.D. Gedragsproblemen: Ontwikkelingen en Risico’s (Behavioral Problems: Developments and Risks), 11th ed.; Lemniscaat: Rotterdam, The Netherlands, 2014; pp. 92–96. ISBN 978-905-637-927-8. [Google Scholar]
- Lacey, R.E.; Howe, L.D.; Kelly-Irving, M.; Bartley, M.; Kelly, Y. The clustering of adverse childhood experiences in the Avon longitudinal study of parents and children: Are gender and poverty important? J. Interpers. Violence 2020, 1–24. [Google Scholar] [CrossRef]
- Walsh, D.; McCartney, G.; Smith, M.; Armour, G. Relationship between childhood socioeconomic position and adverse childhood experiences (ACEs): A systematic review. J. Epidemiol. Community Health 2019, 73, 1087–1093. [Google Scholar] [CrossRef]
- Frothingham, T.E.; Hobbs, C.J.; Wynne, J.M.; Yee, L.; Goyal, A.; Wadsworth, D.J. Follow up study eight years after diagnosis of sexual abuse. Arch. Dis. Child. 2000, 83, 132–134. [Google Scholar] [CrossRef][Green Version]
- Jonson-Reid, M.; Drake, B.; Kim, J.; Porterfield, S.; Han, L. A prospective analysis of the relationship between reported child maltreatment and special education eligibility among poor children. Child Maltreat. 2004, 9, 382–394. [Google Scholar] [CrossRef]
- Leiter, J.; Johnsen, M.C. Child maltreatment and school performance declines: An event-history analysis. Am. Educ. Res. J. 1997, 34, 563–589. [Google Scholar] [CrossRef]
- Scarborough, A.A.; McCrae, J.S. School-age special education outcomes of infants and toddlers investigated for maltreatment. Child. Youth Serv. Rev. 2010, 32, 80–88. [Google Scholar] [CrossRef]
- Barylnik, J. Psychopathology, psychosocial characteristics and family environment in juvenile delinquents. Ger. J. Psychiatry 2003, 6, 30–32. [Google Scholar]
- Oseroff, A.; Oseroff, C.E.; Westling, D.; Gessner, L.J. Teachers’ beliefs about maltreatment of students with emotional/behavioral disorders. Behav. Disord. 1999, 24, 197–209. [Google Scholar] [CrossRef]
- Portwood, S.G.; Lawler, M.J.; Roberts, M.C. Science, practice, and policy related to adverse childhood experiences: Framing the conversation. Am. Psychol. 2021, 76, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Cronholm, P.F.; Forke, C.M.; Wade, R.; Bair-Merritt, M.H.; Davis, M.; Harkins-Schwarz, M.; Pachter, L.M.; Fein, J.A. Adverse childhood experiences: Expanding the concept of adversity. Am. J. Prev. Med. 2015, 49, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Finkelhor, D.; Shattuck, A.; Turner, H.; Hamby, S. Improving the adverse childhood experiences study scale. JAMA Pediatr. 2013, 167, 70–75. [Google Scholar] [CrossRef]
- Danese, A. Annual Research Review: Rethinking childhood trauma-new research directions for measurement, study design and analytical strategies. J. Child. Psychol. Psychiatry 2020, 61, 236–250. [Google Scholar] [CrossRef]
- Stover, C.S.; Hahn, H.; Im, J.J.; Berkowitz, S. Agreement of parent and child reports of trauma exposure and symptoms in the early aftermath of a traumatic event. Psychol. Trauma Theory Res. Pract. Policy 2010, 2, 159–168. [Google Scholar] [CrossRef]
- Zelechoski, A.D.; Cross, H.L.; Luehrs, R.; Freedle, A.; Bruick, S.; Harrison, K.; Harrynen, A.; Hrebic, L.; Dibley, E.; Will, K. Trauma assessment in juvenile justice: Are we asking the right questions in the right ways? J. Aggress. Maltreat. Trauma 2021, 30, 324–346. [Google Scholar] [CrossRef]
- Gubbels, J.; Assink, M.; Prinzie, P.; van der Put, C.E. Why healthcare and education professionals underreport suspicions of child abuse: A qualitative study. Soc. Sci. 2021, 10, 98. [Google Scholar] [CrossRef]
- Nader, K.; Kriegler, J.; Blake, D.; Pynoos, R.; Newman, E.; Weathers, F. Clinician Administered PTSD Scale for Children and Adolescents for DSM-IV (CAPS-CA); Current and Lifetime Diagnostic Version, and Instruction Manual; National Center for PTSD: Boston, MS, USA; UCLA Trauma Psychiatry Program: Los Angeles, CA, USA, 1996. [Google Scholar]
- Diehle, J.; de Roos, C.; Boer, F.; Lindauer, R.J.L. A cross-cultural validation of the clinician administered PTSD scale for children and adolescents in a Dutch population. Eur. J. Psychotraumatol. 2013, 4, 19896. [Google Scholar] [CrossRef] [PubMed]
- Van Meijel, E.P.M.; Verlinden, E.; Diehle, J.; Lindauer, R.J.L. Clinician-Administered PTSD Scale for Children and Adolescents (CAPS-CA), Nederlandse Vertaling; Bohn Stafleu van Loghum: Houten, The Netherlands, 2013. [Google Scholar]
- Gray, M.J.; Litz, B.T.; Hsu, J.L.; Lombardo, T.W. Psychometric properties of the life events checklist. Assessment 2004, 11, 330–341. [Google Scholar] [CrossRef] [PubMed]
- Vink, R.; Pal, S.; Eekhout, I.; Pannebakker, F.; Mulder, T. Ik Heb al Veel Meegemaakt: Ingrijpende Jeugdervaringen (ACE) Bij Leerlingen in Groep 7/8 van Het Regulier Basisonderwijs (I Have Experienced a Lot: Adverse Childhood Experiences (ACE) with Students in Class 7/8 in Mainstream Primary Education (Report Number TNO 2016 R11157)); TNO: Leiden, The Netherlands, 2016. [Google Scholar]
- Anda, R.F.; Felitti, V.J.; Bremner, J.D.; Walker, J.D.; Whitfield, C.H.; Perry, B.D.; Dube, S.R.; Giles, W.H. The enduring effects of abuse and related adverse experiences in childhood. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 174–186. [Google Scholar] [CrossRef] [PubMed]
- Balistreri, K.S.; Alvira-Hammond, M. Adverse childhood experiences, family functioning and adolescent health and emotional well-being. Public Health 2016, 132, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Blodgett, C.; Lanigan, J.D. The association between adverse childhood experience (ACE) and school success in elementary school children. Sch. Psychol. Q. 2018, 33, 137–146. [Google Scholar] [CrossRef]
- Braveman, P.; Heck, K.; Egerter, S.; Rinki, C.; Marchi, K.; Curtis, M. Economic hardship in childhood: A neglected issue in ACE studies? Matern. Child Health J. 2018, 22, 308–317. [Google Scholar] [CrossRef]
- Dennis, C.H.; Clohessy, D.S.; Stone, A.L.; Darnall, B.D.; Wilson, A.C. Adverse childhood experiences in mothers with chronic pain and intergenerational impact on children. J. Pain 2019, 20, 1209–1217. [Google Scholar] [CrossRef]
- De Swart, F.D. Social Processes in Special Education Classrooms: The Role of Teachers and Peers in Pupils’ Adjustment. Ph.D. Thesis, Radboud University, Nijmegen, The Netherlands, 2021. [Google Scholar]
- Dong, M.; Anda, R.F.; Felitti, V.J.; Williamson, D.F.; Dube, S.R.; Brown, D.W.; Giles, W.H. Childhood residential mobility and multiple health risks during adolescence and adulthood: The hidden role of adverse childhood experiences. Arch. Pediatr. Adolesc. Med. 2005, 159, 1104–1110. [Google Scholar] [CrossRef]
- English, D.J.; Thompson, R.; Graham, J.C.; Briggs, E.C. Toward a definition of neglect in young children. Child Maltreat. 2005, 10, 190–206. [Google Scholar] [CrossRef]
- Ersing, R.L.; Sutphen, R.; Loeffler, D.N. Exploring the impact and implications of residential mobility: From the neighborhood to the school. Adv. Soc. Work 2009, 10, 1–18. [Google Scholar] [CrossRef]
- Finkelhor, D. Screening for adverse childhood experiences (ACEs): Cautions and suggestions. Child Abuse Negl. 2018, 85, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Higgins, K.S.; Birnie, K.A.; Chambers, C.T.; Wilson, A.C.; Caes, L.; Clark, A.J.; Lynch, M.; Stinson, J.; Campbell-Yeo, M. Offspring of parents with chronic pain: A systematic review and meta-analysis of pain, health, psychological, and family outcomes. Pain 2015, 156, 2256–2266. [Google Scholar] [CrossRef] [PubMed]
- Jelleyman, T.; Spencer, N. Residential mobility in childhood and health outcomes: A systematic review. J. Epidemiol. Community Health 2008, 62, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Jenny, C. Recognizing and responding to medical neglect. Pediatrics 2007, 120, 1385–1389. [Google Scholar] [CrossRef] [PubMed]
- Kerker, B.D.; Zhang, J.; Nadeem, E.; Stein, R.E.; Hurlburt, M.S.; Heneghan, A.; Landsverk, J.; Horwitz, S.M. Adverse childhood experiences and mental health, chronic medical conditions, and development in young children. Acad. Pediatr. 2015, 15, 510–517. [Google Scholar] [CrossRef]
- Mennen, F.E.; Kim, K.; Sang, J.; Trickett, P.K. Child neglect: Definition and identification of youth’s experiences in official reports of maltreatment. Child Abuse Negl. 2010, 34, 647–658. [Google Scholar] [CrossRef]
- The National Child Trauma Stress Network. Available online: https://www.nctsn.org/what-is-child-trauma/trauma-types/medical-trauma (accessed on 12 October 2021).
- Olweus, D. Victimization among schoolchildren: Intervention and prevention. In Improving Children’s Lives: Global Perspectives on Prevention; Albee, G.W., Bond, L.A., Monsey, T.V.C., Eds.; Sage Publications Inc.: Thousand Oaks, CA, USA, 1992; pp. 279–295. ISBN 080-394-610-4. [Google Scholar]
- Van de Putte, E.M.; Lukkassen, I.M.A.; Russel, I.M.; Teeuw, A.H. (Eds.) Medisch Handboek Kindermishandeling (Medical Handbook Child Abuse); Bohn Stafleu van Loghum: Houten, The Netherlands, 2013; ISBN 978-903-139-184-4. [Google Scholar]
- Van der Veen, H.C.J.; Bogaerts, S. Huiselijk Geweld in Nederland (Domestic Violence in the Netherlands); Boom Juridische Uitgevers: The Hague, The Netherlands, 2010; ISBN 978-908-974-404-3. [Google Scholar]
- Jedwab, M.; Harrington, D.; Dubowitz, H. Predictors of substantiated re-reports in a sample of children with initial unsubstantiated reports. Child Abuse Negl. 2017, 69, 232–241. [Google Scholar] [CrossRef]
- Vink, R.M.; van Dommelen, P.; van der Pal, S.M.; Eekhout, I.; Pannebakker, F.D.; Velderman, M.K.; Haagmans, M.; Mulder, T.; Dekker, M. Self-reported adverse childhood experiences and quality of life among children in the two last grades of Dutch elementary education. Child Abuse Negl. 2019, 95, 104051. [Google Scholar] [CrossRef]
- Van Berkel, S.R.; Prevoo, M.J.; Linting, M.; Pannebakker, F.D.; Alink, L.R. Prevalence of child maltreatment in the Netherlands: An update and cross-time comparison. Child Abuse Negl. 2020, 103, 104439. [Google Scholar] [CrossRef]
- Bethell, C.; Gombojav, N.; Solloway, M.; Wissow, L. Adverse childhood experiences, resilience and mindfulness-based approaches: Common denominator issues for children with emotional, mental, or behavioral problems. Child Adolesc. Psychiatr. Clin. N. Am. 2016, 25, 139–156. [Google Scholar] [CrossRef]
- Pronk, S.; Mulder, E.A.; van den Berg, G.; Stams, G.J.J.M.; Popma, A.; Kuiper, C. Differences between adolescents who do and do not successfully complete their program within a non-residential alternative education facility. Child. Youth Serv. Rev. 2020, 109, 104735. [Google Scholar] [CrossRef]
- Vervoort-Schel, J.; Mercera, G.; Wissink, I.; Mink, E.; van der Helm, P.; Lindauer, R.J.L.; Moonen, X. Adverse childhood experiences in children with intellectual disabilities: An exploratory case-file study in Dutch residential care. Int. J. Environ. Res. Public Health 2018, 15, 2136. [Google Scholar] [CrossRef] [PubMed]
- Baglivio, M.T.; Epps, N.; Swartz, K.; Huq, M.S.; Sheer, A.; Hardt, N.S. The prevalence of adverse childhood experiences (ACE) in the lives of juvenile offenders. J. Juv. Justice 2014, 3, 1–17. [Google Scholar]
- Centraal Bureau voor de Statistiek. Geboorte; Vruchtbaarheid, Migratieachtergrond en Generatie Moeder (Central Agency for Statistics: Birth; Fertility, Migration Background and Generation of the Mother. 2021. Available online: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/83307NED/table?ts=1601451664329 (accessed on 23 November 2021).
- Nederlands Jeugdinstituut: Eenoudergezinnen (Dutch Youth Institute: Single Parent Families). 2021. Available online: https://www.nji.nl/cijfers/eenoudergezinnen (accessed on 23 November 2021).
- Nederlands Jeugdinstituut: Cijfers over Armoede in Gezinnen (Dutch Youth Institute: Figures on Poverty in Families). 2021. Available online: https://www.nji.nl/cijfers/armoede-gezinnen (accessed on 23 November 2021).
- De Bellis, M.D.; Broussard, E.R.; Herring, D.J.; Wexler, S.; Moritz, G.; Benitez, J.G. Psychiatric co-morbidity in caregivers and children involved in maltreatment: A pilot research study with policy implications. Child Abuse Negl. 2001, 25, 923–944. [Google Scholar]
- Reupert, A.; Maybery, D. What do we know about families where parents have a mental illness? A systematic review. Child Youth Serv. 2016, 37, 98–111. [Google Scholar]
- Hambrick, E.P.; Tunno, A.M.; Gabrielli, J.; Jackson, Y.; Belz, C. Using multiple informants to assess child maltreatment: Concordance between case file and youth self-report. J. Aggress. Maltreat. Trauma 2014, 23, 751–771. [Google Scholar]
- Dorado, J.S.; Martinez, M.; McArthur, L.E.; Leibovitz, T. Healthy environments and response to trauma in schools (HEARTS): A whole-school, multi-level, prevention and intervention program for creating trauma-informed, safe and supportive schools. Sch. Ment. Health 2016, 8, 163–176. [Google Scholar]
- Pataky, M.G.; Báez, J.C.; Renshaw, K.J. Making schools trauma informed: Using the ACE study and implementation science to screen for trauma. Soc. Work Ment. Health 2019, 17, 639–661. [Google Scholar]
- Pugach, C.P.; Nomamiukor, F.O.; Gay, N.G.; Wisco, B.E. Temporal stability of self-reported trauma exposure on the life events checklist for DSM-5. J. Trauma. Stress 2021, 34, 248–256. [Google Scholar]
- Hawes, D.J.; Lechowicz, M.; Roach, A.; Fisher, C.; Doyle, F.L.; Noble, S.; Dadds, M.R. Capturing the developmental timing of adverse childhood experiences: The Adverse Life Experiences Scale. Am. Psychol. 2021, 76, 253–267. [Google Scholar]


| Characteristics | M (SD) (Range) | % |
|---|---|---|
| School type | ||
| Primary special education (age 4–12 years) | 65.5 | |
| Secondary special education (age 12–18 years) | 34.5 | |
| Sex | ||
| Male | 85.1 | |
| Female | 14.9 | |
| Age | ||
| Primary special education | 10.08 (1.47) | |
| Secondary special education | 14.43 (1.45) | |
| Primary and secondary special education | 11.58 (2.54) | |
| IQ score | 89.58 (17.85) (49–137) | |
| Family size a | 2.50 (1.23) | |
| Mother’s country of birth | ||
| Netherlands | 49.4 | |
| Western country | 9.2 | |
| Non-western country | 36.2 | |
| Missing | 5.2 | |
| Father’s country of birth | ||
| Netherlands | 33.9 | |
| Western country | 5.7 | |
| Non-western country | 39.1 | |
| Missing | 21.3 | |
| Household composition | ||
| Original household | 33.9 | |
| Blended household | 8.0 | |
| Single parent household | 43.7 | |
| Other | 13.2 | |
| Missing | 1.1 | |
| Educational level (of the primary income earner) | ||
| Low | 13.2 | |
| Moderate | 27.6 | |
| High | 14.9 | |
| Missing | 43.7 |
| Characteristics | Variables | % |
|---|---|---|
| School switches a | 0 | 0 |
| 1 | 32.2 | |
| 2 | 40.2 | |
| 3 | 19.0 | |
| ≥4 | 8.6 | |
| Type of school switch ᵇ | RE-RE | 23.0 |
| RE-SE | 84.5 | |
| SE-SE | 51.1 | |
| SE-RE | 6.3 | |
| Psychological (diagnostic) evaluation | Yes | 98.9 |
| Missing | 1.1 | |
| Diagnostic classification c | Yes | 84.5 |
| No | 15.5 | |
| Diagnostic classification according to DSM-IV or 5 | Autism spectrum disorders d | 35.1 |
| Attention-deficit/hyperactivity disorder | 35.1 | |
| Oppositional defiant disorder | 16.7 | |
| Disruptive behavior disorder NOS | 9.2 | |
| Specific learning disorder | 6.9 | |
| Post-traumatic stress disorder | 6.3 | |
| Reactive attachment disorder | 5.7 | |
| Borderline intellectual functioning | 5.7 | |
| Other | 16.5 | |
| Comorbidity | No diagnosis | 15.5 |
| 1 diagnosis | 43.1 | |
| 2 or more diagnoses | 41.4 | |
| Medication use related to DSM diagnosis | Yes | 53.5 |
| No | 42.0 | |
| Missing | 4.6 | |
| Child therapy | Yes | 87.4 |
| No | 11.5 | |
| Missing | 1.1 | |
| Family-oriented social work and therapy | Yes | 85.6 |
| No | 13.2 | |
| Missing | 1.1 |
| ACEs | Students’ Self-Reports (%) n = 169 | Parent Reports (%) n = 95 | School Files (%) n = 172 |
|---|---|---|---|
| 0 | 3.6 | 10.5 | 4.7 |
| 1 | 3.6 | 11.6 | 12.2 |
| 2 | 9.5 | 10.5 | 13.4 |
| 3 | 8.9 | 14.7 | 9.9 |
| 4–7 | 34.3 | 40.0 | 39.6 |
| ≥8 | 40.2 | 12.7 | 20.3 |
| ≥1 | 96.4 | 89.5 | 95.3 |
| ≥4 | 74.4 | 52.7 | 59.9 |
| M (SD) | 6.89 (4.40) | 3.91 (2.84) | 4.70 (3.27) |
| Min/Max | 0–25 | 0–14 | 0–14 |
| Maximum number of ACEs | 28 | 25 | 25 |
| Included ACEs | Self-Reports (%) | Parent Reports (%) |
| Maltreatment | 84.0 | 74.7 |
| Neglect | 18.3 | 5.3 |
| Supervisory neglect | 14.2 | 3.2 |
| Physical neglect | 5.9 | 4.2 |
| Abuse | 81.1 | 74.7 |
| Physical abuse | 71.0 | 57.9 |
| Emotional abuse | 44.4 | 57.9 |
| Physical assault with a weapon | 27.2 | 8.4 |
| Sexual abuse | 10.7 | 2.1 |
| Forced to be somewhere | 8.3 | 0 |
| Witnessed people having sex or porn | 7.7 | 7.4 |
| Domestic violence | 24.3 | 29.5 |
| Household challenges and/or peer victimization | 85.2 | 76.8 |
| Bullying | 60.4 | 63.2 |
| Death of someone close | 58.6 | 37.9 |
| Forced into doing something (non-sexual) | 18.3 | 9.5 |
| Police arrest of a family member | 17.2 | 13.7 |
| Parental mental health problems | 12.4 | |
| Parental substance abuse | 10.1 | |
| Suicide or attempted suicide of a household member | 7.7 | |
| Community stressors | 33.1 | 8.4 |
| Stalked a | 21.3 | 4.2 |
| Experienced war or neighborhood violence | 15.4 | 4.2 |
| Experienced shooting ᵇ | 11.2 | 1.1 |
| Accident | 75.7 | 46.3 |
| Other serious accident | 55.0 | 19.0 |
| Traffic accident | 47.9 | 24.2 |
| Fire/explosion | 27.2 | 10.5 |
| Natural disaster | 8.3 | 4.2 |
| Exposure to hazardous substances | 5.9 | 0 |
| Other | 62.7 | 30.5 |
| Hurting someone severely | 47.9 | 13.7 |
| Other severe or frightening events | 23.7 | 10.5 |
| Witnessed other people injured or dead | 17.2 | 7.4 |
| Serious illness or near to dear through severe injury | 11.8 | 8.4 |
| Included ACEs | Percentage (%) |
|---|---|
| Maltreatment | 69.0 |
| Neglect (total) | 53.4 |
| Physical/supervisory neglect | 33.9 |
| Psychological neglect | 20.7 |
| Medical neglect | 13.3 |
| Educational neglect | 8.0 |
| Unspecified | 2.3 |
| Abuse (total) | 41.4 |
| Physical abuse | 34.5 |
| Emotional abuse | 19.6 |
| Sexual abuse | 5.1 |
| Unspecified | 1.7 |
| Domestic violence | 29.3 |
| Household challenges | 82.0 |
| Parental separation or divorce | 47.7 |
| Parental mental health problems | 33.3 |
| Separation from parents | 25.9 |
| Economic hardship | 20.1 |
| Many (sudden) relocations | 17.8 |
| Serious accident or physical illness of a parent | 17.2 |
| Substance abuse | 9.7 |
| Parental absence | 9.2 |
| Parental death | 4.6 |
| Parental incarceration | 4.0 |
| Peer victimization | 40.2 |
| Bullying | 32.1 |
| Negative school experiences | 12.1 |
| Community stressors | 3.5 |
| Victim of neighborhood violence | 3.5 |
| Other | 40.1 |
| Other severe or frightening events a | 29.7 |
| Medical trauma | 18.4 |
| Demographic Risk Factors | n | M | M Rank | Test | U/H | z | p |
|---|---|---|---|---|---|---|---|
| Household composition a | 133 | MWU | 1685 | −2.21 | 0.027 | ||
| Original household | 57 | 3.12 | 58.55 | ||||
| Single parent household | 76 | 4.74 | 73.34 | ||||
| Mother’s country of birth | 163 | MWU | 3269 | −0.17 | 0.869 | ||
| Born in NL | 84 | 4.61 | 82.59 | ||||
| Not born in NL | 79 | 4.32 | 81.37 | ||||
| Father’s country of birth | 135 | MWU | 1802 | −1.93 | 0.054 | ||
| Born in NL | 77 | 3.86 | 60.56 | ||||
| Not born in NL | 58 | 4.53 | 73.60 | ||||
| Parents’ country of birth | 132 | MWY | 1788 | −1.24 | 0.215 | ||
| Born in NL | 50 | 3.94 | 61.25 | ||||
| ≥1 not born in NL | 82 | 4.40 | 69.70 | ||||
| Educational level ᵇ | 96 | KWH | 5.619 | 0.060 | |||
| Low | 23 | 4.65 | 49.39 | ||||
| Moderate | 48 | 5.35 | 53.75 | ||||
| High | 25 | 3.68 | 37.60 | ||||
| Family size | 171 | MWU | 3164 | −1.26 | 0.208 | ||
| 0–2 children in household | 99 | 4.82 | 90.04 | ||||
| ≥3 children in household | 72 | 3.99 | 80.55 | ||||
| Economic hardship c | 172 | MWU | 1073 | −5.07 | <0.001 | ||
| Not present | 137 | 3.91 | 76.83 | ||||
| Present | 35 | 6.80 | 124.34 | ||||
| Accumulated risk factors d | 160 | MWU | 2539 | −2.27 | 0.023 | ||
| 0–1 | 81 | 4.00 | 72.34 | ||||
| ≥2 | 79 | 4.81 | 88.87 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Offerman, E.C.P.; Asselman, M.W.; Bolling, F.; Helmond, P.; Stams, G.-J.J.M.; Lindauer, R.J.L. Prevalence of Adverse Childhood Experiences in Students with Emotional and Behavioral Disorders in Special Education Schools from a Multi-Informant Perspective. Int. J. Environ. Res. Public Health 2022, 19, 3411. https://doi.org/10.3390/ijerph19063411
Offerman ECP, Asselman MW, Bolling F, Helmond P, Stams G-JJM, Lindauer RJL. Prevalence of Adverse Childhood Experiences in Students with Emotional and Behavioral Disorders in Special Education Schools from a Multi-Informant Perspective. International Journal of Environmental Research and Public Health. 2022; 19(6):3411. https://doi.org/10.3390/ijerph19063411
Chicago/Turabian StyleOfferman, Evelyne C. P., Michiel W. Asselman, Floor Bolling, Petra Helmond, Geert-Jan J. M. Stams, and Ramón J. L. Lindauer. 2022. "Prevalence of Adverse Childhood Experiences in Students with Emotional and Behavioral Disorders in Special Education Schools from a Multi-Informant Perspective" International Journal of Environmental Research and Public Health 19, no. 6: 3411. https://doi.org/10.3390/ijerph19063411
APA StyleOfferman, E. C. P., Asselman, M. W., Bolling, F., Helmond, P., Stams, G.-J. J. M., & Lindauer, R. J. L. (2022). Prevalence of Adverse Childhood Experiences in Students with Emotional and Behavioral Disorders in Special Education Schools from a Multi-Informant Perspective. International Journal of Environmental Research and Public Health, 19(6), 3411. https://doi.org/10.3390/ijerph19063411