
Displacement and Isolation: Insights from a Mental Stress Survey of Syrian Refugees in Houston, Texas, USA


 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Subject Recruitment
2.2. Measures
2.3. Translations
2.4. Online Survey
2.5. Data Analysis
3. Results
3.1. Demographics
3.2. Survey Scores and Gender
3.3. Correlation Analyses
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nola, S. Legal Protection of Refugees from the Syrian Conflict in the View of International Human Rights. Research Gate. 2022. Available online: https://www.researchgate.net/publication/357553844_LEGAL_PROTECTION_OF_REFUGEES_FROM_THE_SYRIAN_CONFLICT_IN_THE_VIEW_OF_INTERNATIONAL_HUMAN_RIGHTS. (accessed on 1 December 2021).
- Acarturk, C.; Uygun, E.; Ilkkursun, Z.; Yurtbakan, T.; Kurt, G.; Adam-Troian, J.; Senay, I.; Bryant, R.; Cuijpers, P.; Kiselev, N.; et al. Group problem management plus (PM+) to decrease psychological distress among Syrian refugees in Turkey: A pilot randomised controlled trial. BMC Psychiatry 2022, 22, 8. [Google Scholar] [CrossRef] [PubMed]
- Kira, I.A.; Shuwiekh, H.; Rice, K.; Al Ibraheem, B.; Aljakoub, J. A threatened identity: The mental health status of Syrian refugees in Egypt and its etiology. Identity 2017, 17, 176–190. [Google Scholar] [CrossRef]
- Bart, D.B. The Living Conditions and Well-Being of Refugees; United Nations Development Programme: Human Development Reports Research Paper 2009/25 July 2009; UNDP: 2009. Available online: https://mpra.ub.uni-muenchen.de/19208/ (accessed on 1 December 2021).
- Ferris, E.; Winthrop, R. The hidden crisis: Armed conflict and education. In Education and Displacement: Assessing Conditions for Refugees and Internally Displaced Persons Affected by Conflict; Background paper for the EFA Global Monitoring Report 2011; Brookings Institution: Washington, DC, USA, 2010. [Google Scholar]
- Mirza, M.; Luna, R.; Mathews, B.; Hasnain, R.; Hebert, E.; Niebauer, A.; Mishra, U.D. Barriers to healthcare access among refugees with disabilities and chronic health conditions resettled in the US Midwest. J. Immigr. Minor. Heal. 2014, 16, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Tiltnes, Å.A.; Zhang, H.; Pedersen, J. The Living Conditions of Syrian Refugees in Jordan; Fafo: Oslo, Norway, 2019. [Google Scholar]
- Goren, C.; Neter, E. Stereotypical thinking as a mediating factor in the association between exposure to terror and post-traumatic stress disorder symptoms among Israeli youth. Anxiety Stress Coping 2016, 29, 644–659. [Google Scholar] [CrossRef]
- Kijewski, S.; Freitag, M. Civil war and the formation of social trust in Kosovo: Posttraumatic growth or war-related distress? J. Confl. Resolut. 2018, 62, 717–742. [Google Scholar] [CrossRef]
- Kletter, H.; Carrion, V.G. Posttraumatic Stress Disorder in Youth Exposed to War and Terror, in Sleep and Combat-Related Post Traumatic Stress Disorder; Springer: New York, NY, USA, 2018; pp. 363–372. [Google Scholar]
- Miller, K.E.; Rasmussen, A. War exposure, daily stressors, and mental health in conflict and post-conflict settings: Bridging the divide between trauma-focused and psychosocial frameworks. Soc. Sci. Med. 2010, 70, 7–16. [Google Scholar] [CrossRef]
- Steel, Z.; Chey, T.; Silove, D.; Marnane, C.; Bryant, R.A.; van Ommeren, M. Association of torture and other potentially traumatic events with mental health outcomes among populations exposed to mass conflict and displacement: A systematic review and meta-analysis. Jama 2009, 302, 537–549. [Google Scholar] [CrossRef]
- Fino, E.; Mema, D.; Russo, P. War trauma exposed refugees and posttraumatic stress disorder: The moderating role of trait resilience. J. Psychosom. Res. 2020, 129, 109905. [Google Scholar] [CrossRef]
- Gold, P.B.; Engdahl, B.; Eberly, R.E.; Blake, R.J.; Page, W.F.; Frueh, B.C. Trauma exposure, resilience, social support, and PTSD construct validity among former prisoners of war. Soc. Psychiatry Psychiatr. Epidemiol. 2000, 35, 36–42. [Google Scholar] [CrossRef]
- Hanbury, R.F.; Indart, M.J. Resilience Revisited: Toward an Expanding Understanding of Post-Disaster Adaptation. In Resilience in Children, Adolescents, and Adults; Springer: New York, NY, USA, 2013; pp. 213–225. [Google Scholar]
- Sherwood, K.; Liebling-Kalifani, H. A grounded theory investigation into the experiences of African women refugees: Effects on resilience and identity and implications for service provision. J. Int. Women’s Stud. 2012, 13, 86–108. [Google Scholar]
- Vindevogel, S.; Verelst, A. Supporting Mental Health in Young Refugees: A Resilience Perspective. In CHILD, Adolescent and Family Refugee Mental Health; Springer: New York, NY, USA, 2020; pp. 53–65. [Google Scholar]
- Kimerling, R.; Ouimette, P.; Weitlauf, J.C. Gender issues in PTSD. Handb. PTSD Sci. Pract. 2007, 29, 207–228. [Google Scholar]
- Robertson, C.L.; Halcon, L.; Savik, K.; Johnson, D.; Spring, M.; Butcher, J.; Westermeyer, J.; Jaranson, J. Somali and Oromo refugee women: Trauma and associated factors. J. Adv. Nurs. 2006, 56, 577–587. [Google Scholar] [CrossRef]
- Chung, M.C.; AlQarni, N.; Almazrouei, M.; Al Muhairi, S.; Shakra, M.; Mitchell, B.; Al Mazrouei, S.; Al Hashimi, S. Posttraumatic stress disorder and psychiatric co-morbidity among syrian refugees of different ages: The role of trauma centrality. Psychiatr. Q. 2018, 89, 909–921. [Google Scholar] [CrossRef]
- Basheti, I.A.; Ayasrah, S.M.; Basheti, M.M.; Mahfuz, J.; Chaar, B. The Syrian refugee crisis in Jordan: A cross sectional pharmacist-led study assessing post-traumatic stress disorder. Pharm. Pract. 2019, 17, 1475. [Google Scholar] [CrossRef]
- Gwozdziewycz, N.; Mehl-Madrona, L. Meta-analysis of the use of narrative exposure therapy for the effects of trauma among refugee populations. Perm. J. 2013, 17, 70. [Google Scholar]
- Huddy, L.; Feldman, S. Americans respond politically to 9/11: Understanding the impact of the terrorist attacks and their aftermath. Am. Psychol. 2011, 66, 455. [Google Scholar] [CrossRef]
- Powell, T.M.; Shin, O.J.; Li, S.-J.; Hsiao, Y. Post-traumatic stress, social, and physical health: A mediation and moderation analysis of Syrian refugees and Jordanians in a border community. PLoS ONE 2020, 15, e0241036. [Google Scholar] [CrossRef]
- Sartorius, N.; Janca, A. Psychiatric assessment instruments developed by the World Health Organization. Soc. Psychiatry Psychiatr. Epidemiol. 1996, 31, 55–69. [Google Scholar] [CrossRef]
- Beusenberg, M.; Orley, J.H.; Organization W.H.O. A User’s Guide to the Self Reporting Questionnaire (SRQ); World Health Organization: Geneva, Switzerland, 1994. [Google Scholar]
- Ghubash, R.; Daradkeh, T.; El-Rufaie, O.; Abou-Saleh, M. A comparison of the validity of two psychiatric screening questionnaires: The Arabic General Health Questionnaire (AGHQ) and Self-Reporting Questionnaire (SRQ-20) in UAE, using Receiver Operating Characteristic (ROC) analysis. Eur. Psychiatry 2001, 16, 122–126. [Google Scholar] [CrossRef]
- El-Rufaie, O.E.; Absood, G.H. Validity study of the Self-Reporting Questionnaire (SRQ-20) in primary health care in the United Arab Emirates. Int. J. Methods Psychiatr. Res. 1994, 4, 45–53. [Google Scholar]
- Al-Subaie, A.S.; Mohammed, K.; Al-Malik, T. The Arabic self-reporting questionnaire (SRQ) as a psychiatric screening instrument in medical patients. Ann. Saudi Med. 1998, 18, 308–310. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Almadi, T.; Cathers, I.; Mansour, A.M.H.; Chow, C.M. An Arabic version of the perceived stress scale: Translation and validation study. Int. J. Nurs. Stud. 2012, 49, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, A.; Ventevogel, P.; Sancilio, A.; Eggerman, M.; Panter-Brick, C. Comparing the validity of the self reporting questionnaire and the Afghan symptom checklist: Dysphoria, aggression, and gender in transcultural assessment of mental health. BMC Psychiatry 2014, 14, 206. [Google Scholar] [CrossRef]
- Malm, A.; Tinghög, P.; Narusyte, J.; Saboonchi, F. The refugee post-migration stress scale (RPMS)–development and validation among refugees from Syria recently resettled in Sweden. Confl. Health 2020, 14, 2. [Google Scholar] [CrossRef]
- Harpham, T.; Reichenheim, M.; Oser, R.; Thomas, E.; Hamid, N.; Jaswal, S.; Ludermir, A.; Aidoo, M. Measuring mental health in a cost-effective manner. Health Policy Plan. 2003, 18, 344–349. [Google Scholar] [CrossRef]
- Okello, J.; Onen, T.; Musisi, S. Psychiatric disorders among war-abducted and non-abducted adolescents in Gulu district, Uganda: A comparative study. Afr. J. Psychiatry 2007, 10, 225–231. [Google Scholar] [CrossRef][Green Version]
- True, J. The political economy of violence against women: A feminist international relations perspective. Aust. Fem. Law J. 2010, 32, 39–59. [Google Scholar] [CrossRef]
- Alsaba, K.; Kapilashrami, A. Understanding women’s experience of violence and the political economy of gender in conflict: The case of Syria. Reprod. Health Matters 2016, 24, 5–17. [Google Scholar] [CrossRef]
- Hashimoto-Govindasamy, L.; Rose, V. An ethnographic process evaluation of a community support program with Sudanese refugee women in western Sydney. Health Promot. J. Aust. 2011, 22, 107–112. [Google Scholar] [CrossRef]
- Baird, M.B. Well-being in refugee women experiencing cultural transition. Adv. Nurs. Sci. 2012, 35, 249–263. [Google Scholar] [CrossRef]
- Deacon, Z.; Sullivan, C. Responding to the complex and gendered needs of refugee women. Affilia 2009, 24, 272–284. [Google Scholar] [CrossRef]
- Shishehgar, S.; Gholizadeh, L.; DiGiacomo, M.; Green, A.; Davidson, P.M. Health and socio-cultural experiences of refugee women: An integrative review. J. Immigr. Minority Health 2017, 19, 959–973. [Google Scholar] [CrossRef]
- Tinghög, P.; Al-Saffar, S.; Carstensen, J.; Nordenfelt, L. The association of immigrant-and non-immigrant-specific factors with mental ill health among immigrants in Sweden. Int. J. Soc. Psychiatry 2010, 56, 74–93. [Google Scholar] [CrossRef]
- Phillimore, J. Refugees, acculturation strategies, stress and integration. J. Soc. Policy 2011, 40, 575–593. [Google Scholar] [CrossRef]
- Straiton, M.L.; Ledesma, H.M.L.; Donnelly, T.T. A qualitative study of Filipina immigrants’ stress, distress and coping: The impact of their multiple, transnational roles as women. BMC Women’s Health 2017, 17, 72. [Google Scholar] [CrossRef]
- Pavlish, C. Narrative inquiry into life experiences of refugee women and men. Int. Nurs. Rev. 2007, 54, 28–34. [Google Scholar] [CrossRef]
- Falco, G.; Pirro, P.S.; Castellano, E.; Anfossi, M.; Borretta, G.; Gianotti, L. The relationship between stress and diabetes mellitus. J. Neurol. Psychol. 2015, 3, 7. [Google Scholar]
- Kretchy, I.A.; Owusu-Daaku, F.T.; Danquah, S.A. Mental health in hypertension: Assessing symptoms of anxiety, depression and stress on anti-hypertensive medication adherence. Int. J. Ment. Health Syst. 2014, 8, 25. [Google Scholar] [CrossRef]
- Lloyd, C.; Smith, J.; Weinger, K. Stress and diabetes: A review of the links. Diabetes Spectr. 2005, 18, 121–127. [Google Scholar] [CrossRef]
- Zimmerman, R.; Frohlich, E. Stress and hypertension. J. Hypertension. Suppl. Off. J. Int. Soc. Hypertens. 1990, 8, S103–S107. [Google Scholar]
- Whitehead, W.E.; Crowell, M.D.; Robinson, J.C.; Heller, B.R.; Schuster, M.M. Effects of stressful life events on bowel symptoms: Subjects with irritable bowel syndrome compared with subjects without bowel dysfunction. Gut 1992, 33, 825–830. [Google Scholar] [CrossRef] [PubMed]
- Mayer, E.A.; Naliboff, B.D.; Chang, L.; Coutinho, S.V.V. Stress and irritable bowel syndrome. Am. J. Physiol. Gastrointest. Liver Physiol. 2001, 280, G519–G524. [Google Scholar] [CrossRef] [PubMed]
- Acarturk, C.; Cetinkaya, M.; Senay, I.; Gulen, B.; Aker, T.; Hinton, D. Prevalence and predictors of posttraumatic stress and depression symptoms among Syrian refugees in a refugee camp. J. Nerv. Ment. Dis. 2018, 206, 40–45. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Male | Female | Statistics | p-Value | |
|---|---|---|---|---|---|
| (n = 93) | (n = 38) | (n = 55) | |||
| M (SD)/% [%] | |||||
| Demographics | |||||
| Age | 36.11 (9.85) | 37.37 (11.15) | 35.22 (8.82) | 1.03 | 0.306 |
| Age group | 6.9265 | 0.0313 | |||
| ≤25 | 17.39 (16) | 21.05 (8) | 14.81 (8) | ||
| 26–39 | 42.39 (39) | 26.32 (10) | 53.70 (29) | ||
| ≥40 | 40.22 (37) | 52.63 (20) | 31.48 (17) | ||
| What is your highest level of education? | 3.7302 | 0.0534 | |||
| Did not complete high school | 56.52 (52) | 68.42 (26) | 48.15 (26) | ||
| GED/High School and above | 43.48 (40) | 31.58 (12) | 51.85 (28) | ||
| Are you currently employed more than 15 h per week? | 0.6552 | 0.4183 | |||
| Yes | 25.27 (23) | 29.73 (11) | 22.22 (12) | ||
| No | 74.73 (68) | 70.27 (26) | 77.78 (42) | ||
| What is your current relationship status? | 0.0063 | 0.9366 | |||
| Married | 79.35 (73) | 78.95 (30) | 79.63 (43) | ||
| All others | 20.65 (19) | 21.05 (8) | 20.37(11) | ||
| Are you currently living with a spouse/partner? | 0.1779 | 0.6732 | |||
| Yes | 83.52 (76) | 81.58 (31) | 84.91 (45) | ||
| No | 16.48 (15) | 18.42 (7) | 15.09 (8) | ||
| Is your partner or spouse employed for more than 15 h a week? | 3.1249 | 0.0771 | |||
| Yes | 31.51 (23) | 20.00 (6) | 39.53 (17) | ||
| No | 68.49 (50) | 80.00 (24) | 60.47 (26) | ||
| What is your approximate total household income? Include all sources. | 4.3298 | 0.0375 | |||
| less than $10,000 | 60.23 (53) | 72.97 (27) | 50.98 (26) | ||
| $10,000 or above | 39.77 (35) | 27.03 (10) | 49.02 (25) | ||
| How many children live in your household? | 4.2 (2.06) | 4.03 (1.95) | 4.33 (2.15) | −0.67 | 0.5068 |
| Do you have medical insurance? | 0.0666 | 0.7964 | |||
| Yes | 80.22 (73) | 78.95 (30) | 81.13 (43) | ||
| No | 19.78 (18) | 21.05 (8) | 18.87 (10) | ||
| Have you been diagnosed with any of the following? Check all that apply: | |||||
| Diabetes mellitus | 10.75 (10) | 7.89 (3) | 12.73 (7) | 0.5469 | 0.519 |
| Hypertension | 9.68 (9) | 7.89 (3) | 10.91 (6) | 0.2336 | 0.733 |
| Hypothroidism | 9.78 (9) | 5.26 (2) | 12.96 (7) | 1.4983 | 0.2978 |
| Asthma | 5.38 (5) | 5.26 (2) | 5.45 (3) | 0.0016 | 1 |
| Irritable bowel syndrome | 12.9 (12) | 13.16 (5) | 12.73 (7) | 0.0037 | 1 |
| Number of Health Issues | 0.48 (0.73) | 0.39 (0.72) | 0.55 (0.74) | −0.98 | 0.3314 |
| Do you smoke cigarettes? | 31.2903 | <0.0001 | |||
| Never | 78.49 (73) | 50.00 (19) | 98.18 (54) | ||
| I was (Quit) | 4.3 (4) | 10.53 (4) | 0 (0) | ||
| Occasionally | 4.3 (4) | 10.53 (4) | 0 (0) | ||
| Less than 10 cigarettes per day | 7.53 (7) | 15.79 (6) | 1.82 (1) | ||
| More than 10 cigarettes per day | 5.38 (5) | 13.16 (5) | 0 (0) | ||
| Do you smoke Hookah? | 2.2589 | 0.7113 | |||
| Never | 86.02 (80) | 84.21 (32) | 87.27 (58) | ||
| I was (Quit) | 1.08 (1) | 2.63 (1) | 0 (0) | ||
| Occasionally | 11.83 (11) | 13.16 (5) | 10.91 (6) | ||
| Daily | 1.08 (1) | 0 (0) | 1.82 (1) | ||
| Stress Measurements | |||||
| General Mental Health (possible range: 0–20) | 4.37 (4.27) | 3.47 (3.81) | 5.09 (4.50) | −1.78 | 0.0791 |
| Perceived Stress Sale (possible range: 0–56) | 23.74 (8.72) | 23.64 (7.85) | 23.87 (9.46) | −0.12 | 0.9049 |
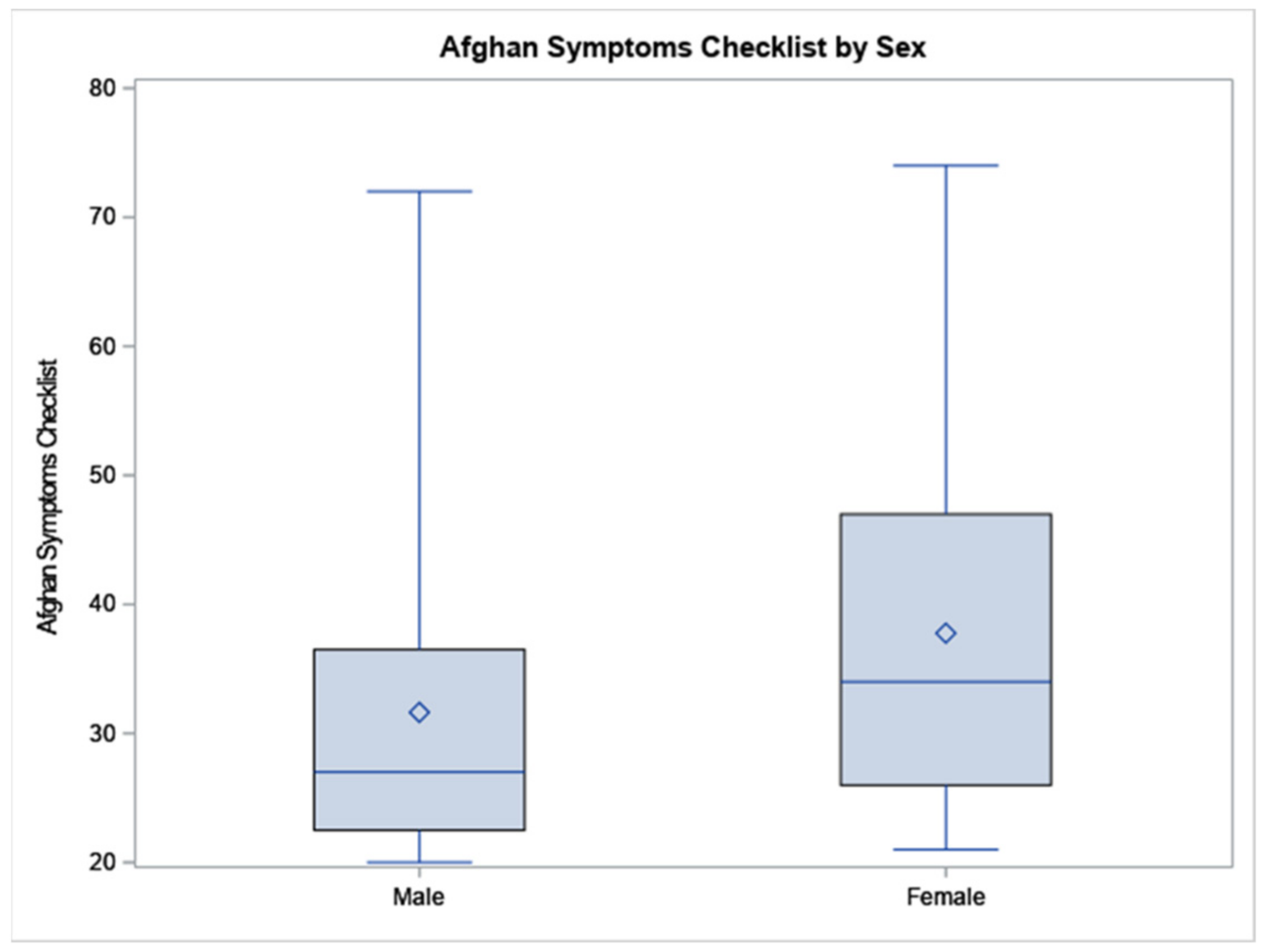
| Afghan Symptoms (possible range: 20–100) | 35.29 (14.18) | 31.64 (12.82) | 37.78 (14.73) | −2.04 | 0.0446 |
| Sadness with Social Withdrawal (possible range: 15–75) | 27 (10.82) | 24.31 (10.01) | 28.89 (11.12) | −1.99 | 0.0495 |
| Fishar Ruminative Sadness (possible range: 2–10) | 4.09 (2.29) | 3.64 (2.09) | 4.36 (2.39) | −1.46 | 0.1467 |
| Stress-Induced Reactivity (possible range: 4–20) | 5.88 (2.53) | 4.86 (1.51) | 6.56 (2.86) | −3.65 | 0.0004 |
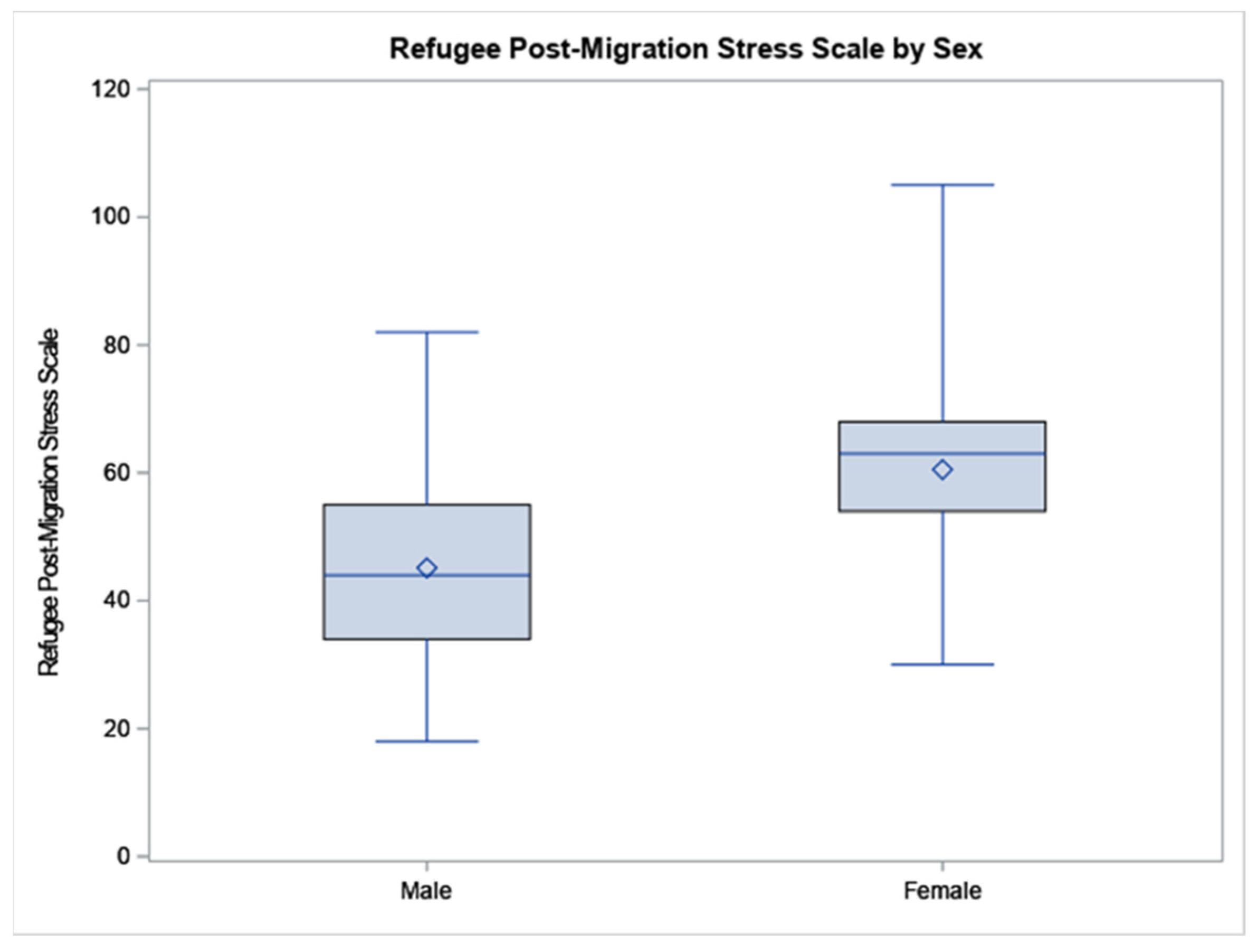
| Refugee Post-Migration Stress Scale (possible range: 21–105) | 54.42 (17.30) | 45.15 (17.53) | 60.54 (13.91) | −3.23 | 0.0022 |
| Perceived Discrimination (possible range: 4–20) | 6.91 (3.62) | 6 (2.77) | 7.33 (4.01) | −1.11 | 0.2721 |
| Lack of Host Country-Specific Competences (possible range: 3–15) | 10 (4.01) | 9.08 (3.82) | 11.05 (3.58) | −1.7 | 0.0961 |
| Material and Economic Strain (possible range: 3–15) | 8.15 (3.73) | 7.91 (4.09) | 8.82 (3.44) | −0.74 | 0.46 |
| Loss of Home Country (possible range: 3–15) | 11.96 (3.55) | 11.09 (2.47) | 12.97 (3.04) | −1.88 | 0.0657 |
| Family and Home Country Concerns (possible range: 2–10) | 8.02 (2.71) | 7.73 (2.20) | 8.62 (2.38) | −1.11 | 0.2723 |
| Social Strain (possible range: 3–15) | 7.15 (3.66) | 5.18 (3.40) | 8.08 (3.57) | −2.4 | 0.0204 |
| Family Conflicts (possible range: 3–15) | 3.88 (2.29) | 4 (1.76) | 3.97 (2.56) | 0.03 | 0.9745 |
| Gender (ref: Male) | Age | Education (ref: Did Not Complete High School) | Employment (ref: No) | Married (ref: All Others) | Living Partner (ref: No) | Partner Employment Status (ref: No) | Family Income (ref: Less than $10,000) | Number of Children Living in Your Household | Health Insurance Status (ref: No) | Number of Health Issues | Smoke Cigarettes (ref: Never) | Hookah Use (ref: Never) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Self-Reporting Questionnaire | r | 0.186 | 0.037 | −0.100 | 0.007 | 0.041 | 0.123 | 0.140 | 0.249 | 0.004 | 0.028 | 0.369 | −0.039 | 0.140 |
| p | 0.079 | 0.733 | 0.351 | 0.948 | 0.700 | 0.251 | 0.244 | 0.021 | 0.968 | 0.799 | 0.000 | 0.716 | 0.189 | |
| Perceived Stress Sale | r | 0.013 | 0.078 | −0.157 | 0.016 | 0.128 | 0.288 | −0.170 | 0.205 | 0.148 | −0.045 | 0.195 | 0.070 | 0.164 |
| p | 0.905 | 0.468 | 0.142 | 0.880 | 0.233 | 0.006 | 0.157 | 0.060 | 0.181 | 0.676 | 0.068 | 0.516 | 0.126 | |
| Afghan Symptoms | r | 0.212 | 0.026 | −0.030 | 0.136 | 0.019 | 0.071 | 0.020 | 0.277 | 0.160 | −0.004 | 0.289 | −0.089 | 0.086 |
| p | 0.045 | 0.809 | 0.779 | 0.205 | 0.856 | 0.506 | 0.866 | 0.010 | 0.142 | 0.970 | 0.006 | 0.406 | 0.421 | |
| Sadness with Social Withdrawal | r | 0.208 | 0.029 | −0.017 | 0.124 | 0.038 | 0.072 | 0.042 | 0.265 | 0.166 | 0.024 | 0.280 | −0.091 | 0.060 |
| p | 0.050 | 0.784 | 0.874 | 0.247 | 0.723 | 0.504 | 0.727 | 0.014 | 0.129 | 0.822 | 0.008 | 0.392 | 0.574 | |
| Fishar Ruminative Sadness | r | 0.155 | 0.003 | −0.085 | 0.189 | 0.040 | 0.082 | 0.015 | 0.300 | 0.104 | −0.010 | 0.269 | 0.033 | 0.113 |
| p | 0.147 | 0.981 | 0.426 | 0.078 | 0.713 | 0.449 | 0.898 | 0.005 | 0.344 | 0.927 | 0.011 | 0.761 | 0.290 | |
| Stress Induced Reactivity | r | 0.328 | 0.016 | 0.020 | 0.044 | −0.100 | 0.010 | −0.036 | 0.198 | 0.153 | −0.115 | 0.241 | −0.224 | 0.151 |
| p | 0.002 | 0.879 | 0.850 | 0.684 | 0.347 | 0.929 | 0.762 | 0.068 | 0.162 | 0.288 | 0.022 | 0.034 | 0.155 | |
| Refugee Post-Migration Stress Scale | r | 0.416 | 0.154 | −0.078 | −0.049 | 0.137 | 0.349 | 0.196 | 0.127 | 0.136 | 0.100 | 0.297 | −0.044 | 0.099 |
| p | 0.002 | 0.275 | 0.585 | 0.729 | 0.333 | 0.012 | 0.225 | 0.385 | 0.350 | 0.492 | 0.033 | 0.757 | 0.484 | |
| Perceived Discrimination | r | 0.155 | 0.048 | −0.073 | 0.209 | −0.089 | 0.151 | 0.021 | 0.192 | 0.439 | −0.038 | 0.265 | −0.051 | 0.007 |
| p | 0.272 | 0.737 | 0.610 | 0.138 | 0.532 | 0.290 | 0.899 | 0.187 | 0.002 | 0.795 | 0.057 | 0.720 | 0.963 | |
| Lack of Host Country Competences | r | 0.233 | 0.058 | −0.186 | 0.103 | 0.104 | 0.191 | −0.029 | 0.159 | −0.058 | −0.114 | 0.043 | 0.105 | 0.051 |
| p | 0.096 | 0.684 | 0.191 | 0.466 | 0.461 | 0.179 | 0.858 | 0.275 | 0.691 | 0.429 | 0.761 | 0.460 | 0.721 | |
| Material and Economic Strain | r | 0.107 | 0.074 | −0.146 | 0.054 | −0.068 | 0.064 | 0.214 | 0.153 | 0.030 | −0.133 | 0.127 | 0.248 | −0.004 |
| p | 0.460 | 0.612 | 0.316 | 0.711 | 0.639 | 0.664 | 0.191 | 0.304 | 0.841 | 0.368 | 0.381 | 0.082 | 0.979 | |
| Loss of Home Country | r | 0.262 | 0.183 | −0.222 | −0.128 | 0.346 | 0.243 | 0.045 | −0.014 | −0.025 | 0.199 | 0.175 | 0.174 | 0.030 |
| p | 0.066 | 0.203 | 0.125 | 0.377 | 0.014 | 0.093 | 0.788 | 0.927 | 0.866 | 0.174 | 0.225 | 0.226 | 0.838 | |
| Family and Home Country Concerns | r | 0.158 | 0.114 | −0.267 | 0.082 | 0.456 | 0.402 | 0.116 | 0.182 | 0.051 | 0.399 | 0.221 | 0.159 | 0.009 |
| p | 0.272 | 0.431 | 0.063 | 0.573 | 0.001 | 0.004 | 0.481 | 0.222 | 0.732 | 0.005 | 0.123 | 0.271 | 0.949 | |
| Social Strain | r | 0.327 | 0.040 | −0.082 | 0.076 | 0.046 | 0.346 | 0.233 | 0.306 | −0.011 | 0.173 | 0.226 | 0.296 | 0.162 |
| p | 0.020 | 0.783 | 0.575 | 0.598 | 0.749 | 0.015 | 0.153 | 0.036 | 0.940 | 0.241 | 0.115 | 0.037 | 0.260 | |
| Family Conflicts | r | −0.005 | 0.040 | −0.037 | 0.352 | −0.339 | 0.026 | 0.033 | 0.225 | 0.495 | −0.152 | 0.110 | −0.034 | 0.222 |
| p | 0.975 | 0.791 | 0.808 | 0.016 | 0.021 | 0.867 | 0.849 | 0.137 | 0.001 | 0.320 | 0.466 | 0.825 | 0.138 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Atrooz, F.; Chen, T.A.; Biekman, B.; Alrousan, G.; Bick, J.; Salim, S. Displacement and Isolation: Insights from a Mental Stress Survey of Syrian Refugees in Houston, Texas, USA. Int. J. Environ. Res. Public Health 2022, 19, 2547. https://doi.org/10.3390/ijerph19052547
Atrooz F, Chen TA, Biekman B, Alrousan G, Bick J, Salim S. Displacement and Isolation: Insights from a Mental Stress Survey of Syrian Refugees in Houston, Texas, USA. International Journal of Environmental Research and Public Health. 2022; 19(5):2547. https://doi.org/10.3390/ijerph19052547
Chicago/Turabian StyleAtrooz, Fatin, Tzuan A. Chen, Brian Biekman, Ghalya Alrousan, Johanna Bick, and Samina Salim. 2022. "Displacement and Isolation: Insights from a Mental Stress Survey of Syrian Refugees in Houston, Texas, USA" International Journal of Environmental Research and Public Health 19, no. 5: 2547. https://doi.org/10.3390/ijerph19052547
APA StyleAtrooz, F., Chen, T. A., Biekman, B., Alrousan, G., Bick, J., & Salim, S. (2022). Displacement and Isolation: Insights from a Mental Stress Survey of Syrian Refugees in Houston, Texas, USA. International Journal of Environmental Research and Public Health, 19(5), 2547. https://doi.org/10.3390/ijerph19052547