
The Mental Health of Employees with Job Loss and Income Loss during the COVID-19 Pandemic: The Mediating Role of Perceived Financial Stress

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
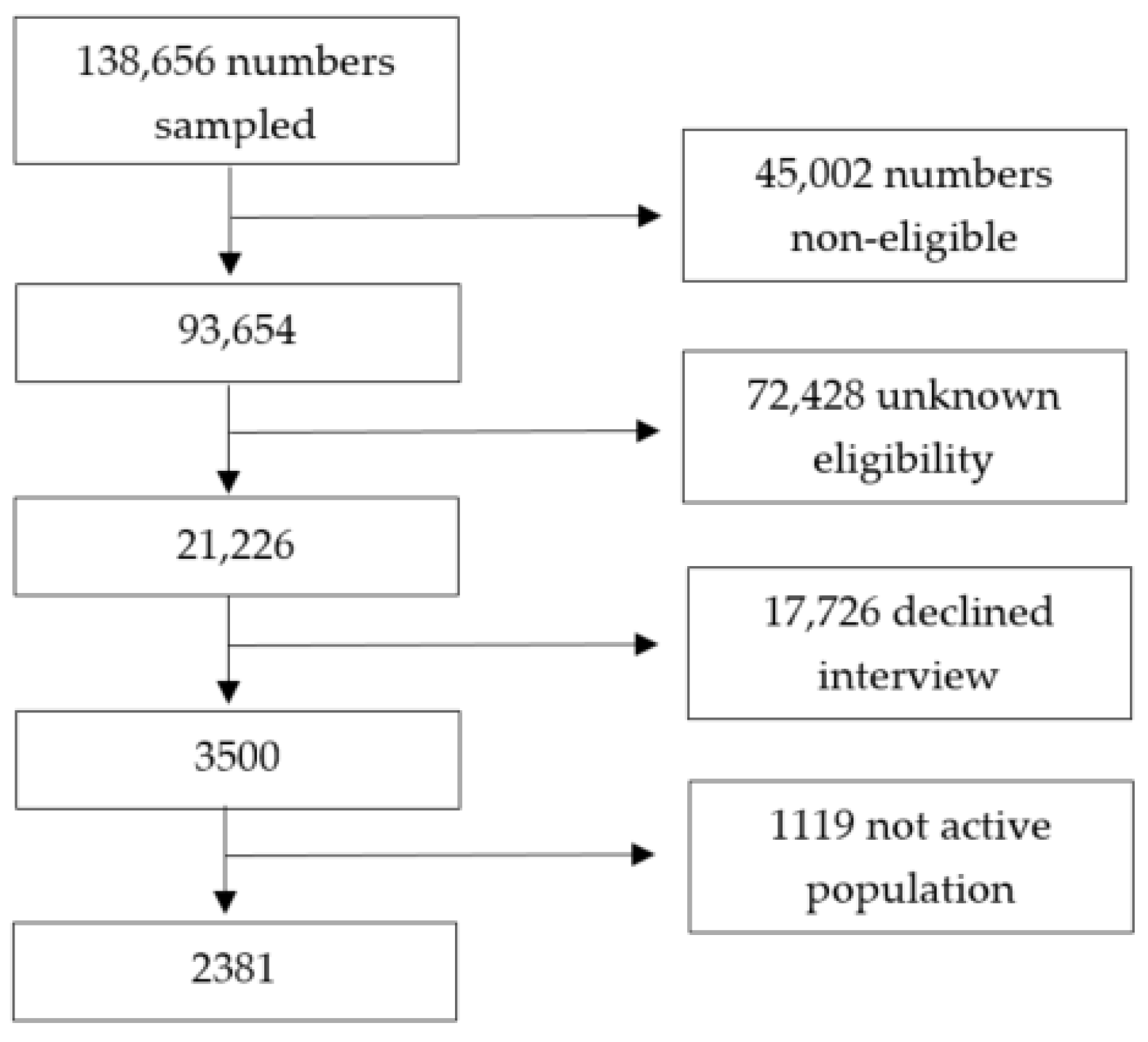
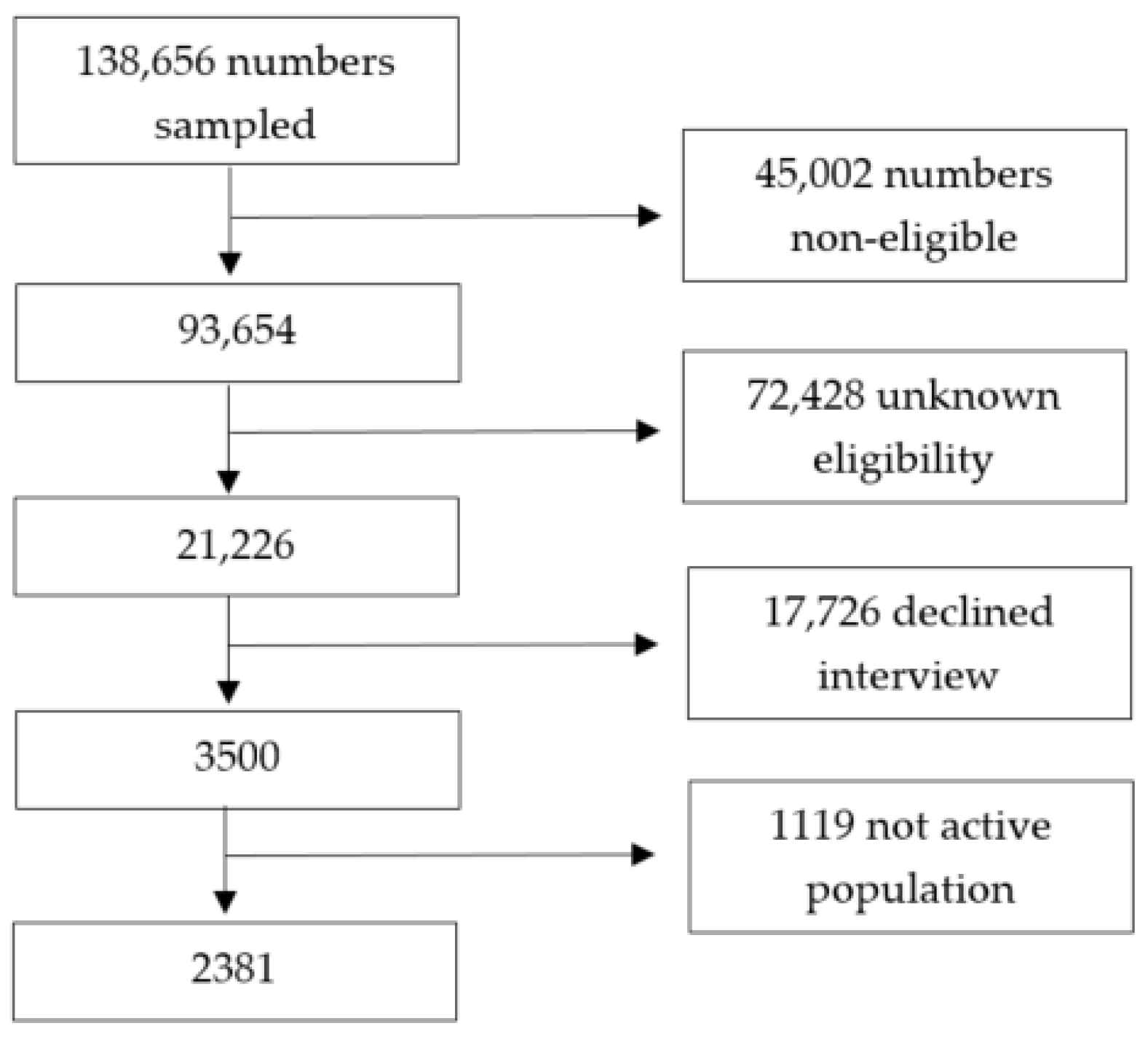
2.1. Sample and Study Design
2.2. Sociodemographic Measures
2.3. Mental Health Measures
2.4. Work-Related Measures
2.5. Statistical Analyses
3. Results
3.1. Sample Sociodemographics
3.2. Regression Analyses
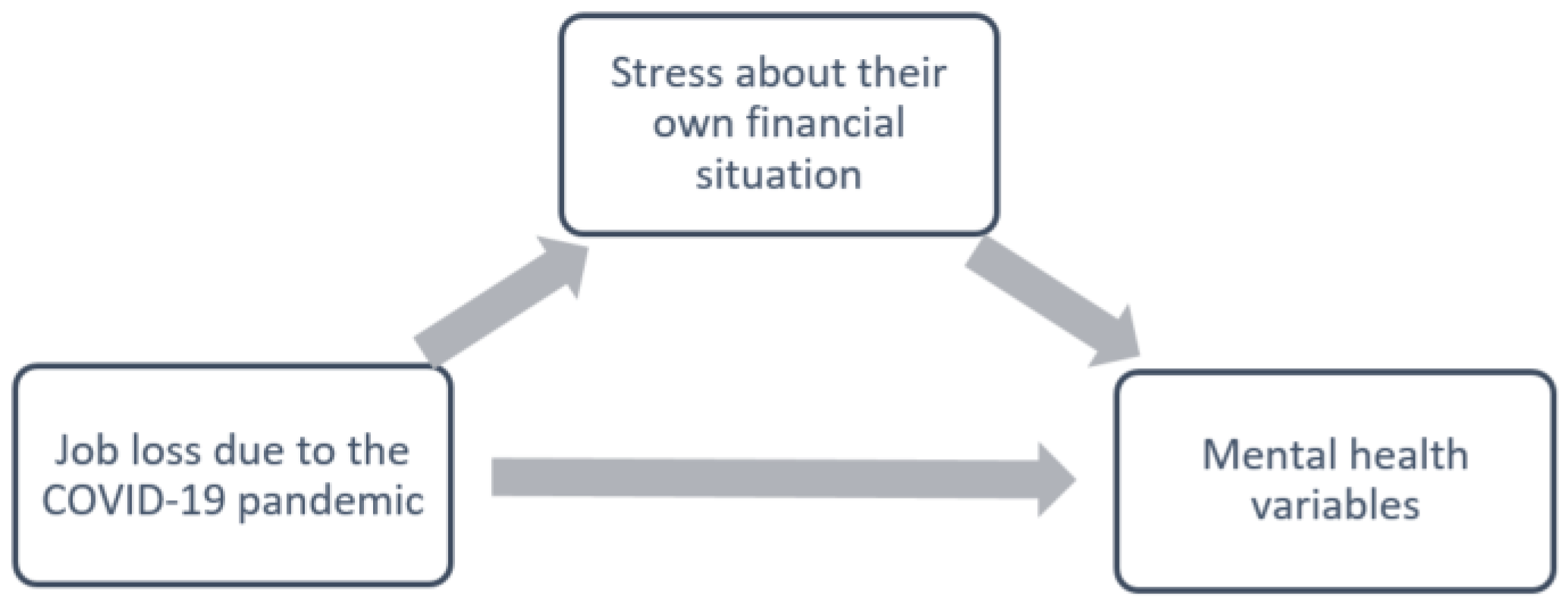
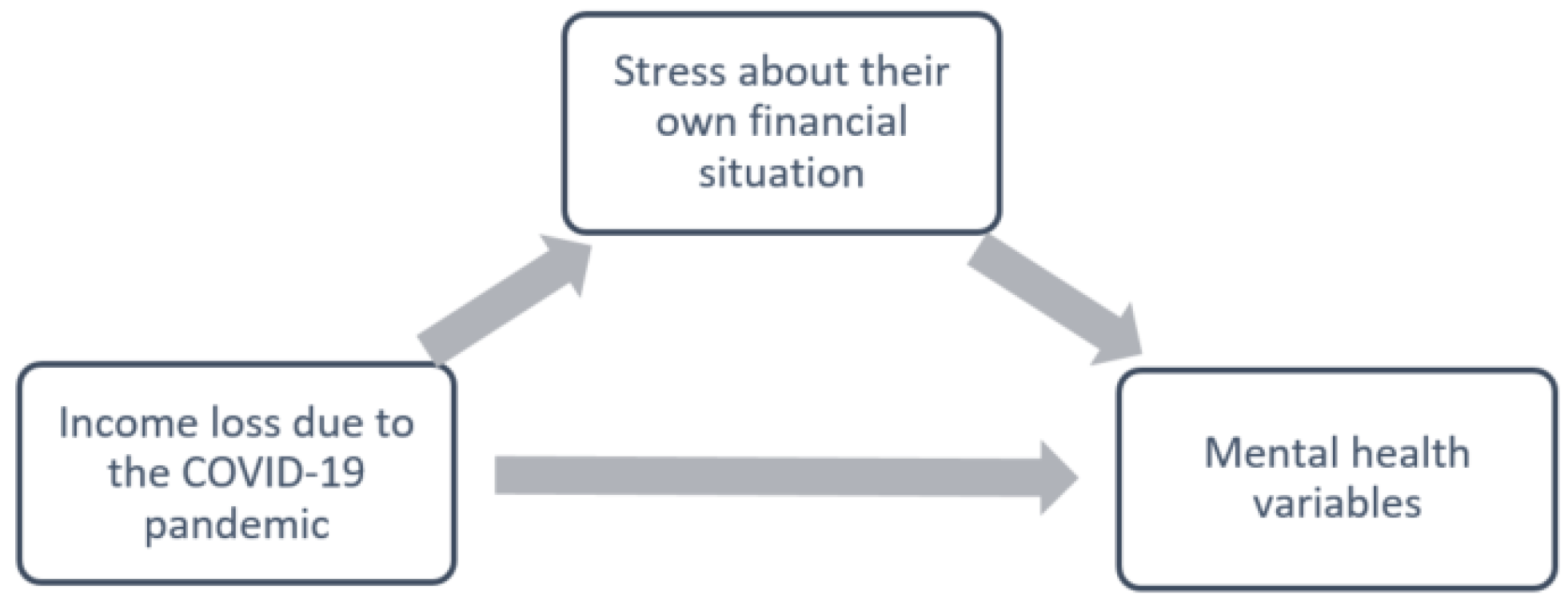
3.3. Mediation Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Salari, N.; Hosseinian-Far, A.; Jalali, R.; Vaisi-Raygani, A.; Rasoulpoor, S.; Mohammadi, M.; Rasoulpoor, S.; Khaledi-Paveh, B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Glob. Health 2020, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Covid-19: WHO declares pandemic because of “alarming levels” of spread, severity, and inaction. BMJ 2020, 368, m1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- ILO. ILO Monitor: COVID-19 and the world of work. Updated Estimates and Analysis, 7th ed.; International Labour Organisation: Geneva, Switzerland, 2021. [Google Scholar]
- Public State Employment Service Demandantes de Empleo, Paro, Contratos y Prestaciones por Desempleo. Diciembre 2020. Datos los Regist. del Serv. Público Empl. Estatal. 2021. Available online: https://www.sepe.es/HomeSepe/que-es-el-sepe/estadisticas/datos-avance/datos.html (accessed on 10 October 2021).
- La Revista de la Seguridad Social. El Número de Personas en ERTE se sitúa en 755000 a 31 de Diciembre. Secretaría de Estado de la Seguridad Social y Pensiones. 2021. Available online: https://revista.seg-social.es/-/el-n%C3%BAmero-de-personas-en-erte-se-sit%C3%BAa-en-755.000-a-31-de-diciembre#:~:text=Publicador%20de%20contenidos-,El%20n%C3%BAmero%20de%20personas%20en%20ERTE%20se,755.000%20a%2031%20de%20diciembre&text=El%20a%C3%B1o%202020%20cerr%C3%B3%20con,el%20pasado%20mes%20de%20septiembre (accessed on 15 October 2021).
- Graetz, B. Health consequences of employment and unemployment: Longitudinal evidence for young men and women. Soc. Sci. Med. 1993, 36, 715–724. [Google Scholar] [CrossRef]
- Burgard, S.A.; Brand, J.E.; House, J.S. Toward a better estimation of the effect of job loss on health. J. Health Soc. Behav. 2007, 48, 369–384. [Google Scholar] [CrossRef]
- Paul, K.I.; Moser, K. Unemployment impairs mental health: Meta-analyses. J. Vocat. Behav. 2009, 74, 264–282. [Google Scholar] [CrossRef]
- Evans-Lacko, S.; Knapp, M.; McCrone, P.; Thornicroft, G.; Mojtabai, R. The Mental Health Consequences of the Recession: Economic Hardship and Employment of People with Mental Health Problems in 27 European Countries. PLoS ONE 2013, 8, e69792. [Google Scholar] [CrossRef] [Green Version]
- International Labour Organization. International Labour Organization COVID-19: Protecting Workers in the Workplace: Almost 25 Million Jobs Could Be Lost Worldwide as a Result of COVID-19, Says ILO. 2020. Available online: https://www.ilo.org/global/about-the-ilo/newsroom/news/WCMS_738742/lang--en/index.htm (accessed on 25 November 2021).
- Frasquilho, D.; Matos, M.G.; Salonna, F.; Guerreiro, D.; Storti, C.C.; Gaspar, T.; Caldas-de-Almeida, J.M. Mental health outcomes in times of economic recession: A systematic literature review. BMC Public Health 2015, 16, 1–40. [Google Scholar] [CrossRef] [Green Version]
- Modrek, S.; Stuckler, D.; McKee, M.; Cullen, M.R.; Basu, S. A Review of Health Consequences of Recessions Internationally and a Synthesis of the US Response during the Great Recession. Public Health Rev. 2013, 35, 1–33. [Google Scholar] [CrossRef] [Green Version]
- Margerison-Zilko, C.; Goldman-Mellor, S.; Falconi, A.; Downing, J. Health Impacts of the Great Recession: A Critical Review. Curr. Epidemiol. Rep. 2016, 3, 81–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Campo, P.; Molnar, A.; Ng, E.; Renahy, E.; Mitchell, C.; Shankardass, K.; St. John, A.; Bambra, C.; Muntaner, C. Social welfare matters: A realist review of when, how, and why unemployment insurance impacts poverty and health. Soc. Sci. Med. 2015, 132, 88–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamayo-Fonseca, N.; Nolasco, A.; Moncho, J.; Barona, C.; Irles, M.Á.; Más, R.; Girón, M.; Gómezbeneyto, M.; Pereyrazamora, P. Contribution of the economic crisis to the risk increase of poor mental health in a region of spain. Int. J. Environ. Res. Public Health 2018, 15, 2517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cuellar, A.; Mark, T.L.; Sharfstein, S.S.; Huskamp, H.A. How to Mitigate the Mental Health Care Consequences of the COVID-19 Financial Crisis. Psychiatr. Serv. 2020, 71, 1317–1319. [Google Scholar] [CrossRef]
- Bareket-Bojmel, L.; Shahar, G.; Margalit, M. COVID-19-Related Economic Anxiety Is As High as Health Anxiety: Findings from the USA, the UK, and Israel. Int. J. Cogn. Ther. 2020, 14, 566–574. [Google Scholar] [CrossRef]
- Giorgi, G.; Lecca, L.I.; Alessio, F.; Finstad, G.L.; Bondanini, G.; Lulli, L.G.; Arcangeli, G.; Mucci, N. COVID-19-related mental health effects in the workplace: A narrative review. Int. J. Environ. Res. Public Health 2020, 17, 7857. [Google Scholar] [CrossRef]
- Ganson, K.T.; Tsai, A.C.; Weiser, S.D.; Benabou, S.E.; Nagata, J.M. Job Insecurity and Symptoms of Anxiety and Depression among, U.S. Young Adults during COVID-19. J. Adolesc. Health 2021, 68, 43–52. [Google Scholar] [CrossRef] [PubMed]
- McDowell, C.P.; Herring, M.P.; Lansing, J.; Brower, C.S.; Meyer, J.D. Associations Between Employment Changes and Mental Health: US Data from during the COVID-19 Pandemic. Front. Psychol. 2021, 12, 255. [Google Scholar] [CrossRef] [PubMed]
- Posel, D.; Oyenubi, A.; Kollamparambil, U. Job loss and mental health during the COVID-19 lockdown: Evidence from South Africa. PLoS ONE 2021, 16, e0249352. [Google Scholar] [CrossRef] [PubMed]
- Ruengorn, C.; Awiphan, R.; Wongpakaran, N.; Wongpakaran, T.; Nochaiwong, S. Association of job loss, income loss, and financial burden with adverse mental health outcomes during coronavirus disease 2019 pandemic in Thailand: A nationwide cross-sectional study. Depress. Anxiety 2021, 38, 648–660. [Google Scholar] [CrossRef] [PubMed]
- Witteveen, D.; Velthorst, E. Economic hardship and mental health complaints during COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 27277–27284. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Richard, S., Lazarus, R.S., Susan, F., Eds.; Springer: New York, NY, USA, 1984. [Google Scholar]
- Marjanovic, Z.; Greenglass, E.R.; Fiksenbaum, L.; De Witte, H.; Garcia-Santos, F.; Buchwald, P.; Peiró, J.M.; Mañas, M.A. Evaluation of the Financial Threat Scale (FTS) in four European, non-student samples. J. Behav. Exp. Econ. 2015, 55, 72–80. [Google Scholar] [CrossRef]
- Fiksenbaum, L.; Marjanovic, Z.; Greenglass, E.; Garcia-Santos, F. Impact of Economic Hardship and Financial Threat on Suicide Ideation and Confusion. J. Psychol. Interdiscip. Appl. 2017, 151, 477–495. [Google Scholar] [CrossRef] [PubMed]
- Marjanovic, Z.; Greenglass, E.R.; Fiksenbaum, L.; Bell, C.M. Psychometric evaluation of the Financial Threat Scale (FTS) in the context of the great recession. J. Econ. Psychol. 2013, 36, 1–10. [Google Scholar] [CrossRef]
- Dawel, A.; Shou, Y.; Smithson, M.; Cherbuin, N.; Banfield, M.; Calear, A.L.; Farrer, L.M.; Gray, D.; Gulliver, A.; Housen, T.; et al. The Effect of COVID-19 on Mental Health and Wellbeing in a Representative Sample of Australian Adults. Front. Psychiatry 2020, 11, 1026. [Google Scholar] [CrossRef]
- Wilson, J.M.; Lee, J.; Fitzgerald, H.N.; Oosterhoff, B.; Sevi, B.; Shook, N.J. Job Insecurity and Financial Concern during the COVID-19 Pandemic Are Associated with Worse Mental Health. J. Occup. Environ. Med. 2020, 62, 686–691. [Google Scholar] [CrossRef]
- Alcover, C.M.; Salgado, S.; Nazar, G.; Ramírez-Vielma, R.; González-Suhr, C. Job insecurity, financial threat and mental health in the COVID-19 context: The buffer role of perceived social support. medRxiv 2020, in press.
- Lee, M.-H.; Tsai, H.-Y. A study of job insecurity and life satisfaction in COVID-19: The multilevel moderating effect of perceived control and work–life balance programs. J. Men’s Health 2022, 18, 21. [Google Scholar] [CrossRef]
- Alonso, J.; Vilagut, G.; Mortier, P.; Ferrer, M.; Alayo, I.; Aragón-Peña, A.; Aragonès, E.; Campos, M.; Cura-González, I.D.; Emparanza, J.I.; et al. Mental health impact of the first wave of COVID-19 pandemic on Spanish healthcare workers: A large cross-sectional survey. Rev. Psiquiatr. Salud Ment. 2021, 14, 90–105. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística España en Cifras 2020. España en Cifras; Instituto Nacional de Estadística España: Madrid, Spain, 2020. [Google Scholar]
- Kroenke, K.; Strine, T.W.; Spitzer, R.L.; Williams, J.B.W.; Berry, J.T.; Mokdad, A.H. The PHQ-8 as a measure of current depression in the general population. J. Affect. Disord. 2009, 114, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Pressler, S.J.; Subramanian, U.; Perkins, S.M.; Gradus-Pizlo, I.; Kareken, D.; Kim, J.S.; Ding, Y.; Sauvé, M.J.; Sloan, R. Measuring depressive symptoms in heart failure: Validity and reliability of the patient health Questionnaire-8. Am. J. Crit. Care 2011, 20, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plummer, F.; Manea, L.; Trepel, D.; McMillan, D. Screening for anxiety disorders with the GAD-7 and GAD-2: A systematic review and diagnostic metaanalysis. Gen. Hosp. Psychiatry 2016, 39, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. The PTSD Checklist for DSM-5 (PCL-5). Natl. Cent. PTSD 2013, 5, 1–3. [Google Scholar]
- Zuromski, K.L.; Ustun, B.; Hwang, I.; Keane, T.M.; Marx, B.P.; Stein, M.B.; Ursano, R.J.; Kessler, R.C. Developing an optimal short-form of the PTSD Checklist for DSM-5 (PCL-5). Depress. Anxiety 2019, 36, 790–800. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Santiago, P.N.; Colpe, L.J.; Dempsey, C.L.; First, M.B.; Heeringa, S.G.; Stein, M.B.; Fullerton, C.S.; Gruber, M.J.; Naifeh, J.A.; et al. Clinical reappraisal of the Composite International Diagnostic Interview Screening Scales (CIDI-SC) in the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). Int. J. Methods Psychiatr. Res. 2013, 22, 303–321. [Google Scholar] [CrossRef]
- Brown, R.L.; Rounds, L.A. Conjoint screening questionnaires for alcohol and other drug abuse: Criterion validity in a primary care practice. Wis. Med. J. 1995, 94, 135–140. [Google Scholar] [PubMed]
- Sáiz, P.A.; G-Portilla, M.P.; Paredes, M.B.; Bascarán, M.T.; Bobes, J. Instrumentos de evaluación en alcoholismo. Adicciones 2002, 14 (Suppl. S1). [Google Scholar] [CrossRef] [Green Version]
- Posner, K.; Brown, G.K.; Stanley, B.; Brent, D.A.; Yershova, K.V.; Oquendo, M.A.; Currier, G.W.; Melvin, G.A.; Greenhill, L.; Shen, S.; et al. The Columbia-suicide severity rating scale: Initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am. J. Psychiatry 2011, 168, 1266–1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dohrenwend, B.S.; Krasnoff, L.; Askenasy, A.R.; Dohrenwend, B.P. Examplification of a method for scaling life events: The Peri life events scale. J. Health Soc. Behav. 1978, 19, 205–229. [Google Scholar] [CrossRef]
- Imai, K.; Keele, L.; Tingley, D. A General Approach to Causal Mediation Analysis. Psychol. Methods 2010, 15, 309. [Google Scholar] [CrossRef] [Green Version]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Commun. Monogr. 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Preacher, K.J.; Hayes, A.F. Contemporary Approaches to Assessing Mediation in Communication Research. In The SAGE Sourcebook of Advanced Data Analysis Methods for Communication Research; SAGE Publishing: Newbury Park, CA, USA, 2014. [Google Scholar]
- Meule, A. Contemporary Understanding of Mediation Testing. Meta-Psychology 2019, 3. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Tingley, D.; Yamamoto, T.; Hirose, K.; Keele, L.; Imai, K. Mediation: R package for causal mediation analysis. J. Stat. Softw. 2014, 59, 1–32. [Google Scholar] [CrossRef] [Green Version]
- Chislett, W. Challenges and Opportunities for Spain in Times of COVID-19; Real Instituto Elcano: Madrid, Spain, 2021. [Google Scholar]
- European Commission Details of Spain’s Support Measures to Help Citizens and Companies during the Significant Economic Impact of the Coronavirus Pandemic. Available online: https://ec.europa.eu/info/live-work-travel-eu/coronavirus-response/jobs-and-economy-during-coronavirus-pandemic/state-aid-cases/spain_en (accessed on 30 October 2021).
- Dirección General de Industria y de la PYME. Cifras PYME. 2021. Available online: http://www.ipyme.org/es-ES/publicaciones/Paginas/estadisticaspyme.aspx (accessed on 30 October 2021).
- Dimson, J.; Mladenov, Z.; Sharma, R.; Tadjeddine, K. COVID-19 and European Small and Medium-Size Enterprises: How They Are Weathering the Storm; McKinsey Co.: New York, NY, USA, 2020. [Google Scholar]
- Zhao, X.; Lynch, J.G.; Chen, Q. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Solove, E.; Fisher, G.G.; Kraiger, K. Coping with Job Loss and Reemployment: A Two-Wave Study. J. Bus. Psychol. 2015, 30, 529–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caravan, M.; Gallo, W.T.; Marshall, G.L. The Moderating Effect of Social Support and Social Integration on the Relationship Between Involuntary Job Loss and Health. J. Appl. Gerontol. 2020, 40, 1272–1279. [Google Scholar] [CrossRef]
- Milner, A.; Krnjacki, L.; Butterworth, P.; LaMontagne, A.D. The role of social support in protecting mental health when employed and unemployed: A longitudinal fixed-effects analysis using 12 annual waves of the HILDA cohort. Soc. Sci. Med. 2016, 153, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; McGonagle, K.A.; Zhao, S.; Nelson, C.B.; Hughes, M.; Eshleman, S.; Wittchen, H.U.; Kendler, K.S. Lifetime and 12-Month Prevalence of DSM-III-R Psychiatric Disorders in the United States: Results from the National Comorbidity Survey. Arch. Gen. Psychiatry 1994, 51, 8–19. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Weighted | |
|---|---|
| Mean ± SD or % (95% CI) | |
| Age (Mean ± SD) | 43.0 ± 11.8 |
| Gender (%) | |
| Female | 47.48% (45.39–49.58%) |
| Male | 52.53% (50.42–54.61%) |
| Marital Status (%) | |
| Single | 42.38% (40.32–44.47%) |
| Married | 47.87% (45.77–49.96%) |
| Divorced | 8.81% (7.66–10.06%) |
| Widower | 0.94% (0.59–1.44%) |
| Education Level (%) | |
| Primary school | 2.88% (2.22–3.66%) |
| Secondary school | 16.55% (15.02–18.16%) |
| High school | 13.89% (12.48–15.40%) |
| Professional Training, intermediate degree | 9.26% (8.09–10.54%) |
| Professional Training, higher degree | 11.92% (10.60–13.33%) |
| Bachelor’s degree | 34.12% (32.16–36.14%) |
| Postgraduate degree | 11.38% (10.09–12.77%) |
| Working situation (%) | |
| Employed | 71.67% (69.75–73.54%) |
| Employed on sick leave for more than 3 months | 3.24% (2.54–4.06%) |
| Unemployed receiving benefits/subsidy | 13.22% (11.84–14.70%) |
| Unemployed without benefits/subsidy | 11.92% (10.60–13.33%) |
| Depression (% above cut-off) | 11.56% (10.26–12.96%) |
| GAD (% above cut-off) | 11.42% (10.13–12.82%) |
| PTSD (% above cut-off) | 10.57% (9.32–11.92%) |
| Panic attacks (% presence of panic attacks) | 10.39% (9.15–11.73%) |
| SUD (% above cut-off) | 3.60% (2.86–4.46%) |
| STB (% presence of STBs) | 3.78% (3.02–4.66%) |
| Unemployment due to pandemic (%) | |
| Yes | 26.93% (25.10–28.83%) |
| No | 73.25% (71.35–75.08%) |
| Loss of income due to pandemic (%) | |
| Yes | 42.49% (40.43–44.58%) |
| No | 57.55% (55.47–59.62%) |
| Perceived financial stress (Mean ± SD) | 2.48 ± 1.33 |
| Depression | GAD | PTSD | Panic Attacks | SUD | STB | |
|---|---|---|---|---|---|---|
| Job loss | 1.48 (1.12–1.95) * | 1.19 (0.90–1.59) | 1.35 (1.01–1.81) * | 1.26 (0.94–1.69) | 0.98 (0.59–1.63) | 2.11 (1.36–3.28) ** |
| Income loss | 1.30 (1.00–1.69) * | 1.28 (0.99–1.67) | 1.37 (1.04–1.79) * | 1.49 (1.13–1.96) * | 0.88 (0.55–1.38) | 0.98 (0.63–1.52) |
| Depression | GAD | PTSD | Panic Attacks | SUD | STB | |
|---|---|---|---|---|---|---|
| Job loss | 1.20 (0.90–1.60) | 0.93 (0.69–1.26) | 1.11 (0.82–1.50) | 1.02 (0.75–1.39) | 0.80 (0.47–1.34) | 1.67 (1.06–2.63) * |
| Income loss | 1.17 (0.90–1.52) | 1.14 (0.87–1.49) | 1.27 (0.96–1.68) | 1.39 (1.05–1.84) * | 0.78 (0.49–1.23) | 0.85 (0.54–1.33) |
| Outcome | Coefficient (95% CI) | p-Value | ||
|---|---|---|---|---|
| Depression | Total Effect | 0.02 (−0.01, 0.05) | 0.19 | |
| (Yes/No) | Direct Effect | −0.01 (−0.04, 0.02) | 0.52 | |
| Financial Stress | Indirect Effect | 0.03 (0.02, 0.04) | <0.001 ** | |
| PTSD (Yes/No) | Total Effect | 0.01 (−0.02, 0.04) | 0.47 | |
| Direct Effect | −0.01 (−0.04, 0.01) | 0.31 | ||
| Financial Stress | Indirect Effect | 0.02 (0.02, 0.03) | <0.001 ** | |
| GAD (Yes/No) | Total Effect | −0.01 (−0.03, 0.02) | 0.71 | |
| Direct Effect | −0.03 (−0.06, 0.00) | 0.03 * | ||
| Financial Stress | Indirect Effect | 0.02 (0.02, 0.03) | <0.001 ** | |
| Panic attacks | Total Effect | 0.00 (−0.02, 0.03) | 0.87 | |
| (Yes/No) | Direct Effect | −0.02 (−0.04, 0.00) | 0.08 | |
| Financial Stress | Indirect Effect | 0.03 (0.02, 0.04) | <0.001 ** | |
| SUD | Total Effect | −0.01 (−0.02, 0.01) | 0.43 | |
| (Yes/No) | Direct Effect | −0.01 (−0.03, 0.00) | 0.15 | |
| Financial Stress | Indirect Effect | 0.01 (0.00, 0.01) | 0.01 * | |
| STB | Total Effect | 0.02 (0.00, 0.04) | 0.04 * | |
| (Yes/No) | Direct Effect | 0.01 (−0.00, 0.03) | 0.16 | |
| Financial Stress | Indirect Effect | 0.01 (0.00, 0.01) | 0.003 * |
| Outcome | Coefficient (95% CI) | p-Value | ||
|---|---|---|---|---|
| Depression | Total Effect | 0.02 (−0.01, 0.04) | 0.25 | |
| (Yes/No) | Direct Effect | −0.02 (−0.05, 0.01) | 0.12 | |
| Financial Stress | Indirect Effect | 0.04 (0.03, 0.05) | <0.001 ** | |
| PTSD (Yes/No) | Total Effect | 0.02 (−0.00, 0.05) | 0.10 | |
| Direct Effect | −0.01 (−0.03, 0.02) | 0.53 | ||
| Financial Stress | Indirect Effect | 0.03 (0.02, 0.04) | <0.001 ** | |
| GAD (Yes/No) | Total Effect | 0.01 (−0.01, 0.04) | 0.32 | |
| Direct Effect | −0.02 (−0.05, 0.01) | 0.18 | ||
| Financial Stress | Indirect Effect | 0.03 (0.02, 0.04) | <0.001 ** | |
| Panic attacks | Total Effect | 0.03 (0.00, 0.06) | 0.02 * | |
| (Yes/No) | Direct Effect | −0.00 (−0.03, 0.02) | 0.91 | |
| Financial Stress | Indirect Effect | 0.03 (0.02, 0.04) | <0.001 ** | |
| SUD | Total Effect | −0.00 (−0.02, 0.01) | 0.30 | |
| (Yes/No) | Direct Effect | −0.02 (−0.03, 0.00) | 0.06 | |
| Financial Stress | Indirect Effect | 0.01 (0.00, 0.01) | 0.01 * | |
| STB | Total Effect | −0.01 (−0.02, 0.01) | 0.50 | |
| (Yes/No) | Direct Effect | −0.02 (−0.03, 0.00) | 0.06 | |
| Financial Stress | Indirect Effect | 0.01 (0.00, 0.02) | <0.001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Miquel, C.; Domènech-Abella, J.; Felez-Nobrega, M.; Cristóbal-Narváez, P.; Mortier, P.; Vilagut, G.; Alonso, J.; Olaya, B.; Haro, J.M. The Mental Health of Employees with Job Loss and Income Loss during the COVID-19 Pandemic: The Mediating Role of Perceived Financial Stress. Int. J. Environ. Res. Public Health 2022, 19, 3158. https://doi.org/10.3390/ijerph19063158
de Miquel C, Domènech-Abella J, Felez-Nobrega M, Cristóbal-Narváez P, Mortier P, Vilagut G, Alonso J, Olaya B, Haro JM. The Mental Health of Employees with Job Loss and Income Loss during the COVID-19 Pandemic: The Mediating Role of Perceived Financial Stress. International Journal of Environmental Research and Public Health. 2022; 19(6):3158. https://doi.org/10.3390/ijerph19063158
Chicago/Turabian Stylede Miquel, Carlota, Joan Domènech-Abella, Mireia Felez-Nobrega, Paula Cristóbal-Narváez, Philippe Mortier, Gemma Vilagut, Jordi Alonso, Beatriz Olaya, and Josep Maria Haro. 2022. "The Mental Health of Employees with Job Loss and Income Loss during the COVID-19 Pandemic: The Mediating Role of Perceived Financial Stress" International Journal of Environmental Research and Public Health 19, no. 6: 3158. https://doi.org/10.3390/ijerph19063158
APA Stylede Miquel, C., Domènech-Abella, J., Felez-Nobrega, M., Cristóbal-Narváez, P., Mortier, P., Vilagut, G., Alonso, J., Olaya, B., & Haro, J. M. (2022). The Mental Health of Employees with Job Loss and Income Loss during the COVID-19 Pandemic: The Mediating Role of Perceived Financial Stress. International Journal of Environmental Research and Public Health, 19(6), 3158. https://doi.org/10.3390/ijerph19063158