
Piloting the Use of Concept Mapping to Engage Geographic Communities for Stress and Resilience Planning in Toronto, Ontario, Canada

Abstract
:1. Introduction
1.1. Chronic Stress and Community Resilience Interventions
1.2. Environmental Determinants of Stress in Neighborhoods
1.3. Concept Mapping for Community Knowledge
1.4. Pilot Testing in Crescent Town, Toronto
2. Materials and Methods
- One issue in this community that causes chronic stress for you and/or others over time is ________________.
- One existing asset in this community that benefits you and/or others over time is _______________.
- How would you rate the importance of these neighborhood issues and assets from 1 (weak) to 5 (strong)?
3. Results
3.1. Clusters of Neighborhood Stressors
3.2. Clusters of Neighborhood Assets
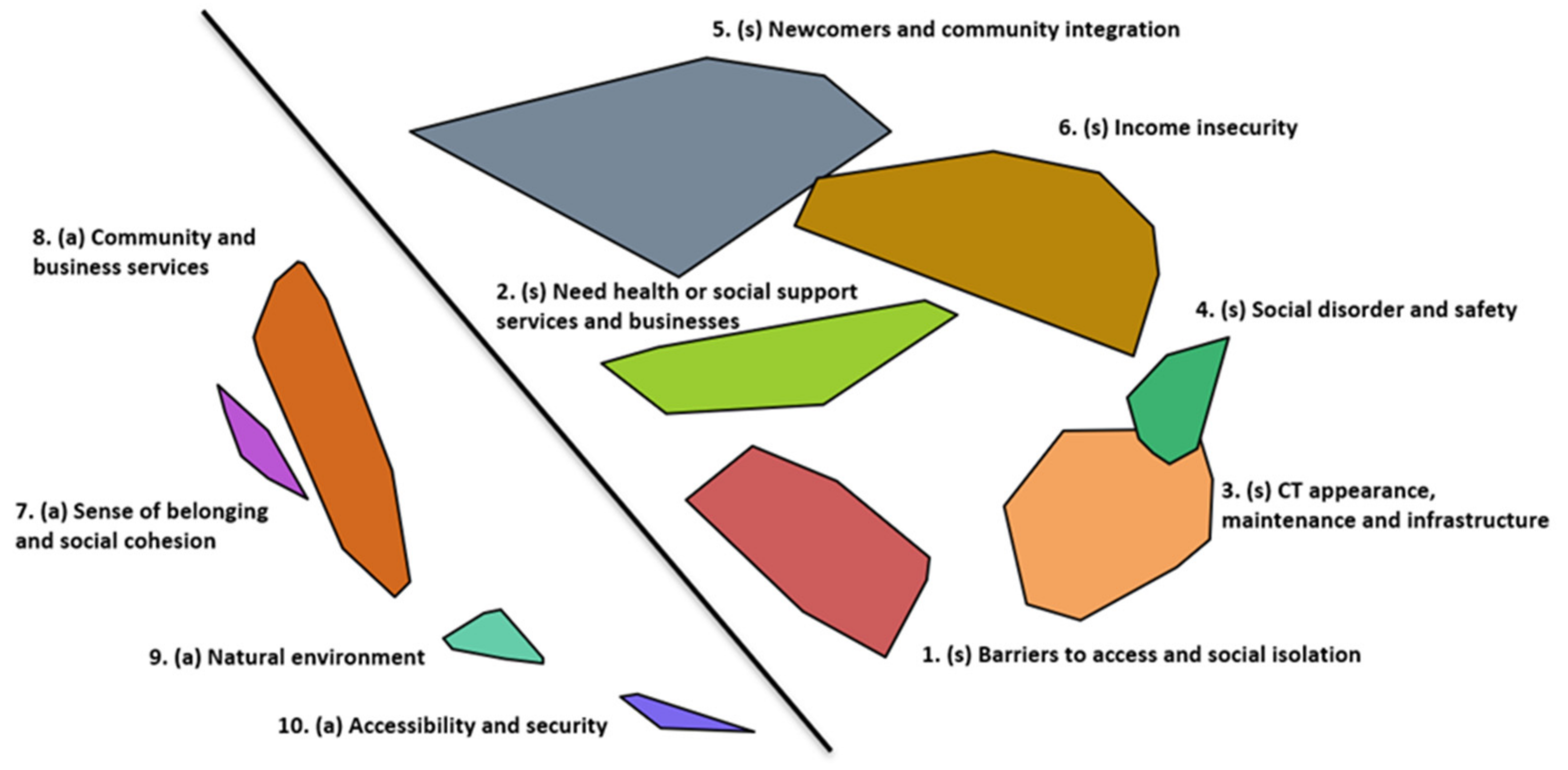
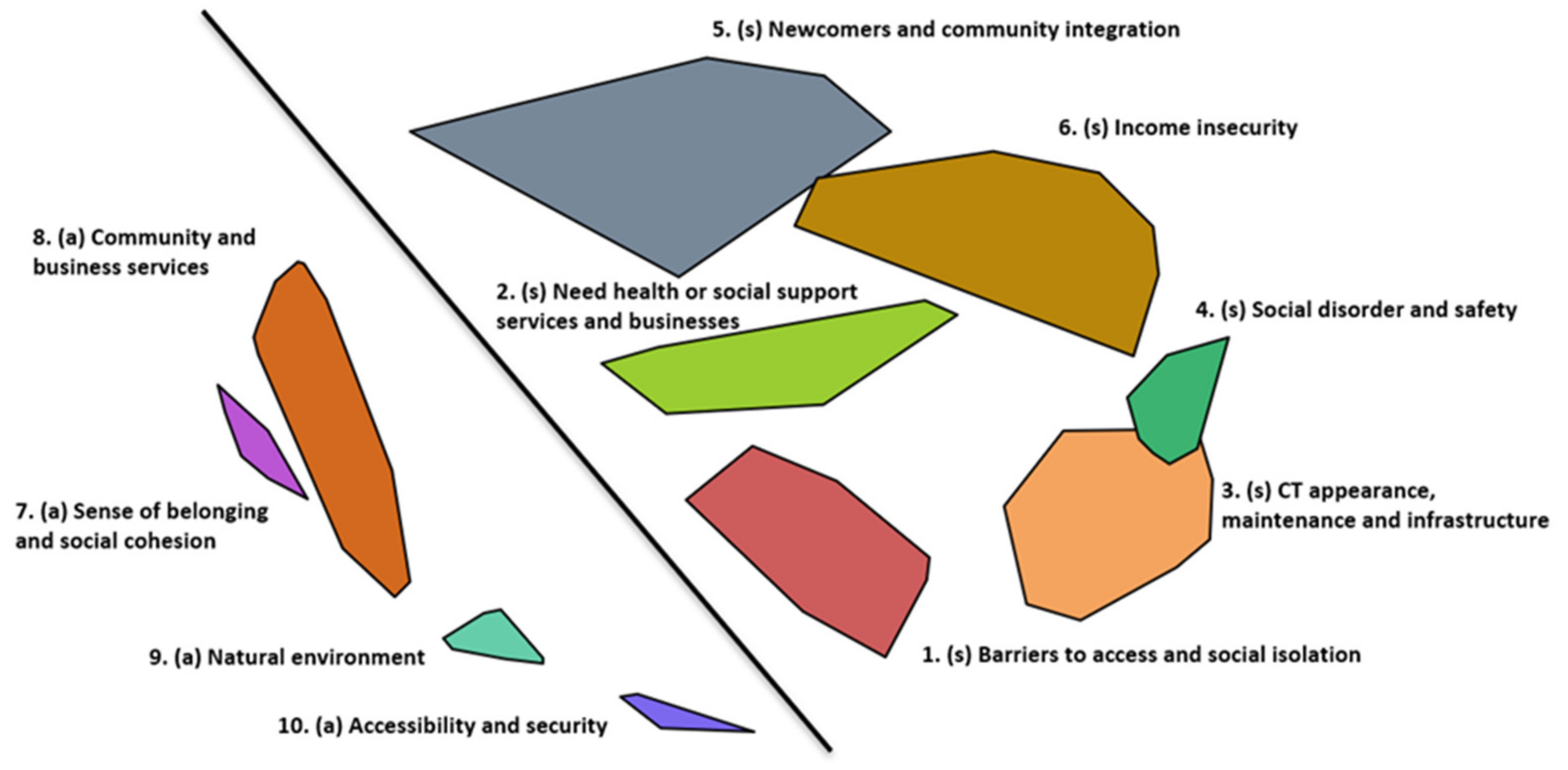
3.3. Interpretation of Clusters and Utilization of Cluster Map
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Pakeman, K. Checking Kingston’s Equity Pulse; Queen’s University: Kingston, ON, Canada, 2017; Available online: https://qspace.library.queensu.ca/bitstream/handle/1974/15439/Pakeman_Kyle_W_201703_MPL.pdf?sequence=1 (accessed on 24 June 2021).
- Social Policy Analysis and Research City of Toronto. TSNS 2020 Neighbourhood Equity Index Methodological Documentation; Social Policy Analysis and Research City of Toronto: Toronto, ON, Canada, 2014; pp. 1–60. Available online: https://www.toronto.ca/wp-content/uploads/2017/11/97eb-TSNS-2020-NEI-equity-index-methodology-research-report-backgroundfile-67350.pdf (accessed on 14 September 2021).
- Northridge, M.E.; Freeman, L. Urban Planning and Health Equity. J. Urban Health 2011, 88, 582–597. [Google Scholar] [CrossRef] [Green Version]
- Prasad, A.; Groot, A.M.M.; Monteiro, T.; Murphy, K.; O’Campo, P.; Broide, E.E.; Kano, M. Linking evidence to action on social determinants of health using Urban HEART in the Americas. Rev. Panam. Salud Publica/Pan Am. J. Public Health 2013, 34, 407–415. [Google Scholar]
- Corburn, J. City planning as preventive medicine. Prev. Med. 2015, 77, 48–51. [Google Scholar] [CrossRef] [PubMed]
- McEwen, B.S. Neurobiological and Systemic Effects of Chronic Stress. Chronic Stress 2017, 1, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankardass, K. Place-Based Stress and Chronic Disease: A Systems View of Environmental Determinants. In Rethinking Social Epidemiology; O’Campo, P., Dunn, J.R., Eds.; Springer: Dordrecht, The Netherlands, 2012; pp. 113–136. [Google Scholar]
- Harper, D.; Speed, E. Uncovering Recovery: The Resistible Rise of Recovery and Resilience. Stud. Soc. Justice 2012, 6, 9–25. [Google Scholar] [CrossRef] [Green Version]
- Bonanno, G.A. Loss, Trauma, and Human Resilience: Have We Underestimated the Human Capacity to Thrive after Extremely Aversive Events? Am. Psychol. 2004, 59, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Norris, F.H.; Stevens, S.P.; Pfefferbaum, B.; Wyche, K.F.; Pfefferbaum, R.L. Community resilience as a metaphor, theory, set of capacities, and strategy for disaster readiness. Am. J. Community Psychol. 2008, 41, 127–150. [Google Scholar] [CrossRef]
- Hansen-Nord, N.S.; Kjaerulf, F.; Almendarez, J.; Rodas, V.M.; Castro, J. Reducing violence in poor urban areas of Honduras by building community resilience through community-based interventions. Int. J. Public Health 2016, 61, 935–943. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.F.; Daffara, P.; Toole, K.O.; Matthews, J.; Thomsen, D.C.; Inayatullah, S.; Fien, J.; Graymore, M. A method for building community resilience to climate change in emerging coastal cities. Futures 2011, 43, 673–679. [Google Scholar] [CrossRef]
- Sukabdi, Z.A. Building community resilience: Strategic role of police with bombing victims. Police Pract. Res. 2016, 17, 160–170. [Google Scholar] [CrossRef]
- Narain, S. The Re-branding Project: The Genealogy of Creating a Neolibeal Jane and Finch. J. Crit. Race Inq. 2012, 2, 54–94. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; Pfefferbaum, R.L.; Horn, R.L.V. Community Resilience Interventions: Participatory, Assessment-Based, Action-Oriented Processes. Am. Behav. Sci. 2015, 59, 238–253. [Google Scholar] [CrossRef]
- A Conceptual Framework for Action on the Social Determinants of Health. Available online: https://www.who.int/sdhconference/resources/ConceptualframeworkforactiononSDH_eng.pdf (accessed on 24 June 2021).
- Macinko, J.A.; Shi, L.; Starfield, B. Income Inequality and Health: A Critical Review of the Literature. Med. Care Res. Rev. 2003, 60, 407–452. [Google Scholar] [CrossRef] [PubMed]
- Duncan, C.; Jones, K.; Moon, G. Smoking and deprivation: Are there neighbourhood effects? Soc. Sci. Med. 1999, 48, 497–505. [Google Scholar] [CrossRef]
- Yen, I.H.; Kaplan, G.A. Neighborhood social environment and risk of death: Multilevel evidence from the Alameda County Study. Am. J. Epidemiol. 1999, 149, 898–907. [Google Scholar] [CrossRef]
- Macintyre, S.; Ellaway, A.; Cummins, S. Place effects on health: How can we conceptualise, operationalise and measure them? Soc. Sci. Med. 2002, 55, 125–139. [Google Scholar] [CrossRef]
- Hazer, M.; Formica, M.K.; Dieterlen, S.; Morley, C.P. The relationship between self-reported exposure to greenspace and human stress in Baltimore, MD. Landsc. Urban Plan. 2018, 169, 47–56. [Google Scholar] [CrossRef]
- Neale, C.; Besa, M.C.; Dickin, S.; Hongsathavij, V.; Kuldna, P.; Muhoza, C.; Pravalprukskul, P.; Cinderby, S. Comparing health, stress, wellbeing and greenspace across six cities in three continents. Cities Health 2020, 4, 290–302. [Google Scholar] [CrossRef]
- Roe, J.J.; Thompson, C.W.; Aspinall, P.A.; Brewer, M.J.; Duff, E.I.; Miller, D.; Mitchell, R.; Clow, A. Green Space and Stress: Evidence from Cortisol Measures in Deprived Urban Communities. Int. J. Environ. Res. Public Health 2013, 10, 4086–4103. [Google Scholar] [CrossRef] [Green Version]
- Dalton, A.M.; Jones, A.P. Residential neighbourhood greenspace is associated with reduced risk of cardiovascular disease: A prospective cohort study. PLoS ONE 2020, 15, e0226524. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, R.; Popham, F. Effect of exposure to natural environment on health inequalities: An observational population study. Lancet 2008, 372, 1655–1660. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Zou, Y.; Gao, H. Role of neighborhood social support in stress coping and psychological wellbeing during the COVID-19 pandemic: Evidence from Hubei, China. Health Place 2021, 69, 102532. [Google Scholar] [CrossRef]
- Brown, S.C.; Mason, C.A.; Lombard, J.L.; Martinez, F.; Plater-Zyberk, E.; Spokane, A.R.; Newman, F.L.; Pantin, H.; Szapocznik, J. The relationship of built environment to perceived social support and psychological distress in Hispanic elders: The role of “eyes on the street”. J. Geronotol. Ser. B 2009, 64B, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Green, A.E.; Fettes, D.L.; Aarons, G.A. A concept mapping approach to guide and understand dissemination and implementation. J. Behav. Health Serv. Res. 2012, 39, 362–373. [Google Scholar] [CrossRef] [Green Version]
- Minh, A.; Patel, S.; Bruce-Barrett, C.; O’Campo, P. Letting youths choose for themselves: Concept mapping as a participatory approach for program and service planning. Fam. Community Health 2015, 38, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Kane, M.; Trochim, W.M.K. Concept Mapping for Planning and Evaluation; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Novak, J.D.; Cañas, A.J. The origins of the concept mapping tool and the continuing evolution of the tool. Inf. Vis. 2006, 45, 175–184. [Google Scholar] [CrossRef]
- Trochim, W.M.K. An Introduction To Concept Mapping For Planning and Evaluation. Eval. Program Plan. 1989, 12, 1–16. [Google Scholar] [CrossRef]
- Burke, J.; O’Campo, P.; Peak, G.L.; Gielen, A.C.; McDonnell, K.A.; Trochim, W.M.K. An introduction to concept mapping as a participatory public health research method. Qual. Health Res. 2005, 15, 1392–1410. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, L.M.; Jones, J.R.; Booth, E.; Burke, J.G. Concept mapping methodology and community-engaged research: A perfect pairing. Eval. Program Plan. 2017, 60, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Hulchanski, J.D. The Three Cities within Toronto: Income Polarization Among Toronto’s Neighbourhoods, 1970–2005; University of Toronto: Toronto, ON, Canada, 2010; pp. 1–28. ISBN 9780772714787. [Google Scholar]
- Hulchanski, J.D. Divided Cities. 2017. Available online: http://neighbourhoodchange.ca/documents/2017/01/divided-cities-course-syllabus-2017.pdf (accessed on 5 January 2017).
- Toronto Community Health Profiles Partnership. Urban HEART @Toronto. Available online: http://www.torontohealthprofiles.ca/urbanheartattoronto.php (accessed on 24 June 2021).
- Toronto, C.o. Wellbeing Toronto. Available online: https://www.toronto.ca/city-government/data-research-maps/neighbourhoods-communities/wellbeing-toronto/ (accessed on 24 June 2021).
- Elayan, S.; Sykora, M.; Shankardass, K.; Robertson, C.; Feick, R.; Shaughnessy, K.; Haydn, L.; Jackson, T. The Stresscapes Ontology System: Detecting and Measuring Stress on Social Media. In Proceedings of the 7th European Conference on Social Media ECSM 2020, Larnaca, Cyprus, 2–3 July 2020; p. 74. Available online: https://www.researchgate.net/profile/Azian-Muhamad-Adzmi/publication/342277981_ECSM20-Proceedings/links/5eeb91ac299bf1faac5f4708/ECSM20-Proceedings.pdf (accessed on 24 June 2021).
- Lipmanowicz, H.; McCandless, K. 1-2-4-All. Available online: https://www.liberatingstructures.com/1-1-2-4-all/ (accessed on 24 June 2021).
- Kwok, E.Y.L.; Moodie, S.T.F.; Cunningham, B.J.; Oram Cardy, J.E. Selecting and tailoring implementation interventions: A concept mapping approach. BMC Health Sci. Res. 2020, 20, 385. [Google Scholar] [CrossRef] [PubMed]
- Kelly, C.K.; Baker, E.A.; Brownson, R.C.; Schootman, M. Translating research into practice: Using concept mapping to determine locally relevant intervention strategies to increase physical activity. Eval. Program Plan. 2007, 30, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, L.M.; Jacquez, F.; McLinden, D. The Use of Concept Mapping to Identify Community-Driven Intervention Strategies for Physical and Mental Health. Health Promot. Pract. 2012, 14. [Google Scholar] [CrossRef] [PubMed]
- Haque, N.; Rosas, S. Concept Mapping of Photovoices-Sequencing and Integrating Methods to Understand Immigrants’ Perceptions of Neighborhood Influences on Health. Fam. Community Health 2010, 33, 193–206. [Google Scholar] [CrossRef] [PubMed]
- Ridings, J.W.; Powell, D.M.; Johnson, J.E.; Pullie, C.J.; Jones, C.M.; Jones, R.L.; Terrell, K.J. Using Concept Mapping to Promote Community Building: The African American Initiative at Roseland. J. Community Pract. 2008, 16, 39–63. [Google Scholar] [CrossRef]
- Risisky, D.; Hogan, V.K.; Kane, M.; Burt, B.; Dove, C.; Payton, M. Concept Mapping as a Tool to Engage a Community in Health Disparity Identification. Ethn. Dis. 2008, 18, 77–83. [Google Scholar] [PubMed]
- Boston, T.; Meagher, S. Crescent Town Study. Final Report of a Study Commissioned by the Crescent Town Club; Public Interest Strategy & Communications: Toronto, ON, Canada, 2007; pp. 1–39. Available online: https://www.crescenttownclub.com/pdfs/Crescent%20Town%20Report%202002.pdf (accessed on 24 June 2021).
- City of Toronto. Toronto Strong Neighbourhoods Strategy 2020. Available online: https://www.toronto.ca/city-government/accountability-operations-customer-service/long-term-vision-plans-and-strategies/toronto-strong-neighbourhoods-strategy-2020/ (accessed on 24 June 2021).
- Toronto Strong Neighbourhoods Strategy 2020. Dawes Road Service Delivery Plan. 2019. Available online: https://scholar.google.com/scholar?hl=zh-CN&as_sdt=0%2C5&q=Toronto+Strong+Neighbourhoods+Strategy+2020.+Dawes+Road+Service+Delivery+Plan.+2019&btnG= (accessed on 4 September 2021).
- Ore, J. Toronto Tenants Unionize to Demand Rent Relief in the Face of Looming Pandemic Evictions. CBC Radio. 2021. Available online: https://globalnews.ca/video/7283925/toronto-tenants-protest-evictions-demand-rent-relief-during-pandemic/ (accessed on 18 August 2020).
- Saravanamuttu, K. Tenant Unions Fighting Back Against Evictions. Available online: https://springmag.ca/tenant-unions-fighting-back-against-evictions (accessed on 17 February 2021).

{kind=link}
| Cluster | Chronic Stressors | Cluster Rating of Importance |
|---|---|---|
| 1 | Barriers to access and social isolation | 2.91 |
| 2 | Need health or social support services or businesses | 3.30 |
| 3 | Crescent Town appearance, maintenance, and infrastructure | 3.60 |
| 4 | Social disorder and safety | 3.51 |
| 5 | Newcomers and community integration | 3.31 |
| 6 | Areas in need of city support | 3.27 |
| Cluster | Assets | Cluster Rating of Importance |
| 7 | Available support system | 3.67 |
| 8 | Community and business services | 3.78 |
| 9 | Housing setting | 4.16 |
| 10 | Accessibility and security | 4.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ta, M.; Shankardass, K. Piloting the Use of Concept Mapping to Engage Geographic Communities for Stress and Resilience Planning in Toronto, Ontario, Canada. Int. J. Environ. Res. Public Health 2021, 18, 10977. https://doi.org/10.3390/ijerph182010977
Ta M, Shankardass K. Piloting the Use of Concept Mapping to Engage Geographic Communities for Stress and Resilience Planning in Toronto, Ontario, Canada. International Journal of Environmental Research and Public Health. 2021; 18(20):10977. https://doi.org/10.3390/ijerph182010977
Chicago/Turabian StyleTa, Martha, and Ketan Shankardass. 2021. "Piloting the Use of Concept Mapping to Engage Geographic Communities for Stress and Resilience Planning in Toronto, Ontario, Canada" International Journal of Environmental Research and Public Health 18, no. 20: 10977. https://doi.org/10.3390/ijerph182010977
APA StyleTa, M., & Shankardass, K. (2021). Piloting the Use of Concept Mapping to Engage Geographic Communities for Stress and Resilience Planning in Toronto, Ontario, Canada. International Journal of Environmental Research and Public Health, 18(20), 10977. https://doi.org/10.3390/ijerph182010977