
The Effectiveness of the Integrated Care Model among Community-Dwelling Older Adults with Depression: A Quasi-Randomized Controlled Trial


Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Eligibility Criteria
- Above 55 years of age;
- Has a medical diagnosis of depressive disorder or depressive mood;
- Brief Symptom Rating Scale (BSRS-5) > 5;
- Mini-Mental State Examination (MMSE) > 20;
- Clear consciousness and attention sustainability of, at least, 20 min; depressed mood or symptoms do not interfere with interviews and data collection;
- Volunteering to participate in this study.
- Visual, hearing, and communication impairments;
- Alcohol or drug dependence.
2.2. Study Design and Procedure
2.3. Measures
2.3.1. The Center for Epidemiologic Studies Depression Scale (CES-D)
2.3.2. Brief Symptom Rating Scale (BSRS-5)
2.3.3. Life Satisfaction Index (LSI)
2.4. Interventions
2.5. Analysis
3. Results
3.1. Characteristics of Participants
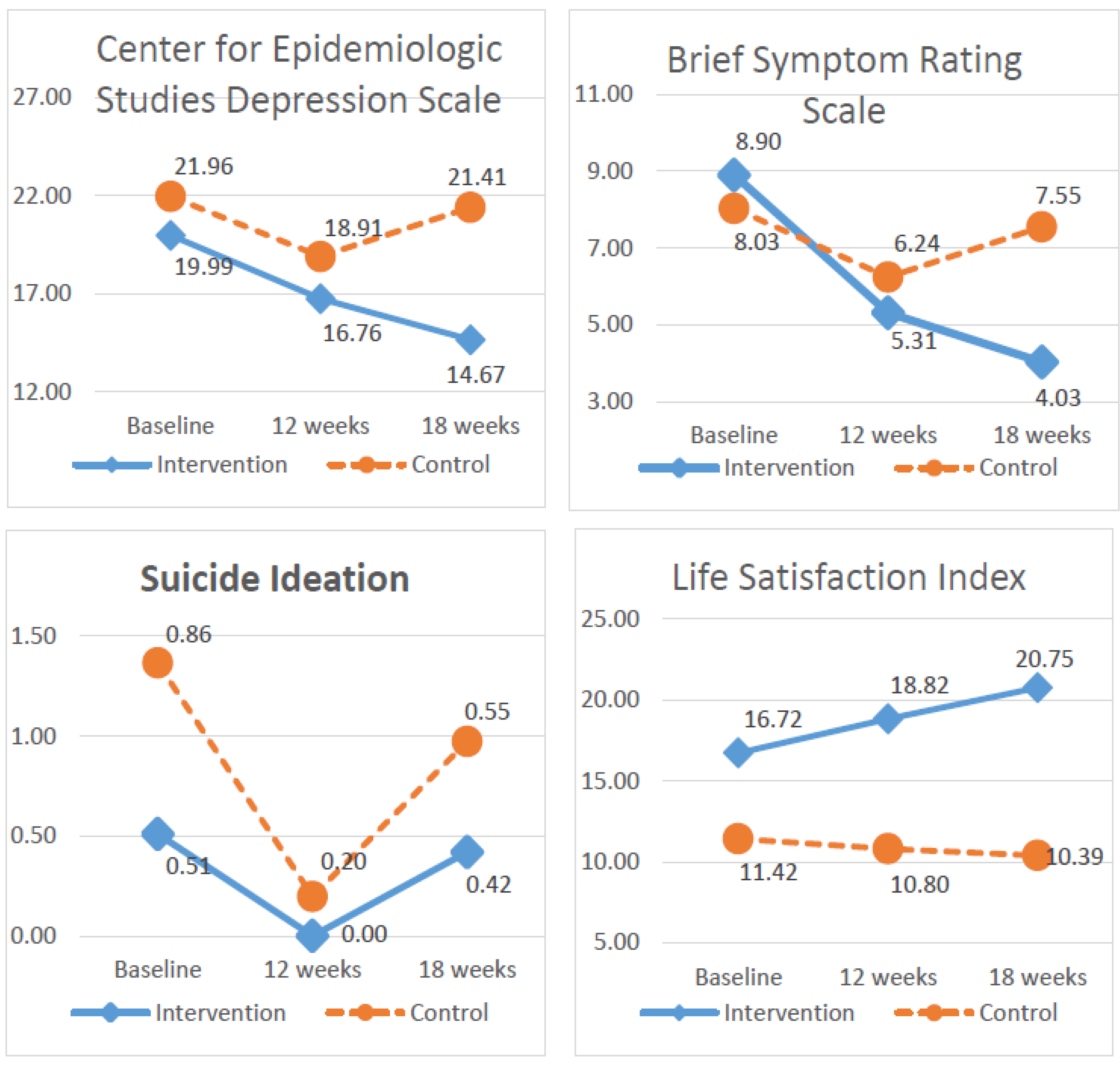
3.2. Results on Outcome Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Depression. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 13 December 2021).
- Health Promotion Administration, Ministry of Health and Welfare. 2015 Taiwan Longitudinal Study on Aging Survey Report; Taiwan Aging Study Series, No.13; Ministry of Health and Welfare: Taipei, Taiwan, 2018.
- Tollanes, M.C.; Knudsen, A.K.; Vollset, S.E.; Kinge, J.M.; Skirbekk, V.; Øverland, S. Disease burden in Norway in 2016. Tidsskr. Nor. Legeforening 2018, 138, 15. [Google Scholar]
- Borza, T.; Engedal, K.; Bergh, S.; Selbaek, G. Older people with depression-a three-year follow-up. Tidsskr. Nor. Legeforening 2019, 139, 16. [Google Scholar]
- Dao, A.T.M.; Nguyen, V.T.; Nguyen, H.V.; Nguyen, L.T.K. Factors Associated with Depression among the Elderly Living in Urban Vietnam. Biomed. Res. Int. 2018, 2018, 1–9. [Google Scholar]
- Cheng, W.S.; Hwang, T.J.; Lee, M.B.; Liao, S.C. Assessment and Management of Geriatric Depression and Suicide. Taiwan Geriatr. Gerontol. 2016, 11, 16–30. [Google Scholar]
- Lin, C.H.; Chen, P.H.; Lin, H.S. A Panel Study on Factors Affecting the Changing Status of Depression among the Elderly in Taiwan. J. Popul. Stud. 2010, 41, 67–109. [Google Scholar]
- Espinoza, R.T.; Unutzer, J. Diagnosis and Management of Late-Life Unipolar Depression; UpTo-Date: Waltham, MA, USA, 2021. [Google Scholar]
- Liao, S.J.; Wu, B.J.; Liu, T.T.; Chou, C.P.; Rong, J.R. Prevalence and characteristics of suicidal ideation among 2199 elderly inpatients with surgical or medical conditions in Taiwan. BMC Psychiatry 2018, 18, 397. [Google Scholar] [CrossRef]
- Connors, M.H.; Sachdev, P.S.; Kochan, N.A.; Xu, J.; Draper, B.; Brodaty, H. Cognition and mortality in older people: The Sydney Memory and Ageing Study. Age Ageing 2015, 44, 1049–1054. [Google Scholar] [CrossRef]
- Oh, I.M.; Cho, M.J.; Hahm, B.J.; Kim, B.S.; Sohn, J.H.; Suk, H.W.; Jung, B.Y.; Kim, H.J.; Kim, H.A.; Choi, K.B.; et al. Effectiveness of a village-based intervention for depression in community-dwelling older adults: A randomized feasibility study. BMC Geriatr. 2020, 20, 89. [Google Scholar] [CrossRef]
- Ho, H.T.; Liu, L.F.; Guo, N.W. Factors of Geriatric Depression in Southern Taiwan. Taiwan J. Fam. Med. 2016, 26, 100–108. [Google Scholar]
- Rong, J.R.; Shiau, S.J.; Su, S.F. The Development of Psychiatric and Mental Health Nursing in Taiwan. J. Nurs. Res. 2014, 61, 5–10. [Google Scholar]
- Hsiang, C.Y.; Lee, J.Z.; Lin, P.C. The Related Factors Affecting Physical and Mental Health of Older People. New Taipei J. Nurs. 2012, 14, 7–16. [Google Scholar]
- Fernandez-Nino, J.A.; Manrique-Espinoza, B.S.; Bojorquez-Chapela, I.; Salinas-Rodriguez, A. Income inequality, socioeconomic deprivation and depressive symptoms among older adults in Mexico. PLoS ONE 2014, 9, 1–9. [Google Scholar] [CrossRef]
- Hegerl, U.; Rummel-Kluge, C.; Várnik, A.; Arensman, E.; Koburger, N. Alliances against depression-A community based approach to target depression and to prevent suicidal behaviour. Neurosci. Biobehav. Rev. 2013, 37, 2404–2409. [Google Scholar] [CrossRef]
- Wilkinson, P.; Ruane, C.; Tempest, K. Depression in older adults. BMJ 2018, 363, k492. [Google Scholar] [CrossRef]
- Li, N.; Pang, L.; Chen, G.; Song, X.; Zhang, J.; Zheng, X. Risk factors for depression in older adults in Beijing. Can. J. Psychiatry 2011, 56, 466–473. [Google Scholar] [CrossRef]
- Park, J.E.; Lee, J.Y.; Jeon, H.J.; Han, K.H.; Sohn, J.H.; Sung, S.J.; Cho, M.J. Age-related differences in the influence of major mental disorders on suicidality: A Korean nationwide community sample. J. Affect. Disord. 2014, 162, 96–101. [Google Scholar] [CrossRef]
- Cole, T.; Winkler, M. The Oxford Book of Aging: Reflections on the Journey of Life; New Century Publishing Co.: Taipei, Taiwan, 1994. [Google Scholar]
- Cicirelli, V.G. Attachment relationships in old age. J. Soc. Pers. Relatsh. 2010, 27, 191–199. [Google Scholar] [CrossRef]
- Shrestha, M.K.; Adhikari, R.D.; Ranjitkar, U.D.; Chand, A. Life Satisfaction among Senior Citizens in a Community of Kathmandu, Nepal. J. Gerontol. Geriatr. Res. 2019, 8, 500. [Google Scholar]
- Hsu, H.C. Trajectories and covariates of life satisfaction among older adults in Taiwan. Arch. Gerontol. Geriatr. 2012, 55, 210–216. [Google Scholar] [CrossRef]
- Lino, V.T.; Portela, M.C.; Camacho, L.A.; Atie, S.; Lima, M.J. Assessment of social support and its association to depression, self-perceived health and chronic diseases in elderly individuals residing in an area of poverty and social vulnerability in rio de janeiro city, Brazil. PLoS ONE 2013, 8, e71712. [Google Scholar] [CrossRef]
- Hsu, T.F.; Huang, H.Y.; Chen, T.C. The elderly in the community; self-perceived general health; self-perceived psychological health; life satisfaction; meaning of life. J. Healthc. Manag. 2015, 16, 246–267. [Google Scholar]
- Dziedzic, B.; Sienkiewicz, Z.; Lenczuk-Gruba, A.; Kobos, E.; Fidecki, W.; Wysokiski, M. Prevalence of Depressive Symptoms in the Elderly Population Diagnosed with Type 2 Diabetes Mellitus. Int. J. Environ. Res. Public Health 2020, 17, 3553. [Google Scholar] [CrossRef] [PubMed]
- Zhao, D.; Hu, C.; Chen, J.; Dong, B.; Ren, Q.; Yu, D.; Zhao, Y.; Li, J.; Huang, Y.; Sun, Y. Risk factors of geriatric depression in rural China based on a generalized estimating equation. Int. Psychogeriatr. 2018, 30, 1489–1497. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.Y.; Lan, Y.H. The relationships of depression, morale and mastery in the community of elders. Community Dev. J. Q. 2013, 141, 387–400. [Google Scholar]
- Schuch, F.B.; Stubbs, B. The Role of Exercise in Preventing and Treating Depression. Exerc. Med. 2019, 18, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.F.; Wu, J.J.; Huang, Y.H.; Ju, L.Y.; Lin, S.Y.; Chou, Y.C.; Lin, C.S. Impact of day care services on physical and cognitive functions in old people with dementia in a medical center in central Taiwan. Health Qual. Life Outcomes 2021, 19, 170. [Google Scholar] [CrossRef]
- Moral, J.C.M.; Terrero, F.B.F.; Galan, A.S.; Rodriguez, T.M. Effect of integrative reminiscence therapy on depression, well-being, integrity, self-esteem, and life satisfaction in older adults. J. Posit. Psychol. 2015, 10, 240–247. [Google Scholar] [CrossRef]
- Li, C.; Jiang, S.; Li, N.; Zhang, Q. Influence of social participation on life satisfaction and depression among Chinese elderly: Social support as a mediator. J. Community Psychol. 2018, 46, 345–355. [Google Scholar] [CrossRef]
- Weng, C.F.; Lin, K.P.; Lu, F.P.; Chen, J.H.; Wen, C.J.; Peng, J.H.; Tseng, A.H.; Chan, D.C. Effects of depression, dementia and delirium on activities of daily living in elderly patients after discharge. BMC Geriatr. 2019, 19, 261. [Google Scholar] [CrossRef] [PubMed]
- Hsu, H.C.; Chen, C.F. LTC 2.0: The 2017 reform of home- and community-based long-term care in Taiwan. Health Policy 2019, 123, 912–916. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Eaton, W.W.; Smith, C.; Ybarra, M.; Muntaner, C.; Tien, A. Center for Epidemiologic Studies Depression Scale: Review and Revision (CESD and CESD-R). In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment: Instruments for Adults; Maruish, M.E., Ed.; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 2004; pp. 363–377. [Google Scholar]
- Chien, C.P.; Cheng, T.A. Depression in Taiwan: Epidemiological survey utilizing CES-D. Bull. Jpn. Soc. Neurol. Psychiatry 1985, 87, 335–338. [Google Scholar]
- Lung, F.W.; Lee, M.B. The five-item Brief-Symptom Rating Scale as a suicide ideation screening instrument for psychiatric inpatients and community residents. BMC Psychiatry 2008, 8, 53. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.B.; Liao, S.C.; Lee, Y.J.; Wu, C.H.; Tseng, M.C.; Gau, S.F.; Rau, C.L. Development and Verification of Validity and Reliability of a Short Screening Instrument to Identify Psychiatric Morbidity. J. Formos. Med. Assoc. 2003, 102, 687–694. [Google Scholar] [PubMed]
- Neugarten, B.L.; Havighurst, R.J.; Tobin, S.S. The measurement of life satisfaction. J. Gerontol. 1961, 16, 134–143. [Google Scholar] [CrossRef]
- Liang, K.Y.; Zeger, S.L. Longitudinal data analysis using generalized linear models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Cui, J.; Qin, Y.; Tian, Y.; Ge, X.; Han, H.; Yang, Z.; Yu, H. Activities of daily living as a longitudinal moderator of the effect of autonomic dysfunction on anxiety and depression of Parkinson’s patients. Brain Behav. 2012, 11, e2297. [Google Scholar] [CrossRef]
- Chen, C.Y. Progress of Geriatric Frailty and Disability Prevention Strategies in 2020 National Healthy People. Formos. J. Med. 2018, 22, 253–260. [Google Scholar]
- WHO. Elder Abuse. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/elder-abuse (accessed on 1 February 2022).
- Liao, S.J.; Rong, J.R.; Liu, T.T.; Sun, H.J. The Life Experiences of Community Older Adults with Mental Illness in Taiwan: A Qualitative Study. Int. J. Stud. Nurs. 2018, 3, 158–167. [Google Scholar] [CrossRef][Green Version]
- Spiers, J.A.; Wood, A. Building a therapeutic alliance in brief therapy: The experience of community mental health nurses. Arch. Psychiatr. Nurs. 2010, 24, 373–386. [Google Scholar] [CrossRef]
- National Institute for Health & Clinical Excellence. The NICE Guideline on the Treatment and Management of in Depression Adults; Updated Edition; The British Psychological Society and The Royal College of Psychiatrists: London, UK, 2011. [Google Scholar]
- Carlson, W.L.; Ong, T.D. Suicide in Later Life. Failed Treatment or Rational Choice? Clin. Geriatr. Med. 2014, 30, 553–576. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Domains | Interventions |
|---|---|
| Assessing and managing health problems | To assess physical condition |
| To manage physical health problems, such as chronic diseases | |
| To assess mental condition | |
| To manage mental health problems, such as dementia and delirium | |
| To assess dangerous behaviors, such as violence, self-injury, and psychiatric symptoms | |
| To provide problem-solving skills for dangerous behaviors, such as violence and self-injury. If necessary, consult psychologists or visit doctors | |
| To provide information about medication | |
| To encourage adherence to medication routines | |
| To collaborate with medical teams for patients’ care | |
| Achieving spiritual and mental wellbeing | To offer emotional support |
| To offer skills for stress management | |
| To encourage exercise | |
| To provide reminiscence therapy in group exercise | |
| Enhancing activities of daily life and mobility | To assess functional activities of daily life |
| To improve functional living skills, such as daily activity training | |
| To provide tangible support, such as assistive devices | |
| To arrange group exercise or individualized activities for facilitating physical activities | |
| To assist in living life independently, such as meal provision by neighborhood representatives or volunteers for those who cannot prepare meals | |
| To provide a safe environment to avoid falls and injuries | |
| Providing social welfare resources | To inform social welfare systems |
| To arrange and provide a rehabilitation bus for medical appointments | |
| To provide services at day care centers | |
| To provide respite care and short break services to decrease family burden | |
| To seek charity for financial difficulties | |
| Providing prevention for elder abuse | To identity characteristics of elder abuse |
| To relieve the burden on the caregiver, such as referral respite care or day care centers | |
| To provide helplines and emergency shelters, if necessary |
| Variable | Intervention Group (n = 67) n (%) | Control Group (n = 76) n (%) | Total (Percentage) | χ2/t * | p |
|---|---|---|---|---|---|
| Gender | 6.18 | 0.013 | |||
| Male | 37 (55.2%) | 57 (75.0%) | 94 (65.7%) | ||
| Female | 30 (44.8%) | 19 (25.0%) | 49 (34.3%) | ||
| Age | 11.95 | 0.102 | |||
| 50–54 y/o | 1 (1.5%) | 0 (0.0%) | 1 (0.7%) | ||
| 55–59 y/o | 17 (25.4%) | 11 (14.5%) | 28 (19.6%) | ||
| 60–64 y/o | 24 (35.8%) | 20 (26.3%) | 44 (30.8%) | ||
| 65–69 y/o | 15 (22.4%) | 21 (27.6%) | 36 (25.2%) | ||
| 70–74 y/o | 7 (10.4%) | 12 (15.8%) | 19 (13.3%) | ||
| 75–79 y/o | 3 (4.5%) | 5 (6.6%) | 8 (5.6%) | ||
| 80–84 y/o | 0 (0.0%) | 6 (7.9%) | 6 (4.2%) | ||
| 85–89 y/o | 0 (0.0%) | 1 (1.3%) | 1 (0.7%) | ||
| Education | 7.30 | 0.121 | |||
| Illiterate | 0 (0.0%) | 4 (5.3%) | 4 (2.8%) | ||
| Elementary school | 45 (67.2%) | 56 (73.7%) | 101 (70.6%) | ||
| Junior high school | 9 (13.4%) | 10 (13.2%) | 19 (13.3%) | ||
| Senior high school and above | 11 (16.4%) | 5 (6.6%) | 16 (11.2%) | ||
| Above college | 2 (3.0%) | 1 (1.3%) | 3 (2.1%) | ||
| Marital status | 7.92 | 0.095 | |||
| Never married | 47 (70.1%) | 53 (69.7%) | 100 (69.9%) | ||
| Widow/widower | 6 (9.0%) | 5 (6.6%) | 11 (7.7%) | ||
| Live-in together | 2 (3.0%) | 0 (0.0%) | 2 (1.4%) | ||
| Married | 3 (4.5%) | 0 (0.0%) | 3 (2.1%) | ||
| Separated/divorced | 9 (13.4%) | 18 (23.7%) | 27 (18.9%) | ||
| Economic status | 9.15 | 0.010 | |||
| Poor | 26 (38.8%) | 45 (59.2%) | 71 (49.7%) | ||
| Fair | 37 (55.2%) | 23 (30.3%) | 60 (42.0%) | ||
| Sufficient | 4 (6.0%) | 8 (10.5%) | 12 (8.4%) | ||
| Health status | −1.54 * | 0.127 | |||
| Very bad | 2 (3.0%) | 6 (7.9%) | 8 (5.6%) | ||
| Bad | 15 (22.4%) | 21 (27.6%) | 36 (25.2%) | ||
| Good | 37 (55.2%) | 38 (50.0%) | 75 (52.4%) | ||
| Very good | 13 (19.4%) | 11 (14.5%) | 24 (16.8%) | ||
| Face scale mood | 0.96 * | 0.337 | |||
| Crying | 7 (10.4%) | 0 (0.0%) | 7 (4.9%) | ||
| Very sad | 3 (4.5%) | 2 (2.6%) | 5 (3.5%) | ||
| Somewhat sad | 11 (16.4%) | 25 (32.9%) | 36 (25.2%) | ||
| Neutral | 28 (41.8%) | 33 (43.4%) | 61 (42.7%) | ||
| Somewhat happy | 14 (20.9%) | 8 (10.5%) | 22 (15.4%) | ||
| Very happy | 3 (4.5%) | 5 (6.6%) | 8 (5.6%) | ||
| Extremely happy | 1 (1.5%) | 3 (3.9%) | 4 (2.8%) | ||
| Mean (SD) | Mean (SD) | Mean (SD) | |||
| Health status | 1.91 (0.73) | 1.71 (0.81) | 1.80 (0.78) | −1.54 * | 0.127 |
| Chronic illness number | 1.81 (1.61) | 1.43 (1.24) | 1.61 (1.43) | −1.56 * | 0.121 |
| CES-D | 19.99 (7.89) | 21.96 (8.74) | 21.03 (8.38) | 1.41 * | 0.160 |
| BSRS-5 | 8.90 (3.05) | 8.03 (2.14) | 8.43 (2.63) | −1.95 * | 0.054 |
| SI | 0.51 (0.89) | 0.86 (0.89) | 0.69 (0.91) | 2.33 * | 0.021 |
| LSI | 16.72 (7.81) | 11.42 (7.49) | 13.9 (8.06) | −4.13 * | <0.001 |
| Parameters | Center for Epidemiologic Studies Depression Scale | Brief Symptom Rating Scale | ||||
|---|---|---|---|---|---|---|
| β | 95% CI | p | β | 95% CI | p | |
| Intercept | 21.33 | 16.51~26.15 | <0.001 | 7.90 | 6.55~9.25 | <0.001 |
| Gender | 1.38 | −1.04~3.80 | 0.265 | −0.04 | −0.99~0.92 | 0.941 |
| Economic status | 0.25 | −1.73~2.23 | 0.804 | −0.05 | −0.74~0.64 | 0.890 |
| Suicide ideation | 1.40 | 0.07~2.74 | 0.039 | 0.82 | 0.15~1.50 | 0.016 |
| Life Satisfaction Index | −0.11 | −0.26~0.03 | 0.131 | −0.04 | −0.09~0.01 | 0.082 |
| Group a | −1.12 | −3.67~1.43 | 0.389 | 1.38 | 0.56~2.21 | 0.957 |
| Time | ||||||
| 12 weeks b | −3.05 | −4.68~−1.42 | <0.001 | −1.79 | −2.57~−1.01 | <0.001 |
| 18 weeks b | −0.55 | −2.38~1.27 | 0.553 | −0.47 | −1.26~0.31 | 0.236 |
| Group * Time | ||||||
| Intervention * 12 weeks c | −0.17 | −2.40~2.06 | 0.880 | −1.79 | −3.01~−0.57 | 0.004 |
| Intervention * 18 weeks c | −4.76 | −7.39~−2.14 | <0.001 | −4.39 | −5.60~−3.18 | <0.001 |
| Parameters | Suicide Ideation | Life Satisfaction Index | ||||
| β | 95% CI | p | β | 95% CI | p | |
| Intercept | 1.36 | 0.91~1.81 | <0.001 | 17.30 | 13.60~20.99 | <0.001 |
| Gender | −0.13 | −0.36~0.10 | 0.265 | −0.46 | −2.21~1.29 | 0.605 |
| Economic status | −0.09 | −0. 28~0.09 | 0.334 | −2.75 | −4.50~−1.01 | 0.002 |
| Suicide ideation | - | - | - | −1.95 | −2.88~−1.02 | <0.001 |
| Life Satisfaction Index | −0.03 | −0.04~0.02 | <0.001 | - | - | - |
| Group a | −0.18 | −0.49~0.13 | 0.248 | 4.27 | 1.87~6.67 | <0.001 |
| Time | ||||||
| 12 weeks b | −0.66 | −0.86~−0.45 | <0.001 | −0.62 | −2.52~1.28 | 0.523 |
| 18 weeks b | −0.30 | −0.54~−0.07 | 0.012 | −1.03 | −3.09~1.04 | 0.331 |
| Group * Time | ||||||
| Intervention * 12 weeks c | 0.75 | 0.45~1.05 | <0.001 | 2.72 | 0.48~4.97 | 0.018 |
| Intervention * 18 weeks c | 0.21 | −0.10~0.53 | 0.186 | 5.06 | 2.57~7.54 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liao, S.-J.; Chao, S.-M.; Fang, Y.-W.; Rong, J.-R.; Hsieh, C.-J. The Effectiveness of the Integrated Care Model among Community-Dwelling Older Adults with Depression: A Quasi-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 3306. https://doi.org/10.3390/ijerph19063306
Liao S-J, Chao S-M, Fang Y-W, Rong J-R, Hsieh C-J. The Effectiveness of the Integrated Care Model among Community-Dwelling Older Adults with Depression: A Quasi-Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(6):3306. https://doi.org/10.3390/ijerph19063306
Chicago/Turabian StyleLiao, Su-Jung, Shu-Mei Chao, Yu-Wen Fang, Jiin-Ru Rong, and Chia-Jou Hsieh. 2022. "The Effectiveness of the Integrated Care Model among Community-Dwelling Older Adults with Depression: A Quasi-Randomized Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 6: 3306. https://doi.org/10.3390/ijerph19063306
APA StyleLiao, S.-J., Chao, S.-M., Fang, Y.-W., Rong, J.-R., & Hsieh, C.-J. (2022). The Effectiveness of the Integrated Care Model among Community-Dwelling Older Adults with Depression: A Quasi-Randomized Controlled Trial. International Journal of Environmental Research and Public Health, 19(6), 3306. https://doi.org/10.3390/ijerph19063306