
Accidentally Swallowing a Toothbrush in a Patient during a Vomiting Attempt: Literature Review and Case Report



{kind=link}
{kind=link}
Abstract
1. Introduction
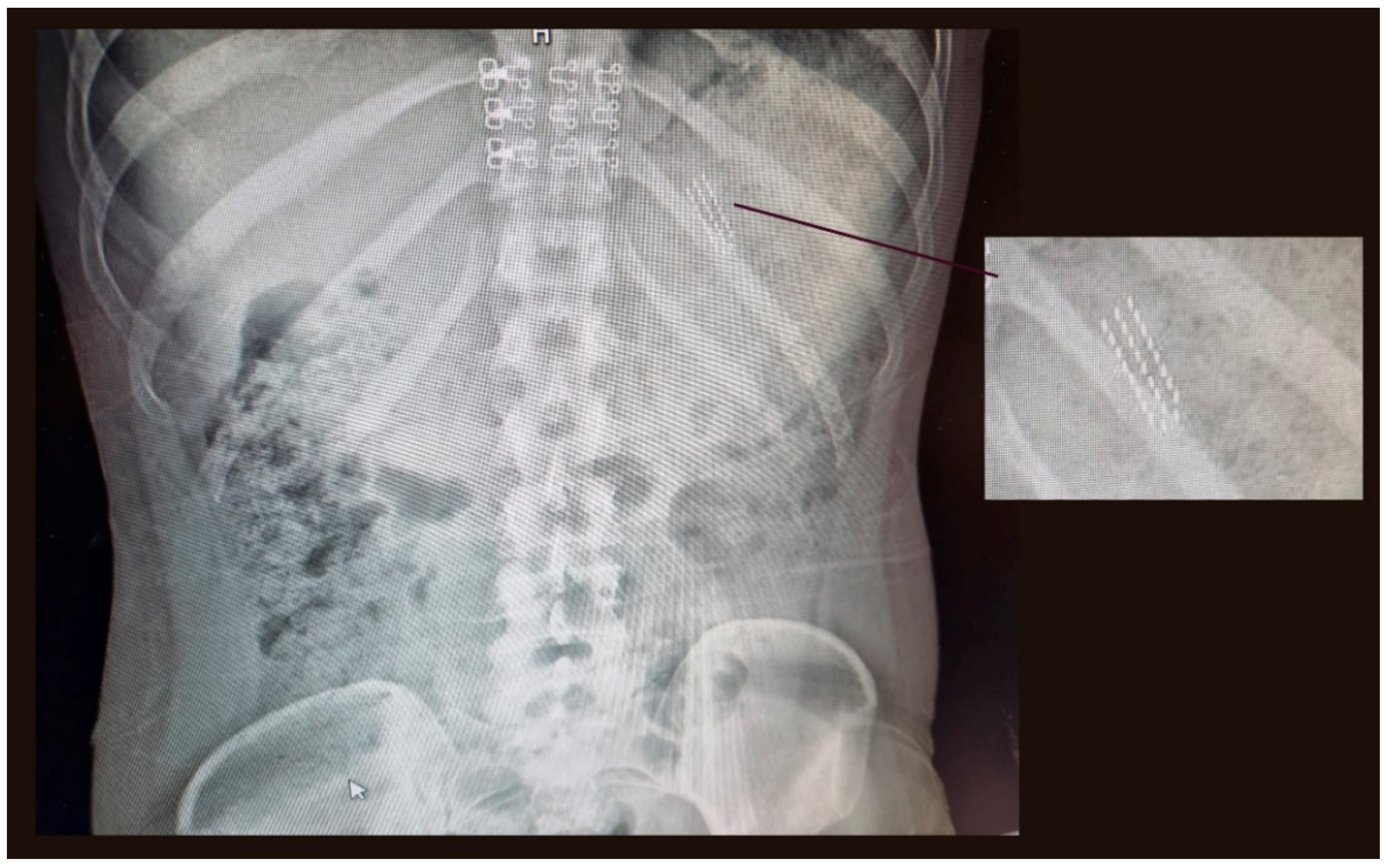
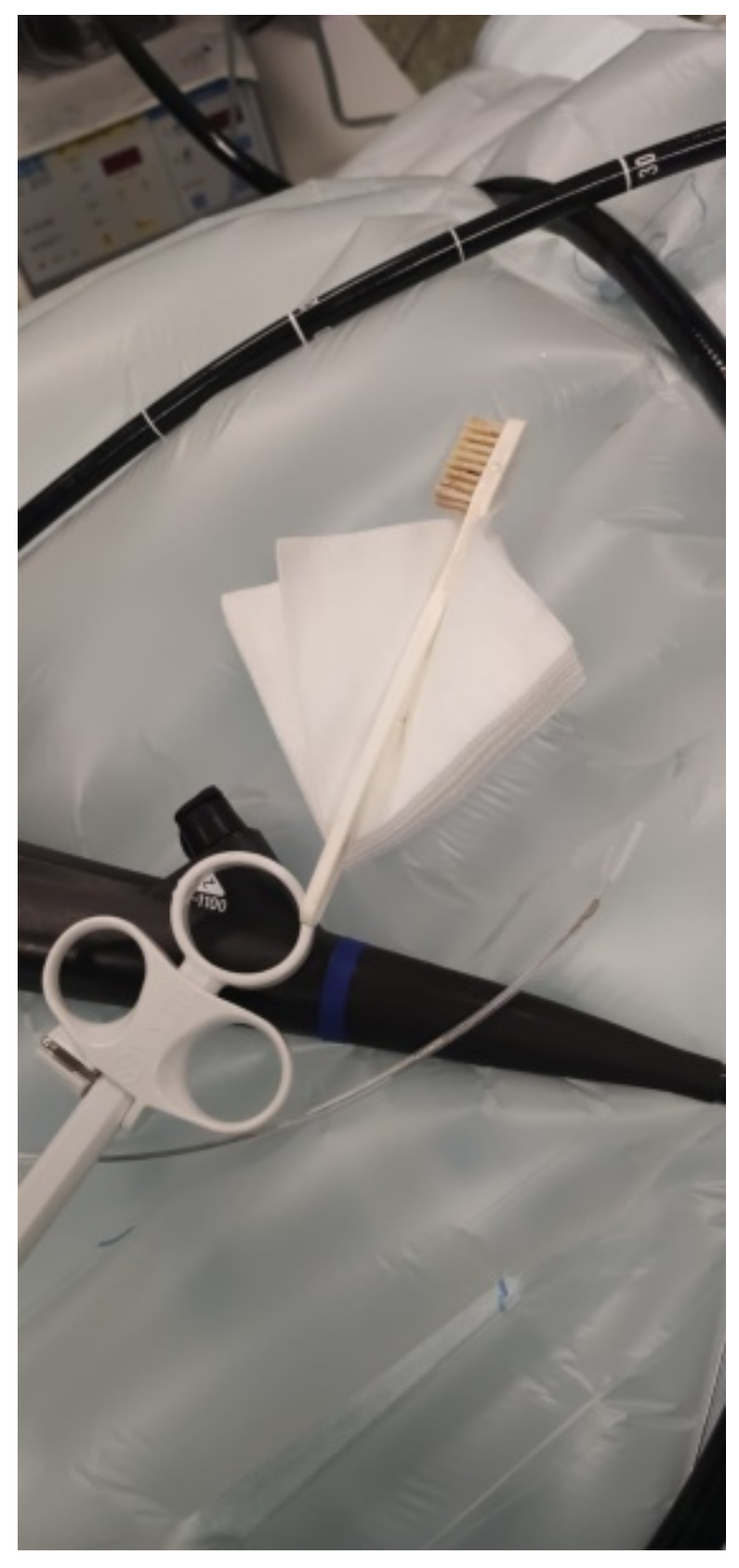
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Niknam, R.; Mahmoudi, L.; Nasseri-Moghaddam, S. An incidentally swallowed toothbrush. Arch. Iran. Med. 2012, 15, 177–178. [Google Scholar] [PubMed]
- Lee, M.R.; Hwang, Y.; Kim, J.H. A case of colohepatic penetration by a swallowed toothbrush. World J. Gastroenterol. 2006, 12, 2464–2465. [Google Scholar] [CrossRef] [PubMed]
- Yaosaka, T.; Chikama, T.; Ishi, S.; Miwa, K.; Murashima, Y. Endoscopic removal of a toothbrush from the second portion of the duodenum. Gastroenterol. Endosc. 1979, 21, 995. [Google Scholar]
- Mokánszki, I.; Adorján, T. Endoscopic removal of a toothbrush from a 13-year-old girl’s stomach. Orv. Hetil. 2002, 143, 1755–1757. [Google Scholar] [PubMed]
- Ertan, A.; Kedia, S.M.; Agrawal, N.M.; Akdamar, K. Endoscopic removal of a toothbrush. Gastrointest. Endosc. 1983, 29, 144–145. [Google Scholar] [CrossRef]
- Wishner, J.D.; Rogers, A.M. Laparoscopic removal of a swallowed toothbrush. Surg. Endosc. 1997, 11, 472–473. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, D.T.; Karamanoukian, H.L.; Glick, P.L. Toothbrush ingestion by bulimics may require laparotomy. J. Pediatr. Surg. 1994, 29, 1596. [Google Scholar] [CrossRef]
- Kirk, A.D.; Bowers, B.A.; Moylan, J.A.; Meyers, W.C. Toothbrush swallowing. Arch. Surg. 1988, 123, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.; Donohue, P.; Costa, V. A swallowed toothbrush causing perforation 2 years after ingestion. Br. J. Hosp. Med. 2007, 68, 559. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Ragnhildstveit, A.; Jackson, L.K.; Cunningham, S.; Good, L.; Tanner, Q.; Roughan, M.; Henrie-Barrus, P. Case Report: Unexpected Remission from Extreme and Enduring Bulimia Nervosa with Repeated Ketamine Assisted Psychotherapy. Front. Psychiatry 2021, 12, 764112. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Wu, Y.; Liu, F.; Zhu, Y.; Jin, H.; Zhang, H.; Wan, Y.; Li, C.; Yu, D. An update on the prevalence of eating disorders in the general population: A systematic review and meta-analysis. Eat. Weight Disord. 2021, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Riddlesberger, M.M.; Cohen, H.L.; Glick, P.L. The swallowed toothbrush: A radiographic clue of bulimia. Pediatr. Radiol. 1991, 21, 262–264. [Google Scholar] [CrossRef] [PubMed]
- Birk, M.; Bauerfeind, P.; Deprez, P.H.; Häfner, M.; Hartmann, D.; Hassan, C.; Hucl, T.; Lesur, G.; Aabakken, L.; Meining, A. Removal of foreign bodies in the upper gastrointestinal tract in adults: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 2016, 48, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, S.B.; Noguera, E.C. Foreign bodies. In The Esophagus, 4th ed.; Castell, D., Richter, J., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2004; pp. 340–353. [Google Scholar]
- Ikenberry, S.O.; Jue, T.L.; Anderson, M.A.; Appalaneni, V.; Banerjee, S.; Ben-Menachem, T.; Decker, G.A.; Fanelli, R.D.; Fisher, L.R.; Fukami, N.; et al. Management of ingested foreing bodies and food impactations: Guideline ASGE. Gastrointest. Endosc. 2011, 73, 1085–1091. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-H.; Cho, S.-I.; Do, N.-Y.; Park, J.-H. A case of pharyngeal injury in a patient with swallowed toothbrush: A case report. BMC Res. Notes 2014, 7, 788. [Google Scholar] [CrossRef] [PubMed]
- Magalhães-Costa, P.; Carvalho, L.; Rodrigues, J.P.; Túlio, M.A.; Marques, S.; Carmo, J.; Bispo, M.; Chagas, C. Endoscopic Management of Foreign Bodies in the Upper Gastrointestinal Tract: An Evidence-Based Review Article. GE Port. J. Gastroenterol. 2015, 23, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Tonkic, A.; Bogdanovic, Z.; Grandić, L. Successful Endoscopic Removal of a Swallowed Toothbrush: Case Report. Case Rep. Gastroenterol. 2011, 5, 122–124. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mesa-López, M.J.; Martínez-Camacho, C.; Mesa, F. Accidentally Swallowing a Toothbrush in a Patient during a Vomiting Attempt: Literature Review and Case Report. Int. J. Environ. Res. Public Health 2022, 19, 2682. https://doi.org/10.3390/ijerph19052682
Mesa-López MJ, Martínez-Camacho C, Mesa F. Accidentally Swallowing a Toothbrush in a Patient during a Vomiting Attempt: Literature Review and Case Report. International Journal of Environmental Research and Public Health. 2022; 19(5):2682. https://doi.org/10.3390/ijerph19052682
Chicago/Turabian StyleMesa-López, Maria José, Carina Martínez-Camacho, and Francisco Mesa. 2022. "Accidentally Swallowing a Toothbrush in a Patient during a Vomiting Attempt: Literature Review and Case Report" International Journal of Environmental Research and Public Health 19, no. 5: 2682. https://doi.org/10.3390/ijerph19052682
APA StyleMesa-López, M. J., Martínez-Camacho, C., & Mesa, F. (2022). Accidentally Swallowing a Toothbrush in a Patient during a Vomiting Attempt: Literature Review and Case Report. International Journal of Environmental Research and Public Health, 19(5), 2682. https://doi.org/10.3390/ijerph19052682