
COVID-19 Pandemic Lockdown and Wellbeing: Experiences from Aotearoa New Zealand in 2020

 , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Aotearoa New Zealand COVID-19 Response
Implications for Mental Health and Wellbeing
1.2. Research Focus
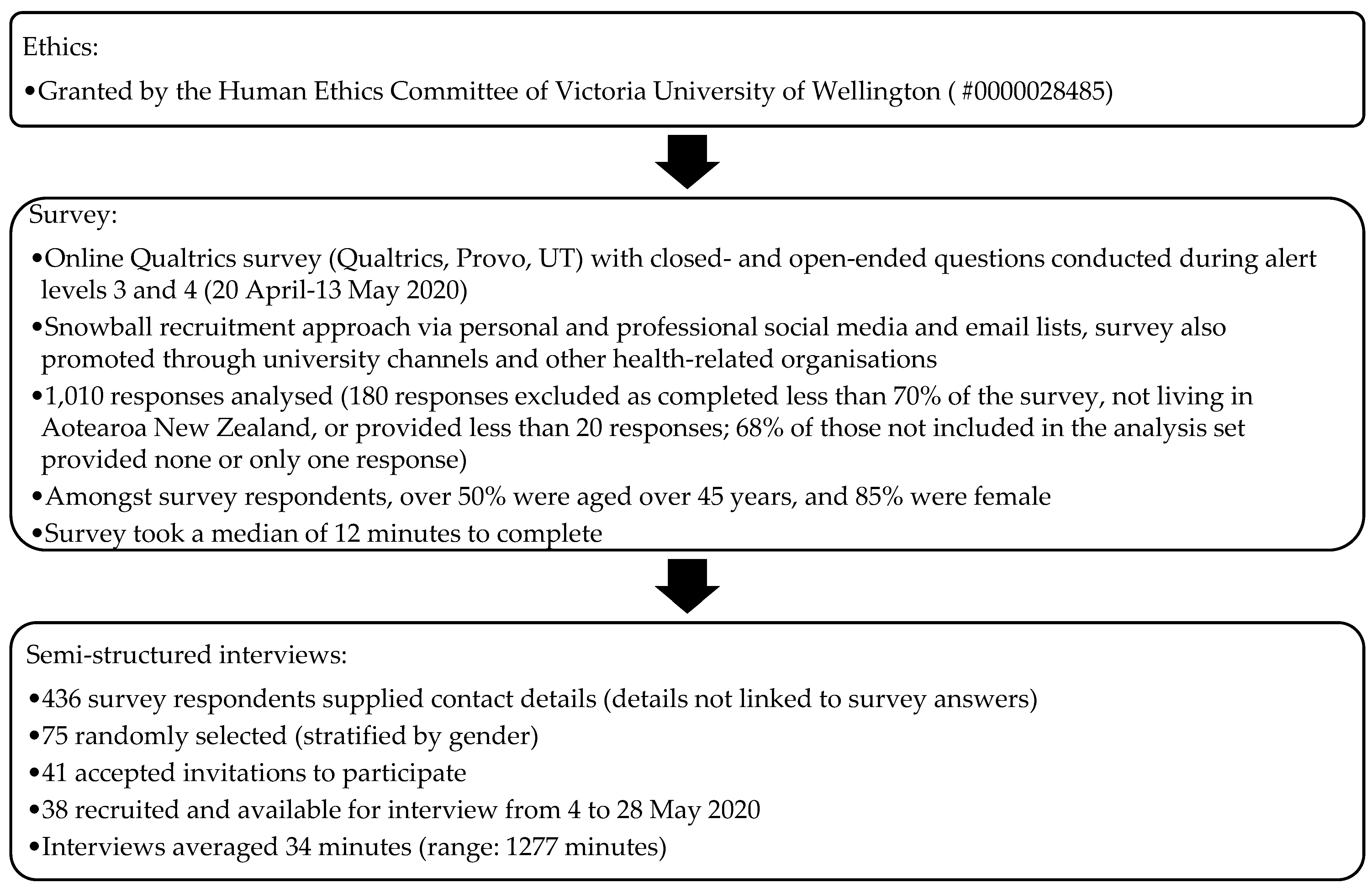
2. Materials and Methods
Qualitative Analysis
3. Results
3.1. Community-Led Solutions
3.1.1. Household Relationships and Responsibilities
What a different experience it would have been had we been here on our own… Having the two littlies certainly was not an unpleasant experience because we had the constant company and the constant joyfulness of young people… It was quite a different experience to a lot of my colleagues and friends who found it very isolating and very lonely.(I: 65-74, F)
Since lockdown, I have my son staying with me while he awaits social housing. He suffers from schizophrenia which can be extremely stressful to live with in my small 1bdrm flat. He is on waiting list for a flat but nothing is happening due to lockdown so it is very hard. I have lost 10 kgs in weight.(S: 55-64, F)
To be honest it’s made me a little bit unhappy just being cooped up with one person.(I: 65-74, M)
Working from home with children has been extremely stressful. You are constantly having to prioritise your kids’ education or your work. Who are you loyal to? The one giving you money or the ones you gave life to?(S: 25-34, F)
Households don’t necessarily represent… family connections [for Pacific]. You have to allow that opportunity to… co-bubble with different households.(I: 45-54, F)
Because my mother-in-law lives alone, we discovered it was within the rules to invite her into our bubble… [It] was just a win-win situation… with her watching her grandson and getting some interaction… It gave both of us space to be able to do our work.(I: 25-34, M)
I have a parent who lives alone, an elderly parent, I am her person… As soon as the [first alert] level announcement happened… it was like “right, that’s it, you [elderly parent] are not leaving the house”… I have to do… [everything] she needed… [It was] quite a lot of pressure… if I fall over, there is nobody else.(I: 45-54, F)
3.1.2. Telecommunications
My parents who are elderly in Dunedin and my siblings spread around the country, we set up a videoconferencing group, so we connect every three or four nights.(I: 55-64, F)
I started doing some Skype calls or WhatsApp calls to touch base with more family members during lockdown because I was needing that… I got back in touch with some friends and family that I didn’t for some time.(I: 25-34, F)
With family overseas,… you need to calculate all the time the time difference… If I want to speak with my mum right now, I can’t call her because it’s 4 am… I just kept in touch a lot more… I really needed it in lockdown.(I: 25-34, F)
People who don’t know how to access the internet… We would have to be here to set it up for Dad, otherwise, he won’t be able to access his Zoom.(I: 45-54, F)
I socialise with a lot of friends just through Zoom… I’ll probably keep that up,… twice a week I catch up with my family who are spread [globally].(I: 25-34, M)
3.1.3. Community and Neighbourly Relationships
I’m thankful for the free food parcels that the local community organisations have been giving out, as some families have faced hardships… and it would have made a big impact on their health and wellbeing.(S: 45-54, F)
Disappointed by lack of neighbourly support. Confusion over [the rule of not] going to the supermarket because of over 70 age. Supermarket not delivering goods to customers.(S: 75-84, F)
My neighbour down the road has health issues and because of the [co-occurring] drought, they ran out of water and usually I would say, “Come over and grab some water.”… [Instead,] I said, “Oh, I don’t think it’s a good idea because of COVID”.(I: 35-44, F)
When things got tense with my flatmate… I reached out to my neighbours by phone… She said to “file a Police report”… You’re trapped inside lockdown…, there were no options. Even though I could reach out to my neighbours, none of them could come.(I: 45-54, F)
3.2. Whānau (Family) and Individuals Look after Their Mental Wellbeing
3.2.1. Physical Lifestyle and Behaviour Changes
I’m doing more AFDs [alcohol-free days] than I used to… It would be terribly easy to get into soaking up a bottle a night… I’m… mindful and don’t let it get away.(I: 55-64, M)
I started out exercising more and I ended up drinking more… A couple of weeks ago I was like… ‘This is temporary, it’s fine if I just do whatever.’ And then I was thinking, ‘Maybe I should get back into good habits.’(I: 25-34, F)
The big thing has been about creating routine,… having purposeful work and at times when my work has not felt purposeful, that’s some of the times I’ve really struggled.(I: 45-54, F)
I am a diabetic, and my 10 h/day physical job is a large part of keeping my sugar levels in check. Being off-work, gyms closed, pools closed, not being allowed to kick a ball around…, I have regressed mentally to the point of being totally locked-in.(S: 55-64, M)
When we were in Level 4 and my husband was home, we were walking during the day, it was beautiful, and just doing things we never usually do… Because I’ve got a mobile phone for work and everything, I just took it with me. That kind of lifestyle freedom was- it’s beautiful.(I: 45-54, F)
3.2.2. Pace of Life and Mindset
People were saying they couldn’t wait to get into shopping centres… You know when you’re in a shop,… you see things and you buy them, and I’ve found [without the shops] financially I feel better off,… It has been great, almost like a reset…(I: 45-54, F)
I was diagnosed with breast cancer just right at the start, so I actually think it’s worked really well because the whole world has slowed down. So, for me, being in lockdown actually meant that it wasn’t so stressful.(I: 45-54, F)
Everybody else was out going for walks with their dogs and biking and things. I left home when it was dark and come home when it was dark… My lifestyle over this whole period is worse… I had all these great intentions… but I just haven’t…(I: 45-54, F)
Almost 21 years I have napped… since we’ve been in lockdown I don’t need to sleep during the day… It tells me that being around so many people actually is exhausting.(I: 45-54, F)
If we could just get through this blasted thing, with our mental health not too badly damaged, that’s a win. You’ve probably seen various comments on this online—if you don’t get through without learning three new skills, what kind of a person are you?... I’m a little bit careful not to set myself too ambitious goals for getting through this.(I: 55-64, M)
I just have a greater appreciation for the sense of connection and reliance that we have on one another… I am reliant on everybody in the community and they are reliant on me. So, when I buy my coffee now, I’m consciously choosing who I buy it from and it’s an investment in their lives… that carries a different spiritual experience.(I: 45-54, F)
3.2.3. Stuck or Safe at Home
Since I don’t go out and socialise,… it wasn’t really a big change. I’m actually finding now that I really like it, so the whole stuck at home syndrome or whatever they’re calling it now, I’m actually quite liking it.(I: 55-64, F)
When D and R go to work [at essential jobs] and it just being me, eight hours a day and I would sort of be looking at these walls, and finding anything possible that I could clean… I am an extrovert, I need to be connecting with people all the time, that [lockdown] just became a bit hard.(I: 45-54, F)
I didn’t like getting stuck in the house… [But] if you look at the situation and weigh up everything, we are very lucky. Although there is a lockdown, we are still able to go out and go to the park… [But] you have to be doing something, you can’t wait in the house, that is waiting to die.(I: 75+, M)
I have suffered less from my arthritis… whilst working from home, and not having to commute a long distance by car, [but]… I have missed out on the flu vaccine I would normally have received… I have also had a regular mole map screening postponed, and a blood test and CV risk review have been postponed.(S: 55-64, F)
Both my parents are almost 80 and my ex-partner is a diabetic and he’s recovering from surgery and so I was like, right, well you three are incredibly vulnerable… I didn’t feel like I could play fast and loose with any of the restrictions.(I: 35-44, F)
[Going out] I had got quite distressed because the general energy… was an unpleasant sort of racy, kind of everyone on edge, super-suspicious kind of sketchy feel to it.(I: 45-54, F)
3.3. Primary and Specialist Mental Health and Wellbeing Support
3.3.1. Accessibility
My mother rang the 1737 line [Mental Health Helpline]… It took two phone conversations and 25 minutes of being on the line before anyone answered her. I understand that there is pressure on this sector due to not having enough service available… How many of our people have… ended their life because they haven’t been able to talk to someone.(S: 45-54, F)
I wouldn’t know how to access counselling services or mental health services in my community. GP, yes, but anything else, I don’t know,… If I was experiencing isolation, issues of suicide and I was on my own, I wouldn’t know, who do you ring, do you still ring Healthline because no one is on the other line of those crisis centres, are they still open?(I: 45-54, F)
I freaking attempted suicide… I felt I couldn’t even seek mental health care because the services were already stretched more and they had to go slower to disinfect everything between people. So, I got no help. Nobody knows what happened and I’m stuck still.(S: 18-24, F)
I have been unable to access mental health support during the second half of the lock-down as my psychologist became unavailable. This has severely impacted my mental health during transition periods between alert levels.(S: 18-24, F)
The mental health service delivery for my husband and myself has been awful, with restricted access to respite even when beds are available, overly coercive practices during admission and unnecessarily restrictive processes within the unit that mean even patients in the open ward cannot go for a single walk outside each day escorted by staff.(S: 35-44, F)
3.3.2. The Form of Service Delivery
This is four weeks since somebody touched me, and it’s to draw my blood, it was just the weirdest thing… I lost something in the four weeks… I don’t know why it’s so meaningful but there is… a sadness,… grief.(I: 25-34, F)
I suffer from anxiety and depression anyway, but unfortunately exacerbated a lot during lockdown because on top of that my dad’s got terminal cancer, and I was denied compassionate grounds to travel to see him by the Government. So that deeply affected me.(I: 45-54, F)
Sometimes when it comes to asking the straight-up questions a GP asks about mental health conditions, it’s just a bit easier to do it over the phone rather than have a pair of eyes staring at you.(S: 18-24, F)
If I were in a serious mental health crisis and I was to find myself on the phone with them; I’d find it really unsafe for them as well as me… There’s so much more they can assess… if I was physically present.(I: 25-34, M)
Sometimes we’ll have really good conversations, but then I’ll be like… is someone from my family… has anybody heard? You can’t let your guard down in the way that you normally would.(I: 35-44, F)
3.3.3. Clinician–Patient Relationships
When I’m starting to hear voices or… getting intrusive flashbacks or intrusive thinking, what potential risk that poses in terms of talking to a health professional… I was really grateful that… I had an established relationship with my GP... And she followed up with me.(I: 45-54, F)
I found it hard for the consult surrounding my mental distress to be upset on the phone. It felt less personal. I am so grateful that I had a longer-term relationship with my GP. If I hadn’t I would not have felt okay to contact a GP. I just would not have done it.(S: 35-44, F)
I had an absolutely terrible experience with (a call centre) when I was concerned I had COVID-19. The member of staff I spoke to was incredibly dispassionate, uninterested in helping me and useless, leaving me feeling anxious and helpless.(S: 18-24, F)
I’m terrified as a disabled person that my health might be compromised during the pandemic, not just the risk of COVID-19 but that my health as a disabled patient isn’t a priority (to others).(S: 35-44, gender diverse)
3.4. Social and Economic Foundations
[My wife’s] boss was rather inflexible and wanted her staff to all do online meetings and professional development… which was equivalent to sort of full-time work… [This] made it quite challenging with a one-and-a-half-year-old who needs constant attention.(I: 25-34, M)
I actually find it slightly less stressful because I have plenty of quiet time to myself… In my office, we’ve talked about that we will be more flexible… I’m likely to establish a regular routine where I work from home… I don’t really need to go to the office… it’s nice to work from home.(I: 45-54, M)
It was an awful letter they [the workplace] sent to everyone just saying you are an essential worker, you must come to work. If you are over 70 or a vulnerable person you may use your holiday leave and then take leave without pay... And there’s people that have to make those awful decisions about working for a place where they feel unsupported or not coping financially.(I: 45-54, F)
From going from a good pay to a little pay and still have to pay child support, I had to use a bit of my annual leave, just to survive this… I’m behind in all my bills, letters coming asking to pay.(S: 35-44, F)
We had some staff who said,… ‘It’s going to cost us so much more for power and heating all day while we’re working’. It was like, but you are working, you are getting an income,… there are people who have lost their lives,… their jobs,… their livelihood.(I: 45-54, F)
4. Discussion
- The role of the community, households, and long-distance relationships;
- The dichotomy between feeling safer at home and undergoing positive behaviour changes, and feeling stuck at home while managing work and health issues;
- Accessibility and appropriateness of formal mental health support; and
- Social and economic factors.
Limitations and Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Mental Health and Psychosocial Considerations during the COVID-19 Outbreak; World Health Organization: Geneva, Switzerland, 2020.
- Adhanom Ghebreyesus, T. Addressing mental health needs: An integral part of COVID-19 response. World Psychiatry 2020, 19, 129–130. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef] [PubMed]
- Gloster, A.T.; Lamnisos, D.; Lubenko, J.; Presti, G.; Squatrito, V.; Constantinou, M.; Nicolaou, C.; Papacostas, S.; Aydın, G.; Chong, Y.Y.; et al. Impact of COVID-19 pandemic on mental health: An international study. PLoS ONE 2021, 15, e0244809. [Google Scholar] [CrossRef]
- Pierce, M.; Hope, H.; Ford, T.; Hatch, S.; Hotopf, M.; John, A.; Kontopantelis, E.; Webb, R.; Wessely, S.; McManus, S.; et al. Mental health before and during the COVID-19 pandemic: A longitudinal probability sample survey of the UK population. Lancet Psychiatry 2020, 7, 883–892. [Google Scholar] [CrossRef]
- Marshall, L.; Bibby, J.; Abbs, I. Emerging Evidence on COVID-19′s Impact on Mental Health and Health Inequalities. Available online: https://www.health.org.uk/news-and-comment/blogs/emerging-evidence-on-covid-19s-impact-on-mental-health-and-health?utm_source=charityemail&utm_medium=email&utm_campaign=jun-2020&pubid=healthfoundation&description=jun-2020&dm_i=4Y2,6XD7S,1Q239,RUIY3,1 (accessed on 19 December 2021).
- Allwood, L.; Bell, A. COVID-19: Understanding Inequalities in Mental Health during the Pandemic; Centre for Mental Health: London, UK, 2020. [Google Scholar]
- Mental Health Foundation UK. The COVID-19 Pandemic, Financial Inequality and Mental Health; Mental Health Foundation UK: London, UK, 2020. [Google Scholar]
- O’Connor, R.C.; Wetherall, K.; Cleare, S.; McClelland, H.; Melson, A.J.; Niedzwiedz, C.L.; O’Carroll, R.E.; O’Connor, D.B.; Platt, S.; Scowcroft, E.; et al. Mental health and well-being during the COVID-19 pandemic: Longitudinal analyses of adults in the UK COVID-19 Mental Health & Wellbeing study. Br. J. Psychiatry 2021, 218, 326–333. [Google Scholar] [CrossRef]
- White, R.G.; Van Der Boor, C. Impact of the COVID-19 pandemic and initial period of lockdown on the mental health and well-being of adults in the UK. BJPsych Open 2020, 6, e90. [Google Scholar] [CrossRef]
- Dawel, A.; Shou, Y.; Smithson, M.; Cherbuin, N.; Banfield, M.; Calear, A.L.; Farrer, L.M.; Gray, D.; Gulliver, A.; Housen, T.; et al. The effect of COVID-19 on mental health and wellbeing in a representative sample of Australian adults. Front. Psychiatry 2020, 11, 579985. [Google Scholar] [CrossRef]
- Gori, A.; Topino, E. Across the COVID-19 Waves; Assessing Temporal Fluctuations in Perceived Stress, Post-Traumatic Symptoms, Worry, Anxiety and Civic Moral Disengagement over One Year of Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 5651. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.K.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef]
- Hyland, P.; Shevlin, M.; Murphy, J.; McBride, O.; Fox, R.; Bondjers, K.; Karatzias, T.; Bentall, R.P.; Martinez, A.; Vallières, F. A longitudinal assessment of depression and anxiety in the Republic of Ireland before and during the COVID-19 pandemic. Psychiatry Res. 2021, 300, 113905. [Google Scholar] [CrossRef] [PubMed]
- Creese, B.; Khan, Z.; Henley, W.; O’Dwyer, S.; Corbett, A.; Vasconcelos Da Silva, M.; Mills, K.; Wright, N.; Testad, I.; Aarsland, D.; et al. Loneliness, physical activity, and mental health during COVID-19: A longitudinal analysis of depression and anxiety in adults over the age of 50 between 2015 and 2020. Int. Psychogeriatr. 2021, 33, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Boldrini, M.; Canoll, P.D.; Klein, R.S. How COVID-19 Affects the Brain. JAMA Psychiatry 2021, 78, 682–683. [Google Scholar] [CrossRef] [PubMed]
- Low, R.; Overall, N.; Chang, V.; Henderson, A.; Sibley, C. Emotion regulation and psychological and physical health during a nationwide COVID-19 lockdown. Emotion 2021, 21, 1671–1690. [Google Scholar] [CrossRef] [PubMed]
- Kousoulis, A.A.; Van Bortel, T.; Hernandez, P.; John, A. The long term mental health impact of covid-19 must not be ignored. BMJ Opin. 2020. Available online: https://blogs.bmj.com/bmj/2020/05/05/the-long-term-mental-health-impact-of-covid-19-must-not-be-ignored/ (accessed on 19 December 2021).
- Chu, I.Y.-H.; Alam, P.; Larson, H.J.; Lin, L. Social consequences of mass quarantine during epidemics: A systematic review with implications for the COVID-19 response. J. Travel Med. 2020, 27, taaa192. [Google Scholar] [CrossRef]
- Ausín, B.; González-Sanguino, C.; Castellanos, M.Á.; Muñoz, M. Gender-related differences in the psychological impact of confinement as a consequence of COVID-19 in Spain. J. Gend. Stud. 2021, 30, 29–38. [Google Scholar] [CrossRef]
- van Tilburg, T.G.; Steinmetz, S.; Stolte, E.; van der Roest, H.; de Vries, D.H. Loneliness and Mental Health During the COVID-19 Pandemic: A Study Among Dutch Older Adults. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e249–e255. [Google Scholar] [CrossRef]
- Bu, F.; Steptoe, A.; Fancourt, D. Who is lonely in lockdown? Cross-cohort analyses of predictors of loneliness before and during the COVID-19 pandemic. Public Health 2020, 186, 31–34. [Google Scholar] [CrossRef]
- Luchetti, M.; Lee, J.H.; Aschwanden, D.; Sesker, A.; Strickhouser, J.E.; Terracciano, A.; Sutin, A.R. The trajectory of loneliness in response to COVID-19. Am. Psychol. 2020, 75, 897–908. [Google Scholar] [CrossRef]
- McGinty, E.E.; Presskreischer, R.; Han, H.; Barry, C.L. Psychological Distress and Loneliness Reported by US Adults in 2018 and April 2020. JAMA 2020, 324, 93–94. [Google Scholar] [CrossRef]
- Prime, H.; Wade, M.; Browne, D.T. Risk and resilience in family well-being during the COVID-19 pandemic. Am. Psychol. 2020, 75, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Kerr, M.L.; Rasmussen, H.F.; Fanning, K.A.; Braaten, S.M. Parenting During COVID-19: A Study of Parents’ Experiences Across Gender and Income Levels. Fam. Relat. 2021, 70, 1327–1342. [Google Scholar] [CrossRef] [PubMed]
- Patrick, S.W.; Henkhaus, L.E.; Zickafoose, J.S.; Lovell, K.; Halvorson, A.; Loch, S.; Letterie, M.; Davis, M.M. Well-being of Parents and Children during the COVID-19 Pandemic: A National Survey. Pediatrics 2020, 146, e2020016824. [Google Scholar] [CrossRef] [PubMed]
- Gassman-Pines, A.; Ananat, E.O.; Fitz-Henley, J., 2nd. COVID-19 and Parent-Child Psychological Well-being. Pediatrics 2020, 146, e2020007294. [Google Scholar] [CrossRef] [PubMed]
- Daks, J.S.; Peltz, J.S.; Rogge, R.D. Psychological flexibility and inflexibility as sources of resiliency and risk during a pandemic: Modeling the cascade of COVID-19 stress on family systems with a contextual behavioral science lens. J. Contextual Behav. Sci. 2020, 18, 16–27. [Google Scholar] [CrossRef] [PubMed]
- McLaren, H.J.; Wong, K.R.; Nguyen, K.N.; Mahamadachchi, K.N.D. Covid-19 and women’s triple burden: Vignettes from Sri Lanka, Malaysia, Vietnam and Australia. Soc. Sci. 2020, 9, 87. [Google Scholar] [CrossRef]
- Chu, K.A.; Schwartz, C.; Towner, E.; Kasparian, N.A.; Callaghan, B. Parenting under pressure: A mixed-methods investigation of the impact of COVID-19 on family life. J. Affect. Disord. Rep. 2021, 5, 100161. [Google Scholar] [CrossRef]
- Mooi-Reci, I.; Risman, B.J. The Gendered Impacts of COVID-19: Lessons and Reflections. Gend. Soc. 2021, 35, 161–167. [Google Scholar] [CrossRef]
- Schieman, S.; Badawy, P.J.; Milkie, M.A.; Bierman, A. Work-Life Conflict During the COVID-19 Pandemic. Socius 2021, 7, 2378023120982856. [Google Scholar] [CrossRef]
- Lades, L.K.; Laffan, K.; Daly, M.; Delaney, L. Daily emotional well-being during the COVID-19 pandemic. Br. J. Health Psychol. 2020, 25, 902–911. [Google Scholar] [CrossRef] [PubMed]
- Jefferies, S.; French, N.; Gilkison, C.; Graham, G.; Hope, V.; Marshall, J.; McElnay, C.; McNeill, A.; Muellner, P.; Paine, S.; et al. COVID-19 in New Zealand and the impact of the national response: A descriptive epidemiological study. Lancet Public Health 2020, 5, e612–e623. [Google Scholar] [CrossRef]
- ESR. NZ COVID-19 Dashboard. Available online: https://nzcoviddashboard.esr.cri.nz/#!/ (accessed on 19 December 2021).
- Cumming, J. COVID-19 Health System Response Monitor: New Zealand; World Health Organization Regional Office for South-East Asia: New Delhi, India, 2021. [Google Scholar]
- Steyn, N.; Binny, R.N.; Hannah, K.; Hendy, S.C.; James, A.; Kukutai, T.; Lustig, A.; McLeod, M.; Plank, M.J.; Ridings, K.; et al. Estimated inequities in COVID-19 infection fatality rates by ethnicity for Aotearoa New Zealand. N. Z. Med. J. 2020, 133, 28–39. [Google Scholar] [PubMed]
- Steyn, N.; Binny, R.N.; Hannah, K.; Hendy, S.C.; James, A.; Lustig, A.; Ridings, K.; Plank, M.J.; Sporle, A. Māori and Pacific people in New Zealand have a higher risk of hospitalisation for COVID-19. N. Z. Med. J. 2021, 134, 28–43. [Google Scholar]
- Waitangi Tribunal. Haumaru: The COVID-19 Priority Report—Pre-Publication Version; Waitangi Tribunal: Wellington, New Zealand, 2021. [Google Scholar]
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; Webster, S.; Cameron-Blake, E.; Hallas, L.; Majumdar, S.; et al. A Global Panel Database of Pandemic Policies (Oxford COVID-19 Government Response Tracker). Nat. Hum.Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- Ministry of Health. History of the COVID-19 Alert System. Available online: https://covid19.govt.nz/about-our-covid-19-response/history-of-the-covid-19-alert-system/#alert-levels (accessed on 17 December 2021).
- Kearns, N.; Shortt, N.; Kearns, C.; Eathorne, A.; Holliday, M.; Mackle, D.; Martindale, J.; Semprini, A.; Weatherall, M.; Beasley, R.; et al. How big is your bubble? Characteristics of self-isolating household units (‘bubbles’) during the COVID-19 Alert Level 4 period in New Zealand: A cross-sectional survey. BMJ Open 2021, 11, e042464. [Google Scholar] [CrossRef]
- Ministry of Health. COVID-19: Vaccine Data. Available online: https://www.health.govt.nz/our-work/diseases-and-conditions/covid-19-novel-coronavirus/covid-19-data-and-statistics/covid-19-vaccine-data (accessed on 10 January 2021).
- New Zealand Doctor. Timeline Coronavirus. Available online: https://www.nzdoctor.co.nz/timeline-coronavirus (accessed on 17 December 2021).
- Every-Palmer, S.; Jenkins, M.; Gendall, P.; Hoek, J.; Beaglehole, B.; Bell, C.; Williman, J.; Rapsey, C.; Stanley, J. Psychological distress, anxiety, family violence, suicidality, and wellbeing in New Zealand during the COVID-19 lockdown: A cross-sectional study. PLoS ONE 2020, 15, e0241658. [Google Scholar] [CrossRef]
- Bell, C.; Williman, J.; Beaglehole, B.; Stanley, J.; Jenkins, M.; Gendall, P.; Rapsey, C.; Every-Palmer, S. Psychological distress, loneliness, alcohol use and suicidality in New Zealanders with mental illness during a strict COVID-19 lockdown. Aust. N. Z. J. Psychiatry 2021, 48674211034317. [Google Scholar] [CrossRef]
- Sibley, C.G.; Greaves, L.M.; Satherley, N.; Wilson, M.S.; Overall, N.C.; Lee, C.H.J.; Milojev, P.; Bulbulia, J.; Osborne, D.; Milfont, T.L.; et al. Effects of the COVID-19 pandemic and nationwide lockdown on trust, attitudes toward government, and well-being. Am. Psychol. 2020, 75, 618–630. [Google Scholar] [CrossRef]
- Gasteiger, N.; Vedhara, K.; Massey, A.; Jia, R.; Ayling, K.; Chalder, T.; Coupland, C.; Broadbent, E. Depression, anxiety and stress during the COVID-19 pandemic: Results from a New Zealand cohort study on mental well-being. BMJ Open 2021, 11, e045325. [Google Scholar] [CrossRef]
- Nicolson, M.N.; Flett, J.A. The mental wellbeing of New Zealanders during and post-lockdown. N. Z. Med. J. 2020, 133, 110–112. [Google Scholar] [PubMed]
- Bell, C.; Williman, J.; Beaglehole, B.; Stanley, J.; Jenkins, M.; Gendall, P.; Rapsey, C.; Every-Palmer, S. Challenges facing essential workers: A cross-sectional survey of the subjective mental health and well-being of New Zealand healthcare and ‘other’ essential workers during the COVID-19 lockdown. BMJ Open 2021, 11, e048107. [Google Scholar] [CrossRef] [PubMed]
- Joyce, L.R.; Richardson, S.K.; McCombie, A.; Hamilton, G.J.; Ardagh, M.W. Mental health presentations to Christchurch Hospital Emergency Department during COVID-19 lockdown. Emerg. Med. Australas. 2021, 33, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Dicker, B.; Swain, A.; Todd, V.F.; Tunnage, B.; McConachy, E.; Drake, H.; Brett, M.; Spearing, D.; Howie, G.J. Changes in demand for emergency ambulances during a nationwide lockdown that resulted in elimination of COVID-19: An observational study from New Zealand. BMJ Open 2020, 10, e044726. [Google Scholar] [CrossRef]
- Salvation Army. SPPU COVID-19 Social Impact Dashboard—Report 5; Salvation Army: Wellington, New Zealand, 2020. [Google Scholar]
- Elers, C.; Jayan, P.; Elers, P.; Dutta, M.J. Negotiating health amidst COVID-19 lockdown in low-income communities in Aotearoa New Zealand. Health Commun. 2021, 36, 109–115. [Google Scholar] [CrossRef]
- Ministry of Health. COVID-19 Health and Wellbeing Survey: Week 13 Results; Ministry of Health: Wellington, New Zealand, 2020. [Google Scholar]
- Prickett, K.C.; Fletcher, M.; Chapple, S.; Doan, N.; Smith, C. Life in Lockdown: The Economic and Social Effect of Lockdown during Alert Level 4 in New Zealand; Victoria University of Wellington: Wellington, New Zealand, 2020. [Google Scholar]
- Jenkins, M.; Hoek, J.; Jenkin, G.; Gendall, P.; Stanley, J.; Beaglehole, B.; Bell, C.; Rapsey, C.; Every-Palmer, S. Silver linings of the COVID-19 lockdown in New Zealand. PLoS ONE 2021, 16, e0249678. [Google Scholar] [CrossRef]
- Nielsen. Impact of COVID-19; Health Promotion Agency: Wellington, New Zealand, 2020. [Google Scholar]
- Ministry of Health. Kia Kaha, Kia Māia, Kia Ora Aotearoa: COVID-19 Psychosocial and Mental Wellbeing Recovery Plan; Ministry of Health: Wellington, New Zealand, 2020.
- Poulton, R.; Gluckman, P.; Menzeis, R.; Bardsley, A.; McIntosh, T.; Faleafa, M. Protecting and Promoting Mental Wellbeing during (and after) COVID-19. ‘The Future is Now’ Conversation Series; University of Auckland: Auckland, New Zealand, 2020. [Google Scholar]
- McCartan, C.; Adell, T.; Cameron, J.; Davidson, G.; Knifton, L.; McDaid, S.; Mulholland, C. A scoping review of international policy responses to mental health recovery during the COVID-19 pandemic. Health Res. Policy Syst. 2021, 19, 58. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual. Res. Psychol. 2021, 18, 328–352. [Google Scholar] [CrossRef]
- Byrne, D. A worked example of Braun and Clarke’s approach to reflexive thematic analysis. Qual. Quant. 2021. [Google Scholar] [CrossRef]
- New Zealand Government. Digital Inclusion and Wellbeing in New Zealand. Available online: https://www.digital.govt.nz/dmsdocument/161~digital-inclusion-and-wellbeing-in-new-zealand/html (accessed on 23 November 2021).
- Pirkis, J.; John, A.; Shin, S.; DelPozo-Banos, M.; Arya, V.; Analuisa-Aguilar, P.; Appleby, L.; Arensman, E.; Bantjes, J.; Baran, A.; et al. Suicide trends in the early months of the COVID-19 pandemic: An interrupted time-series analysis of preliminary data from 21 countries. Lancet Psychiatry 2021, 8, 579–588. [Google Scholar] [CrossRef]
- Tušl, M.; Brauchli, R.; Kerksieck, P.; Bauer, G.F. Impact of the COVID-19 crisis on work and private life, mental well-being and self-rated health in German and Swiss employees: A cross-sectional online survey. BMC Public Health 2021, 21, 741. [Google Scholar] [CrossRef] [PubMed]
- Women’s Mental Health Alliance. Policy Brief: Women’s Mental Health in the Context of COVID 19 and Recommendations for Action; Women’s Health Victoria: Melbourne, Australia, 2020. [Google Scholar]
- Roesch, E.; Amin, A.; Gupta, J.; García-Moreno, C. Violence against women during covid-19 pandemic restrictions. BMJ 2020, 369, m1712. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.; Singh, T. Gender-based violence during COVID-19 pandemic: A mini-review. Front. Glob. Womens Health 2020, 1. [Google Scholar] [CrossRef]
- Government Inquiry into Mental Health and Addiction. He Ara Oranga: Report of the Government Inquiry into Mental Health and Addiction; Government Inquiry into Mental Health and Addiction: Wellington, New Zealand, 2018.
- StatsNZ. Wellbeing Statistics: 2018. Available online: https://www.stats.govt.nz/information-releases/wellbeing-statistics-2018 (accessed on 11 July 2021).
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- González-Monroy, C.; Gómez-Gómez, I.; Olarte-Sánchez, C.M.; Motrico, E. Eating Behaviour Changes during the COVID-19 Pandemic: A Systematic Review of Longitudinal Studies. Int. J. Environ. Res. Public Health 2021, 18, 11130. [Google Scholar] [CrossRef] [PubMed]
- Arora, T.; Grey, I. Health behaviour changes during COVID-19 and the potential consequences: A mini-review. J. Health Psychol. 2020, 25, 1155–1163. [Google Scholar] [CrossRef]
- Roberts, A.; Rogers, J.; Mason, R.; Siriwardena, A.N.; Hogue, T.; Whitley, G.A.; Law, G.R. Alcohol and other substance use during the COVID-19 pandemic: A systematic review. Drug Alcohol Depend. 2021, 229, 109150. [Google Scholar] [CrossRef]
- Puyat, J.; Ahmad, H.; Avina-Galindo, A.M.; Kazanjian, A.; Gupta, A.; Ellis, U.; Vila-Rodriguez, F.; Halli, P.; Salmon, A.; Vigo, D.; et al. Home-based activities that can support and promote mental wellness and resiliency during the COVID-19 Pandemic: A rapid review; Canadian Institutes of Health Research: Ottawa, ON, Canada, 2020. [Google Scholar]
- Behan, C. The benefits of meditation and mindfulness practices during times of crisis such as COVID-19. Ir. J. Psychol. Med. 2020, 37, 256–258. [Google Scholar] [CrossRef]
- Pouso, S.; Borja, Á.; Fleming, L.E.; Gómez-Baggethun, E.; White, M.P.; Uyarra, M.C. Contact with blue-green spaces during the COVID-19 pandemic lockdown beneficial for mental health. Sci. Total Environ. 2021, 756, 143984. [Google Scholar] [CrossRef]
- Oakman, J.; Kinsman, N.; Stuckey, R.; Graham, M.; Weale, V. A rapid review of mental and physical health effects of working at home: How do we optimise health? BMC Public Health 2020, 20, 1825. [Google Scholar] [CrossRef] [PubMed]
- Boulton, A.; Allport, T.; Kaiwai, H.; Harker, R.; Potaka Osborne, G. Māori perceptions of ‘home’: Māori housing needs, wellbeing and policy. Kōtuitui N. Z. J. Soc. Sci. Online 2022, 17, 44–55. [Google Scholar] [CrossRef]
- Te One, A.; Clifford, C. Tino Rangatiratanga and well-being: Māori self determination in the face of Covid-19. Front. Sociol. 2021, 6. [Google Scholar] [CrossRef] [PubMed]
- BBC News. Zoom Sees More Growth after ‘Unprecedented’ 2020. Available online: https://www.bbc.com/news/business-56247489 (accessed on 17 December 2021).
- Greer, B.; Robotham, D.; Simblett, S.; Curtis, H.; Griffiths, H.; Wykes, T. Digital Exclusion Among Mental Health Service Users: Qualitative Investigation. J. Med. Internet Res. 2019, 21, e11696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seifert, A.; Cotten, S.R.; Xie, B. A Double Burden of Exclusion? Digital and Social Exclusion of Older Adults in Times of COVID-19. J. Gerontol. B Psychol. Sci. Soc. Sci. 2021, 76, e99–e103. [Google Scholar] [CrossRef] [PubMed]
- Imlach, F.; McKinlay, E.; Kennedy, J.; Pledger, M.; Middleton, L.; Cumming, J.; McBride-Henry, K. Seeking healthcare during lockdown: Challenges, opportunities and lessons for the future. Int. J. Health Policy Manag. 2021. [Google Scholar] [CrossRef]
- Chan, H.Y. Mental wellbeing in a pandemic: The role of solidarity and care. Public Health Ethics 2021, 14, 47–58. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Imlach, F.; McKinlay, E.; Middleton, L.; Kennedy, J.; Pledger, M.; Russell, L.; Churchward, M.; Cumming, J.; McBride-Henry, K. Telehealth consultations in general practice during a pandemic lockdown: Survey and interviews on patient experiences and preferences. BMC Fam. Pract. 2020, 21, 269. [Google Scholar] [CrossRef]
- Lee, C.H.J.; Sibley, C.G. Attitudes toward vaccinations are becoming more polarized in New Zealand: Findings from a longitudinal survey. EClinicalMedicine 2020, 23, 100387. [Google Scholar] [CrossRef]
- Latif, J. ‘Everything Seems Like an Emergency’—Homeless Auckland Teens Struggle in Lockdown. Available online: https://www.rnz.co.nz/news/ldr/453183/everything-seems-like-an-emergency-homeless-auckland-teens-struggle-in-lockdown (accessed on 5 November 2021).


{kind=link}
| Focus Area | Desired Outcome |
|---|---|
| Social and economic foundations for psychosocial and mental wellbeing | Whānau and communities have the resources and supportive environments on which psychosocial and mental wellbeing is built. |
| Community-led solutions | Whānau and communities are empowered and supported to respond to mental distress and lead recovery solutions. |
| Whānau and individuals look after their mental wellbeing | People know how to look after their mental wellbeing and know where to get help if they need it. |
| Primary mental health and addiction support | Whānau and communities have free and easy access to mental wellbeing support services in their communities. |
| Specialist services | People with severe mental distress and addictions and their whānau get high quality timely mental health and addiction support. |
| Age Range (Years) | Interviewees (n (%)) |
|---|---|
| 18–34 | 7 (18) |
| 35–44 | 6 (16) |
| 45–54 | 12 (32) |
| 55–64 | 3 (8) |
| 65+ | 10 (26) |
| Gender * | |
| Female | 24 (63) |
| Male | 14 (37) |
| Prioritised ethnicity | |
| Māori | 6 (16) |
| Pacific peoples | 3 (8) |
| Asian | 4 (11) |
| New Zealand European/Other | 25 (66) |
| Current work status | |
| In paid employment without change caused by COVID-19 | 22 (58) |
| In paid employment with reduced pay due to COVID-19 | 3 (8) |
| Not in paid employment and not looking for a job | 13 (34) |
| Grouped District Health Board (DHB) region # | |
| Northern region | 7 (18) |
| Midland region | 3 (8) |
| Central region | 20 (53) |
| South Island | 8 (21) |
| Focus Area | Subthemes | ||
|---|---|---|---|
| Community-led solutions | Household relationships and responsibilities | Telecommunications | Community and neighbourly relationships |
| Whānau (family) and individuals look after their mental wellbeing | Physical lifestyle and behaviour changes | Pace of life and mindset | Stuck or safe at home |
| Primary and specialist mental health and wellbeing support | Accessibility | The form of service delivery | Clinician-patient relationships |
| Social and economic foundations | |||
| Recommendation | Who? | Description |
|---|---|---|
| Opportunities for person-centred care | Health professionals, funders |
|
| Support for working from home options | Employers |
|
| Promote positive coping strategies and messaging | Central and local government, health professionals |
|
| Reduce digital exclusion | Central government, tertiary education providers, health professional representative organisations |
|
| Integrated whole of society response to COVID-19 | Workplaces, government and social services |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Officer, T.N.; Imlach, F.; McKinlay, E.; Kennedy, J.; Pledger, M.; Russell, L.; Churchward, M.; Cumming, J.; McBride-Henry, K. COVID-19 Pandemic Lockdown and Wellbeing: Experiences from Aotearoa New Zealand in 2020. Int. J. Environ. Res. Public Health 2022, 19, 2269. https://doi.org/10.3390/ijerph19042269
Officer TN, Imlach F, McKinlay E, Kennedy J, Pledger M, Russell L, Churchward M, Cumming J, McBride-Henry K. COVID-19 Pandemic Lockdown and Wellbeing: Experiences from Aotearoa New Zealand in 2020. International Journal of Environmental Research and Public Health. 2022; 19(4):2269. https://doi.org/10.3390/ijerph19042269
Chicago/Turabian StyleOfficer, Tara N., Fiona Imlach, Eileen McKinlay, Jonathan Kennedy, Megan Pledger, Lynne Russell, Marianna Churchward, Jacqueline Cumming, and Karen McBride-Henry. 2022. "COVID-19 Pandemic Lockdown and Wellbeing: Experiences from Aotearoa New Zealand in 2020" International Journal of Environmental Research and Public Health 19, no. 4: 2269. https://doi.org/10.3390/ijerph19042269
APA StyleOfficer, T. N., Imlach, F., McKinlay, E., Kennedy, J., Pledger, M., Russell, L., Churchward, M., Cumming, J., & McBride-Henry, K. (2022). COVID-19 Pandemic Lockdown and Wellbeing: Experiences from Aotearoa New Zealand in 2020. International Journal of Environmental Research and Public Health, 19(4), 2269. https://doi.org/10.3390/ijerph19042269