
Androgen Deprivation Therapy for Prostate Cancer Did Not Increase the Risk of Retinal Vascular Occlusion: A Population-Based Cohort Study

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
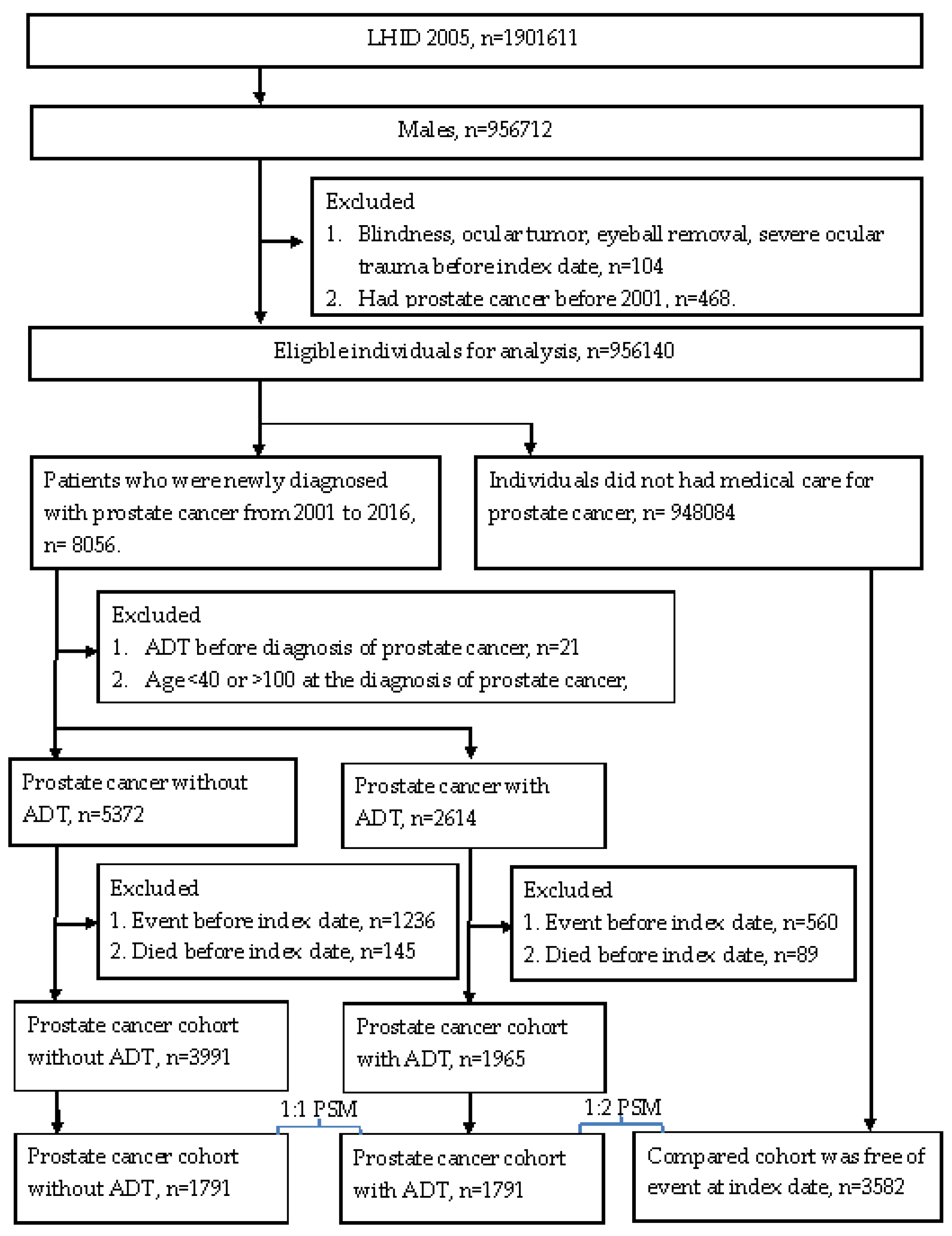
2.2. Patient Selection
2.3. Primary Outcome Measurement
2.4. Demographic and Comorbidity Variables
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Bolla, M.; Gonzalez, D.; Warde, P.; Dubois, J.B.; Mirimanoff, R.O.; Storme, G.; Bernier, J.; Kuten, A.; Sternberg, C.; Gil, T.; et al. Improved survival in patients with locally advanced prostate cancer treated with radiotherapy and goserelin. N. Engl. J. Med. 1997, 337, 295–300. [Google Scholar] [CrossRef] [PubMed]
- Bian, S.X.; Kuban, D.A.; Levy, L.B.; Oh, J.; Castle, K.O.; Pugh, T.J.; Choi, S.; McGuire, S.E.; Nguyen, Q.N.; Frank, S.J.; et al. Addition of short-term androgen deprivation therapy to dose-escalated radiation therapy improves failure-free survival for select men with intermediate-risk prostate cancer. Ann. Oncol. 2012, 23, 2346–2352. [Google Scholar] [CrossRef] [PubMed]
- Higano, C.S. Side effects of androgen deprivation therapy: Monitoring and minimizing toxicity. Urology 2003, 61, 32–38. [Google Scholar] [CrossRef]
- Nead, K.T.; Boldbaatar, N.; Yang, D.D.; Sinha, S.; Nguyen, P.L. Association of Androgen Deprivation Therapy and Thromboembolic Events: A systematic review and metaanalysis. Urology 2018, 114, 155–162. [Google Scholar] [CrossRef]
- Teoh, J.Y.; Chan, S.Y.; Chiu, P.K.; Poon, D.M.; Cheung, H.Y.; Hou, S.S.; Ng, C.F. Risk of acute myocardial infarction after androgen-deprivation therapy for prostate cancer in a Chinese population. BJU Int. 2015, 116, 382–387. [Google Scholar] [CrossRef]
- Teoh, J.Y.; Chiu, P.K.; Chan, S.Y.; Poon, D.M.; Cheung, H.Y.; Hou, S.S.; Ng, C.F. Risk of ischemic stroke after androgen deprivation therapy for prostate cancer in the Chinese population living in Hong Kong. Jpn. J. Clin. Oncol. 2015, 45, 483–487. [Google Scholar] [CrossRef]
- Tsai, H.K.; D’Amico, A.V.; Sadetsky, N.; Chen, M.H.; Carroll, P.R. Androgen deprivation therapy for localized prostate cancer and the risk of cardiovascular mortality. J. Natl. Cancer Inst. 2007, 99, 1516–1524. [Google Scholar] [CrossRef]
- Nguyen, P.L.; Je, Y.; Schutz, F.A.; Hoffman, K.E.; Hu, J.C.; Parekh, A.; Beckman, J.A.; Choueiri, T.K. Association of androgen deprivation therapy with cardiovascular death in patients with prostate cancer: A metaanalysis of randomized trials. JAMA 2011, 306, 2359–2366. [Google Scholar] [CrossRef]
- Hayreh, S.S. Prevalent misconceptions about acute retinal vascular occlusive disorders. Prog. Retin. Eye Res. 2005, 24, 493–519. [Google Scholar] [CrossRef]
- O’Mahoney, P.R.; Wong, D.T.; Ray, J.G. Retinal vein occlusion and traditional risk factors for atherosclerosis. Arch. Ophthalmol. 2008, 126, 692–699. [Google Scholar] [CrossRef] [PubMed]
- Rudkin, A.K.; Lee, A.W.; Chen, C.S. Vascular risk factors for central retinal artery occlusion. Eye (Lond.) 2010, 24, 678–681. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wang, L.Y.; Jiang, T.Y.; Zhang, H.P.; Dou, Y.; Zhao, J.H.; Zhao, H.; Qiao, Z.D.; Qiao, J.T. Effects of testosterone and 17-beta-estradiol on TNF-alpha-induced E-selectin and VCAM-1 expression in endothelial cells. Analysis of the underlying receptor pathways. Life Sci. 2002, 71, 15–29. [Google Scholar] [CrossRef]
- Death, A.K.; Mcgrath, K.C.; Sader, M.A.; Nakhla, S.; Jessup, W.; Handelsman, D.J.; Celermajer, D.S. Dihydrotestosterone promotes vascular cell adhesion molecule-1 expression in male human endothelial cells via a nuclear factor-kappaB-dependent pathway. Endocrinology 2004, 145, 1889–1897. [Google Scholar] [CrossRef] [PubMed]
- Lanthier, A.; Patwardhan, V.V. In vitro steroid metabolism by rat retina. Brain Res. 1988, 463, 403–406. [Google Scholar] [CrossRef]
- Rocha, E.M.; Wickham, L.A.; da Silveira, L.A.; Krenzer, K.L.; Yu, F.S.; Toda, I.; Sullivan, B.D.; Sullivan, D.A. Identification of androgen receptor protein and 5α-reductase mRNA in human ocular tissues. Br. J. Ophthalmol. 2000, 84, 76–84. [Google Scholar] [CrossRef]
- Annibalini, G.; Agostini, D.; Calcabrini, C.; Martinelli, C.; Colombo, E.; Guescini, M.; Tibollo, P.; Stocchi, V.; Sestili, P. Effects of sex hormones on inflammatory response in male and female vascular endothelial cells. J. Endocrinol. Investig. 2014, 37, 861–869. [Google Scholar] [CrossRef]
- Dedania, V.S.; Zacks, D.N.; Pan, W.; VanderBeek, B.L. Testoserone supplementation and retinal vascular disease. Retina 2018, 38, 2247–2252. [Google Scholar] [CrossRef]
- Azoulay, L.; Yin, H.; Benayoun, S.; Renoux, C.; Boivin, J.F.; Suissa, S. Androgen deprivation therapy and the risk of stroke in patients with prostate cancer. Eur. Urol. 2011, 60, 1244–1250. [Google Scholar] [CrossRef]
- Chung, S.D.; Chen, Y.K.; Wu, F.J.; Lin, H.C. Hormone therapy for prostate cancer and the risk of stroke: A 5-year follow-up study. BJU Int. 2012, 109, 1001–1005. [Google Scholar] [CrossRef]
- Kaur, H.; Siemens, D.R.; Black, A.; Robb, S.; Barr, S.; Graham, C.H.; Othman, M. Effects of androgen-deprivation therapy on hypercoagulability in prostate cancer patients: A prospective, longitudinal study. Can. Urol. Assoc. J. 2017, 11, 33–38. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Liao, K.M.; Huang, Y.B.; Chen, C.Y.; Kuo, C.C. Risk of ischemic stroke in patients with prostate cancer receiving androgen deprivation therapy in Taiwan. BMC Cancer 2019, 19, 1263. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Control | Prostate Cancer without ADT | Prostate Cancer with ADT | p Value |
|---|---|---|---|---|
| Age at index date (years) | 0.9607 | |||
| <50 | 19 (0.53%) | 9 (0.50%) | 10 (0.56%) | |
| 50–59 | 220 (6.14%) | 101 (5.64%) | 107 (5.97%) | |
| 60–69 | 922 (25.74%) | 453 (25.29%) | 463 (25.85%) | |
| 70–79 | 1498 (41.82%) | 778 (43.44%) | 737 (41.15%) | |
| ≧80 | 923 (25.77%) | 450 (25.13%) | 474 (26.47%) | |
| Urbanization | 0.8220 | |||
| Urban | 2017 (56.31%) | 995 (55.56%) | 982 (54.83%) | |
| Sub-urban | 1160 (32.38%) | 580 (32.38%) | 596 (33.28%) | |
| Rural | 405 (11.31%) | 216 (12.06%) | 213 (11.89%) | |
| Occupation | 0.7806 | |||
| Government employees | 279 (7.79%) | 138 (7.71%) | 139 (7.76%) | |
| Labor | 1336 (37.30%) | 661 (36.91%) | 657 (36.68%) | |
| Farmer and fisherman | 1047 (29.23%) | 553 (30.88%) | 529 (29.54%) | |
| Low income | 13 (0.36%) | 13 (0.73%) | 12 (0.67%) | |
| Unemployed | 855 (23.87%) | 401 (22.39%) | 428 (23.90%) | |
| Others | 52 (1.45%) | 25 (1.40%) | 26 (1.45%) | |
| Education years | 0.8728 | |||
| <6 | 1987 (55.47%) | 989 (55.22%) | 971 (54.22%) | |
| 6–9 | 454 (12.67%) | 235 (13.12%) | 253 (14.13%) | |
| 9–12 | 830 (23.17%) | 408 (22.78%) | 408 (22.78%) | |
| ≥12 | 311 (8.68%) | 159 (8.88%) | 159 (8.88%) | |
| Comorbidities | ||||
| Hypertension | 1907 (53.24%) | 951 (53.10%) | 961 (53.66%) | 0.9389 |
| DM | 637 (17.78%) | 336 (18.76%) | 360 (20.10%) | 0.1182 |
| CAD | 567 (15.83%) | 287 (16.02%) | 316 (17.64%) | 0.2185 |
| AMI | 17 (0.47%) | 10 (0.56%) | 13 (0.73%) | 0.5072 |
| Hyperlipidemia | 616 (17.20%) | 291 (16.25%) | 326 (18.20%) | 0.3010 |
| Cerebrovascular disease | 430 (12.00%) | 227 (12.67%) | 238 (13.29%) | 0.3920 |
| Dementia | 91 (2.54%) | 47 (2.62%) | 56 (3.13%) | 0.4446 |
| Retinopathy-related medications | ||||
| Aminoquinolines | 7 (0.20%) | 4 (0.22%) | 4 (0.22%) | 0.9671 |
| Phenothiazines | 13 (0.36%) | 18 (1.01%) | 9 (0.50%) | 0.0111 |
| Nitrofurantoin | 0 (0.00%) | 20 (1.12%) | 0 (0.00%) | - |
| ADT type | - | |||
| LHRH agonists | 1108 (61.86%) | |||
| Antiandrogens | 1212 (67.67%) | |||
| Estrogens | 140 (7.82%) | |||
| Bilateral orchiectomy | 202 (11.28%) | |||
| Procedure prior to ADT | ||||
| Surgery | 589 (32.89%) | |||
| Radiotherapy | 547 (30.54%) | |||
| Combined surgery and radiotherapy | 649 (36.24%) | |||
| None | 6 (0.33%) |
| Event | Control | Prostate Cancer without ADT | Prostate Cancer with ADT |
|---|---|---|---|
| Follow-up (person month) | 236,871 | 122,287 | 96,035 |
| New case | 38 | 10 | 3 |
| Incidence rate # (95% CI) | 1.60 (1.17–2.20) | 0.82 (0.44–1.52) | 0.31 (0.10–0.97) |
| Crude relative risk (95% CI) | Reference | 0.509 (0.254–1.022) | 0.196 (0.061–0.636) * |
| Adjusted HR (95% CI) | Reference | 0.525 (0.261–1.056) | 0.191 (0.059–0.621) * |
| Covariate | aHR | 95% CI | p Value |
|---|---|---|---|
| Group | |||
| Control | Reference | ||
| Prostate cancer without ADT | 0.525 | 0.261–1.056 | 0.0707 * |
| Prostate cancer with ADT | 0.191 | 0.059–0.621 | 0.0059 * |
| Age (years) | |||
| <50 | - | ||
| 50–59 | |||
| 60–69 | 3.566 | 0.466–27.281 | 0.2207 |
| 70–79 | 3.099 | 0.405–23.739 | 0.2762 |
| ≧80 | 4.107 | 0.511–32.997 | 0.1839 |
| Urbanization | |||
| Urban | |||
| Sub-urban | 0.981 | 0.495–1.945 | 0.9572 |
| Rural | 1.184 | 0.412–3.399 | 0.7535 |
| Occupation | |||
| Government employees | 1.338 | 0.480–3.728 | 0.5772 |
| Labor | |||
| Farmer and fisherman | 0.757 | 0.312–1.838 | 0.5391 |
| Low income | 5.238 | 0.581–47.240 | 0.1400 |
| Unemployed | 0.988 | 0.456–2.141 | 0.9749 |
| Others | 1.826 | 0.226–14.764 | 0.5724 |
| Education years | |||
| <6 | 1.436 | 0.546–3.773 | 0.4632 |
| 6–9 | |||
| 9–12 | 1.642 | 0.586–4.598 | 0.3454 |
| ≥12 | 0.855 | 0.200–3.652 | 0.8326 |
| Comorbidities | |||
| Hypertension | 2.130 | 1.127–4.027 | 0.0199 * |
| DM | 1.600 | 0.817–3.135 | 0.1707 |
| CAD | 0.770 | 0.348–1.704 | 0.5195 |
| AMI | 5.279 | 0.677–41.141 | 0.1122 |
| Hyperlipidemia | 0.390 | 0.149–1.022 | 0.0555 |
| Cerebrovascular disease | 1.187 | 0.543–2.597 | 0.6671 |
| Dementia | 1.070 | 0.143–8.003 | 0.9475 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, H.-L.; Lee, C.-Y.; Huang, J.-Y.; Tseng, P.-C.; Yang, S.-F. Androgen Deprivation Therapy for Prostate Cancer Did Not Increase the Risk of Retinal Vascular Occlusion: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 2268. https://doi.org/10.3390/ijerph19042268
Lin H-L, Lee C-Y, Huang J-Y, Tseng P-C, Yang S-F. Androgen Deprivation Therapy for Prostate Cancer Did Not Increase the Risk of Retinal Vascular Occlusion: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(4):2268. https://doi.org/10.3390/ijerph19042268
Chicago/Turabian StyleLin, Hsin-Le, Chia-Yi Lee, Jing-Yang Huang, Po-Chen Tseng, and Shun-Fa Yang. 2022. "Androgen Deprivation Therapy for Prostate Cancer Did Not Increase the Risk of Retinal Vascular Occlusion: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 19, no. 4: 2268. https://doi.org/10.3390/ijerph19042268
APA StyleLin, H.-L., Lee, C.-Y., Huang, J.-Y., Tseng, P.-C., & Yang, S.-F. (2022). Androgen Deprivation Therapy for Prostate Cancer Did Not Increase the Risk of Retinal Vascular Occlusion: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health, 19(4), 2268. https://doi.org/10.3390/ijerph19042268