
Understanding Factors to COVID-19 Vaccine Adoption in Gujarat, India



Abstract
:1. Introduction
1.1. Vaccine Hesitancy
1.2. Factors Related to Vaccine Hesitancy
1.3. Vaccination Campaign and Status in India
1.4. Setting
2. Method
3. Results
3.1. Low Uptake of Vaccines
“I already had corona once. Now, we are safe at least for three to four months. We have antibodies in our body, so we do not need to take the vaccination”.(participant 7)
“I have heard all this kind of news of vaccine inefficacy. I do have hesitancy and fear. You will not believe it; I have not even taken a test to check whether I have corona or not till today! So, forget about the vaccine”.(participant 27)
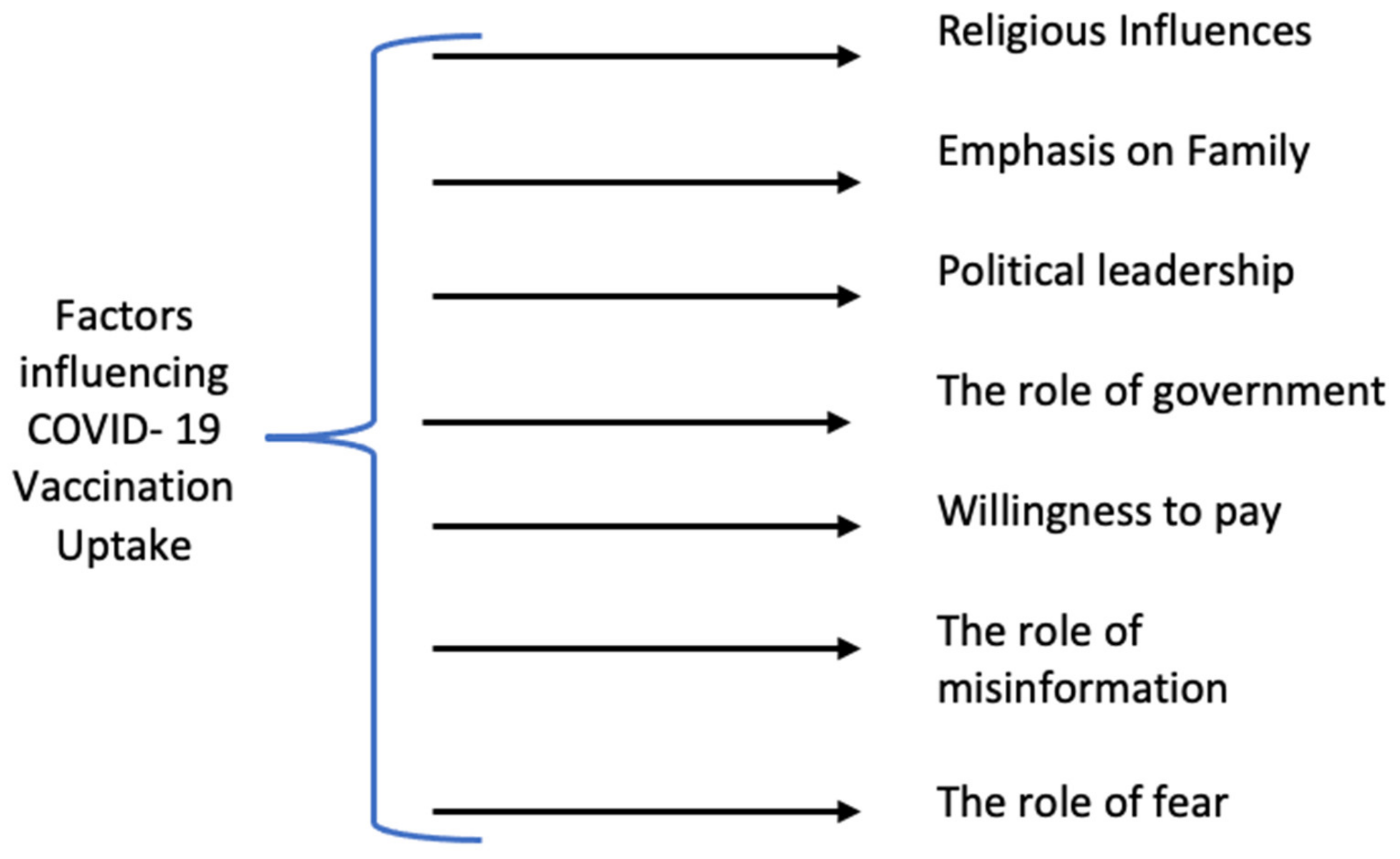
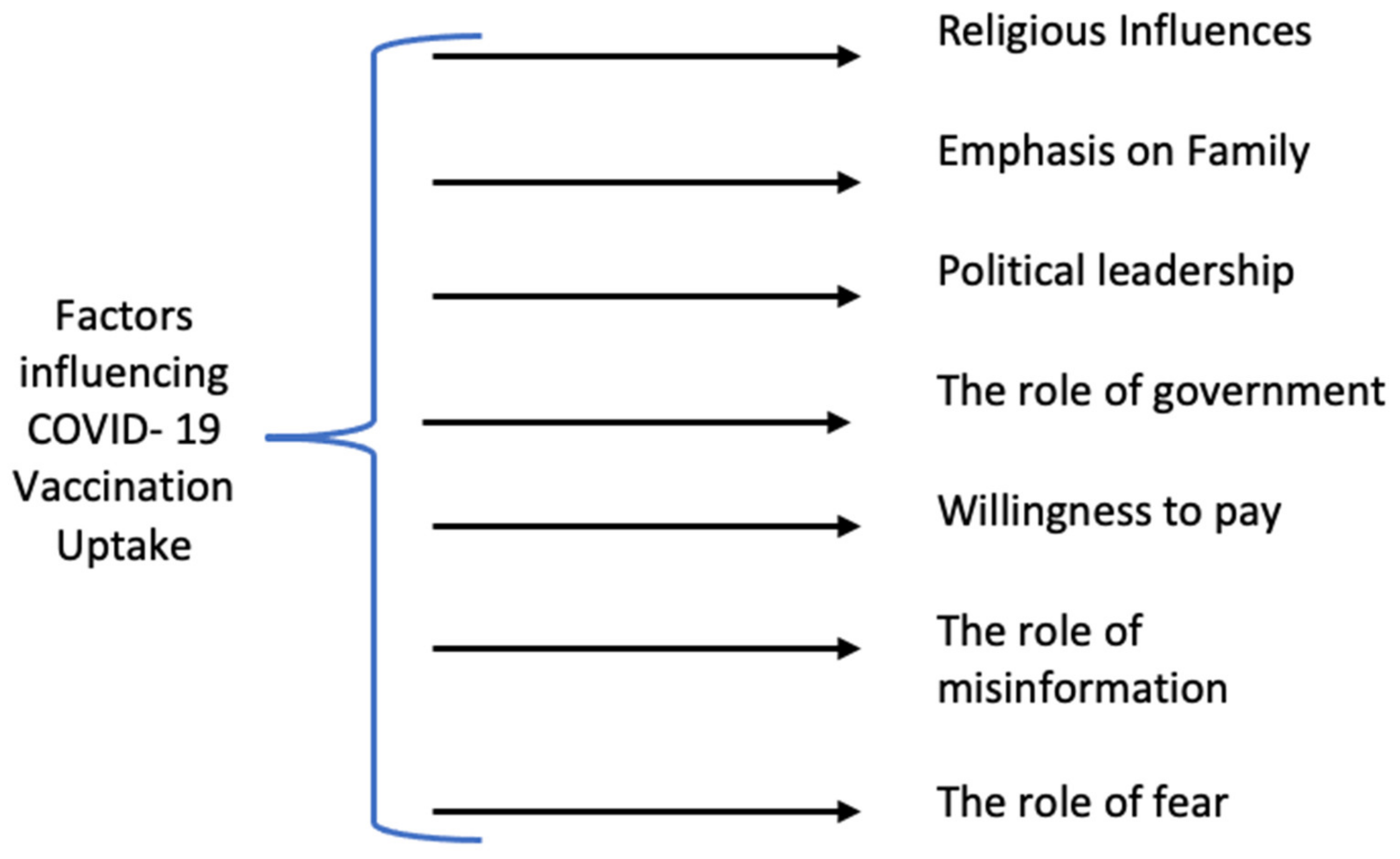
3.2. Themes
3.2.1. Religious Influence
“Religion will play a role. See, the thing is that Indians are quite religious. We always bring religious sentiments when eating food or wearing dresses like Western culture dresses. Also, I feel that many people would not prefer to have it (the vaccine) based on religious sentiments”.(participant 14)
Influence of Religious Leaders
“If religious leaders are educated about the vaccination process, they will educate the local people or their community and explain to them the importance of vaccine”.(participant 18)
Ingredients of Vaccine and Religious Sentiments
“When it comes to vaccine ingredients, it will not matter to me what is inside the dose. For example, we are given medicine like cough syrup when we have an illness. It contains alcohol (which is haram), but we overlook this aspect. We take medicines regularly, so we cannot claim that we have not taken alcohol. I will take the vaccine as vaccine and avoid thinking about this aspect”.(participant 42)
“The main reason I am apprehensive about the vaccine is that I do not know exactly what is in the vaccine. I will accept it only if the ingredients are halal (and not haram)”.(participant 6)
3.2.2. Emphasis on Family
Children
“When it comes to children, one has to be very careful as they have a long life ahead. It will be a big problem if some major side effect happens. The first thing is to consult a doctor, make sure that they are mentally and physically capable of taking the vaccines, only then the vaccine should be given to them”.(participant 25)
Seniors
“Yes, elders should go for vaccination because their immune system is not strong. Also, many of them have other diseases and co-morbidities. The doctor’s advice is vital before taking the vaccine in such cases”.(participant 14)
“I feel like old people should go for the vaccination, but if they have some other major disease like high blood pressure, diabetes or cancer, then they need to think twice, and for the same, they should take the advice from their family doctor first”.(participant 17)
Young People
“Young people should go for vaccination because they are the main sources of spreading. Since they travel to different places for professional and personal reasons, they meet many people who might be the carriers of the virus”.(participant 19)
3.2.3. Political Leadership
“Our honorable prime minister of India, as well as the chief minister of Delhi, have taken the vaccine, and hence people are influenced to follow suit. People felt assured that they took vaccinations as they were certain about their effects. Thus, personally taking the vaccine and suggesting others do the same will significantly influence creating a positive attitude towards the vaccine. Celebrities and politicians generally have a strong influence on people”.(participant 8)
3.2.4. The Role of Government
“Yes, the government (across India) has undertaken sufficient initiatives to guide people; they have created awareness about vaccines using local languages like Gujarati, Hindi, Marathi and that too in layman’s terms. They have even put a caller tune of around 30 s to spread awareness about taking vaccines when the slots are available. Sometimes it was irritating, but they have used it positively to influence people by delivering necessary information”.(participant 12)
“From Rajkot municipality corporation, a team of three people including a doctor used to come to our home at a regular interval to check about our health condition. They used to bring the COVID test kit, and if found positive, they would provide free basic medicine”.(participant 40)
“As my daughter was found COVID positive, she returned for a few days from her in-law’s family. She told me, every Tuesday and Friday, she used to get a call from the local municipality to check about her health”.(participant 37)
- (a)
- to control the spread of misinformation both online and offline
- (b)
- to provide vital information to the masses, especially to those located in rural areas and the weaker sections
- (c)
- to increase the supply of vaccines to private hospitals for easy access
- (d)
- to provide data of state-wise measures taken in the country
- (e)
- to ensure transparency concerning the vaccination process
- (f)
- to provide vaccines to private corporate employees as a priority
- (g)
- to collaborate with NGOs and other service provider organizations, and
- (h)
- to bring transparency by sharing vaccination data
3.2.5. Willingness to Pay
“I paid for my parents’ vaccination. My reason was not safety or hygiene or anything like that. My reason was that I did not want to burden the government with additional 500 rupees”.(participant 28)
“If I am supposed to take the vaccine, I will pay for it because I can afford it. US $7 for two shots is fine. The genuine reason for not going to the government health center is that if I give up my vaccine shot, a needy person can get that shot, and they will not have to pay for it. As I can afford it, so I can get it from a private hospital”.(participant 43)
3.2.6. The Role of Misinformation
“There are stories related to vaccine floating around saying that if we take the vaccine, then our genetic makeup changes. We are surrounded by a lot of misinformation about the vaccine because we do not have 100% information related to the vaccine”.(participant 30)
3.2.7. The Role of Fear
“My grandmother and my mother both have blood pressure and diabetics. I insisted they go for vaccination, but they were concerned about what would happen after taking the vaccine. That is why they were hesitant”.(participant 15)
“I am afraid because as we are young. I do not think corona will easily enter our body if we take care. Because of the lockdown, we have already improved our health. So, I do not feel the need for the vaccine because it may instead cause damage”.(participant 4)
“When I have a health problem, I choose Ayurveda medicine since my brother’s wife, brother-in-law, and father-in-law are all ayurvedic physicians. Only ayurvedic medicines are used to treat illnesses in our family, and I am fearful of other drugs”.(participant 7)
4. How Do Our Findings Compare with the Rest of the World?
5. Discussion, a Review of Government Efforts, and Recommendations
Practical Implications
6. Limitations and Future Research
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| No. | |
|---|---|
| A | Set of demographics details |
| B | Set of main questions |
| 1 | What are your views about the COVID vaccine? |
| 2 | What have you heard about the vaccine from various sources? |
| 3 | Do you have any hesitancy or fear regarding taking the vaccine? |
| 4 | Have you taken or would you take the vaccine? Why or why not? |
| 5 | What about your family members? Will you allow them to take the vaccine? [Emphasize both on children and elders, also try to find if they have co-morbidities] |
| 6 | What do you think is the role of religion in the acceptance of the COVID vaccine? For example, the role of religious leaders or halal? Do you know of anyone who has opted not to take the vaccine due to religious reasons? |
| 7 | What is your opinion on the effectiveness of the vaccine? |
| 8 | What is the role of misinformation in vaccine hesitancy? |
| 9 | What steps should be taken be taken to remove misinformation? |
| 10 | Do you think the government has taken sufficient measures to communicate the vaccine’s effectiveness? |
References
- Eskola, J.; Duclos, P.; Schuster, M.; MacDonald, N.E. How to deal with vaccine hesitancy? Vaccine 2015, 33, 4215–4217. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Ten Great Public Health Achievements—United States, 1900–1999. Available online: https://www.cdc.gov/mmwr/preview/mmwrhtml/00056796.htm (accessed on 12 December 2021).
- Wang, C.; Han, B.; Zhao, T.; Liu, H.; Liu, B.; Chen, L.; Xie, M.; Liu, J.; Zheng, H.; Zhang, S.; et al. Vaccination willingness, vaccine hesitancy, and estimated coverage at the first round of COVID-19 vaccination in China: A national cross-sectional study. Vaccine 2021, 39, 2833–2842. [Google Scholar] [CrossRef]
- MacDonald, N.E.; SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Domek, G.J.; O’Leary, S.T.; Bull, S.; Bronsert, M.; Contreras-Roldan, I.L.; Bolaños Ventura, G.A.; Kempe, A.; Asturias, E.J. Measuring vaccine hesitancy: Field testing the WHO SAGE Working Group on Vaccine Hesitancy survey tool in Guatemala. Vaccine 2018, 36, 5273–5281. [Google Scholar] [CrossRef]
- The Strategic Advisory Group of Experts (SAGE). Report of the SAGE Working Group on Vaccine Hesitancy. Available online: https://www.who.int/immunization/sage/meetings/2014/october/SAGE_working_group_revised_report_vaccine_hesitancy.pdf?ua=1 (accessed on 20 December 2020).
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 28 December 2021).
- Edwards, B.; Biddle, N.; Gray, M.; Sollis, K. COVID-19 vaccine hesitancy and resistance: Correlates in a nationally representative longitudinal survey of the Australian population. PLoS ONE 2021, 16, e0248892. [Google Scholar] [CrossRef]
- Schaffer DeRoo, S.; Pudalov, N.J.; Fu, L.Y. Planning for a COVID-19 vaccination program. JAMA 2020, 323, 2458–2459. [Google Scholar] [CrossRef]
- Agrawal, A.; Kolhapure, S.; Di Pasquale, A.; Rai, J.; Mathur, A. Vaccine hesitancy as a challenge or vaccine confidence as an opportunity for childhood immunization in India. Infect. Dis. Ther. 2020, 9, 421–432. [Google Scholar] [CrossRef]
- Kahana, D.; Yamin, D. Accounting for the spread of vaccination behavior to optimize influenza vaccination programs. PLoS ONE 2021, 16, e0252510. [Google Scholar] [CrossRef]
- Reñosa, M.D.C.; Wachinger, J.; Bärnighausen, K.; Aligato, M.F.; Landicho-Guevarra, J.; Endoma, V.; Landicho, J.; Bravo, T.A.; Demonteverde, M.P.; Guevarra, J.R.; et al. How can human-centered design-build a story-based video intervention that addresses vaccine hesitancy and bolsters vaccine confidence in the Philippines? A mixed-method protocol for project SALUBONG. BMJ Open 2021, 11, e046814. [Google Scholar] [CrossRef]
- Lane, S.; MacDonald, N.E.; Marti, M.; Dumolard, L. Vaccine hesitancy around the globe: Analysis of three years of WHO/UNICEF Joint Reporting form data-2015–2017. Vaccine 2018, 36, 3861–3867. [Google Scholar] [CrossRef]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef]
- Prime Minister of Canada Justin Trudeau. Prime Minister Announces Mandatory Vaccination for the Federal Workforce and Federally Regulated Transportation Sectors. Available online: https://pm.gc.ca/en/news/news-releases/2021/10/06/prime-minister-announces-mandatory-vaccination-federal-workforce-and (accessed on 24 November 2021).
- Bogart, L.M.; Ojikutu, B.O.; Tyagi, K.; Klein, D.J.; Mutchler, M.G.; Dong, L.; Lawrence, S.J.; Thomas, D.R.; Kellman, S. COVID-19 related medical mistrust, health impacts, and potential vaccine hesitancy among black Americans Living With HIV. J. Acquir. Immune Defic. Syndr. 2021, 86, 200–207. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 11, 1–15. [Google Scholar] [CrossRef]
- Opel, D.J.; Diekema, D.S.; Lee, N.R.; Marcuse, E.K. Social Marketing as a Strategy to Increase Immunization Rates. Arch. Pediatrics Adolesc. Med. 2009, 163, 432–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoda, T.; Katsuyama, H. Willingness to receive COVID-19 vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Khan, A. State Must Not Drag Its Feet and Make COVID Vaccination Mandatory for All Adults. Available online: https://www.news18.com/news/opinion/state-must-not-drag-its-feet-make-covid-vaccination-mandatory-4526342.html (accessed on 3 February 2022).
- The Economic Times. India’s Vaccination Drive Picks Up Pace in June but Still Isn’t Fast Enough. Available online: https://economictimes.indiatimes.com/news/india/indias-vaccination-drive-picks-up-pace-in-june-but-still-isnt-fast-enough/articleshow/83475665.cms (accessed on 3 October 2021).
- Ministry of Health and Family Welfare. COVID-19 Vaccine Operational Guidelines. Available online: https://main.mohfw.gov.in/sites/default/files/COVID19VaccineOG111Chapter16.pdf (accessed on 12 November 2021).
- Kumar, V.M.; Pandi-Perumal, S.R.; Trakht, I.; Thyagarajan, S.P. Strategy for COVID-19 vaccination in India: The country with the second-highest population and number of cases. npj Vaccines 2021, 6, 60. [Google Scholar] [CrossRef] [PubMed]
- Bhuyan, A. Covid-19: India sees a new spike in cases despite vaccine rollout. BMJ 2021, 372, n854. [Google Scholar] [CrossRef]
- Statista. Cumulative Number of COVID-19 Vaccine Doses Administered Across States and Union Territories in India as of 29 November 2021. Available online: https://www.statista.com/statistics/1222266/india-cumulative-coverage-of-covid-19-vaccine-across-india/ (accessed on 18 December 2021).
- PIB Headquarters. PIB’S Bulletin on COVID-19. Available online: https://pib.gov.in/PressReleaseIframePage.aspx?PRID=1741093 (accessed on 3 February 2022).
- Business Line. Covid-19 Vaccination: Gujarat Covers 50% Population with the First Dose. Available online: https://www.thehindubusinessline.com/news/national/covid-19-vaccination-gujarat-covers-50-population-with-first-dose/article35622212.ece (accessed on 3 October 2021).
- Aggarwal, P.; Mishra, M. How much of India’s Population has been Inoculated, Age-Wise. Available online: https://www.indiatoday.in/diu/story/how-much-of-india-population-has-been-inoculated-age-wise-1823256-2021-07-02 (accessed on 8 February 2022).
- Usmani, A. India Sustains Improved Vaccination Rates in July with 12.9 Crore Doses Given. Available online: https://www.bloombergquint.com/coronavirus-outbreak/india-sustains-improved-vaccination-rates-in-july-with-129-crore-doses-given (accessed on 9 February 2022).
- Choudhury, S.R. India’s Ambitious Vaccine Targets Alone Will Not Help Immunize Its Massive Population. Available online: https://www.cnbc.com/2021/06/14/india-covid-crisis-making-vaccines-readily-available-is-a-challenge.html (accessed on 3 October 2021).
- Ministry of Health & Family Welfare India. Population Projections for India and States 2011–2036. Available online: https://main.mohfw.gov.in/sites/default/files/Population%20Projection%20Report%202011-2036%20-%20upload_compressed_0.pdf (accessed on 12 December 2021).
- Census Population Data. Gujarat Population 2011–2021. Available online: https://www.census2011.co.in/census/state/gujarat.html (accessed on 9 February 2022).
- Bhattacharya, M. Advantage Gujarat in medical tourism. In Proceedings of the Conference on Tourism in India—Challenges Ahead, Kozhikode, India, 15–17 May 2008. [Google Scholar]
- Rawat, S. Ramdev Now Says the Covid Vaccine Has No Use; He Has a Dual Cover with Yoga, Ayurveda. Available online: https://www.hindustantimes.com/india-news/ramdev-now-says-vaccine-has-no-use-he-has-dual-cover-with-yoga-ayurveda-101622398963396.html (accessed on 30 January 2022).
- Washington State Department of Health. Social Marketing Recommendations for COVID-19 Vaccine. Available online: https://www.doh.wa.gov/Portals/1/Documents/1600/coronavirus/VaccineSocialMarketingPlan.pdf (accessed on 3 October 2021).
- Deshpande, S.; Lee, N.R. Social Marketing in India; Sage Publications: Delhi, India, 2013. [Google Scholar]
- Evans, W.D.; French, J. Demand creation for COVID-19 vaccination: Overcoming vaccine hesitancy through social marketing. Vaccines 2021, 9, 319. [Google Scholar] [CrossRef]
- French, J.; Deshpande, S.; Evans, W.; Obregon, R. Key guidelines in developing a pre-emptive COVID-19 vaccination uptake promotion strategy. Int. J. Environ. Res. Public Health 2020, 17, 5893. [Google Scholar] [CrossRef]
- Sharma, M. 73,600 COVID Vaccination Centres Operational in India on Monday, Highest till Date. Available online: https://www.indiatoday.in/coronavirus-outbreak/vaccine-updates/story/highest-operational-covid-vaccination-centres-india-monday-1792833-2021-04-20 (accessed on 3 October 2021).
- Das, T. Pfizer’s COVID-19 Vaccine May Cost Less than $10 a Dose in India. Available online: https://www.business-standard.com/article/current-affairs/pfizer-s-coronavirus-vaccine-may-cost-less-than-rs-730-a-dose-in-india-121060901739_1.html (accessed on 3 October 2021).
- Morse, J.M. The significance of saturation. Qual. Health Res. 1995, 5, 147–149. [Google Scholar] [CrossRef]
- Cresswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Traditions; Sage: London, UK, 1998. [Google Scholar]
- McGrath, C.; Palmgren, P.J.; Liljedahl, M. Twelve tips for conducting qualitative research interviews. Med. Teach. 2019, 41, 1002–1006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hair, J.F.; Bush, R.P.; Ortinau, D.J. Marketing Research: Within a Changing Environment, 3rd ed.; McGraw-Hill/Irwin: New York, NY, USA, 2006. [Google Scholar]
- Mason, M. Sample size and saturation in PhD studies using qualitative interviews. Forum Qual. Soz. Forum Qual. Soc. Res. 2010, 11, 1428. [Google Scholar] [CrossRef]
- Sinkovics, R.R.; Penz, E.; Ghauri, P.N. Enhancing the trustworthiness of qualitative research in international business. Manag. Int. Rev. 2008, 48, 689–714. [Google Scholar] [CrossRef]
- Boeije, H. A purposeful approach to the constant comparative method in the analysis of qualitative interviews. Qual. Quant. 2002, 36, 391–409. [Google Scholar] [CrossRef]
- Reuters. Reuters COVID-19 Tracker. Available online: https://graphics.reuters.com/world-coronavirus-tracker-and-maps/countries-and-territories/brazil/ (accessed on 27 November 2021).
- Rigoli, F. The link between COVID-19, anxiety, and religious beliefs in the United States and the United Kingdom. J. Relig. Health 2021, 60, 2196–2208. [Google Scholar] [CrossRef]
- Graves, G. Maine Provides Leadership on Religion and Vaccines. Available online: https://americanprogress.org/people/graves-fitzsimmons-guthrie/ (accessed on 26 November 2021).
- Smith, D.T.; Attwell, K.; Evers, U. Support for a COVID-19 vaccine mandate in the face of safety concerns and political affiliations: An Australian study. Politics 2021, 02633957211009066. [Google Scholar] [CrossRef]
- Wong, L.P.; Wong, P.-F.; Megat Hashim, M.M.A.A.; Han, L.; Lin, Y.; Hu, Z.; Zhao, Q.; Zimet, G.D. Multidimensional social and cultural norms influencing HPV vaccine hesitancy in Asia. Hum. Vaccines Immunother. 2020, 16, 1611–1622. [Google Scholar] [CrossRef]
- Huda, E.; Zainudin, E.N.; Mohammad, K.A.; Aris, A.; Shahdan, I.A. Vaccination: Influencing factors and view from an Islamic perspective. IIUM Med. J. Malays. 2018, 17, 997. [Google Scholar] [CrossRef]
- Padhi, B.K.; Al-Mohaithef, M. Determinants of COVID-19 vaccine acceptance in Saudi Arabia: A web-based national survey. medRxiv 2020. [Google Scholar] [CrossRef]
- Pakkawan, A. Prayers Allowed at Mosques Where 70% of Local People Are Vaccinated. Available online: https://www.bangkokpost.com/thailand/general/2176019/prayers-allowed-at-mosques-where-70-of-local-people-are-vaccinated (accessed on 24 November 2021).
- Lahav, E.; Shahrabani, S.; Rosenboim, M.; Tsutsui, Y. Is stronger religious faith associated with a greater willingness to take the COVID-19 vaccine? Evidence from Israel and Japan. Eur. J. Health Econ. 2021, 1–17. [Google Scholar] [CrossRef]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination hesitancy in the United States: A rapid national assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef] [PubMed]
- Mant, M.; Aslemand, A.; Prine, A.; Jaagumägi Holland, A. University students’ perspectives, planned uptake, and hesitancy regarding the COVID-19 vaccine: A multi-methods study. PLoS ONE 2021, 16, e0255447. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Wyka, K.; Rauh, L.; Rabin, K.; Ratzan, S.; Gostin, L.O.; Larson, H.J.; El-Mohandes, A. Hesitant or not? The association of age, gender, and education with potential acceptance of a COVID-19 vaccine: A country-level analysis. J. Health Commun. 2020, 25, 799–807. [Google Scholar] [CrossRef]
- Griffith, J.; Marani, H.; Monkman, H. COVID-19 vaccine hesitancy in Canada: Content analysis of tweets using the Theoretical Domains Framework. J. Med. Internet Res. 2021, 23, e26874. [Google Scholar] [CrossRef] [PubMed]
- BBC News. Covid: Who Can Have a Booster Jab, and How Can You Get One? Available online: https://www.bbc.com/news/health-55045639 (accessed on 24 November 2021).
- Mirza, A. Coronavirus Vaccine: Is It Halal or Not? Available online: https://timesofindia.indiatimes.com/readersblog/marginalia/coronavirus-vaccine-is-it-halal-or-not-28978/ (accessed on 24 November 2021).
- Ministers Department of Health. Australia Secures a Further 50 Million Doses of the COVID-19 Vaccine. Available online: https://www.health.gov.au/ministers/the-hon-greg-hunt-mp/media/australia-secures-a-further-50-million-doses-of-covid-19-vaccine (accessed on 5 November 2021).
- Burki, T. No end in sight for the Brazilian COVID-19 crisis. Lancet Microbe 2021, 2, e180. [Google Scholar] [CrossRef]
- Fonseca, E.M.d.; Shadlen, K.C.; Bastos, F.I. The politics of COVID-19 vaccination in middle-income countries: Lessons from Brazil. Soc. Sci. Med. 2021, 281, 114093. [Google Scholar] [CrossRef]
- The Lancet. COVID-19 in Brazil: “So what?”. Lancet 2020, 395, 1461. [Google Scholar] [CrossRef]
- Marcello, M.; Boadle, A. Brazil’s Former Health Minister Shields Bolsonaro in COVID-19 Inquiry. Available online: https://www.reuters.com/world/americas/brazils-former-health-minister-shields-bolsonaro-covid-19-inquiry-2021-05-19/ (accessed on 19 May 2021).
- Reuters Staff. Saudi Arabia’s Crown Prince Receives the First Dose of COVID-19 Vaccine—SPA. Available online: https://www.reuters.com/article/uk-health-coronavirus-saudi-idUSKBN28Z0VD (accessed on 3 January 2022).
- Kosaka, M.; Hashimoto, T.; Ozaki, A.; Tanimoto, T.; Kami, M. Delayed COVID-19 vaccine rollout in Japan. Lancet 2021, 397, 2334–2335. [Google Scholar] [CrossRef]
- The White House. Path Out of the Pandemic President Biden’s COVID-19 Action Plan. Available online: https://www.whitehouse.gov/covidplan/ (accessed on 3 October 2021).
- Holzmann-Littig, C.; Braunisch, M.C.; Kranke, P.; Popp, M.; Seeber, C.; Fichtner, F.; Littig, B.; Carbajo-Lozoya, J.; Allwang, C.; Frank, T. COVID-19 vaccination acceptance and hesitancy among healthcare workers in Germany. Vaccines 2021, 9, 777. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Government of Canada Funds Four New Projects to Encourage COVID-19 Vaccination in Canada. Available online: https://www.canada.ca/en/public-health/news/2021/06/government-of-canada-funds-four-new-projects-to-encourage-covid-19-vaccination-in-canada.html (accessed on 24 November 2021).
- Australian government. National Plan to Transition Australia’s National COVID-19 Response. Available online: https://www.pm.gov.au/sites/default/files/media/national-plan-060821_0.pdf (accessed on 12 January 2022).
- Bennett, C.M. Learning to live with COVID-19 in Australia: Time for a new approach. Public Health Res. Pract. 2021, 31, e3132110. [Google Scholar] [CrossRef]
- Australian government. TGA Issues Warning about Illegal Advertising Relating to COVID-19. Available online: https://www.tga.gov.au/node/904127 (accessed on 12 January 2022).
- Freckelton Qc, I. COVID-19: Fear, quackery, false representations and the law. Int. J. Law Psychiatry 2020, 72, 101611. [Google Scholar] [CrossRef] [PubMed]
- The Tribune. Brazil Aims to Vaccinate the Entire Population against COVID-19 in 2021. Available online: https://www.tribuneindia.com/news/world/brazil-aims-to-vaccinate-entire-population-against-covid-19-in-2021-182451 (accessed on 27 November 2021).
- Al-Mohaithef, M.; Padhi, B.K.; Ennaceur, S. Socio-demographics correlate of COVID-19 vaccine hesitancy during the second wave of COVID-19 pandemic: A cross-sectional web-based survey in Saudi Arabia. Front. Public Health 2021, 9, 698106. [Google Scholar] [CrossRef] [PubMed]
- Ani. Saudi Arabia Issues New Guidelines for Umrah Pilgrims. Available online: https://www.deccanchronicle.com/world/middle-east/060421/saudi-arabia-issues-new-guidelines-for-umrah-pilgrims.html (accessed on 24 November 2021).
- Rattanachaikunsopon, P.; Phumkhachorn, P. A glimpse of the covid-19 situation in Thailand. Int. J. Curr. Res. Rev. 2020, 12, 1–2. [Google Scholar] [CrossRef]
- Namwat, C.; Suphanchaimat, R.; Nittayasoot, N.; Iamsirithaworn, S. Thailand’s response against coronavirus disease 2019: Challenges and lessons learned. OSIR J. 2020, 13, 33–37. [Google Scholar]
- Hayes, R. Japan: From Vaccine Hesitancy to Vaccine Success. Available online: https://www.bbc.com/news/world-asia-59342308 (accessed on 24 November 2021).
- Wong, L.P.; Alias, H.; Wong, P.F.; Lee, H.Y.; Abubakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccine Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef] [PubMed]
- Catma, S.; Reindl, D. Parents’ willingness to pay for a COVID-19 vaccine for themselves and their children in the United States. Hum. Vaccines Immunother. 2021, 17, 2919–2925. [Google Scholar] [CrossRef]
- Godói, I.; Sarmento, T.; Reis, E.; Gargano, L.; Godman, B.; Acurcio, F.; Alvares, J.; Guerra Junior, A.; Ruas, C. Acceptability and willingness to pay for a hypothetical vaccine against SARS CoV-2 by the Brazilian consumer: A cross-sectional study and the implications. Expert Rev. Pharm. Outcomes Res. 2021, 22, 119–129. [Google Scholar] [CrossRef]
- Sprengholz, P.; Eitze, S.; Felgendreff, L.; Korn, L.; Betsch, C. Money is not everything: Experimental evidence that payments do not increase willingness to be vaccinated against COVID-19. J. Med. Ethics 2021, 47, 547–548. [Google Scholar] [CrossRef]
- Borriello, A.; Master, D.; Pellegrini, A.; Rose, J.M. Preferences for a COVID-19 vaccine in Australia. Vaccine 2021, 39, 473–479. [Google Scholar] [CrossRef]
- Kitro, A.; Sirikul, W.; Piankusol, C.; Rirermsoonthorn, P.; Seesen, M.; Wangsan, K.; Assavanopakun, P.; Surawattanasakul, V.; Kosai, A.; Sapbamrer, R. Acceptance, attitude, and factors affecting the intention to accept COVID-19 vaccine among Thai people and expatriates living in Thailand. Vaccine 2021, 39, 7554–7561. [Google Scholar] [CrossRef]
- Evanega, S.; Lynas, M.; Adams, J.; Smolenyak, K. Coronavirus misinformation: Quantifying sources and themes in the COVID-19 ‘infodemic’. JMIR Preprints 2020. [Google Scholar] [CrossRef]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 960. [Google Scholar] [CrossRef] [PubMed]
- Desveaux, L.; Savage, R.D.; Tadrous, M.; Kithulegoda, N.; Thai, K.; Stall, N.M.; Ivers, N.M. Beliefs associated with intentions of non-physician healthcare workers to receive the COVID-19 vaccine in Ontario, Canada. medRxiv 2021. [Google Scholar] [CrossRef]
- Lewsey, F. Cambridge Game ‘Pre-Bunks’ Coronavirus Conspiracies. Available online: https://www.goviralgame.com/ (accessed on 3 October 2021).
- OECD. Enhancing Public Trust in COVID-19 Vaccination: The Role of Governments. Available online: https://www.oecd.org/coronavirus/policy-responses/enhancing-public-trust-in-covid-19-vaccination-the-role-of-governments-eae0ec5a/ (accessed on 17 October 2021).
- Rozbroj, T.; Lyons, A.; Lucke, J. The mad leading the blind: Perceptions of the vaccine-refusal movement among Australians who support vaccination. Vaccine 2019, 37, 5986–5993. [Google Scholar] [CrossRef]
- Taylor, J. TikTok Takes Down Hundreds of Australian Videos in Misinformation Crackdown. Available online: https://www.theguardian.com/technology/2021/may/22/tiktok-takes-down-hundreds-of-australian-videos-in-misinformation-crackdown (accessed on 24 November 2021).
- Pickles, K.; Cvejic, E.; Nickel, B.; Copp, T.; Bonner, C.; Leask, J.; Ayre, J.; Batcup, C.; Cornell, S.; Dakin, T.; et al. COVID-19 Misinformation trends in Australia: Prospective longitudinal national survey. J. Med. Internet Res. 2021, 23, e23805. [Google Scholar] [CrossRef]
- Coletiva.net. A Survey Warns That Seven Out of Ten Brazilians Believe in Fake News about COVID-19. Available online: https://coletiva.net/noticias/pesquisa-alerta-que-sete-em-cada-dez-brasileiros-acreditam-em-fake-news-sobre-covid-19,358082.jhtml (accessed on 24 November 2021).
- Alasmari, A.; Addawood, A.; Nouh, M.; Rayes, W.; Al-Wabil, A. A retrospective analysis of the COVID-19 infodemic in Saudi Arabia. Future Internet 2021, 13, 254. [Google Scholar] [CrossRef]
- Mongkhon, P.; Ruengorn, C.; Awiphan, R.; Thavorn, K.; Hutton, B.; Wongpakaran, N.; Wongpakaran, T.; Nochaiwong, S. Exposure to COVID-19-related information and its association with mental health problems in Thailand: Nationwide, cross-sectional survey study. J. Med. Internet Res. 2021, 23, e25363. [Google Scholar] [CrossRef]
- Nomura, S.; Eguchi, A.; Yoneoka, D.; Kawashima, T.; Tanoue, Y.; Murakami, M.; Sakamoto, H.; Maruyama-Sakurai, K.; Gilmour, S.; Shi, S.; et al. Reasons for being unsure or unwilling regarding the intention to take COVID-19 vaccine among Japanese people: A large cross-sectional national survey. Lancet Reg. Health West. Pac. 2021, 14, 100223. [Google Scholar] [CrossRef]
- Trent, M.; Seale, H.; Chughtai, A.A.; Salmon, D.; MacIntyre, C.R. Trust in government, intention to vaccinate and COVID-19 vaccine hesitancy: A comparative survey of five large cities in the United States, United Kingdom, and Australia. Vaccine 2021. [Google Scholar] [CrossRef]
- Kirzinger, A.; Kearney, A.; Hamel, L.; Brodie, M. KFF/The Washington Post Frontline Health Care Workers Survey. Available online: https://www.kff.org/report-section/kff-washington-post-frontline-health-care-workers-survey-vaccine-intentions/ (accessed on 12 January 2022).
- Bauernfeind, S.; Hitzenbichler, F.; Huppertz, G.; Zeman, F.; Koller, M.; Schmidt, B.; Plentz, A.; Bauswein, M.; Mohr, A.; Salzberger, B. Brief report: Attitudes towards COVID-19 vaccination among hospital employees in a tertiary care university hospital in Germany in December 2020. Infection 2021, 49, 1307–1311. [Google Scholar] [CrossRef]
- Iyengar, K.P.; Vaishya, R.; Jain, V.K.; Ish, P. BAME community hesitancy in the UK for COVID-19 vaccine: Suggested solutions. Postgrad. Med. J. 2021, postgradmedj-2021-139957. [Google Scholar] [CrossRef]
- Rhodes, A.; Hoq, M.; Measey, M.-A.; Danchin, M. Intention to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2021, 21, e110. [Google Scholar] [CrossRef]
- BBC News. COVID: Australia’s Vaccine Hesitancy Worries Medical Experts. Available online: https://www.bbc.com/news/world-australia-57181038 (accessed on 27 November 2021).
- The New Indian Express. Australians’ Fear of COVID-19 Infection Hits an All-Time High. Available online: https://www.newindianexpress.com/world/2021/nov/20/australians-fear-of-covid-19-infection-hits-all-time-high-2386039.html (accessed on 27 November 2021).
- Moore, D.C.B.C.; Nehab, M.F.; Camacho, K.G.; Reis, A.T.; Junqueira-Marinho, M.d.F.; Abramov, D.M.; Azevedo, Z.M.A.d.; Menezes, L.A.d.; Salú, M.d.S.; Figueiredo, C.E.d.S.; et al. Low COVID-19 vaccine hesitancy in Brazil. Vaccine 2021, 39, 6262–6268. [Google Scholar] [CrossRef]
- Thanapluetiwong, S.; Chansirikarnjana, S.; Sriwannopas, O.; Assavapokee, T.; Ittasakul, P. Factors associated with COVID-19 Vaccine hesitancy in Thai seniors. Patient Prefer. Adherence 2021, 15, 2389–2403. [Google Scholar] [CrossRef] [PubMed]
- Okubo, R.; Yoshioka, T.; Ohfuji, S.; Matsuo, T.; Tabuchi, T. COVID-19 Vaccine hesitancy and its associated factors in Japan. Vaccines 2021, 9, 662. [Google Scholar] [CrossRef] [PubMed]
- Vaughan, D. What Is the Most Widely Practiced Religion in the World? Available online: https://www.britannica.com/story/what-is-the-most-widely-practiced-religion-in-the-world (accessed on 3 October 2021).
- Entringer, T.; Gebauer, J.; Eck, J.; Bleidorn, W.; Rentfrow, P.; Potter, J.; Gosling, S. Big Five facets and religiosity: Three large-scale, cross-cultural, theory-driven, and process-attentive tests. J. Personal. Soc. Psychol. 2020, 120, 1662–1695. [Google Scholar] [CrossRef] [PubMed]
- Hanegraaff, W.J. Imagining the future study of religion and spirituality. Religion 2020, 50, 72–82. [Google Scholar] [CrossRef]
- Purzycki, B.G.; Willard, A.K.; Klocová, E.K.; Apicella, C.; Atkinson, Q.; Bolyanatz, A.; Cohen, E.; Handley, C.; Henrich, J.; Lang, M.; et al. The moralization bias of Gods’ minds: A cross-cultural test. Relig. Brain Behav. 2021. submitted. [Google Scholar]
- Leger. Leger’s North American Tracker—16 February 2021. Available online: https://leger360.com/surveys/legers-north-american-tracker-february-16-2021/ (accessed on 3 October 2021).
- Kim, S.-y.; Sagiraju, H.K.R.; Russell, L.B.; Sinha, A. Willingness-to-pay for vaccines in low-and middle-income countries: A systematic review. Ann. Vaccines Immun. 2014, 1, 1001. [Google Scholar]
- Gupta, A.; Li, H.; Farnoush, A.; Kayla Jiang, W. Understanding patterns of COVID infodemic: A systematic and pragmatic approach to curb fake news. J. Bus. Res. 2021, 140, 670–683. [Google Scholar] [CrossRef]
- Singh, L.; Bansal, S.; Bode, L.; Budak, C.; Chi, G.; Kawintiranon, K.; Padden, C.; Vanarsdall, R.; Vraga, E.; Wang, Y. A first look at COVID-19 information and misinformation sharing on Twitter. arXiv 2020, arXiv:2003.13907. [Google Scholar]
- Saunders, S.G.; Barrington, D.J.; Sridharan, S. Redefining social marketing: Beyond behavioural change. J. Soc. Mark. 2015, 5, 160–168. [Google Scholar] [CrossRef]
- Truong, V.D.; Saunders, S.G.; Dong, X.D. Systems social marketing: A critical appraisal. J. Soc. Mark. 2019, 9, 180–203. [Google Scholar] [CrossRef]
- World Health Organization. World Immunization Week 2021 Vaccines bring us closer. Available online: https://www.worldimmunizationweek.org/ (accessed on 30 January 2022).
- National Information Center India. #India Fights Corona COVID-19. Available online: https://www.mygov.in/covid-19 (accessed on 3 October 2021).
- Alabama Public Health. Vaccinate Alabama TikTok Contest. Available online: https://www.alabamapublichealth.gov/covid19vaccine/tiktok.html (accessed on 12 December 2021).
- Ministry of Health and Family Welfare. Covid-19 Vaccine Communication Strategy. Available online: https://www.mohfw.gov.in/pdf/Covid19CommunicationStrategy2020.pdf (accessed on 24 November 2021).
- Public Health Agency of Canada. Participation in the “My Why” Social Campaign and How You Can Share Your Vaccination Story. Available online: https://www.canada.ca/en/public-health/services/publications/diseases-conditions/covid-19-share-vaccination-story.html (accessed on 29 November 2021).
- Government of India. Jan Adolan for COVID-19 Appropriate Behaviour. Available online: https://pledge.mygov.in/janandolan-covid/ (accessed on 24 November 2021).
- Unnithan, C. Gujarat Tops in Social Media Users Via Smartphone. Available online: http://timesofindia.indiatimes.com/articleshow/22183206.cms?utm_source=contentofinterest&utm_medium=text&utm_campaign=cppst (accessed on 9 February 2022).
- Parikh, N. Gujarat’s Teledensity Crosses the 100% Mark. Available online: https://timesofindia.indiatimes.com/city/ahmedabad/states-tele-density-crosses-100-mark/articleshow/86565666.cms (accessed on 3 February 2021).
- Ansari, M.A.; Khan, Z.; Khan, I.M. Reducing resistance against polio drops. J. R. Soc. Promot. Health 2007, 127, 276–279. [Google Scholar] [CrossRef]
| Gender | Male | 21 (48%) |
| Female | 23 (52%) | |
| Age | 18–25 years | 9 (21%) |
| 26–35 years | 16 (36%) | |
| 36–45 years | 14 (32%) | |
| 46–55 years | 4 (9%) | |
| 56–65 years | 1 (2%) | |
| Religion | Hindu | 37 (84%) |
| Muslims | 2 (5%) | |
| Christian | 2 (5%) | |
| Jain | 1 (2%) | |
| Not Stated | 2 (5%) | |
| Level of education | Less than 10th grade | 8 (18%) |
| High school | 2 (5%) | |
| Diploma | 2 (5%) | |
| Bachelor | 4 (9%) | |
| Master | 19 (43%) | |
| PhD | 9 (20%) | |
| Working Status | Academics: Teaching staff | 21 (48%) |
| Driver | 9 (20%) | |
| Academics: Non-teaching staff | 5 (11%) | |
| Corporate job | 2 (5%) | |
| Businessperson | 2 (5%) | |
| Coaching class counsellor | 1 (2%) | |
| Coaching class teacher | 1 (2%) | |
| Fashion designer | 1 (2%) | |
| Homemaker | 1 (2%) | |
| Street hawker | 1 (2%) | |
| Marital Status | Married | 29 (66%) |
| Unmarried | 13 (30%) | |
| Prefer not to say | 2 (5%) | |
| City in Gujarat | Rajkot | 37 (84%) |
| Surat | 3 (7%) | |
| Ahmedabad | 1 (2%) | |
| Anand | 1 (2%) | |
| Vadodara (Baroda) | 1 (2%) | |
| Bharuch | 1 (2%) |
| Major Factors | Northern America | Europe | Oceania | Latin America and the Caribbean | Asia | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Country | USA | Germany | Canada | UK | Australia | Brazil | Saudi Arabia | Thailand | Japan | India (Current Study) | |
| Eligible population (million) and % of population given at least one dose of vaccine (accessed on 27 November 2021) [48] | 200 (65.3%) | 60 (76%) | 30 (77.9%) | 50 (73.1%) | 20 (66.4%) | 200 (71.6%) | 20 (68.2%) | 30 (42.3%) | 90 (70.6.%) | 700 (47.7.%) | |
| 1 | Religious influence | Rigoli [49], Graves [50] | - | Rigoli [49] | Edwards, Biddle, Gray and Sollis [8], Smith et al. [51] | - | Wong et al. [52], Huda E. Zainudin et al. [53], Padhi and Al-Mohaithef [54] | Pakkawan [55] | Lahav et al. [56] | Yes | |
| 2 | Emphasis on family members | Khubchandani et al. [57] | - | Mant et al. [58], Lazarus et al. [59] | Lazarus, Wyka, Rauh, Rabin, Ratzan, Gostin, Larson and El-Mohandes [59] | - | Lazarus, Wyka, Rauh, Rabin, Ratzan, Gostin, Larson and El-Mohandes [59] | - | - | Yoda and Katsuyama [19] | Yes |
| 3 | Political leadership | Khubchandani, Sharma, Price, Wiblishauser, Sharma and Webb [57] | - | Griffith et al. [60] | BBC news [61], Mirza [62] | Ministers Department of Health [63] | Burki [64], Fonseca et al. [65], Lancet [66] Marcello and Boadle [67] | Reuters Staff [68] | - | Kosaka et al. [69] | Yes |
| 4 | The role of government | The White House [70] | Holzmann-Littig et al. [71] | Public Health Agency of Canada [72], [15] | The White House [70] | Australian Government [73], Bennett [74], Australian Government [75], Freckelton Qc [76] | The Tribune [77], Reuters [48] | Al-Mohaithef et al. [78], Ani [79] | Rattanachaikunsopon and Phumkhachorn [80], Namwat et al. [81] | Kosaka, Hashimoto, Ozaki, Tanimoto and Kami [69], Hayes [82] | Yes |
| 5 | Willingness to pay | Wong et al. [83], Catma and Reindl [84], Godói et al. [85] | Sprengholz et al. [86] | Wong, Alias, Wong, Lee and AbuBakar [83] | Borriello et al. [87] | Kitro et al. [88] | - | - | - | Yes | |
| 6 | The role of misinformation | Evanega et al. [89], Loomba et al. [90] | - | Desveaux et al. [91] | Loomba, de Figueiredo, Piatek, de Graaf and Larson [90] Lewsey [92], OECD [93] | Rozbroj et al. [94], Taylor [95], Pickles et al. [96]. | Coletiva.net [97] | Alasmari et al. [98] | Mongkhon et al. [99] | Freckelton Qc [76], Nomura et al. [100] | Yes |
| 7 | The role of fear | Trent et al. [101], Kirzinger et al. [102] | Bauernfeind et al. [103] | Griffith, Marani and Monkman [60], Mant, Aslemand, Prine and Jaagumägi Holland [58] | Iyengar et al. [104] | Rhodes et al. [105], BBC News [106], The New Indian Express [107], Yoda and Katsuyama [19] | Moore et al. [108] | Padhi and Al-Mohaithef [54] | Thanapluetiwong et al. [109] | Nomura, Eguchi, Yoneoka, Kawashima, Tanoue, Murakami, Sakamoto, Maruyama-Sakurai, Gilmour, Shi, Kunishima, Kaneko, Adachi, Shimada, Yamamoto and Miyata [100], Okubo et al. [110], Yoda and Katsuyama [19] | Yes |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tolia, V.; Renin Singh, R.; Deshpande, S.; Dave, A.; Rathod, R.M. Understanding Factors to COVID-19 Vaccine Adoption in Gujarat, India. Int. J. Environ. Res. Public Health 2022, 19, 2707. https://doi.org/10.3390/ijerph19052707
Tolia V, Renin Singh R, Deshpande S, Dave A, Rathod RM. Understanding Factors to COVID-19 Vaccine Adoption in Gujarat, India. International Journal of Environmental Research and Public Health. 2022; 19(5):2707. https://doi.org/10.3390/ijerph19052707
Chicago/Turabian StyleTolia, Viral, Rajkumar Renin Singh, Sameer Deshpande, Anupama Dave, and Raju M. Rathod. 2022. "Understanding Factors to COVID-19 Vaccine Adoption in Gujarat, India" International Journal of Environmental Research and Public Health 19, no. 5: 2707. https://doi.org/10.3390/ijerph19052707
APA StyleTolia, V., Renin Singh, R., Deshpande, S., Dave, A., & Rathod, R. M. (2022). Understanding Factors to COVID-19 Vaccine Adoption in Gujarat, India. International Journal of Environmental Research and Public Health, 19(5), 2707. https://doi.org/10.3390/ijerph19052707