
Understanding Trustful Relationships between Community Health Workers and Vulnerable Citizens during the COVID-19 Pandemic: A Realist Evaluation




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Ethics
2.3. Study Design
2.4. Recruitment of Participants, Data Collection, and Data Analysis
3. Results
3.1. Study Participants
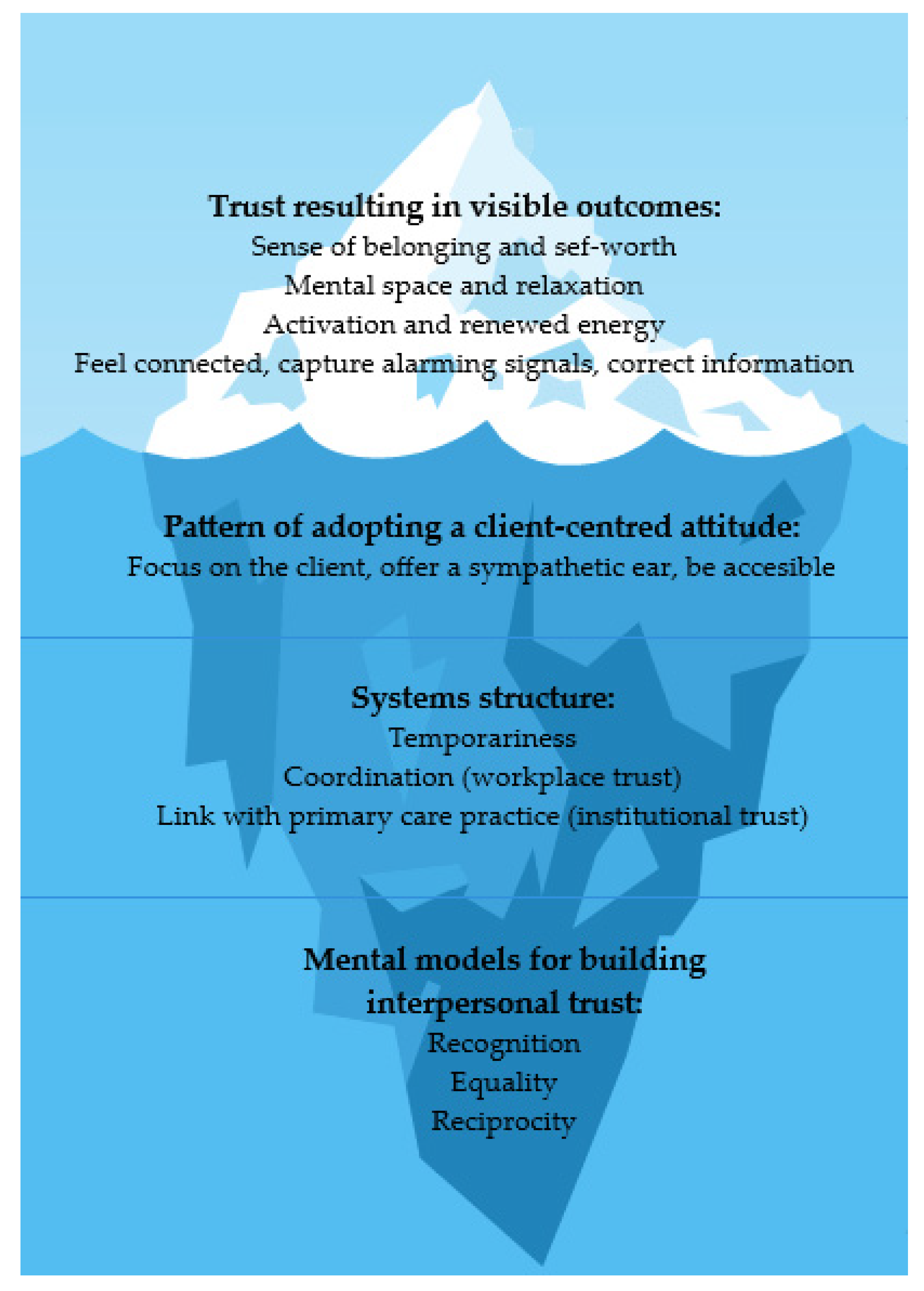
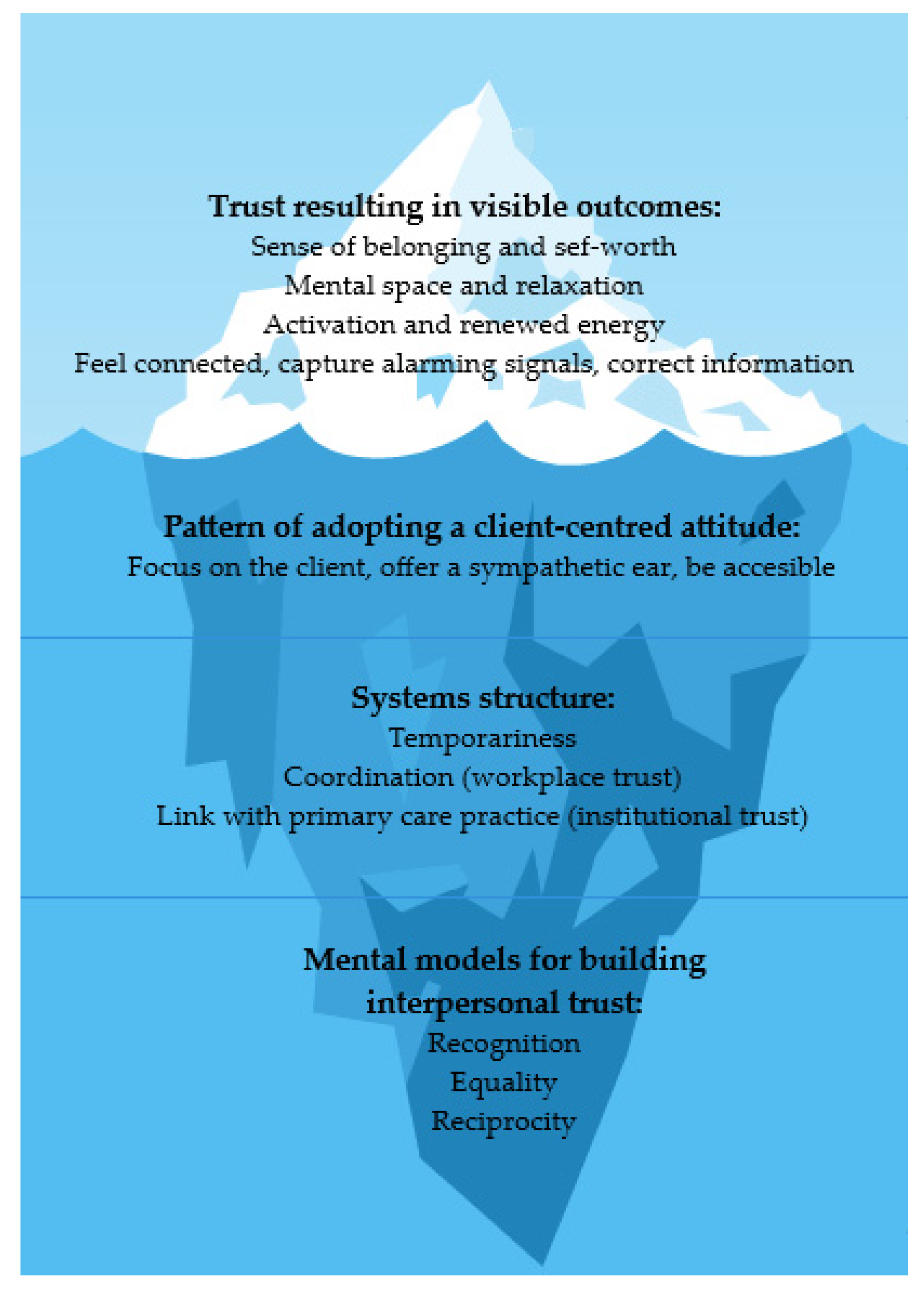
3.2. Outcomes of the Intervention
She also said, ah, I am not alone. Someone gave my phone number to someone. I am not alone in life, after all. We are human, and we need this.(CHW 1)
Then I thought, “Yes, I see someone.” I had not seen anyone for three weeks, and suddenly someone was standing there smiling for you, and he just asked: “Can I do something for you?” ... That gives the feeling of “Yes, I count in this society!”. And look, just, someone standing at your door, a laugh.(Client 1)
I felt that it was a relief for her that there was someone just to eat together with or take a walk.(CHW 2)
The first time I remember well, she had a bowl of strawberries with her. And we ate half of it. And we have been chatting a bit about my kids. Time flew by.(Client 3)
We talked about everything. We went for a walk 3 or 4 times. I was happy, and I needed that. I had to walk and move. I needed air. I needed a slight push, and she was. After that, I also started exercising several times.(Client 2)
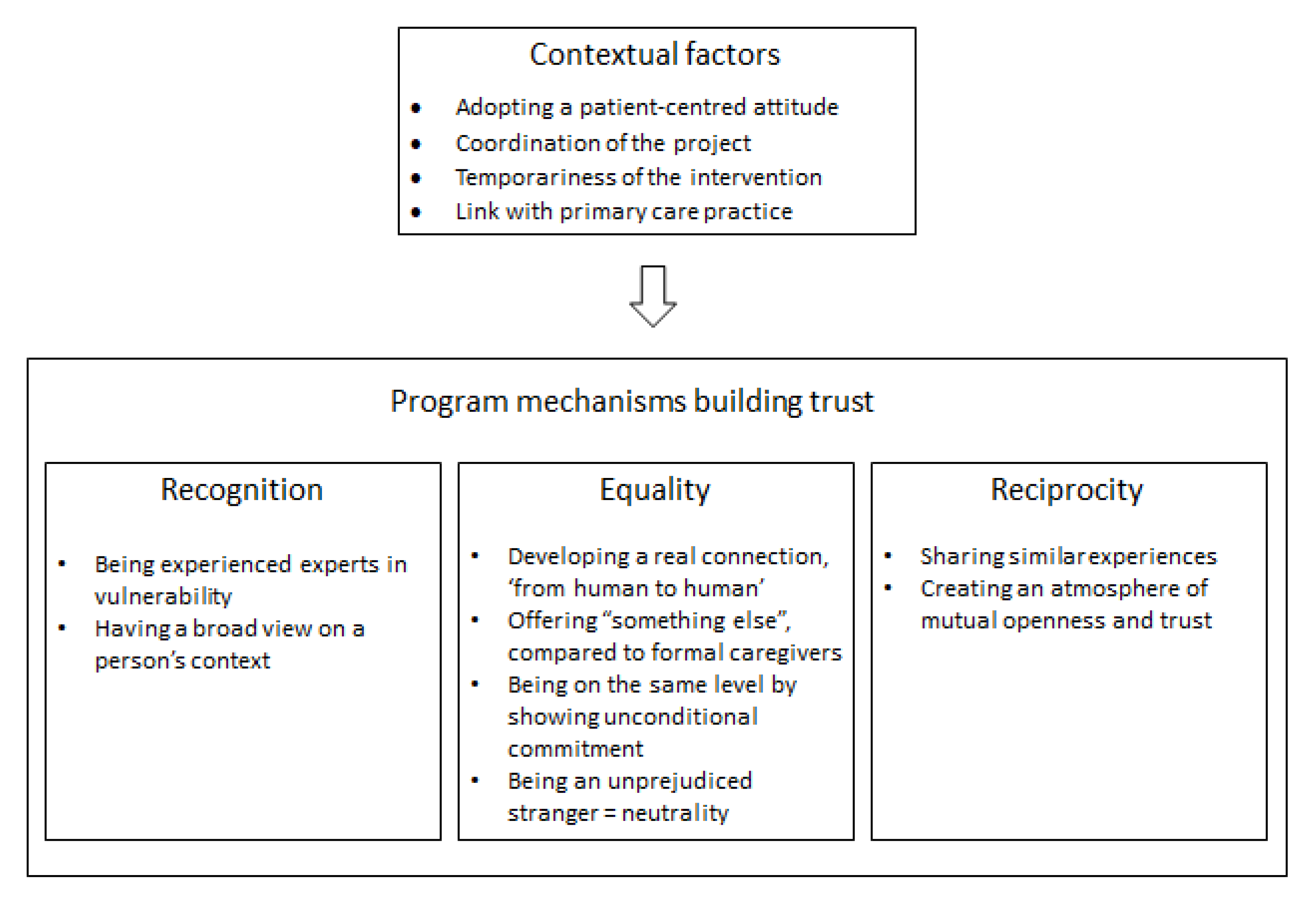
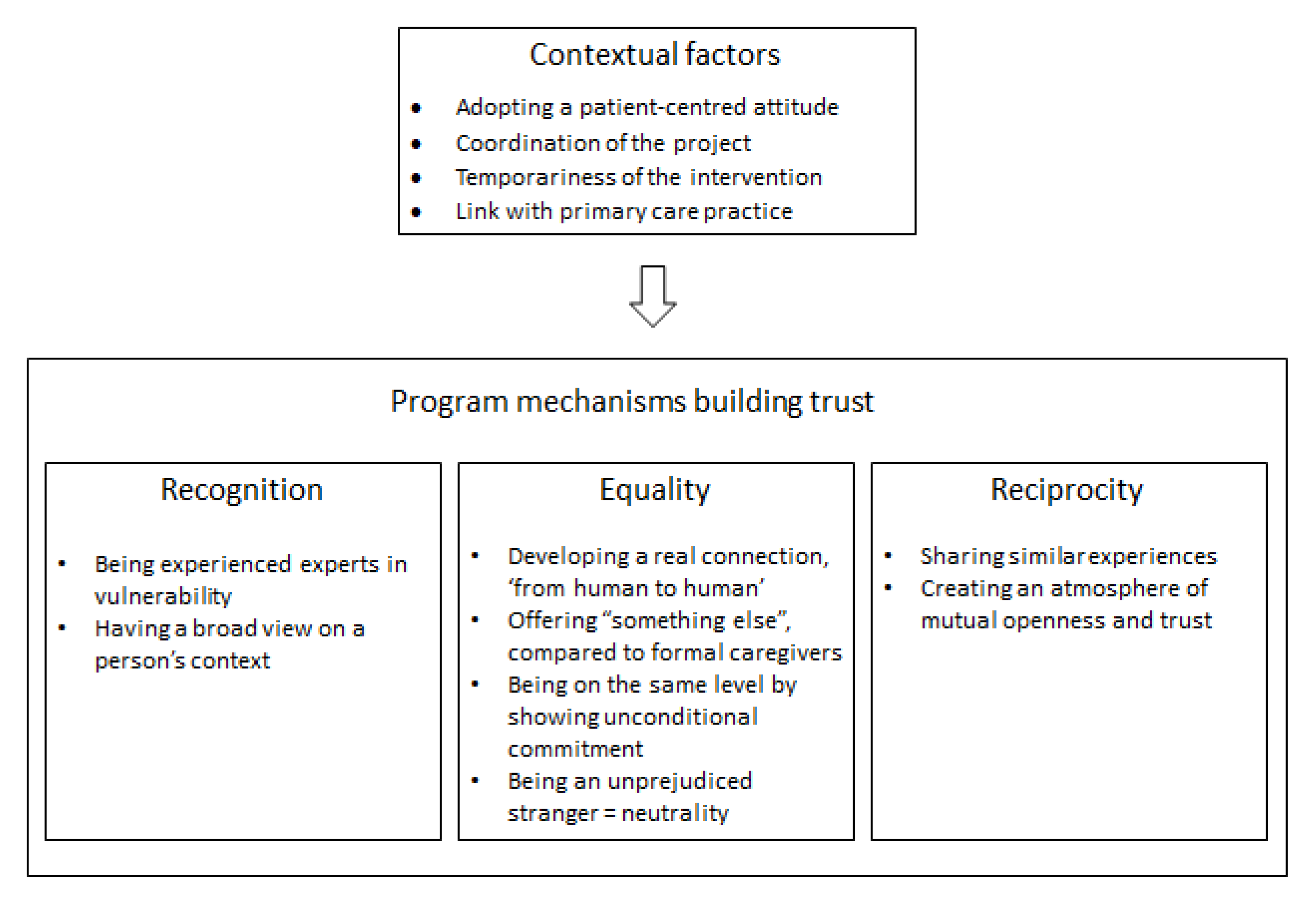
3.3. The Program Mechanisms That Produce Outcomes
3.3.1. Recognition
I also have a background. I am actually an expert in poverty and social exclusion. I have experienced well, by being honest myself and by trying to create trust, that it is a nice interaction. I think it helps me very well. I’ve been through a lot of things myself, and I think people feel that when you’re with them. It’s relatable. They see that, and they feel that.(CHW 3)
I don’t mind that at all, but I really don’t have any experience with that at all. Sometimes I felt a bit incompetent. I did know that a social worker also came to visit him. But I sometimes felt more like I was sitting in the chair as the psychiatrist (nervous chuckle), and that I had to hear him out about his problems, but that I didn’t know what to ask for or what to say.(CHW 4)
For example, by going with that person to a hospital. And while waiting, when the door is open, you can already see that this person has probably had a hard time due to Corona. Or when you walk to the bus together with that person, while talking, then you hear that that person didn’t eat that day. That person doesn’t have one problem; health. But that person has so many other problems.(CHW 3)
3.3.2. Equality
I think it’s mostly the fact that ordinary people can help. That she also felt “That’s not a doctor or nurse here but just someone who calls to ask how I’m doing”.(CHW 2)
I’m voluntary. I only come to listen and to chat. That is something different from what you (professional caregivers) can already give to that lady. I’ll give something else. I am a human being, she tells what is on her mind. And I try to listen and say something once at a time—but in the meantime, I’m not deciding about her life.(CHW 1)
I think the big difference lies in the fact that the contact is from person to person. There’s nothing attached to it. It costs zero euros. Nothing is obligatory. It’s not a mandatory therapy and you shouldn’t get anywhere. It is non-committal. It is authentic. I think there is a very big difference there, that you have that buffer. That you are not immediately professionally valued as “Something is wrong with you”.(CHW 5)
The doctor-patient relationship is something else. They’re higher. She just says X and I say Y. There is no title. I mean, there’s no hierarchical difference. We just sit on a bench together to chat.(CHW 6)
I think that does give more confidence. Because we’re just going somewhere next to and with those people. And sometimes it scares people off when you say “I’m a doctor”. I think people might automatically start to conceal things or their lifestyle. I have found that people speak more easily. Like when walking: we walk next to each other, it is quiet and automatically they tell something more. Then sometimes things come up.(CHW 3)
I think the barrier is smaller for some people. That they can tell someone else about their concerns instead of their own children or their partner, who have already heard it all. I think sometimes it’s easier to be open to people who aren’t that close to you.(CHW 2)
Another person (an outsider) just listens and another person will not draw any conclusions or judge.(CHW 7)
3.3.3. Reciprocity
That creates a bond. They say something, and you say something. That makes us equal.(CHW 8)
Yes, there were similar things. And that she also heard that I was also afraid, I was also scared. No one knew in the beginning what that Corona was. And yes, I know very well what it is to be alone. I’m actually alone too... That one woman I mentored, I really did feel that pain from her. And I think it’s because of that, because I knew what it was, that it was possible to listen to her, to let her tell and to gain confidence. Because I also once dared to say: I know what it is, to be alone. You still feel safer to talk further. I think that’s a surplus.(CHW 3)
3.4. The Contextual Factors That Support the Program Mechanisms
- Adopting a client-centered attitude
- Coordination of the intervention
- The temporariness of the intervention
- Link with the primary care practice
I think you have stronger foundations. First, you know there are people standing next to you. The case will be resolved. Then, you are already feeling more secure to go to that person next time. The more information you get, the more knowledge and insight you get.(CHW 9)
This way, it is possible for me to keep it bearable in terms of time use. If I were there for three to four hours, that would be too much for me. And then maybe, from what I think I can add, I would lose my strength.(CHW 8)
4. Discussion
4.1. Program Theory
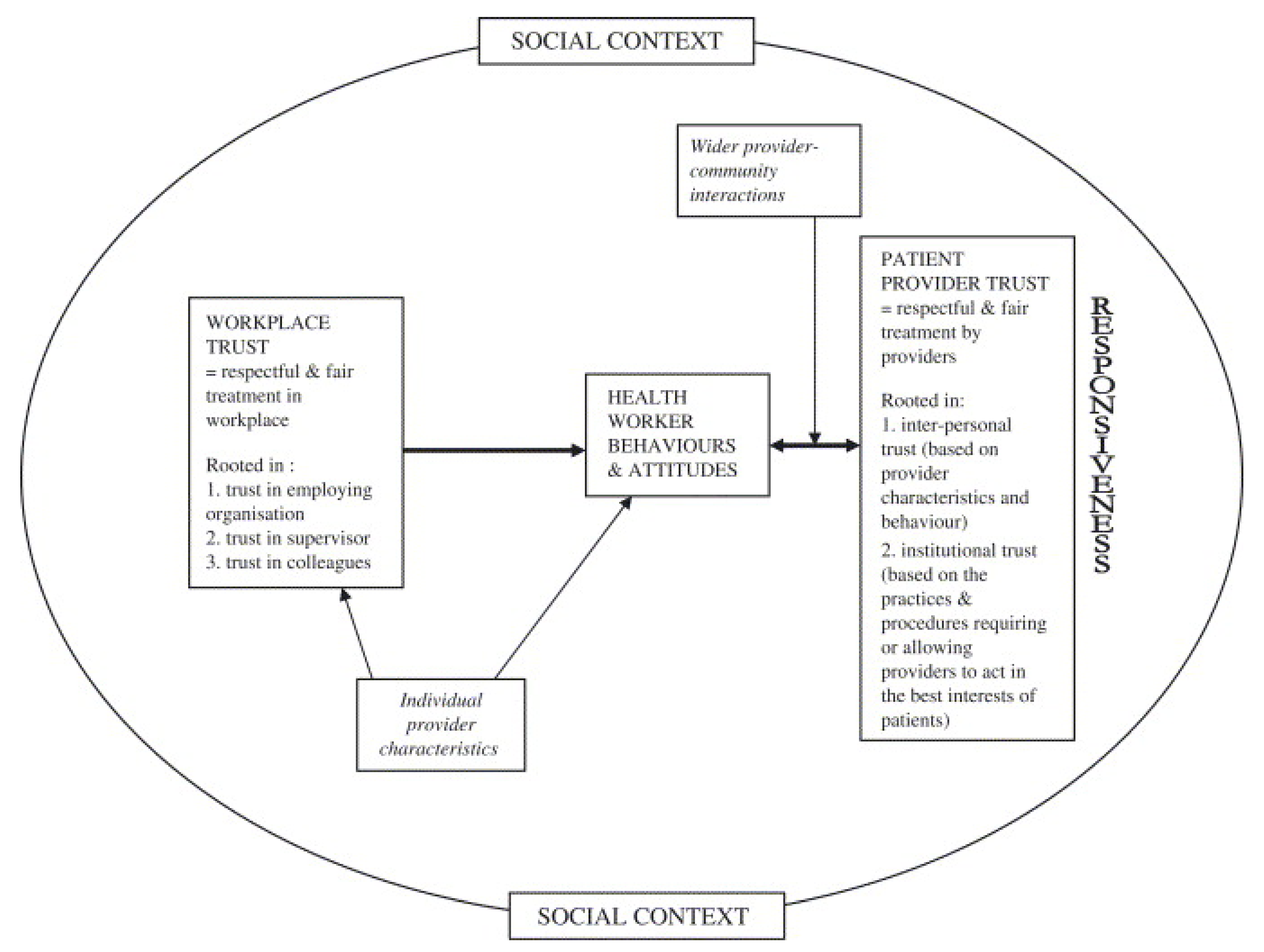
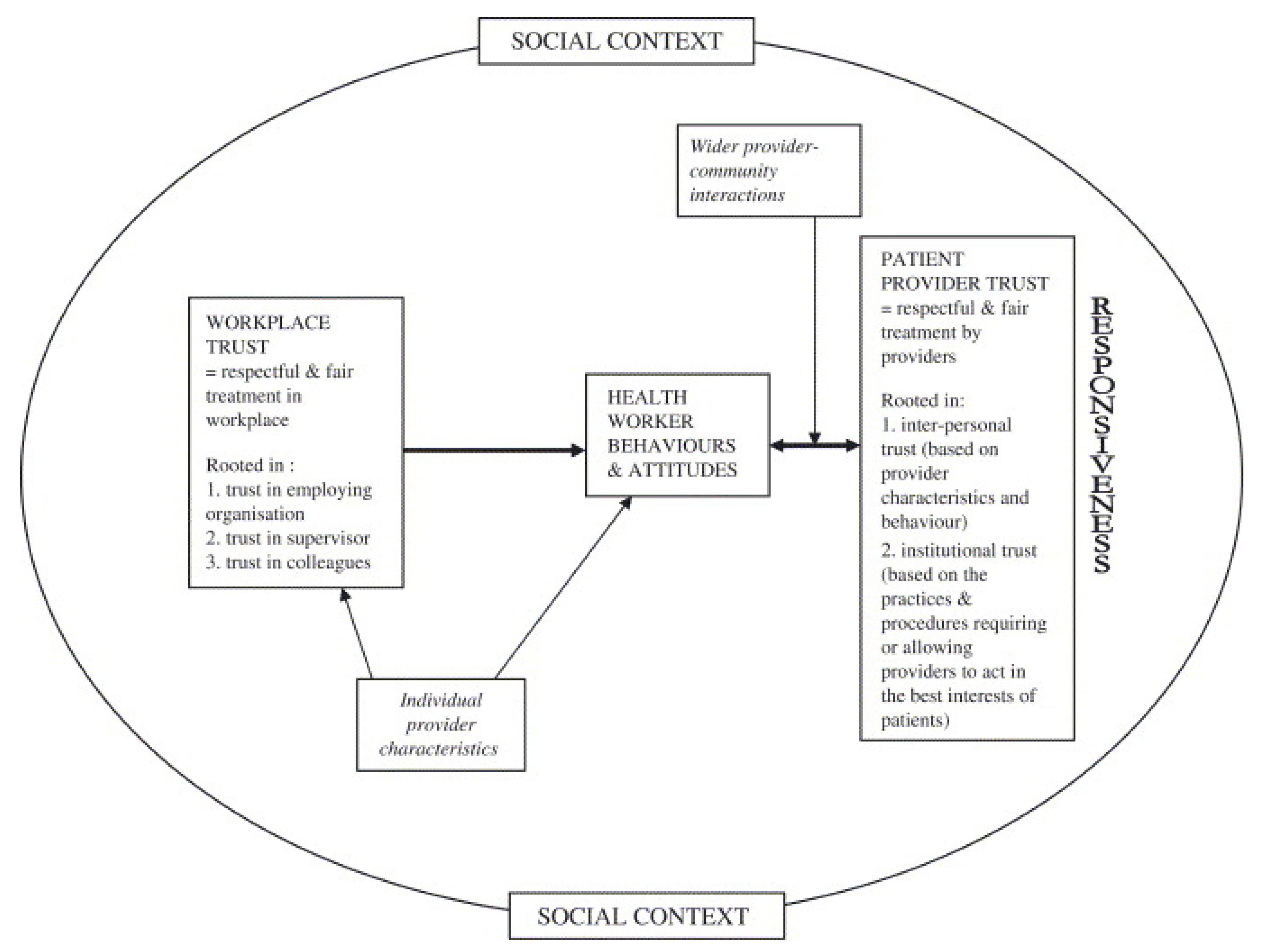
4.2. The Role of Trust in Primary Healthcare
4.3. Strengths, Limitations, and Future Research Opportunities
4.4. Study Implications and Recommendations for Policymakers and Practitioners
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roles, D.C. Support for Community Health Workers to Increase Health Access and to Reduce Health Inequities; Policy Statement Database; American Public Health Association: Washington, DC, USA, 2009. [Google Scholar]
- Waitzkin, H.; Getrich, C.; Heying, S.; Rodríguez, L.; Parmar, A.; Willging, C.; Yager, J.; Santos, R. Promotoras as mental health practitioners in primary care: A multi-method study of an intervention to address contextual sources of depression. J. Community Health 2011, 36, 316–331. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kangovi, S.; Mitra, N.; Grande, D.; Huo, H.; Smith, R.A.; Long, J.A. Community Health Worker Support for Disadvantaged Patients with Multiple Chronic Diseases: A Randomized Clinical Trial. Am. J. Public Health 2017, 107, 1660–1667. [Google Scholar] [CrossRef] [PubMed]
- Kangovi, S.; Mitra, N.; Grande, D.; White, M.L.; McCollum, S.; Sellman, J.; Shannon, R.P.; Long, J.A. Patient-centered community health worker intervention to improve posthospital outcomes: A randomized clinical trial. JAMA Intern. Med. 2014, 174, 535–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kangovi, S.; Mitra, N.; Norton, L.; Harte, R.; Zhao, X.; Carter, T.; Grande, D.; Long, J.A. Effect of Community Health Worker Support on Clinical Outcomes of Low-Income Patients across Primary Care Facilities: A Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 1635–1643. [Google Scholar] [CrossRef]
- Morgan, A.U.; Grande, D.T.; Carter, T.; Long, J.A.; Kangovi, S. Penn Center for Community Health Workers: Step-by-Step Approach to Sustain an Evidence-Based Community Health Worker Intervention at an Academic Medical Center. Am. J. Public Health 2016, 106, 1958–1960. [Google Scholar] [CrossRef]
- Boyce, M.R.; Katz, R. Community Health Workers and Pandemic Preparedness: Current and Prospective Roles. Front. Public Health 2019, 7, 62. [Google Scholar] [CrossRef] [Green Version]
- Perry, H.B.; Dhillon, R.S.; Liu, A.; Chitnis, K.; Panjabi, R.; Palazuelos, D.; Koffi, A.K.; Kandeh, J.N.; Camara, M.; Camara, R. Community health worker programmes after the 2013–2016 Ebola outbreak. Bull. World Health Organ. 2016, 94, 551. [Google Scholar] [CrossRef]
- Haines, A.; de Barros, E.F.; Berlin, A.; Heymann, D.L.; Harris, M.J. National UK programme of community health workers for COVID-19 response. Lancet 2020, 395, 1173–1175. [Google Scholar] [CrossRef]
- Waters, R. Community Workers Lend Human Connection to COVID-19 Response: Article examines the role of community health workers in responding to the COVID-19 pandemic. Open Access 2020, 39, 7. [Google Scholar] [CrossRef]
- Peretz, P.J.; Islam, N.; Matiz, L.A. Community Health Workers and Covid-19—Addressing Social Determinants of Health in Times of Crisis and Beyond. N. Engl. J. Med. 2020, 383, e108. [Google Scholar] [CrossRef]
- Tayyib, N.M. An action plan to address the mental health impact of COVID-19 on communities: Five effective strategies. Psychol. Serv. 2021. [Google Scholar] [CrossRef] [PubMed]
- Barnett, M.L.; Gonzalez, A.; Miranda, J.; Chavira, D.A.; Lau, A.S. Mobilizing Community Health Workers to Address Mental Health Disparities for Underserved Populations: A Systematic Review. Adm. Policy Ment. Health 2018, 45, 195–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mistry, S.K.; Harris-Roxas, B.; Yadav, U.N.; Shabnam, S.; Rawal, L.B.; Harris, M.F. Community Health Workers Can Provide Psychosocial Support to the People during COVID-19 and beyond in Low- and Middle-Income Countries. Front. Public Health 2021, 9, 666753. [Google Scholar] [CrossRef] [PubMed]
- Vanden Bossche, D.; Lagaert, S.; Willems, S.; Decat, P. Community Health Workers as a Strategy to Tackle Psychosocial Suffering Due to Physical Distancing: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 3097. [Google Scholar] [CrossRef]
- Taylor, J.; Jones, R.M.; O’Reilly, P.; Oldfield, W.; Blackburn, A. The Station Community Mental Health Centre Inc: Nurturing and empowering. Rural Remote Health 2010, 10, 1411. [Google Scholar] [CrossRef]
- LeBan, K.; Kok, M.; Perry, H.B. Community health workers at the dawn of a new era: 9. CHWs’ relationships with the health system and communities. Health Res. Policy Syst. 2021, 19, 116. [Google Scholar] [CrossRef]
- Anstey Watkins, J.; Griffiths, F.; Goudge, J. Community health workers’ efforts to build health system trust in marginalised communities: A qualitative study from South Africa. BMJ Open 2021, 11, e044065. [Google Scholar] [CrossRef]
- Mishra, A. ‘Trust and teamwork matter’: Community health workers’ experiences in integrated service delivery in India. Glob. Public Health 2014, 9, 960–974. [Google Scholar] [CrossRef] [Green Version]
- Mohajer, N.; Singh, D. Factors enabling community health workers and volunteers to overcome socio-cultural barriers to behaviour change: Meta-synthesis using the concept of social capital. Hum. Resour. Health 2018, 16, 63. [Google Scholar] [CrossRef] [Green Version]
- Schneider, H.; Okello, D.; Lehmann, U. The global pendulum swing towards community health workers in low- and middle-income countries: A scoping review of trends, geographical distribution and programmatic orientations, 2005 to 2014. Hum. Resour. Health 2016, 14, 65. [Google Scholar] [CrossRef] [Green Version]
- Ware, N.C.; Idoko, J.; Kaaya, S.; Biraro, I.A.; Wyatt, M.A.; Agbaji, O.; Chalamilla, G.; Bangsberg, D.R. Explaining adherence success in sub-Saharan Africa: An ethnographic study. PLoS Med. 2009, 6, e11. [Google Scholar] [CrossRef] [Green Version]
- Rowe, R.; Calnan, M. Trust relations in health care—The new agenda. Eur. J. Public Health 2006, 16, 4–6. [Google Scholar] [CrossRef] [Green Version]
- Thiede, M. Information and access to health care: Is there a role for trust? Soc. Sci. Med. 2005, 61, 1452–1462. [Google Scholar] [CrossRef]
- Okello, D.R.; Gilson, L. Exploring the influence of trust relationships on motivation in the health sector: A systematic review. Hum. Resour. Health 2015, 13, 16. [Google Scholar] [CrossRef] [Green Version]
- Gilson, L. Trust and the development of health care as a social institution. Soc. Sci. Med. 2003, 56, 1453–1468. [Google Scholar] [CrossRef]
- Gilson, L.; Palmer, N.; Schneider, H. Trust and health worker performance: Exploring a conceptual framework using South African evidence. Soc. Sci Med. 2005, 61, 1418–1429. [Google Scholar] [CrossRef]
- Pawson, R.; Tilley, N. Realistic Evaluation. Lond. SAGE 1997. [Google Scholar]
- Greenhalgh, T.; Pawson, R.; Wong, G.; Westhorp, G.; Greenhalgh, J.; Manzano, A.; Jagosh, J. Retroduction in Realist Evaluation. RAMESES II Proj. 2017, 5, 28. [Google Scholar]
- Plsek, P.E.; Greenhalgh, T. Complexity science: The challenge of complexity in health care. BMJ 2001, 323, 625–628. [Google Scholar] [CrossRef]
- Glaser, B.G.; Strauss, A.L. Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine: Chicago, IL, USA, 1967. [Google Scholar]
- Van der Veken, K.; Lauwerier, E.; Willems, S.J. How community sport programs may improve the health of vulnerable population groups: A program theory. Int. J. Equity Health 2020, 19, 74. [Google Scholar] [CrossRef]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef]
- Strauss, A.; Corbin, J. Basics of Qualitative Research Techniques; San Jose State University: San Jose, CA, USA, 1998. [Google Scholar]
- Oliver, C. Critical realist grounded theory: A new approach for social work research. Br. J. Soc. Work 2012, 42, 371–387. [Google Scholar] [CrossRef]
- Raviola, G.; Naslund, J.A.; Smith, S.L.; Patel, V. Innovative Models in Mental Health Delivery Systems: Task Sharing Care with Non-specialist Providers to Close the Mental Health Treatment Gap. Curr. Psychiatry Rep. 2019, 21, 44. [Google Scholar] [CrossRef]
- Detollenaere, J.; Hanssens, L.; Vyncke, V.; De Maeseneer, J.; Willems, S. Do We Reap What We Sow? Exploring the Association between the Strength of European Primary Healthcare Systems and Inequity in Unmet Need. PLoS ONE 2017, 12, e0169274. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| FGDs | In-Depth Interviews | |||
|---|---|---|---|---|
| CHWs | CHWs | Clients | ||
| N = 8 (%) | N = 13 (%) | N = 11 (%) | ||
| Sex | Male | 3 (37.5%) | 3 (23.1%) | 4 (36.4%) |
| Female | 5 (62.5%) | 10 (76.9%) | 7 (63.6) | |
| Age (yrs) | <25 | 0 | 1 (7.7%) | 0 |
| 25–39 | 3 (37.5%) | 7 (53.8%) | 1 (9.1%) | |
| 40–64 | 5 (62.5%) | 5 (38.5%) | 4 (36.4%) | |
| ≥65 | 0 | 0 | 6 (54.5%) | |
| Work or activity | Student | 0 | 2 (15.4%) | 1 (9.1%) |
| Worker/Servant/Self-employed | 4 (50%) | 6 (46.1%) | 0 | |
| Job-seeking | 1 (12.5%) | 2 (15.4%) | 1 (9.1%) | |
| Retired | 2 (25%) | 2 (15.4%) | 6 (54.5%) | |
| Disability | 1 (12.5%) | 1 (7.7%) | 3 (27.3%) | |
| Migration background | No | 8 (100%) | 9 (69.2%) | 7 (63.6) |
| Yes, | ||||
| Living <1 year in Belgium | 0 | 0 | 1 (9.1%) | |
| Living 1–5 years in Belgium | 0 | 0 | 0 | |
| Living 6–10 years in Belgium | 0 | 1 (7.7%) | 1 (9.1%) | |
| Living >10 years in Belgium | 0 | 3 (23.1%) | 2 (18.2%) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vanden Bossche, D.; Willems, S.; Decat, P. Understanding Trustful Relationships between Community Health Workers and Vulnerable Citizens during the COVID-19 Pandemic: A Realist Evaluation. Int. J. Environ. Res. Public Health 2022, 19, 2496. https://doi.org/10.3390/ijerph19052496
Vanden Bossche D, Willems S, Decat P. Understanding Trustful Relationships between Community Health Workers and Vulnerable Citizens during the COVID-19 Pandemic: A Realist Evaluation. International Journal of Environmental Research and Public Health. 2022; 19(5):2496. https://doi.org/10.3390/ijerph19052496
Chicago/Turabian StyleVanden Bossche, Dorien, Sara Willems, and Peter Decat. 2022. "Understanding Trustful Relationships between Community Health Workers and Vulnerable Citizens during the COVID-19 Pandemic: A Realist Evaluation" International Journal of Environmental Research and Public Health 19, no. 5: 2496. https://doi.org/10.3390/ijerph19052496
APA StyleVanden Bossche, D., Willems, S., & Decat, P. (2022). Understanding Trustful Relationships between Community Health Workers and Vulnerable Citizens during the COVID-19 Pandemic: A Realist Evaluation. International Journal of Environmental Research and Public Health, 19(5), 2496. https://doi.org/10.3390/ijerph19052496