Abstract
Sexual violence (SV) has an important impact on mental health. Childhood sexual abuse is linked to internalising disorders in later life. In older adults, SV occurs more often than previously believed. Moreover, health care workers lack the skills to address SV in later life. Studies researching the mental health impact of lifetime SV, i.e., SV during childhood, adulthood, and old age, are lacking. Between July 2019 and March 2020, 513 older adults living in Belgium participated in structured face-to-face-interviews. Selection occurred via a cluster random probability sampling with a random walk finding approach. Depression, anxiety, and posttraumatic stress syndrome (PTSD) were measured using validated scales. Participants were asked about suicide attempts and self-harm during their lifetime and in the past 12 months. SV was measured using behaviourally specific questions based on a broad SV definition. We found rates for depression, anxiety, and PTSD of 27%, 26%, and 6% respectively, while 2% had attempted suicide, and 1% reported self-harm in the past 12 months. Over 44% experienced lifetime SV and 8% in the past 12 months. Lifetime SV was linked to depression (p = 0.001), anxiety (p = 0.001), and PTSD in participants with a chronic illness/disability (p = 0.002) or no/lower education (p < 0.001). We found no link between lifetime SV and suicide attempts or self-harm in the past 12 months. In conclusion, lifetime SV is linked to mental health problems in late life. Tailored mental health care for older SV victims is necessary. Therefore, capacity building of professionals and development of clinical guidelines and care procedures are important.
1. Introduction
Sexual violence (SV) [1] is increasingly considered an important public health problem of major societal concern [2]. In older adults, SV has been studied in the broader context of elder abuse and neglect for many years. Moreover, most studies only included hands-on SV (e.g., unwanted kissing, rape), whereas hands-off SV (sexual harassment without physical contact) was not studied. Therefore, prevalence numbers have been underestimated for a long time [3]. A recent study, which assessed SV independently from other forms of violence and used a broad definition of SV encompassing both hands-off and hands-on SV, showed that SV in older adults occurs more frequently than previously believed [4].
In older adults, mental health problems are common and lead to impaired functioning in daily life [5]. Research has shown that up to one in three older adults reports depressive symptoms [6], and up to 14% suffers from an anxiety disorder [7] and 3% from PTSD [8]. Furthermore, older adults complete suicide proportionally more often than any other age group [9]. Physical and verbal abuse against older adults have been associated with adverse mental health outcomes [10]. When it comes to SV, studies tend to focus only on the long-term mental health outcomes of child sexual abuse (CSA), indicating that CSA victims suffer more from internalising disorders in later life [11,12]. However, studies taking a life-course perspective and researching the mental health impact of lifetime sexual victimisation, including SV that happened during childhood, adulthood, and old age, are currently lacking. Several risk factors have been associated with both elder abuse and neglect and adverse mental health outcomes in late life, such as being female, increasing age, low education level, financial difficulties, suffering from a chronic illness or disability, being care dependent, low social support, and lacking resilience [7,8,9,13,14]. Both being resilient and having a high level of social support have already shown to decrease the mental health impact of sexual victimisation in younger populations [15,16,17,18]. Moreover, identifying as non-heterosexual has been associated specifically with SV in older adults and has also been linked to mental health problems in older age [4,19]. Additionally, a recent study showed that sexual victimisation remains largely undetected by mental health care workers [20]. Although the World Psychiatric Association (WPA) petitioned a routine inquiry on SV in all psychiatric assessments [21], health care workers lack the appropriate communication skills to adequately address SV in later life. They are worried that talking about SV will break down the victims’ defence mechanisms and that they will feel shocked and helpless when confronted with SV disclosure by older victims [22].
In order to provide tailored care to older victims of SV, a better understanding of the mental health impact of lifetime sexual victimisation is needed. To our knowledge, this study is the first to assess the impact of lifetime sexual victimisation on mental health outcomes in a representative sample of older adults. We used a broad definition of SV and included sexual victimisation across the life course, including SV that happened during childhood, adulthood, and old age. This study was a part of the first gender- and age-sensitive SV prevalence study in Belgium, which aimed for a better understanding of the mechanisms, nature, magnitude, and impact of SV [23]. The objectives of this paper are three-fold: (1) to establish the prevalence of depression, anxiety, PTSD, suicide attempts, and self-harm and its moderators in older adults in Belgium; (2) to research whether lifetime sexual victimisation is associated with depression, anxiety, PTSD, suicide attempts, and self-harm in older adults; (3) to test the moderating effect of the previous identified moderators of elder abuse and neglect, SV, and mental health problems (i.e., past 12-months SV, sociodemographic characteristics, health status, social support, and resilience) in the relationship between lifetime sexual victimisation and depression, anxiety, and PTSD in older adults. Based on our results, we formulate recommendations for future research and health care practices.
2. Materials and Methods
2.1. Sample Selection
Between 8 July 2019 and 12 March 2020, a representative sample of the Belgian older population participated in a structured face-to-face interview. Participants were selected using a cluster random probability sampling with a random walk finding approach [24]. They had to live in Belgium; speak Dutch, French, or English; be at least 70 years old; and have sufficient cognitive ability to complete the interview. Cognitive status was not formally tested, but it was assessed based on the ability to maintain attention during the interview and the consistency of the participant’s answers, by means of a control question comparing the participant’s birth year and age. Structured face-to-face interviews were carried out in private at the participant’s place of residence by trained interviewers. Both older adults living in the community and living in nursing homes or assisted living facilities were included. In total, 513 interviews were included in the analysis. Participation rate was 34%. The full study protocol is available elsewhere [24].
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. The study received ethical approval from the ethical committee of Ghent University/University Hospital (B670201837542) and was conducted according to the WHO ethical and safety recommendations for SV research [25]. As recommended by these guidelines, the study was presented as the “Belgian study on health, sexuality and well-being.” Written informed consent was obtained from all participants. After participation, participants received a brochure with the contact details of several helplines.
2.2. Definitions and Measures
This study was a part of a national SV prevalence study in the Belgian population between 16 and 100 years old [23]. The questionnaire consisted of several modules, including sociodemographic characteristics, sexual health and relations, mental health, and sexual victimisation. The questions in these modules were identical across all age groups.
Mental health was measured using international scales, which were validated in several age groups. Depression was measured using the Patient Health Questionnaire (PHQ)-9 (Cronbach’s alpha (α) = 0.737) [26] and anxiety using the General Anxiety Disorder (GAD)-7 (α = 0.827) [27]. Both scales assessed symptoms in the two weeks before the interview. PTSD was assessed with the Primary Care PTSD Screen for DSM-5 (PC-PTSD-5) (α = 0.572) [28], which questioned symptoms in the month before the interview. Resilience was estimated using the Brief Resilience Scale (BRS) (α = 0.821) [29]. Additionally, participants were asked about self-harm and suicide attempts both during their lifetime and in the past 12 months. Social support was measured by number of confidants.
SV was defined according to the WHO definition, which encompasses different forms of sexual harassment without physical contact, sexual abuse with physical contact but without penetration, and (attempted) rape [1]. As a result of recent insights in the field of SV in older adults, this definition was expanded to include sexual neglect [3], which was measured as “touching in care” due to the absence of a standardised measure (See Appendix A). We used behaviourally specific questions (BSQ) to assess lifetime and past 12-month SV experiences. The SV items were based on existing surveys [30,31,32] and adapted to the Belgian social and legal context [33]. To calculate lifetime and past 12-month sexual victimisation, we created dichotomous variables out of all 17 SV items. Due to a high level of multicollinearity between hands-off and hands-on SV (Variance Inflation Factor (VIF) > 4) [34], they were not added separately in the analyses but were combined into the variables lifetime and past 12-month SV. Lifetime SV is defined as exposure to any of the 17 SV items (Yes/No) provided in Appendix A during the lifetime of the participant (age 0 till time of the survey).
2.3. Statistical Analysis
Statistical analysis was performed using SPSS Statistics 26 [35] and R version 3.6.3 [36]. Descriptive statistics (means, standard deviations, and percentages) were calculated for all variables. Outcome variables were described in a categorical way, as this is how the scales are used in clinical practice. We conducted a bivariate analysis to compare the proportion of sexual victimisation within the different categories of depression, anxiety, and PTSD using a chi-square test or a Fisher’s exact test if the assumptions of the chi-square test were not met.
To assess the association between lifetime sexual victimisation and depression, anxiety, and PTSD, we performed stepwise linear regression analyses for each outcome variable separately. In each model, we used the score on the PHQ-9, the GAD-7, and the PC-PTSD-5 scale as a continuous outcome variable. The assumption of normally distributed residuals was checked through a Q-Q plot and a histogram (see Appendix B). Moreover, the kurtosis (<5) and skewness (<2) were checked for all outcome variables and were considered acceptable [37,38]. In each analysis, main effects were added and/or deleted stepwise based on selection criteria (p < 0.05). The multi-collinearity assumption of multivariate regression analyses was tested for the main effects with the VIF and indicated no violation. Given the low numbers for suicide attempts and self-harm in the past 12 months, we did not perform a regression analysis on these variables. We constructed cross-product terms to further explore the moderating effects of past 12-month SV, sex at birth, age, sexual orientation, resilience, education level, perceived health status, care dependency, and social support in the relationship between lifetime sexual victimisation and depression, anxiety, or PTSD. The potential moderators were dichotomised. Continuous variables were dichotomised based on the mean value. Afterwards, cross-product terms were created between each of the binary moderators and lifetime SV. Again, stepwise linear regression analyses were conducted. In each analysis, the cross-product terms were added and/or deleted stepwise together with their main effects based on selection criteria (p < 0.10). Interactions were further explored if p < 0.10 to account for possible underpowering of the sample. In that case, separate regression analyses were run to further analyse the interaction effect (e.g., separate analyses for higher versus no/lower education). In the final model, only significant (p < 0.05) main effects and interaction effects were retained. p-values, coefficients, and 95% confidence intervals (CI) are presented.
3. Results
3.1. Descriptive Statistics
The study sample consisted of a representative sample of the Belgian population aged 70 years and older (n = 513) [24]. The mean age was 79 years (SD: 6.4 yrs, range 70–99 yrs), 58.3% was female, 7.4% identified themselves as non-heterosexual, 89.8% was community-dwelling, 31.2% had completed higher education, 26.1% labelled their financial situation as difficult, and 48.3% reported low social support. Regarding health status, 45.8% indicated that they suffered from an illness or disability limiting their daily activities, 46.4% was care-dependent, and 26.5% reported low resilience. Over 44% of the participants experienced SV during their lifetime and 8.4% in the past 12 months. A detailed description of the different forms of sexual victimisation has been published elsewhere [4]. More information on the characteristics of the study sample can be found in Table 1.

Table 1.
Descriptive statistics of sociodemographic characteristics, health status, social support, resilience, and sexual victimisation (n = 513).
Regarding mental health status (see Table 2), 19.9% reported mild, 5.1% moderate, and 2.5% severe depressive symptoms; and 17.5% mild, 4.5% moderate, and 3.5% severe anxiety symptoms during the two weeks prior to the interview. During the month prior to the interview, 5.7% suffered from symptoms of PTSD. We found a significant difference in level of depression, anxiety, and PTSD between SV victims and non-victims (p < 0.05). Over 5% attempted suicide during their lifetime and 1.6% in the past 12 months; 2.1% reported self-harm during their lifetime and 1.4% in the past 12 months. For both suicide attempts and self-harm, we found no significant difference between SV victims and non-victims.
Table 2.
Descriptive statistics of depression, anxiety, PTSD, suicide attempts, self-harm, and sexual victimisation.
3.2. Association between Lifetime SV and Depression, Anxiety, and PTSD
The linear regression analysis (Table 3) showed that having experienced lifetime SV, financial difficulties, having a chronic illness or disability limiting daily activities, being care dependent, and having fewer than three confidants were associated with depression in old age. Exposure to SV in the past 12 months, sex at birth, age, sexual orientation, education level, and resilience were not associated with depression in our sample. Anxiety was associated with lifetime exposure to SV, a higher education, financial difficulties, a chronic illness or disability limiting daily activities, being care dependent, fewer than three confidants, and low resilience. Exposure to SV in the past 12 months, sex at birth, age, and sexual orientation were not associated with anxiety in our sample. Financial difficulties were associated with PTSD. Lifetime SV was only associated with PTSD in respondents with a chronic illness/disability or no/lower education. Exposure to SV in the past 12 months, sex at birth, age, sexual orientation, care dependency, social support, and resilience were not associated with PTSD in our sample.
Table 3.
Association of lifetime sexual victimization with depression, anxiety, and PTSD.
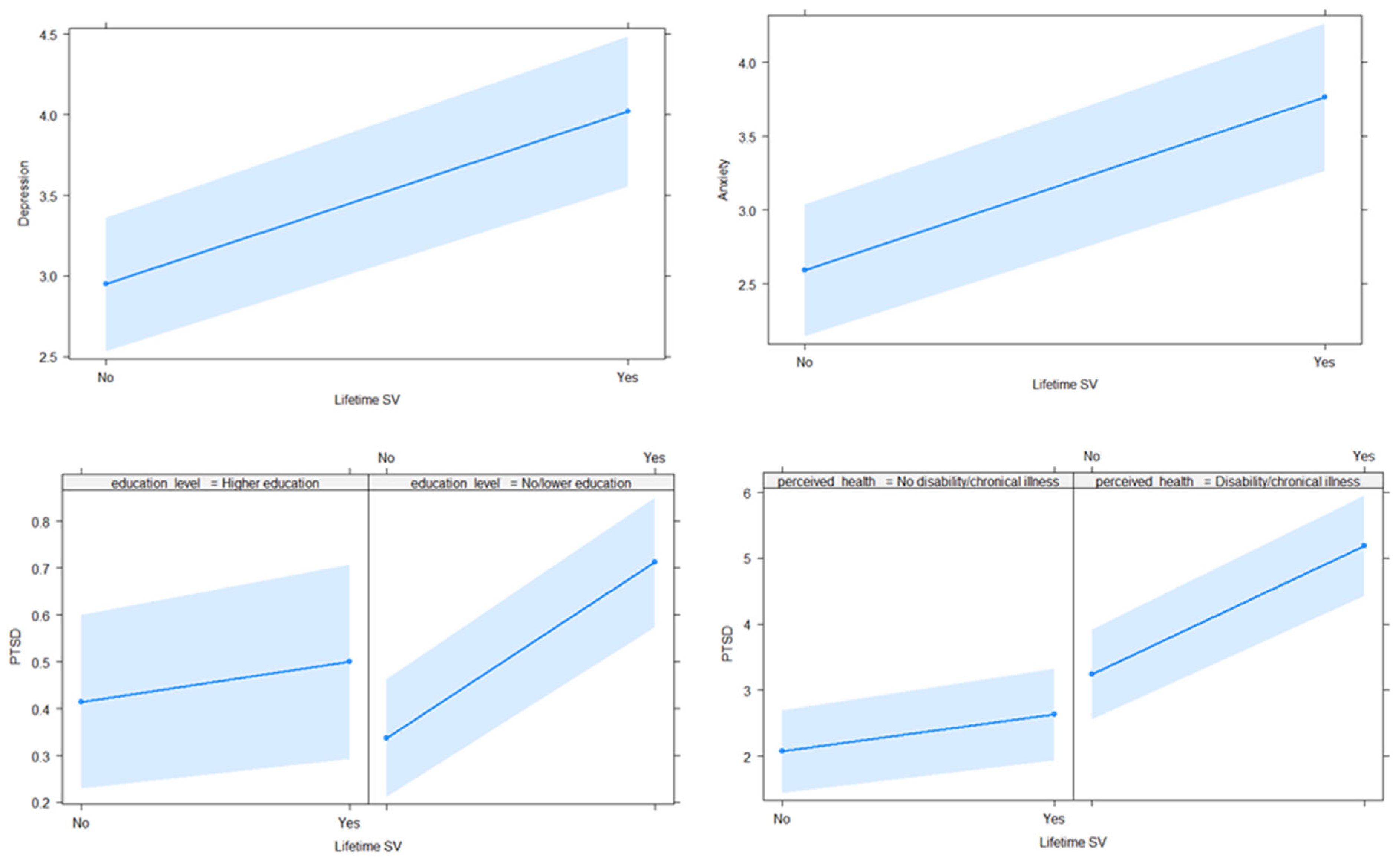
The direction of the association between lifetime SV, depression, and anxiety are shown in the first two graphs of Figure 1. The last two graphs show the interaction effect between lifetime SV and education level and between lifetime SV and perceived health status in the case of PTSD.
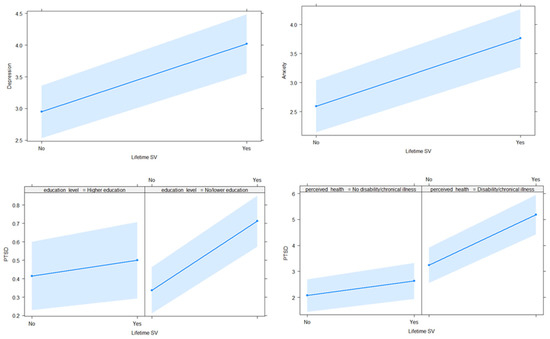
Figure 1.
Association between lifetime sexual victimisation and depression, anxiety, and PTSD.
4. Discussion
In this paper, we present the results of a study on the mental health impact of sexual victimisation in a representative sample of 513 older adults living in Belgium. We established the prevalence of depression, anxiety, PTSD, suicide attempts, and self-harm in the Belgian population of 70 years and older. Moreover, we studied the association between lifetime sexual victimisation and depression, anxiety, PTSD, suicide attempts, and self-harm in later life. Furthermore, we examined the moderating effects of sexual victimisation in the past 12 months, sociodemographic characteristics, health status, social support, and resilience in the relationship between lifetime sexual victimisation and depression, anxiety, and PTSD.
4.1. Mental Health Problems Are Common in Older Adults in Belgium
Our results confirm that mental health problems are common in older adults [5]. Almost 20% of participants reported mild depressive symptoms, 5.1% reported moderate depressive symptoms, and 2.5% suffered from severe depressive symptoms. Over 17% reported mild, 4.5% moderate, and 3.5% severe anxiety symptoms, and 5.7% suffered from PTSD. Previous studies found similar numbers regarding depression and anxiety [6,7] but lower prevalence numbers for PTSD compared to our study [8]. However, our PTSD prevalence numbers even seem underestimated, as some studies indicate subclinical ranges of PTSD in older adults up to 17% [39]. Several studies have shown that different symptoms clusters may exist between younger and older adults with PTSD. Older adults may report more somatic and affective complaints [39,40], which are not questioned in the PC-PTSD-5, the PTSD measurement instrument used in our study. Moreover, the use of different definitions and measurement instruments makes comparing PTSD prevalence rates between studies difficult. While previous studies defined PTSD according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV), we used the DSM-5 PTSD criteria, which could influence prevalence rates. Although studies in younger populations showed no difference in prevalence rates when using the DSM-IV versus the DSM-5 criteria [41,42], this has not yet been researched in older adults. Additionally, studies using the DSM-5 criteria use different measurement instruments, such as the Clinician-Administered PTSD scale for DSM-5 (CAPS-5) [43], the PTSD Checklist for DSM-5 (PCL-5) [44], or the PC-PTSD-5 [28]. This complicates the comparison of PTSD prevalence rates between different studies using the same DSM-5 definition. Therefore, more research comparing different measurement instruments and their validity in older adults is needed. Regarding suicide attempts and self-harm, we found that 1.6% of our study population reported a suicide attempt and 1.4% self-harm in the past 12 months. Similar rates were found by the Flemish Centre for Suicide Prevention (VLESP) in the same period [45]. Although our results and previous research shows low numbers for suicide attempts and self-harm, it is known that older adults complete suicide proportionally more than any other age group [9,45]. However, information on SV and mental health of older adults who completed suicide were not available in our study.
In addition to the high prevalence of mental health disorders, our study confirms previous findings indicating that financial difficulties, suffering from a chronic illness or disability, being care dependent, and having low social support are associated with adverse mental health outcomes in later life [7,9,46]. Therefore, we endorse previous calls to invest in psychosocial interventions that combat isolation in older adults, including befriending programmes and peer support schemes [47]. Although previous studies link a low education level to adverse mental health outcomes in later life [7,9,46], our study shows mixed results. In our sample, older adults with a low education level showed fewer anxiety symptoms compared to highly educated older adults. For depression and PTSD, we found no link between education level and symptom severity. Concerning resilience, our results show that resilient older adults report fewer anxiety symptoms. Whereas previous studies indicated a link between resilience and depressive symptoms in older adults [47], we found no association in our sample. Since the definition and measurement of resilience continues to be the subject of debate [48], and new scales for resilience in older adults were developed and tested very recently [49], the different results could possibly be explained by different measurement instruments. More research comparing the reliability of different measurement instruments for resilience in older adults is needed to draw conclusions concerning its moderating effect on mental health outcomes in later life.
4.2. Lifetime Sexual Victimisation Is Linked with Depression, Anxiety, and PTSD in Older Adults
The second objective of this paper was to check whether lifetime sexual victimisation was associated with depression, anxiety, PTSD, suicide attempts, and self-harm in late life. Both the bivariate and the regression analysis showed an association between lifetime sexual victimisation and current depression and anxiety in old age. For PTSD, we found an association in respondents with a chronic illness/disability or no/lower education. Lifetime sexual victimisation and suicide attempts or self-harm in the past 12 months were not significantly associated. This could be due to the low prevalence rates for suicide-attempts and self-harm limiting the power of our analysis. As discussed earlier, studies show low numbers of suicide attempts in older adults [45]. Since sexual victimisation is a known risk factor for suicide attempts, and older adults are more likely to die after a suicide attempt [9,45], we can partly assume that we could not establish a link between sexual victimisation and suicide attempts in our sample since possible victims might have died by suicide.
4.3. Past 12-Month Sexual Violence, Social Support, and Resilience Do Not Moderate the Relationship between Lifetime Sexual Victimisation and Depression, Anxiety, and PTSD
Thirdly, this paper examined the moderating effect of past 12-month SV, sociodemographic characteristics, health status, social support, and resilience in the relationship between lifetime sexual victimisation and depression, anxiety, and PTSD in older adults. In our sample, past 12-month SV did not moderate the relation between lifetime sexual victimisation and any of the mental health outcomes, suggesting that exposure to SV earlier in life had such an important impact on the victims’ mental health that the impact of a recent SV event made no difference. Regarding sociodemographic characteristics, we found a moderating effect of education level on the relationship between lifetime sexual victimisation and PTSD. Similarly, health status moderates the relationship between lifetime sexual victimisation and PTSD. Although previous research found that social support in the acute phase after exposure to SV is crucial to decrease adverse mental health outcomes [15,16], our study indicated that social support does not influence long-term mental health outcomes after SV. We assume this could be explained by the limited help-seeking behaviour of older adults upon sexual victimisation. Recent research has shown that 60% of older SV victims never disclosed their experiences to their informal network, and 94% never sought professional help [50]. Similar to younger victims [51], older SV victims experience many barriers to disclose SV experiences or seek professional help [20,50]. We hypothesize that social support is only beneficial for long-term mental health outcomes following sexual victimisation when the confidants are aware of the victim’s SV history. More research on the interaction between social support, SV disclosure, and mental health outcomes in older adults is needed to confirm this hypothesis. Furthermore, resilience did not moderate the effect between lifetime sexual victimisation and depression, anxiety, and PTSD in our sample. Previous studies on the effect of resilience showed mixed results. Some found that resilient subjects may be partly protected against the long-term mental health effect of SV [17], but others could not establish high resilience as a protective factor against adverse mental health outcomes after SV [18]. More research on the association between sexual victimisation and resilience on mental health outcomes in older adults is warranted to clarify this.
4.4. Limitations
Our study has several limitations. First, our study applied a cross-sectional design, which makes it impossible to establish a causal relation between sexual victimisation and mental health outcomes in later life. Although a longitudinal study described an association between childhood sexual abuse and internalising disorders in old age [12], another study has shown that people with severe mental illness (SMI) experience substantially more SV during their lifetime compared to those who do not suffer from SMI [52]. Second, sexual victimisation was reported retrospectively by the participants. Although there is evidence that the magnitude of associations with mental disorders does not differ according to whether sexual victimisation was reported prospectively or retrospectively [53], evidence from a prospective study would further strengthen our conclusions. Third, we applied a broad definition of SV, including both hands-off and hands-on SV. One might assume that different forms of SV might have a different mental health impact. However, due to a high level of multicollinearity between hands-off and hands-on SV (VIF > 4) [34], our study was not able to differentiate between the mental health impact of lifetime hands-off versus hands-on SV. Fourth, although several studies have indicated that the age of first exposure to different types of violence, including SV, may be associated to differential risks of various mental health outcomes [54,55,56], our study does not distinguish between lifetime sexual victimisation during childhood and adulthood. We recommend future studies to add a follow-up question in the SV module regarding the age of first SV exposure. This would allow us to differentiate the mental health impact of SV exposure during childhood and adulthood. Finally, seeking (in)formal help upon sexual victimisation was not included as a confounding variable in our model. Although seeking (in)formal help might have a positive effect on long-term mental health outcomes following SV, research has shown that very few older SV victims had disclosed their experiences or sought professional help [50]. Therefore, we assume a limited impact of help-seeking upon SV on mental health outcomes in old age.
4.5. Recommendations for Future Research and Clinical Practice
Despite its limitations, this study improves the current understanding of the mental health impact of SV in older adults. Being the first to apply a life course perspective in the analysis, including sexual victimisation during childhood, adulthood and old age, and using a broad definition of SV, this study offers a unique understanding of the mental health impact of SV in late life. To strengthen our conclusions, studies using the same approach and SV definition in older adults from different countries and different cultural backgrounds are warranted. Moreover, in order to provide tailored care for older victims of SV, mental health care should be better aligned with the needs of older victims of SV. Therefore, incorporating a routine inquiry about sexual victimisation, as proposed by the WPA [21], should become the gold standard of care for older adults who present with mental health problems. However, since health care workers rarely feel comfortable discussing SV with older adults [22], capacity building for healthcare workers and the development of clinical guidelines and care procedures seem of the utmost importance.
5. Conclusions
Lifetime sexual victimisation is linked to depression and anxiety in older adults in Belgium and is associated with PTSD in older adults with a chronic illness/disability or no/lower education. Our findings confirm the long-lasting mental health impact of sexual victimisation and show the need for tailored mental health care for older victims of SV. Therefore, more research on the specific needs of older SV victims regarding mental health care is needed. In addition, professionals working with older adults urgently need capacity building regarding SV and its mental health impact. Furthermore, the development of clinical guidelines and care procedures seems particularly important.
Author Contributions
Conceptualization, A.N., G.L., M.B., C.V. and I.K.; methodology, A.N., G.L., M.B., C.V. and I.K.; training of interviewers, A.N. and I.K.; validation, A.N., G.L., L.T., M.B., C.V. and I.K.; formal analysis, A.N. and L.T.; investigation, A.N.; writing—original draft preparation, A.N.; writing—review and editing, G.L., L.T., M.B., C.V. and I.K.; supervision, G.L., C.V. and I.K.; project administration and coordination: I.K.; funding acquisition, C.V. and I.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was predominantly supported by the Belgian Federal Science Policy Belgian Research Action through the Interdisciplinary Networks funding scheme, grant number BR/175/A5/UN-MENAMAIS. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Ghent University/University Hospital (B670201837542) on the 16 November 2018.
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
By request from the corresponding author.
Acknowledgments
The authors want to thank Adina Cismaru-Inescu, Lotte De Schrijver, Joke Depraetere, and Laurent Nisen for their input during the questionnaire development. In addition, we want to thank Adina Cismaru-Inescu, Bastien Hahaut, and Laurent Nisen for their support during the data-collection process. Many thanks to our interviewers for their time and dedication to our study, Elizaveta Fomenko for her statistical advice, and Howard Ryland for his help with the language editing. Finally, we want to thank all older adults who participated in our study for sharing their stories with us.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| α | Cronbach’s alpha |
| BRS | Brief Resilience Scale |
| BSQ | Behavioural Specific Questions |
| CAPS-5 | Clinician-Administered PTSD scale for DSM-5 |
| CI | Confidence Interval |
| CSA | Child Sexual Abuse |
| DSM-IV | Diagnostic and Statistical Manual of Mental Disorders, fourth edition |
| DSM-5 | Diagnostic and Statistical Manual of Mental Disorders, fifth edition |
| GAD-7 | General Anxiety Disorder- 7 |
| PCL-5 | PTSD Checklist for DSM-5 |
| PC-PTSD-5 | Primary Care PTSD Screen for DSM-5 |
| PHQ-9 | Patient Health Questionnaire-9 |
| PTSD | Post-Traumatic Stress Disorder |
| SMI | Severe Mental Illness |
| SV | Sexual Violence |
| VIF | Variance Inflation factor |
| VLESP | Vlaamse Expertisecentrum Suïcidepreventie/Flemish Centre for Suicide Prevention |
| WHO | World Health Organization |
| WPA | World Psychiatric Association |
Appendix A. Detailed Outcome Measurements Sexual Victimization
Hands-Off Sexual Victimisation (No Physical Contact)
- Sexual staring: Someone stared at me in a sexual way or looked at my intimate body parts (e.g., breasts, vagina, penis, anus) when I didn’t want it to happen.
- Sexual innuendo: Someone made teasing comments of a sexual nature about my body or appearance even though I didn’t want it to happen.
- Showing sexual images: Someone showed me sexual or obscene materials, such as pictures or videos, directly or over the internet (including email, social networks, and chat platforms), even though I didn’t want to look at them. This does not include mass mailings or spam.
- Sexual calls or texts: Someone made unwelcome sexual or obscene phone calls or texts to me.
- Voyeurism: I caught someone watching me, taking photos, or filming me when I didn’t want it to happen while I was undressing, nude, or having sex.
- Distribution of sexual images: Someone distributed naked pictures or videos of me directly or over the internet (including email, social networks, and chat platforms) when I didn’t want it to happen.
- Exhibitionism: Someone showed their intimate body parts (e.g., breasts, vagina, penis, anus) to me in a sexual way and/or masturbated in front of me when I didn’t want to see it.
- Forcing to show intimate body parts: Someone made me show my intimate body parts (e.g., breasts, vagina, penis, anus) online or face-to-face when I didn’t want to do it.Hands-on sexual victimisationSexual abuse (physical contact but no penetration):
- Kissing: Someone kissed me against my will.
- Touching in care: Someone touched my intimate body parts (e.g., breasts, vagina, penis, anus) during care against my will.
- Fondling/rubbing: Someone fondled or rubbed up against my intimate body parts (e.g., breasts, vagina, penis, anus) against my will.
- Forced undressing: Someone removed (some of) my clothes against my will.Rape and attempted rape (physical contact with attempted or completed penetration):
- Oral penetration: Someone had oral sex with me or made me give oral sex against my will.
- Attempt of oral penetration: Someone tried but did not succeed to have oral sex with me or tried to make me give oral sex against my will.
- Vaginal or anal penetration: Someone put their penis, finger(s), or object(s) into my vagina or anus against my will.
- Attempt of vaginal or anal penetration: Someone tried but did not succeed to put their penis, finger(s), or object(s) into my vagina or anus against my will.
- Forcing to penetrate: Someone made me put my penis, finger(s), or object(s) into their (or someone’s) vagina or anus against my will.
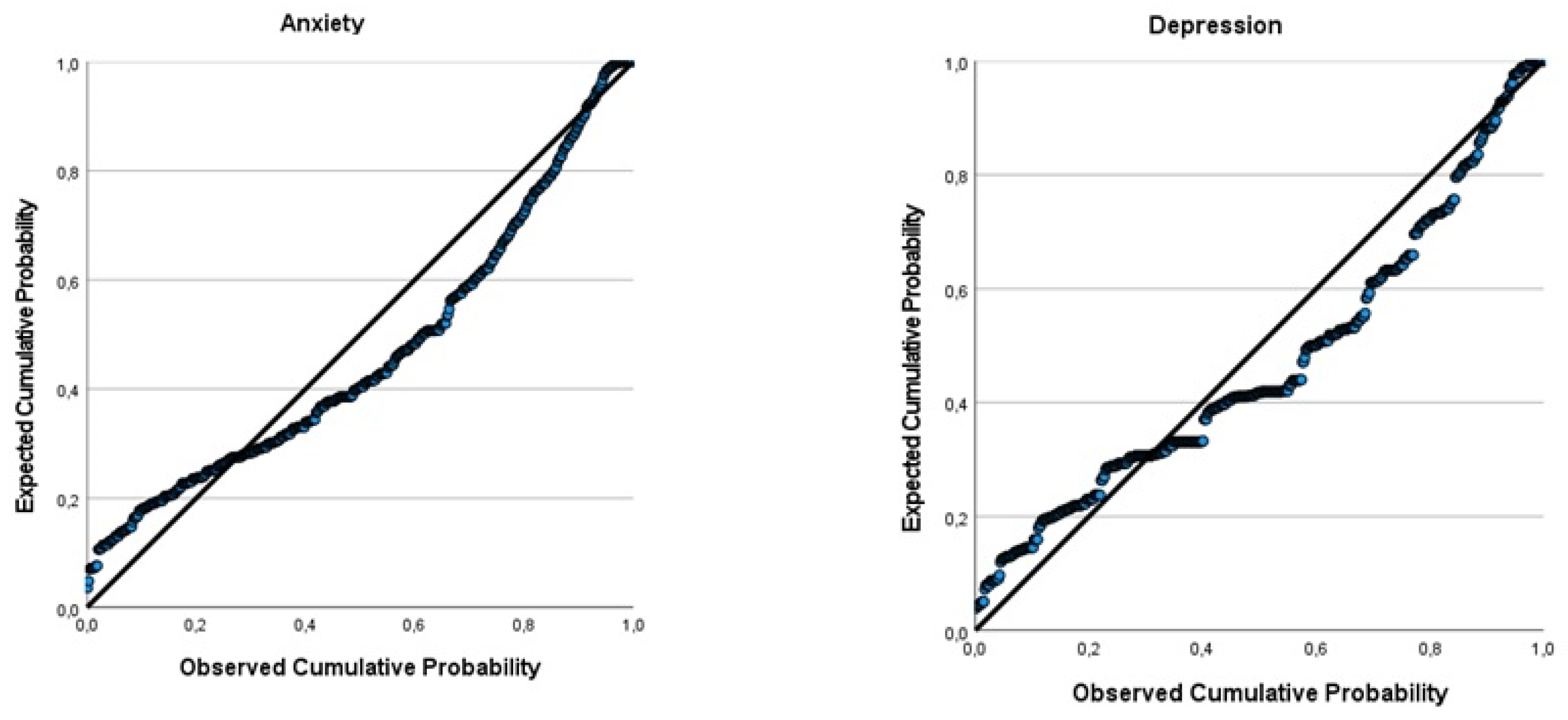
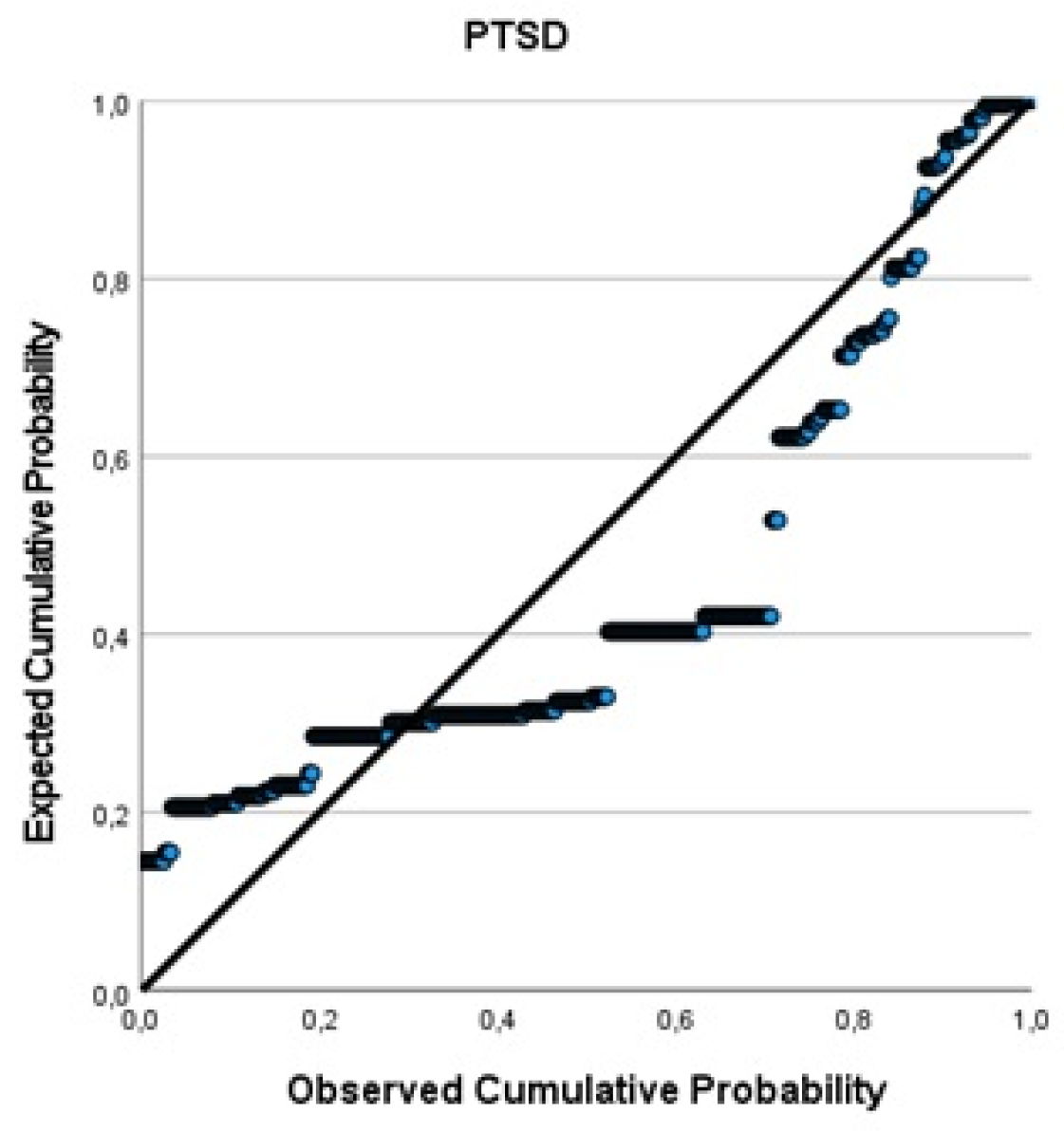
Appendix B. Q-Q Plots of the Outcome Variables of the Linear Regression Model
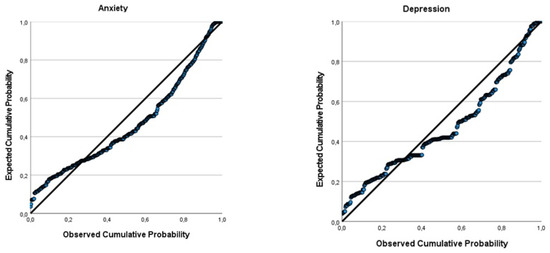

Figure A1.
Q-Q Plots of the Outcome Variables of the Linear Regression Model.
Figure A1.
Q-Q Plots of the Outcome Variables of the Linear Regression Model.
References
- World Health Organization. Violence Against Women Factsheet No. 239. 2017. Available online: http://www.who.int/mediacentre/factsheets/fs239/en/ (accessed on 4 April 2021).
- World Health Assembly. Prevention of violence: A public health priority. In Proceedings of the Forty-Ninth World Health Assembly, Geneva, Switzerland, 13 November 1996. [Google Scholar]
- Nobels, A.; Vandeviver, C.; Beaulieu, M.; Cismaru-Inescu, A.; Nisen, L.; Van Den Noortgate, N.; Vander Beken, T.; Lemmens, G.; Keygnaert, I. “Too Grey to Be True?” Sexual Violence in Older Adults: A Critical Interpretive Synthesis of Evidence. Int. J. Environ. Res. Public Health 2020, 17, 4117. [Google Scholar] [CrossRef] [PubMed]
- Nobels, A.; Cismaru-Inescu, A.; Nisen, L.; Hahaut, B.; Beaulieu, M.; Lemmens, G.; Adam, S.; Schapanksy, E.; Vandeviver, C.; Keygnaert, I. Sexual Violence in Older Adults: A Belgian Prevalence Study. BMC Geriatr. 2021, 21, 601. [Google Scholar] [CrossRef] [PubMed]
- Mental Health of Older Adults-Factsheet. 2017. Available online: https://www.who.int/newsroom/fact-sheets/detail/mental-health-of-older-adults (accessed on 30 March 2021).
- Meeks, T.W.; Vahia, I.V.; Lavretsky, H.; Kulkarni, G.; Jeste, D.V. A tune in “a minor” can “b major”: A review of epidemiology, illness course, and public health implications of subthreshold depression in older adults. J. Affect. Disord. 2011, 129, 126–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolitzky-Taylor, K.B.; Castriotta, N.; Lenze, E.J.; Stanley, M.A.; Craske, M.G. Anxiety disorders in older adults: A comprehensive review. Depress. Anxiety 2010, 27, 190–211. [Google Scholar] [CrossRef]
- Böttche, M.; Kuwert, P.; Knaevelsrud, C. Posttraumatic stress disorder in older adults: An overview of characteristics and treatment approaches. Int. J. Geriatr. Psychiatry 2012, 27, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Rodda, J.; Walker, Z.; Carter, J. Depression in older adults. BMJ 2011, 343, d5219. [Google Scholar] [CrossRef]
- Olofsson, N.; Lindqvist, K.; Danielsson, I. Fear of crime and psychological and physical abuse associated with ill health in a Swedish population aged 65–84 years. Public Health 2012, 126, 358–364. [Google Scholar] [CrossRef] [Green Version]
- Ege, M.A.; Messias, E.; Thapa, P.B.; Krain, L.P. Adverse childhood experiences and geriatric depression: Results from the 2010 BRFSS. Am. J. Geriatr. Psychiatry 2015, 23, 110–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapsey, C.M.; Scott, K.M.; Patterson, T. Childhood sexual abuse, poly-victimization and internalizing disorders across adulthood and older age: Findings from a 25-year longitudinal study. J. Affect. Disord. 2019, 244, 171–179. [Google Scholar] [CrossRef]
- Naughton, C.; Drennan, J.; Lyons, I.; Lafferty, A.; Treacy, M.; Phelan, A.; O’Loughlin, A.; Delaney, L. Elder abuse and neglect in Ireland: Results from a national prevalence survey. Age Ageing 2012, 41, 98–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luoma, M.; Koivusilta, M.; Lang, G.; Enzenhofer, E.; De Donder, L.; Verté, D.; Reingarde, J.; Tamutiene, I.; Ferreira-Alves, J.; Santos, A.J.; et al. Prevalence Study of Abuse and Violence against Older Women; Results of a Multi-Cultural Survey in Austria, Belgium, Finland, Lithuania, and Portugal (European Report of the AVOW Project); National Institute for Health and Welfare (THL): Helsinki, Finland, 2011. [Google Scholar]
- Declercq, F.; Palmans, V. Two subjective factors as moderators between critical incidents and the occurrence of post-traumatic stress disorders: Adult attachment and perception of social support. Psychol. Psychother. Theory Res. Pract. 2006, 79, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Declercq, F.; Vanheule, S.; Markey, S.; Willemsen, J. Posttraumatic distress in security guards and the various effects of social support. J. Clin. Psychol. 2007, 63, 1239–1246. [Google Scholar] [CrossRef]
- Schulz, A.; Becker, M.; Van der Auwera, S.; Barnow, S.; Appel, K.; Mahler, J.; Schmidt, C.O.; John, U.; Freyberger, H.J.; Grabe, H.J. The impact of childhood trauma on depression: Does resilience matter? Population-based results from the Study of Health in Pomerania. J. Psychosom. Res. 2014, 77, 97–103. [Google Scholar] [CrossRef]
- Fedina, L.; Nam, B.; Jun, H.-J.; Shah, R.; Von Mach, T.; Bright, C.L.; De Vylder, J. Moderating effects of resilience on depression, psychological distress, and suicidal ideation associated with interpersonal violence. J. Interpers. Violence 2021, 36, NP1335–1358NP. [Google Scholar] [CrossRef]
- Yarns, B.C.; Abrams, J.M.; Meeks, T.W.; Sewell, D.D. The Mental Health of Older LGBT Adults. Curr. Psychiatry Rep. 2016, 18, 60. [Google Scholar] [CrossRef] [PubMed]
- Nobels, A.; Keygnaert, I.; Robert, E.; Vandeviver, C.; Haekens, A.; Lemey, L.; Strobbe, M.; Van Den Noortgate, N.; Lemmens, G. ‘Breaking the silence’: Sexual victimisation in an old age psychiatry patient population in Flanders. Int. J. Geriat. Psychiatry. 2021, 36, 1550–1558. [Google Scholar] [CrossRef] [PubMed]
- Steward, E.D.; Chandra, P.S. WPA Position Paper on Intimate Partner Violence and Sexual Violence against Women: Geneva, Switerland. 2017. Available online: https://globalalliancematernalmentalhealth.org/wp-content/uploads/2018/03/WPA_position_Intimate_Partner_Violence_Sexual_Violence_Against_Women29012018.pdf (accessed on 30 June 2021).
- Goldblatt, H.; Band-Winterstein, T.; Lev, S.; Harel, D. “Who Would Sexually Assault an 80-Year-Old Woman?” Barriers to Exploring and Exposing Sexual Assault Against Women in Late Life. J. Interpers. Violence 2020, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Keygnaert, I.; Vandeviver, C.; Nisen, L.; De Schrijver, L.; Depraetere, J.; Nobels, A.; Cismaru-Inescu, A.; Lemonne, A.; Renard, B.; Vander Beken, T. Seksueel geweld in België: Eerste representatieve prevalentiestudie naar de aard, omvang en impact van seksueel geweld in België. Sci. Connect. 2018, 59, 28–31. [Google Scholar]
- Nobels, A.; Cismaru-Inescu, A.; Nisen, L.; Hahaut, B.; Lemmens, G.; Vandeviver, C.; Keygnaert, I. Challenges in conducting sexual health and violence research in older adults beyond the general data protection regulation: A Belgian case study. J. Interpers. Violence 2021, 1–21. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ethical and Safety Recommendations for Intervention Research on Violence against Women: Building on Lessons from the WHO Publication Putting Women First: Ethical and Safety Recommendations for Research on Domestic Violence against Women; WHO: Geneva, Switerland, 2016. [Google Scholar]
- Kroenke, K.; Spitzer, R.L. The PHQ-9: A new depression diagnostic and severity measure. Psychiatr. Ann. 2002, 32, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Prins, A.; Bovin, M.J.; Kimerling, R.; Kaloupek, D.G.; Marx, B.P.; Pless Kaiser, A.; Schnurr, P.P. Primary Care PTSD Screen for DSM-5 (PC-PTSD-5); National Centre for PTSD, US Department of Veteran Affairs: Washington, DC, USA, 2015.
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Koss, M.P.; Gidycz, C.A. Sexual experiences survey: Reliability and validity. J. Consult. Clin. Psychol. 1985, 53, 422–423. [Google Scholar] [CrossRef] [PubMed]
- Krahé, B.; Berger, A.; Vanwesenbeeck, I.; Bianchi, G.; Chliaoutakis, J.; Fernández-Fuertes, A.A.; Fuertes, A.; de Matos, M.G.; Hadjigeorgiou, E.; Haller, B. Prevalence and correlates of young people’s sexual aggression perpetration and victimisation in 10 European countries: A multi-level analysis. Cult. Health Sex. 2015, 17, 682–699. [Google Scholar] [CrossRef] [PubMed]
- Keygnaert, I.; Dias, S.F.; Degomme, O.; Deville, W.; Kennedy, P.; Kovats, A.; De Meyer, S.; Vettenburg, N.; Roelens, K.; Temmerman, M. Sexual and gender-based violence in the European asylum and reception sector: A perpetuum mobile? Eur. J. Public Health 2015, 25, 90–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Depraetere, J.; Cismaru-Inscu, A.; De Schrijver, L.; Nobels, A.; Keygnaert, I.; Vandeviver, C. Measuring Sexual Victimisation and Perpetration in Today’s Society: Modifications to the Sexual Experience Survey. SocArXiv 2020. [Google Scholar] [CrossRef]
- Allison, P.D. Logistic Regression Using SAS: Theory and Applications; SAS Institute: Carey, NC, USA, 2012. [Google Scholar]
- IBM Corp. IBM SPSS Statistics for Windows, Version 26.0. Armonk; IBM Corp: New York, NY, USA, 2019. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2014; Available online: http://www.R-project.org/ (accessed on 14 February 2022).
- Hair, J.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Educational International: Bergen County, NJ, USA, 2010. [Google Scholar]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming; Routledge: New York, NY, USA, 2010. [Google Scholar]
- Kaiser, A.P.; Wachen, J.S.; Potter, C.; Moye, J.; Davison, E. With the Stress, Health, and Aging Research Program (SHARP. Posttraumatic Stress Symptoms among Older Adults: A Review. PTSD: National Centre for PTSD. Available online: https://www.ptsd.va.gov/professional/treat/specific/symptoms_older_adults.asp (accessed on 7 February 2022).
- Rutherford, B.R.; Zilcha-Mano, S.; Chrisanthopolous, M.; Salzman, C.; Zhu, C.; Cimino, N.; Yehuda, R.; Neria, Y.; Roose, S.P. Symptoms profiles and treatment status of older adults with chronic post-traumatic stress disorder. Int. J. Geriatr. Psychiatry 2021, 36, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Calhoun, P.S.; Hertzberg, J.S.; Kirby, A.C.; Dennis, M.F.; Hair, L.P.; Dedert, E.A.; Beckham, J.C. The effect of draft DSM-V criteria on posttraumatic stress disorder prevalence. Depress. Anxiety 2012, 29, 1032–1042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilpatrick, D.G.; Resnick, H.S.; Milanak, M.E.; Miller, M.W.; Keyes, K.M.; Friedman, M.J. National estimates of exposure to traumatic events and PTSD prevalence using DSM-IV and DSM-5 criteria. J. Trauma. Stress 2013, 26, 537–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weathers, F.W.; Blake, D.D.; Schnurr, P.P.; Kaloupek, D.G.; Marx, B.P.; Keane, T.M. Clinician-Administered PTSD Scale for DSM-5 (CAPS-5); National Center for Posttraumatic Stress Disorder, US Department of Veteran Affairs: Washington, DC, USA, 2013.
- Weathers, F.W.; Litz, B.T.; Keane, T.M.; Palmieri, P.A.; Marx, B.P.; Schnurr, P.P. PTSSD Checklist for DSM-5 (PCL-5); National Center for Posttraumatic Stress Disorder, US Department of Veteran Affairs: Washington, DC, USA, 2013.
- Zelfmoord 1813. Zelfmoord Bij Ouderen Factsheet 2018. Available online: https://www.zelfmoord1813.be/sites/default/files/Factsheet%20Ouderen-min.pdf (accessed on 30 June 2021).
- Cole, M.G.; Dendukuri, N. Risk factors for depression among elderly community subjects: A systematic review and meta-analysis. Am. J. Psychiatry 2003, 160, 1147–1156. [Google Scholar] [CrossRef]
- Hardy, S.E.; Concato, J.; Gill, T.M. Resilience of community-Dwelling older persons. J. Am. Geriatr. Soc. 2004, 52, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Leys, C.; Arnal, C.; Wollast, R.; Rolin, H.; Kotsou, I.; Fossion, P. Perspectives on resilience: Personality trait or skill? Eur. J. Trauma Dissociation 2020, 4, 100074. [Google Scholar] [CrossRef]
- Akatsuka, E.; Tadaka, E. Development of a resilience scale for oldest-old age (RSO). BMC Geriatr. 2021, 21, 174. [Google Scholar] [CrossRef] [PubMed]
- Nobels, A.; De Schrijver, L.; Van Landuyt, M.; Vandeviver, C.; Lemmens, G.; Beaulieu, M.; Keygnaert, I. “In the end you keep silent”: Help-seeking behaviour upon sexual victimisation in older adults. Preprint 2022. [Google Scholar]
- Dartnall, E.; Jewkes, R. Sexual violence against women: The scope of the problem. Best Pract. Res. Clin. Obstet. Gynaecol. 2013, 27, 3–13. [Google Scholar] [CrossRef]
- Khalifeh, H.; Moran, P.; Borschmann, R.; Dean, K.; Hart, C.; Hogg, J.; Osborn, D.; Johnson, S.; Howard, L.M. Domestic and sexual violence against patients with severe mental illness. Psychol. Med. 2015, 45, 875–886. [Google Scholar] [CrossRef] [Green Version]
- Scott, K.M.; McLaughlin, K.A.; Smith, D.A.; Ellis, P.M. Childhood maltreatment and DSM-IV adult mental disorders: Comparison of prospective and retrospective findings. Br. J. Psychiatry 2012, 200, 469–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, E.C.; Nishimi, K.; Powers, A.; Bradley, B. Is developmental timing of trauma exposure associated with depressive and post-traumatic stress disorder symptoms in adulthood? J. Psychiatr. Res. 2017, 84, 119–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaplow, J.B.; Widom, C.S. Age of onset of child maltreatment predicts long-term mental health outcomes. J. Abnorm. Psychol. 2007, 116, 176–187. [Google Scholar] [CrossRef] [PubMed]
- Mueller-Pfeiffer, C.; Moergeli, H.; Schumacher, S.; Martin-Soelch, C.; Wirtz, G.; Fuhrhans, C.; Hindermann, E.; Rufer, M. Characteristics of child maltreatment and their relation to dissociation, posttraumatic stress symptoms, and depression in adult psychiatric patients. J. Nerv. Ment. Dis. 2013, 201, 471–477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).