
The Development, Implementation, and Feasibility of a Circadian, Light, and Sleep Skills Program for Shipboard Military Personnel (CLASS-SM)

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
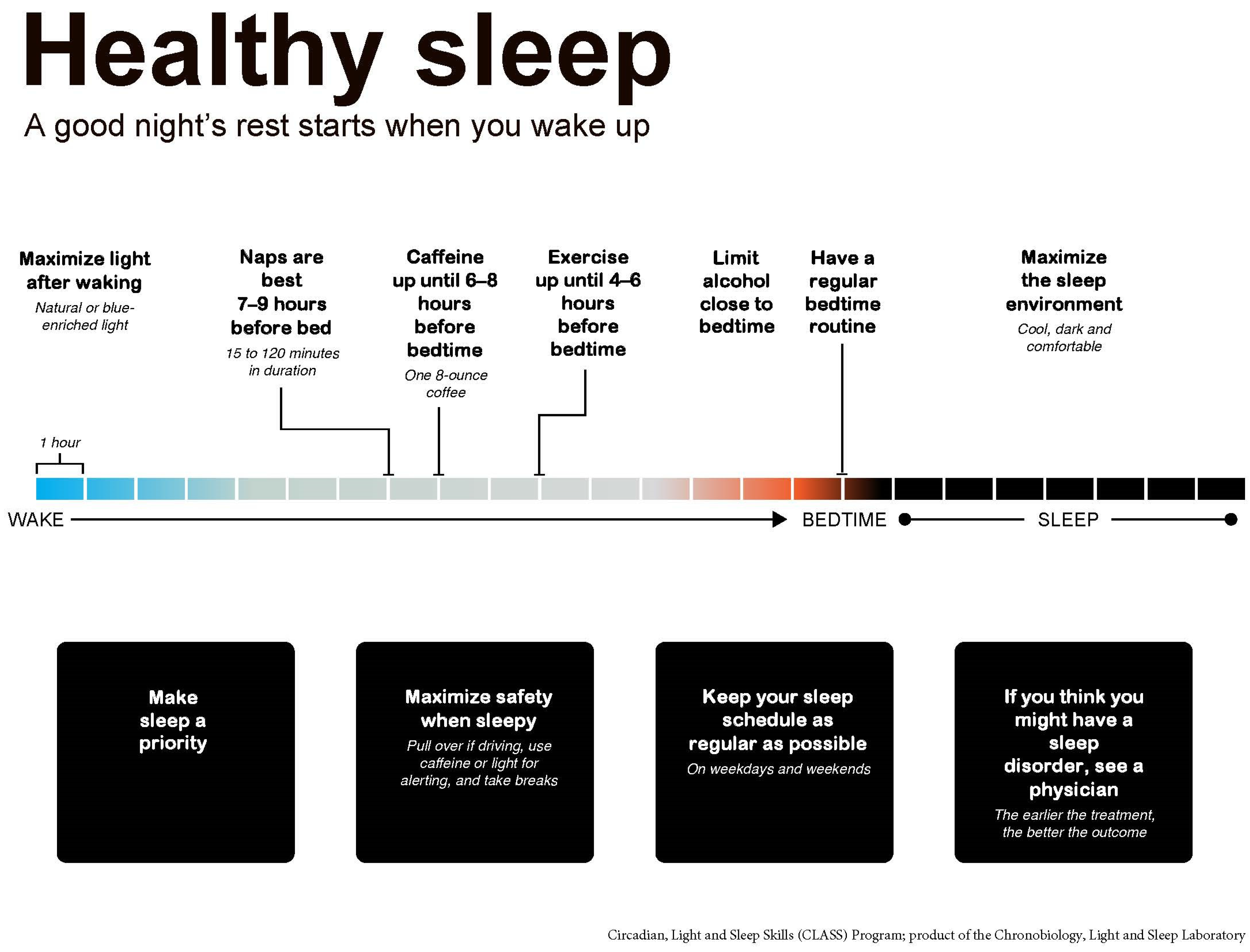
2.2. CLASS Program Description
2.3. Adaptation of CLASS Content Areas
2.4. Reinforcing Text Messages
- Week 1: Sleep is important to both physical and mental functioning. Make sleep a priority, as best as you can, wherever you can.
- Week 2: To help you feel more alert when you wake up, expose yourself to bright light right after waking, using sunlight or artificial blue-enriched light.
- Week 3: If needed, caffeine is best earlier in the day, and should be avoided (if possible) in the 6 h before bedtime, to prevent trouble falling asleep later.
- Week 4: Having trouble falling asleep? Try a muscle relaxation exercise, such as the one you learned in the sleep CLASS.
2.5. Program Length
2.6. Participants and Recruitment
2.7. Phase 1: Formative Evaluation of CLASS-M and Evolution to CLASS-SM
2.7.1. Methods
2.7.2. Measures
2.8. Phase 2—Feasibility and Acceptability of CLASS-SM
2.8.1. Methods
2.8.2. Measures
2.9. Analysis
3. Results
3.1. Phase 1—Participant Characteristics and Feedback
3.2. Phase 2—Participant Characteristics
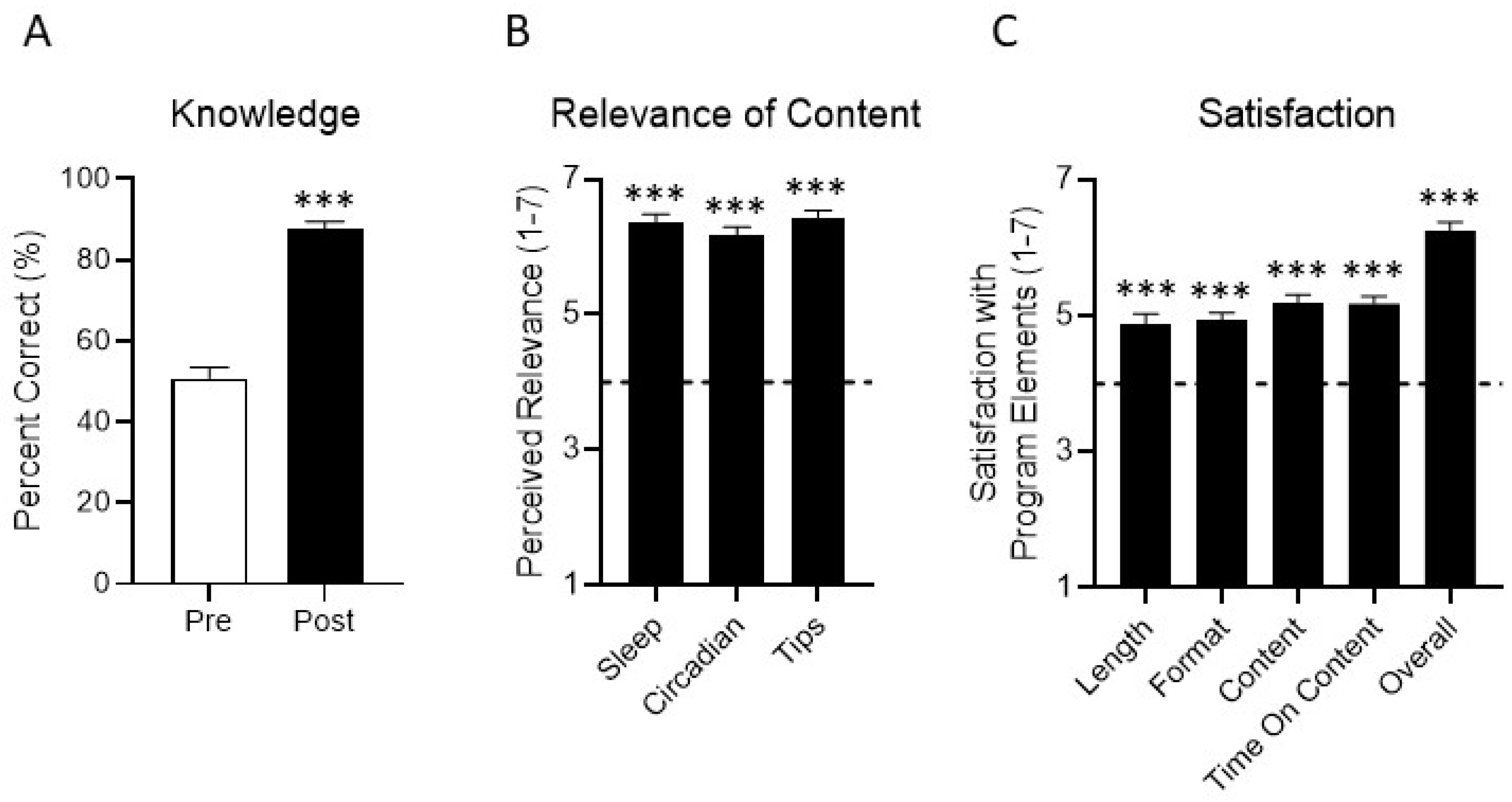
3.3. Sleep-Related Knowledge
3.4. Acceptability Indicators (Program Relevance and Satisfaction)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Harrison, E.M.; Glickman, G.L.; Beckerley, S.; Taylor, M.K. Self-Reported Sleep During U.S. Navy Operations and the Impact of Deployment-Related Factors. Mil. Med. 2017, 182, 189–194. [Google Scholar] [CrossRef] [PubMed]
- LoPresti, M.L.; Anderson, J.A.; Saboe, K.N.; McGurk, D.L.; Balkin, T.J.; Sipos, M.L. The impact of insufficient sleep on combat mission performance. Mil. Behav. Health 2016, 4, 356–363. [Google Scholar] [CrossRef]
- Seelig, A.D.; Jacobson, I.G.; Donoho, C.J.; Trone, D.W.; Crum-Cianflone, N.F.; Balkin, T.J. Sleep and Health Resilience Metrics in a Large Military Cohort. Sleep 2016, 39, 1111–1120. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.D.; Kolaja, C.A.; Markwald, R.R.; Jacobson, I.G.; Chinoy, E.D. Longitudinal associations of military-related factors on self-reported sleep among U.S. service members. Sleep 2021, 44, zsab168. [Google Scholar] [CrossRef] [PubMed]
- Caldwell, J.A.; Caldwell, J.L. Fatigue in military aviation: An overview of US military-approved pharmacological countermeasures. Aviat. Space Environ. Med. 2005, 76, C39–C51. [Google Scholar] [PubMed]
- Crowley, S.K.; Wilkinson, L.L.; Burroughs, E.L.; Muraca, S.T.; Wigfall, L.T.; Louis-Nance, T.; Williams, E.M.; Glover, S.H.; Youngstedt, S.D. Sleep during basic combat training: A qualitative study. Mil. Med. 2012, 177, 823–828. [Google Scholar] [CrossRef] [PubMed]
- Miller, N.L.; Shattuck, L.G. Sleep patterns of young men and women enrolled at the United States Military Academy: Results from year 1 of a 4-year longitudinal study. Sleep 2005, 28, 837–841. [Google Scholar] [CrossRef]
- Troxel, W.M.; Shih, R.A.; Pedersen, E.R.; Geyer, L.; Fisher, M.P.; Griffin, B.A.; Haas, A.C.; Kurz, J.; Steinberg, P.S. Sleep in the military: Promoting healthy sleep among US servicemembers. Rand Health Q. 2015, 5, 19. [Google Scholar]
- Mantua, J.; Bessey, A.; Sowden, W.J.; Chabuz, R.; Brager, A.J.; Capaldi, V.F.; Simonelli, G. A Review of Environmental Barriers to Obtaining Adequate Sleep in the Military Operational Context. Mil. Med. 2019, 184, e259–e266. [Google Scholar] [CrossRef]
- Good, C.H.; Brager, A.J.; Capaldi, V.F.; Mysliwiec, V. Sleep in the United States Military. Neuropsychopharmacology 2020, 45, 176–191. [Google Scholar] [CrossRef]
- Schmied, E.A.; Harrison, E.M.; Dell’Acqua, R.G.; Perez, V.G.; Glickman, G.; Hurtado, S.L. A Qualitative Examination of Factors That Influence Sleep Among Shipboard Sailors. Mil. Med. 2021, 186, e160–e168. [Google Scholar] [CrossRef] [PubMed]
- Lincoln, M.L.; Moore, R.S.; Ames, G.M. Sleep disturbances after deployment: National Guard soldiers’ experiences and strategies. Sleep Health 2018, 4, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.G.; Collen, J.; Wickwire, E.; Lettieri, C.J.; Mysliwiec, V. The impact of sleep on soldier performance. Curr. Psychiatry Rep. 2014, 16, 459. [Google Scholar] [CrossRef] [PubMed]
- Shattuck, N.L.M.P.; Dahlman, A.S. Sleep and Fatigue Issues in Military Operations. In Sleep and Combat-Related Post Traumatic Stress Disorder; Vermetten, E., Ed.; Springer Science + Business Media LLC: New York, NY, USA, 2018; pp. 69–76. [Google Scholar]
- Mysliwiec, V.; McGraw, L.; Pierce, R.; Smith, P.; Trapp, B.; Roth, B.J. Sleep disorders and associated medical comorbidities in active duty military personnel. Sleep 2013, 36, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; Kushida, C.; et al. Recommended Amount of Sleep for a Healthy Adult: A Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society. Sleep 2015, 38, 843–844. [Google Scholar] [CrossRef] [PubMed]
- Meadows, S.O.; Engel, C.C.; Collins, R.L.; Beckman, R.L.; Breslau, J.; Bloom, E.L.; Dunbar, M.S.; Gilbert, M.L.; Grant, D.; Hawes-Dawson, J. 2018 Department of Defense Health Related Behaviors Survey (HRBS); Rand Health Quarterly: Santa Monica, CA, USA, 2021. [Google Scholar]
- Smith, C.D.; Cooper, A.D.; Merullo, D.J.; Cohen, B.S.; Heaton, K.J.; Claro, P.J.; Smith, T. Sleep restriction and cognitive load affect performance on a simulated marksmanship task. J. Sleep Res. 2019, 28, e12637. [Google Scholar] [CrossRef] [PubMed]
- Lentino, C.V.; Purvis, D.L.; Murphy, K.J.; Deuster, P.A. Sleep as a component of the performance triad: The importance of sleep in a military population. US Army Med. Dep. J. 2013, 98–108. Available online: https://pubmed.ncbi.nlm.nih.gov/24146247/ (accessed on 29 November 2021).
- Shattuck, N.L.; Shattuck, L.G.; Matsangas, P. Combat effectiveness and sleep patterns in US Marines. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, Los Angeles, CA, USA, 19–23 September 2016; pp. 886–890. [Google Scholar]
- Luyster, F.S.; Strollo, P.J.; Zee, P.C.; Walsh, J.K. Sleep: A health imperative. Sleep 2012, 35, 727–734. [Google Scholar] [CrossRef]
- Boyko, E.J.; Seelig, A.D.; Jacobson, I.G.; Hooper, T.I.; Smith, B.; Smith, T.C.; Crum-Cianflone, N.F.; Team, M.C.S. Sleep characteristics, mental health, and diabetes risk: A prospective study of US military service members in the Millennium Cohort Study. Diabetes Care 2013, 36, 3154–3161. [Google Scholar] [CrossRef]
- Livingston, W.S.; Rusch, H.L.; Nersesian, P.V.; Baxter, T.; Mysliwiec, V.; Gill, J.M. Improved sleep in military personnel is associated with changes in the expression of inflammatory genes and improvement in depression symptoms. Front. Psychiatry 2015, 6, 59. [Google Scholar] [CrossRef]
- Wentz, L.M.; Ward, M.D.; Potter, C.; Oliver, S.J.; Jackson, S.; Izard, R.M.; Greeves, J.P.; Walsh, N.P. Increased Risk of Upper Respiratory Infection in Military Recruits Who Report Sleeping Less Than 6 h per night. Mil. Med. 2018, 183, e699–e704. [Google Scholar] [CrossRef]
- Gehrman, P.; Seelig, A.D.; Jacobson, I.G.; Boyko, E.J.; Hooper, T.I.; Gackstetter, G.D.; Ulmer, C.S.; Smith, T.C.; Team, M.C.S. Predeployment sleep duration and insomnia symptoms as risk factors for new-onset mental health disorders following military deployment. Sleep 2013, 36, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Richardson, J.D.; King, L.; Cyr, K.S.; Shnaider, P.; Roth, M.L.; Ketcheson, F.; Balderson, K.; Elhai, J.D. Depression and the relationship between sleep disturbances, nightmares, and suicidal ideation in treatment-seeking Canadian Armed Forces members and veterans. BMC Psychiatry 2018, 18, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Gurubhagavatula, I.; Barger, L.K.; Barnes, C.M.; Basner, M.; Boivin, D.B.; Dawson, D.; Drake, C.L.; Flynn-Evans, E.E.; Mysliwiec, V.; Patterson, P.D. Guiding principles for determining work shift duration and addressing the effects of work shift duration on performance, safety, and health: Guidance from the American Academy of Sleep Medicine and the Sleep Research Society. Sleep 2021, 44, zsab161. [Google Scholar] [CrossRef] [PubMed]
- Hansen, L.P.; Kinskey, C.; Koffel, E.; Polusny, M.; Ferguson, J.; Schmer-Galunder, S.; Erbes, C.R. Sleep patterns and problems among Army National Guard soldiers. Mil. Med. 2018, 183, e396–e401. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.L.; Ganulin, M.L.; LoPresti, M.L.; Adler, A.B. Sleep knowledge, goals, and habits in soldiers. Sleep Health 2019, 5, 426–428. [Google Scholar] [CrossRef]
- Harrison, E.M.; Easterling, A.P.; Yablonsky, A.M.; Glickman, G.L. Sleep-Scheduling Strategies in Hospital Shiftworkers. Nat. Sci. Sleep 2021, 13, 1593. [Google Scholar] [CrossRef]
- Adler, A.B.; Bliese, P.D.; LoPresti, M.L.; McDonald, J.L.; Merrill, J.C. Sleep leadership in the army: A group randomized trial. Sleep Health 2021, 7, 24–30. [Google Scholar] [CrossRef]
- Holbrook, M.I.; White, M.H.; Hutt, M.J. Increasing awareness of sleep hygiene in rotating shift workers: Arming law-enforcement officers against impaired performance. Percept. Mot. Skills 1994, 79, 520–522. [Google Scholar] [CrossRef]
- Nakamura, Y.; Lipschitz, D.L.; Landward, R.; Kuhn, R.; West, G. Two sessions of sleep-focused mind–body bridging improve self-reported symptoms of sleep and PTSD in veterans: A pilot randomized controlled trial. J. Psychosom. Res. 2011, 70, 335–345. [Google Scholar] [CrossRef]
- Germain, A.; Richardson, R.; Moul, D.E.; Mammen, O.; Haas, G.; Forman, S.D.; Rode, N.; Begley, A.; Nofzinger, E.A. Placebo-controlled comparison of prazosin and cognitive-behavioral treatments for sleep disturbances in US Military Veterans. J. Psychosom. Res. 2012, 72, 89–96. [Google Scholar] [CrossRef]
- Ulmer, C.S.; Edinger, J.D.; Calhoun, P.S. A multi-component cognitive-behavioral intervention for sleep disturbance in veterans with PTSD: A pilot study. J. Clin. Sleep Med. 2011, 7, 57–68. [Google Scholar] [CrossRef] [PubMed]
- Patterson, P.D.; Buysse, D.J.; Weaver, M.D.; Doman, J.M.; Moore, C.G.; Suffoletto, B.P.; McManigle, K.L.; Callaway, C.W.; Yealy, D.M. Real-time fatigue reduction in emergency care clinicians: The SleepTrackTXT randomized trial. Am. J. Ind. Med. 2015, 58, 1098–1113. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.P.; O’Brien, C.S.; Barger, L.K.; Rajaratnam, S.M.; Czeisler, C.A.; Lockley, S.W.; Harvard Work Hours, H.; Group, S. Randomized, prospective study of the impact of a sleep health program on firefighter injury and disability. Sleep 2017, 40, zsw001. [Google Scholar] [CrossRef]
- Harrison, E.M.; Easterling, A.P.; Schmied, E.A.; Hurtado, S.L.; Glickman, G.L. Chronotype and self-reported sleep, alertness, and mental health in U.S. sailors. Mil. Med. Res. 2021, 8, 43. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.M.; Schmied, E.A.; Easterling, A.P.; Yablonsky, A.M.; Glickman, G.L. A Hybrid Effectiveness-Implementation Study of a Multi-Component Lighting Intervention for Hospital Shift Workers. Int. J. Environ. Res. Public Health 2020, 17, 9141. [Google Scholar] [CrossRef] [PubMed]
- Ee, J.S.; Berry-Cabán, C.S.; Nguyen, D.R.; Boyd, M.; Bennett, N. Soldiers’ perspectives of insomnia behavioral treatment in a primary care setting. J. Sleep Disord. Manag. 2016, 2, 012. [Google Scholar] [CrossRef][Green Version]
- Pedersen, E.R.; Troxel, W.M.; Shih, R.A.; Pinder, E.; Lee, D.; Geyer, L. Increasing resilience through promotion of healthy sleep among service members. Mil. Med. 2015, 180, 4–6. [Google Scholar] [CrossRef]
- Wesensten, N.J.; Balkin, T.J. The challenge of sleep management in military operations. US Army Med. Dep. J. 2013, 109–118. Available online: https://pubmed.ncbi.nlm.nih.gov/24146248/ (accessed on 29 November 2021).
- Albakri, U.; Drotos, E.; Meertens, R. Sleep Health Promotion Interventions and Their Effectiveness: An Umbrella Review. Int. J. Environ. Res. Public Health 2021, 18, 5533. [Google Scholar] [CrossRef]
- Duncan, E.; O’Cathain, A.; Rousseau, N.; Croot, L.; Sworn, K.; Turner, K.; Yardley, L.; Hoddinott, P. Guidance for reporting intervention development studies in health research (GUIDED): An evidence-based consensus study. BMJ Open 2020, 10, e033516. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, g1687. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.M.; Schmied, E.A.; Perez, V.G.; Hurtado, S.L.; Glickman, G.L. Can A Brief Sleep Education Training Improve Sleep Quality among Shipboard Sailors? Sleep 2021, 44, A124. [Google Scholar] [CrossRef]
- Glickman, G.L.; Harrison, E.M. It Takes a Village to Get a Good Night’s Sleep. In Proceedings of the University of Californa San Diego Center for Circadian Biology Symposium, San Diego, CA, USA, 26 February 2016. [Google Scholar]
- Becker, S.P.; Jarrett, M.A.; Luebbe, A.M.; Garner, A.A.; Burns, G.L.; Kofler, M.J. Sleep in a large, multi-university sample of college students: Sleep problem prevalence, sex differences, and mental health correlates. Sleep Health 2018, 4, 174–181. [Google Scholar] [CrossRef]
- Kinzie, M.B. Instructional design strategies for health behavior change. Patient Educ. Couns. 2005, 56, 3–15. [Google Scholar] [CrossRef]
- Rosenstock, I.M. Historical origins of the health belief model. Health Educ. Monogr. 1974, 2, 328–335. [Google Scholar] [CrossRef]
- Matsangas, P.; Shattuck, N.L. Habitability in berthing compartments and well-being of sailors working on US Navy surface ships. Hum. Factors 2021, 63, 462–473. [Google Scholar]
- Irish, L.A.; Kline, C.E.; Gunn, H.E.; Buysse, D.J.; Hall, M.H. The role of sleep hygiene in promoting public health: A review of empirical evidence. Sleep Med. Rev. 2015, 22, 23–36. [Google Scholar] [CrossRef]
- Youngstedt, S.D.; Elliott, J.A.; Kripke, D.F. Human circadian phase–response curves for exercise. J. Physiol. 2019, 597, 2253–2268. [Google Scholar] [CrossRef]
- Janse van Rensburg, D.C.; Jansen van Rensburg, A.; Fowler, P.M.; Bender, A.M.; Stevens, D.; Sullivan, K.O.; Fullagar, H.H.; Alonso, J.-M.; Biggins, M.; Claassen-Smithers, A. Managing travel fatigue and jet lag in athletes: A review and consensus statement. Sports Med. 2021, 51, 2029–2050. [Google Scholar] [CrossRef]
- Boivin, D.B.; Boudreau, P.; Kosmadopoulos, A. Disturbance of the Circadian System in Shift Work and Its Health Impact. J. Biol. Rhythm. 2022, 37, 3–28. [Google Scholar] [CrossRef]
- Eastman, C.I.; Boulos, Z.; Terman, M.; Campbell, S.S.; Dijk, D.-J.; Lewy, A.J. Light treatment for sleep disorders: Consensus report: VI. Shift work. J. Biol. Rhythm. 1995, 10, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Cajochen, C. Alerting effects of light. Sleep Med. Rev. 2007, 11, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Lowden, A.; Öztürk, G.; Reynolds, A.; Bjorvatn, B. Working Time Society consensus statements: Evidence based interventions using light to improve circadian adaptation to working hours. Ind. Health 2019, 57, 213–227. [Google Scholar] [PubMed]
- Richter, K.; Acker, J.; Adam, S.; Niklewski, G. Prevention of fatigue and insomnia in shift workers—a review of non-pharmacological measures. EPMA J. 2016, 7, 1–11. [Google Scholar] [CrossRef]
- Neil-Sztramko, S.E.; Pahwa, M.; Demers, P.A.; Gotay, C.C. Health-related interventions among night shift workers: A critical review of the literature. Scand. J. Work Environ. Health 2014, 40, 543–556. [Google Scholar] [CrossRef] [PubMed]
- Vetter, C.; Pattison, P.M.; Houser, K.; Herf, M.; Phillips, A.J.; Wright, K.P.; Skene, D.J.; Brainard, G.C.; Boivin, D.B.; Glickman, G. A Review of Human Physiological Responses to Light: Implications for the Development of Integrative Lighting Solutions. Leukos 2021, 1–28. [Google Scholar] [CrossRef]
- Milner, C.E.; Cote, K.A. Benefits of napping in healthy adults: Impact of nap length, time of day, age, and experience with napping. J. Sleep Res. 2009, 18, 272–281. [Google Scholar] [CrossRef]
- Borbély, A.A. A two process model of sleep regulation. Hum. Neurobiol. 1982, 1, 195–204. [Google Scholar]
- Vetter, C.; Phillips, A.J.; Silva, A.; Lockley, S.W.; Glickman, G. Light me up? Why, when, and how much light we need. J. Biol. Rhythm. 2019, 34, 573–575. [Google Scholar] [CrossRef]
- Carskadon, M.A.; Dement, W.C. Normal human sleep: An overview. Princ. Pract. Sleep Med. 2005, 4, 13–23. [Google Scholar]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Sack, R.L. Jet lag. N. Engl. J. Med. 2010, 362, 440–447. [Google Scholar] [CrossRef]
- Keystone, J.S.; Steffen, R.; Kozarsky, P.E. Health advice for international travel. In Tropical Infectious Diseases: Principles, Pathogens and Practice; Elsevier: Amsterdam, The Netherlands, 2011; pp. 887–901. [Google Scholar]
- Sack, R.L.; Auckley, D.; Auger, R.R.; Carskadon, M.A.; Wright, K.P., Jr.; Vitiello, M.V.; Zhdanova, I.V. Circadian rhythm sleep disorders: Part I, basic principles, shift work and jet lag disorders. Sleep 2007, 30, 1460–1483. [Google Scholar] [CrossRef] [PubMed]
- Morgenthaler, T.I.; Lee-Chiong, T.; Alessi, C.; Friedman, L.; Aurora, R.N.; Boehlecke, B.; Brown, T.; Chesson, A.L., Jr.; Kapur, V.; Maganti, R. Practice parameters for the clinical evaluation and treatment of circadian rhythm sleep disorders. Sleep 2007, 30, 1445–1459. [Google Scholar] [CrossRef] [PubMed]
- Harrison, E.M.; Schmied, E.A.; Yablonsky, A.M.; Glickman, G.L. Implementation of interventions designed to promote healthy sleep and circadian rhythms in shiftworkers. Chronobiol. Int. 2021, 38, 467–479. [Google Scholar] [CrossRef] [PubMed]
- Capaldi, V.F.; Kim, J.R.; Grillakis, A.A.; Taylor, M.R.; York, C.M. Insomnia in the military: Application and effectiveness of cognitive and pharmacologic therapies. Curr. Psychiatry Rep. 2015, 17, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Schmied, E.A.; Martin, R.M.; Harrison, E.M.; Perez, V.G.; Thomsen, C.J. Studying the Health and Performance of Shipboard Sailors: An Evidence Map. Mil. Med. 2021, 186, e512–e524. [Google Scholar] [CrossRef]
- Russell, D.W.; Markwald, R.R.; Jameson, J.T. Self-reported sleep and sleep deficiency: Results from a large initiative of sailors attached to US Navy warships. J. Sleep Res. 2021, 30, e13397. [Google Scholar] [CrossRef]
- Parthasarathy, S.; Carskadon, M.A.; Jean-Louis, G.; Owens, J.; Bramoweth, A.; Combs, D.; Hale, L.; Harrison, E.; Hart, C.N.; Hasler, B.P.; et al. Implementation of Sleep and Circadian Science: Recommendations from the Sleep Research Society and National Institutes of Health Workshop. Sleep 2016, 39, 2061–2075. [Google Scholar] [CrossRef]
- Hoddinott, P. A new era for intervention development studies. Pilot Feasibility Stud. 2015, 1, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Arnedt, J.T.; Cuddihy, L.; Swanson, L.M.; Pickett, S.; Aikens, J.; Chervin, R.D. Randomized controlled trial of telephone-delivered cognitive behavioral therapy for chronic insomnia. Sleep 2013, 36, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Filion, A.J.; Darlington, G.; Chaput, J.P.; Ybarra, M.; Haines, J. Examining the influence of a text message-based sleep and physical activity intervention among young adult smokers in the United States. BMC Public Health 2015, 15, 671. [Google Scholar] [CrossRef] [PubMed]
- Gunia, B.C.; Sipos, M.L.; LoPresti, M.; Adler, A.B. Sleep leadership in high-risk occupations: An investigation of soldiers on peacekeeping and combat missions. Mil. Psychocol. 2015, 27, 197–211. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n (%) |
|---|---|
| Gender | |
| Male Female | 49 (89.1) 6 (10.9) |
| Age 17–24 25–29 30–39 40+ | 3 (5.5) 15 (27.3) 32 (58.2) 5 (9.1) |
| Race/ethnicity White Black Hispanic Asian Other/multiple | 26 (47.3) 9 (16.4) 10 (18.2) 3 (5.5) 7 (12.7) |
| Marital status Married/cohabitating Divorced/widowed Never married | 31 (56.4) 7 (12.7) 17 (30.9) |
| Paygrade/rank 1 E1–E3 E4–E6 E7–E9 Officer | 2 (3.6) 25 (45.5) 18 (32.7) 10 (18.2) |
| Education High school Some college Two-year degree Four-year degree or higher | 19 (34.5) 11 (20.0) 9 (16.4) 16 (29.1) |
| Questions | Answers | T1 % Correct | T2 % Correct |
|---|---|---|---|
| The two primary regulators of sleep include the ____ and ____ systems. | a. Circadian and homeostatic [63]. | 61.1 | 96.3 *** |
| b. Circadian and vestibular. | |||
| c. Homeostatic and vestibular. | |||
| d. Vestibular and visual. | |||
| In order to optimize sleep and circadian health, short wavelength (blue) light: | a. Is an important signal of day during active periods [64]. | 20.4 | 79.6 *** |
| b. Helps you to fall asleep when used close to bedtime. | |||
| c. Should be avoided at all costs. | |||
| d. Is meaningless. All wavelengths/colors of light affect our biology in the same way. | |||
| Which of the following stages of sleep occurs more often in the second half of an eight-hour sleep episode? | a. NREM. | ||
| b. REM [65]. | 68.5 | 88.9 ** | |
| c. Both, NREM and REM increase over the course of the sleep episode. | |||
| d. Neither, NREM and REM decrease over the course of the sleep episode. | |||
| How many hours of sleep per night are recommended for adults? Between ____ and ____ hours | 7–9 [16,66]. (7–8 and 8–9 also accepted). | 16.7 | 81.5 *** |
| If you are feeling sleepy, and then you go outside into the sunshine for half an hour, what might you expect to feel? | a. More sleepy. | ||
| b. Less sleepy [57]. | 70.4 | 98.2 *** | |
| c. No difference. | |||
| Approximately how long does it take your circadian system to adjust when you change your light schedule by three hours (by flying from one U.S. coast to the other)? | a. It adjusts immediately. | ||
| b. One day. | |||
| c. Three days [64]. | 40.7 | 74.1 *** | |
| d. One week. | |||
| e. Three weeks. | |||
| If you are trying to adjust to a new timezone, when during the “new” day is it most important for you to get bright light? | a. In the “new” morning * [67,68]. | 77.8 | 94.4 * |
| b. In the “new” afternoon. | |||
| c. In the “new” evening. | |||
| d. In the “new” night. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harrison, E.M.; Schmied, E.A.; Hurtado, S.L.; Easterling, A.P.; Glickman, G.L. The Development, Implementation, and Feasibility of a Circadian, Light, and Sleep Skills Program for Shipboard Military Personnel (CLASS-SM). Int. J. Environ. Res. Public Health 2022, 19, 3093. https://doi.org/10.3390/ijerph19053093
Harrison EM, Schmied EA, Hurtado SL, Easterling AP, Glickman GL. The Development, Implementation, and Feasibility of a Circadian, Light, and Sleep Skills Program for Shipboard Military Personnel (CLASS-SM). International Journal of Environmental Research and Public Health. 2022; 19(5):3093. https://doi.org/10.3390/ijerph19053093
Chicago/Turabian StyleHarrison, Elizabeth M., Emily A. Schmied, Suzanne L. Hurtado, Alexandra P. Easterling, and Gena L. Glickman. 2022. "The Development, Implementation, and Feasibility of a Circadian, Light, and Sleep Skills Program for Shipboard Military Personnel (CLASS-SM)" International Journal of Environmental Research and Public Health 19, no. 5: 3093. https://doi.org/10.3390/ijerph19053093
APA StyleHarrison, E. M., Schmied, E. A., Hurtado, S. L., Easterling, A. P., & Glickman, G. L. (2022). The Development, Implementation, and Feasibility of a Circadian, Light, and Sleep Skills Program for Shipboard Military Personnel (CLASS-SM). International Journal of Environmental Research and Public Health, 19(5), 3093. https://doi.org/10.3390/ijerph19053093