
Health-Seeking Behaviors in Mozambique: A Mini-Study of Ethnonursing


Abstract
:1. Introduction
1.1. Overview of Mozambique
1.1.1. Brief Ethnohistory
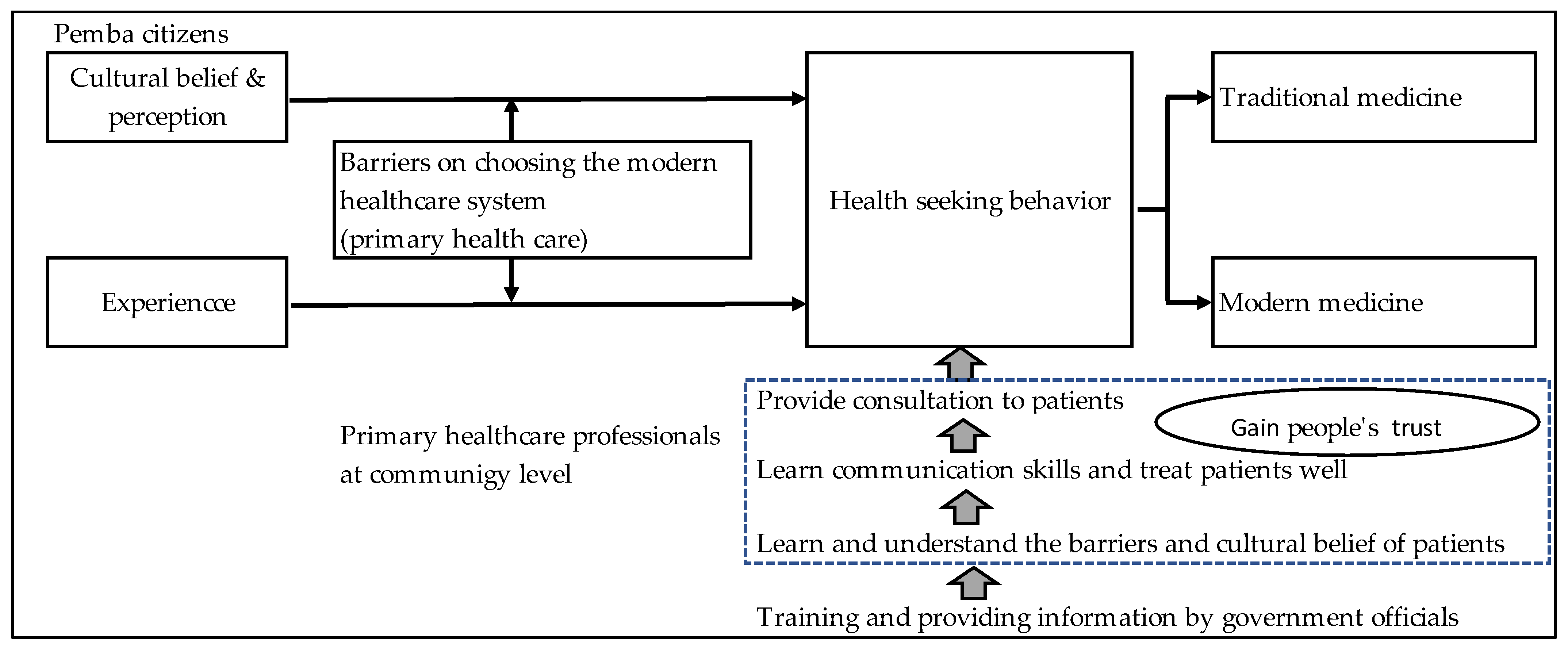
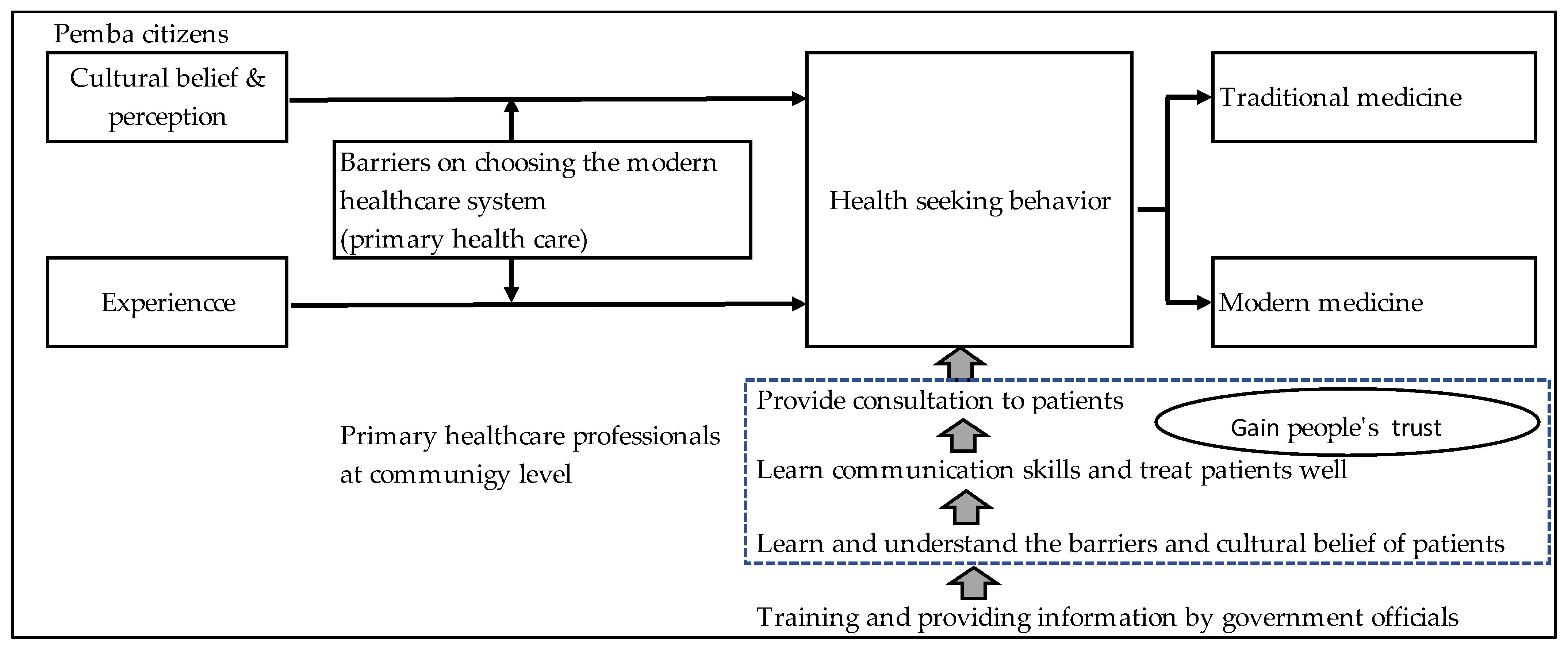
1.1.2. Theoretical Guide and Conceptual Framework
2. Materials and Methods
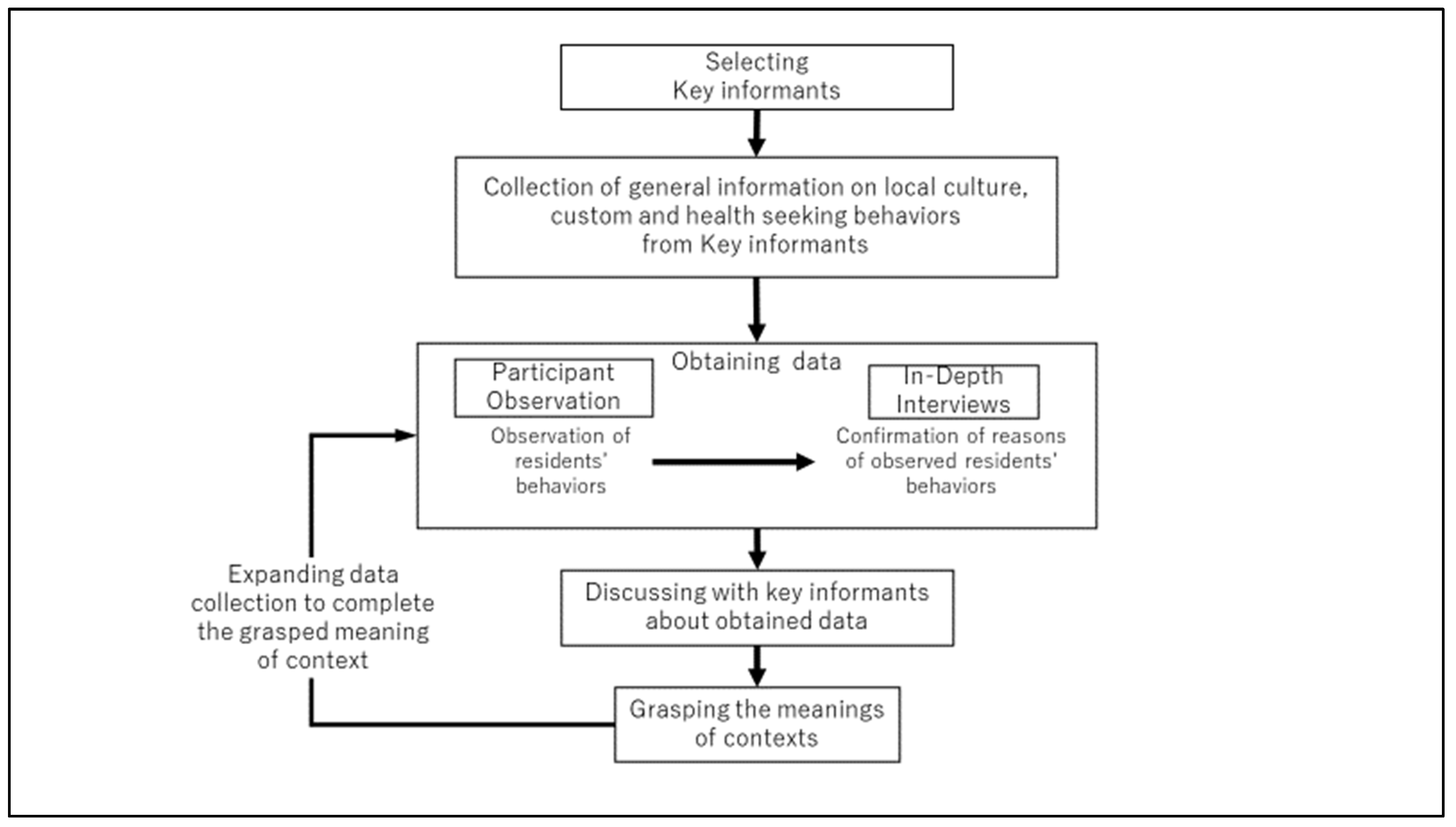
2.1. Study Design
2.2. Study Area
2.3. Participants and Data Collection
2.4. Participant Observation
2.5. Recruitment and In-Depth Interviews
2.6. Data Analysis
3. Results
3.1. Socio-Demographic Characteristics of Informants
3.2. Themes Discerned from Patterns
4. Discussion
Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Berg, A.; Patel, S.; Aukrust, P.; David, C.; Gonca, M.; Berg, E.S.; Dalen, I.; Langeland, N. Increased severity and mortality in adults co-infected with malaria and HIV in Maputo, Mozambique: A prospective cross-sectional study. PLoS ONE 2014, 9, e88257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whetten, K.; Leserman, J.; Whetten, R.; Ostermann, J.; Thielman, N.; Swartz, M.; Stangl, D. Exploring lack of trust in care providers and the government as a barrier to health service use. Am. J. Public Health 2006, 96, 716–721. [Google Scholar] [CrossRef] [PubMed]
- Cassy, A.; Saifodine, A.; Candrinho, B.; do Rosário Martins, M.; da Cunha, S.; Pereira, F.M.; Gudo, E.S. Care-seeking behaviour and treatment practices for malaria in children under 5 years in Mozambique: A secondary analysis of 2011 DHS and 2015 IMASIDA datasets. Malar. J. 2019, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Alemu, T.; Biadgilign, S.; Deribe, K.; Escudero, H.R. Experience of stigma and discrimination and the implications for healthcare seeking behavior among people living with HIV/AIDS in resource-limited setting. SAHARA-J J. Soc. Asp. HIV AIDS 2013, 10, 1–7. [Google Scholar] [CrossRef]
- Munguambe, K.; Boene, H.; Vidler, M.; Bique, C.; Sawchuck, D.; Firoz, T.; Makanga, P.T.; Qureshi, R.; Macete, E.; Menéndez, C. Barriers and facilitators to health care seeking behaviours in pregnancy in rural communities of southern Mozambique. Reprod. Health 2016, 13, 83–97. [Google Scholar] [CrossRef] [Green Version]
- Posse, M.; Meheus, F.; Van Asten, H.; Van Der Ven, A.; Baltussen, R. Barriers to access to antiretroviral treatment in developing countries: A review. Trop. Med. Int. Health 2008, 13, 904–913. [Google Scholar] [CrossRef]
- Ostherr, K.; Killoran, P.; Shegog, R.; Bruera, E. Death in the digital age: A systematic review of information and communication technologies in end-of-life care. J. Palliat. Med. 2016, 19, 408–420. [Google Scholar] [CrossRef] [Green Version]
- Anselmi, L.; Lagarde, M.; Hanson, K. Health service availability and health seeking behaviour in resource poor settings: Evidence from Mozambique. Health Econ. Rev. 2015, 5, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Honwana, A.M. Healing for peace: Traditional healers and post-war reconstruction in Southern Mozambique. Peace Confl. 1997, 3, 293–305. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Report on Traditional and Complementary Medicine 2019; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Ferrão, L.J.; Fernandes, T.H. Community oriented interprofessional health education in Mozambique: One student/one family program. Educ. Health 2014, 27, 103. [Google Scholar]
- Atwine, F.; Hultsjö, S.; Albin, B.; Hjelm, K. Health-care seeking behaviour and the use of traditional medicine among persons with type 2 diabetes in south-western Uganda: A study of focus group interviews. Pan. Afr. Med. J. 2015, 20, 76. [Google Scholar] [CrossRef] [PubMed]
- Napier, A.D.; Ancarno, C.; Butler, B.; Calabrese, J.; Chater, A.; Chatterjee, H.; Guesnet, F.; Horne, R.; Jacyna, S.; Jadhav, S. Culture and health. Lancet 2014, 384, 1607–1639. [Google Scholar] [CrossRef]
- Winiger, F.; Peng-Keller, S. Religion and the World Health Organization: An evolving relationship. BMJ Glob. Health 2021, 6, e004073. [Google Scholar] [CrossRef] [PubMed]
- Abubakar, A.; Van Baar, A.; Fischer, R.; Bomu, G.; Gona, J.K.; Newton, C.R. Socio-cultural determinants of health-seeking behaviour on the Kenyan coast: A qualitative study. PLoS ONE 2013, 8, e71998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibanez-Gonzalez, D.L.; Mendenhall, E.; Norris, S.A. A mixed methods exploration of patterns of healthcare utilization of urban women with non-communicable disease in South Africa. BMC Health Serv. Res. 2014, 14, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Audet, C.M.; Sidat, M.; Blevins, M.; Moon, T.D.; Vergara, A.; Vermund, S.H. HIV knowledge and health-seeking behavior in Zambe zia Province, Mozambique. SAHARA-J J. Soc. Asp. HIV AIDS 2012, 9, 41–46. [Google Scholar] [CrossRef]
- Leininger, M.M.; McFarland, M.R. Culture Care Diversity and Universality: A Worldwide Nursing Theory; Jones & Bartlett Learning: Burlington, MA, USA, 2006. [Google Scholar]
- Bonate, L. Islam in northern Mozambique: A historical overview. Hist. Compass 2010, 8, 573–593. [Google Scholar] [CrossRef]
- Burchett, W.G. Southern Africa Stands Up: The Revolutions in Angola, Mozambique, Rhodesia, Namibia, and South Africa; Urizen Books: New York, NY, USA, 1978. [Google Scholar]
- Gumende, A. Mozambique: Historical Trajectories and Development. Hisp. Res. J. 2010, 11, 172–185. [Google Scholar] [CrossRef]
- WorldAtlas. Ethnic Groups of Mozambique. 2022. Available online: https://www.worldatlas.com/articles/ethnic-groups-of-mozambique.html#:~:text=The%20main%20ethnic%20groups%20in,of%20the%20population%2C%20as%20well (accessed on 14 February 2022).
- The World Factbook. Mozambique. Available online: https://www.cia.gov/the-world-factbook/countries/mozambique/#people-and-society (accessed on 14 February 2022).
- Creasey, A. Willingness-to-Pay for Halal and Branded Poultry in Northern Mozambique. Agricultural Education, Communications and Technology Undergraduate Honors Theses. 2021. Available online: https://scholarworks.uark.edu/aectuht/13 (accessed on 14 December 2021).
- Mozambique. International Religious Freedom Report. 2019. Available online: https://mz.usembassy.gov/wp-content/uploads/sites/182/MOZAMBIQUE-2019-INTERNATIONAL-RELIGIOUS-FREEDOM-REPORT.pdf (accessed on 14 February 2022).
- Wikipedia. Economy of Mozambique. 2022. Available online: https://en.wikipedia.org/wiki/Economy_of_Mozambique (accessed on 14 February 2022).
- Minter, W. Apartheid’s Contras: An Inquiry into the Roots of War in Angola and Mozambique; Zed Books: London, UK, 1994. [Google Scholar]
- Govindasamy, D.; Ford, N.; Kranzer, K. Risk factors, barriers and facilitators for linkage to antiretroviral therapy care: A systematic review. Aids 2012, 26, 2059–2067. [Google Scholar] [CrossRef]
- Roper, J.M.; Shapira, J. Ethnography in Nursing Research; SAGE Publications Inc.: Los Angeles, CA, USA, 2000; Volume 1. [Google Scholar]
- World Health Organization. World Health Organization Global Health Observatory Data Repository; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. Regional Office for Africa. Wkly. Bull. Outbreak Other Emergencies Week 2021, 1, 2. [Google Scholar]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage Publications Inc: Los Angeles, CA, USA, 2014. [Google Scholar]
- Chukwuneke, F.; Ezeonu, C.; Onyire, B.; Ezeonu, P. Culture and biomedical care in Africa: The influence of culture on biomedical care in a traditional African society, Nigeria, West Africa. Niger. J. Med. 2012, 21, 331–333. [Google Scholar] [PubMed]
- McElroy, A. Medical Anthropology in Ecological Perspective; Routledge, Taylor & Francis: New York, NY, USA, 2018. [Google Scholar]
- Audet, C.M.; Ngobeni, S.; Wagner, R.G. Traditional healer treatment of HIV persists in the era of ART: A mixed methods study from rural South Africa. BMC Complementary Altern. Med. 2017, 17, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabuni, L.P. Dilemma with the local perception of causes of illnesses in central Africa: Muted concept but prevalent in everyday life. Qual. Health Res. 2007, 17, 1280–1291. [Google Scholar] [CrossRef] [PubMed]
- Fearon, J.D. Ethnic and cultural diversity by country. J. Econ. Growth 2003, 8, 195–222. [Google Scholar] [CrossRef]
- Makundi, E.A.; Malebo, H.M.; Mhame, P.; Kitua, A.Y.; Warsame, M. Role of traditional healers in the management of severe malaria among children below five years of age: The case of Kilosa and Handeni Districts, Tanzania. Malar. J. 2006, 5, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdullahi, A.A. Trends and challenges of traditional medicine in Africa. Afr. J. Tradit. Complementary Altern. Med. 2011, 8, 115–123. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables |
|---|
|
| Number | Number |
|---|---|
| Age by Decade | |
| 20 s | 2 |
| 30 s | 4 |
| 40 s | 2 |
| 50 s | 4 |
| Gender | |
| Male | 8 |
| Female | 4 |
| Tribe | |
| Makonde | 6 |
| Makuwa | 5 |
| Shona | 1 |
| Education | |
| No education | 1 |
| Under 8th grade | 3 |
| Under 12th grade | 6 |
| Associate degree | 1 |
| Bachelor’s degree | 1 |
| Occupation | |
| Teacher | 3 |
| Public officer | 1 |
| Office worker | 2 |
| Health worker | 1 |
| Pension recipient | 2 |
| Plasterer | 1 |
| Guard man | 1 |
| No occupation | 1 |
| Themes | Categories | Codes |
|---|---|---|
| Perceptions of health and illness |
|
|
|
| |
|
| |
| Local perception of causes of diseases |
|
|
|
| |
|
| |
| Trust in the indigenous medical system |
|
|
|
| |
|
| |
| Dissatisfaction with governmental medical services |
|
|
|
| |
|
|
| Category | Public Medical Health System | Traditional Medical Health System |
|---|---|---|
| Theory | European Medicine | Curandeirismo |
| Who provides treatment | Physician and medical technician | Traditional healer (curandeiro) |
| Medicine | Chemical agents | Medicinal herbs and natural agents (including minerals) Magic |
| Treatment site | Medical facilities One provincial hospital and nine health centers in each ward | Traditional healer’s house or another site |
| Access | One provincial hospital and nine health centers, and all facilities are open to anybody who visits | Open access, but the patients need to search by themselves based on personal information |
| Consultant fee | 1 mt (1 United States Dollar = 75 Metical) | Expensive consultant fee (More than 10,000 mt) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeyama, N.; Muzembo, B.A.; Jahan, Y.; Moriyama, M. Health-Seeking Behaviors in Mozambique: A Mini-Study of Ethnonursing. Int. J. Environ. Res. Public Health 2022, 19, 2462. https://doi.org/10.3390/ijerph19042462
Takeyama N, Muzembo BA, Jahan Y, Moriyama M. Health-Seeking Behaviors in Mozambique: A Mini-Study of Ethnonursing. International Journal of Environmental Research and Public Health. 2022; 19(4):2462. https://doi.org/10.3390/ijerph19042462
Chicago/Turabian StyleTakeyama, Naoko, Basilua Andre Muzembo, Yasmin Jahan, and Michiko Moriyama. 2022. "Health-Seeking Behaviors in Mozambique: A Mini-Study of Ethnonursing" International Journal of Environmental Research and Public Health 19, no. 4: 2462. https://doi.org/10.3390/ijerph19042462
APA StyleTakeyama, N., Muzembo, B. A., Jahan, Y., & Moriyama, M. (2022). Health-Seeking Behaviors in Mozambique: A Mini-Study of Ethnonursing. International Journal of Environmental Research and Public Health, 19(4), 2462. https://doi.org/10.3390/ijerph19042462