
Capacitive-Type Pressure-Mapping Sensor for Measuring Bite Force

 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Usage of Sensor Sheets
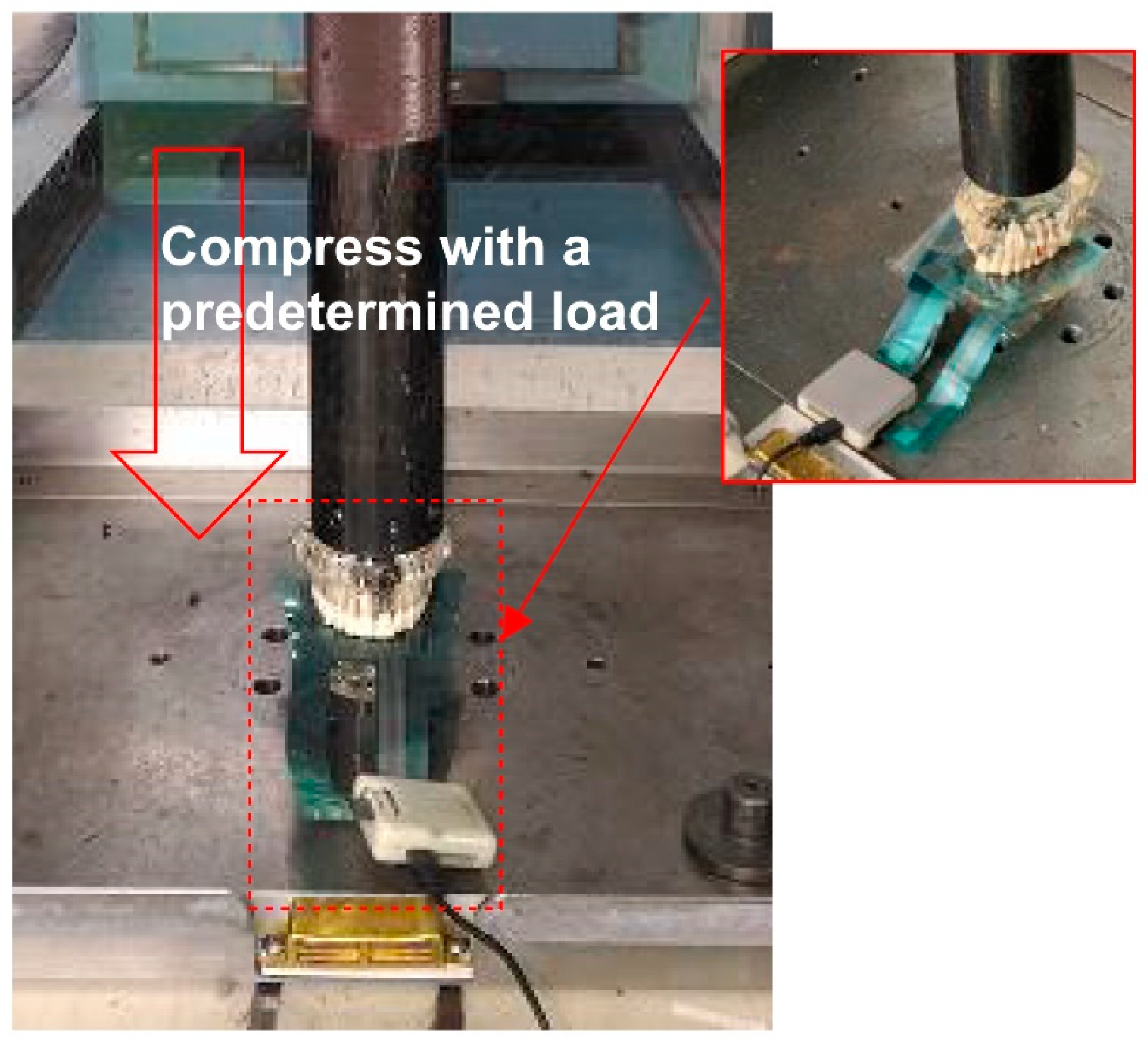
2.2. Comparison of Output Value against Compressive Load
3. Results
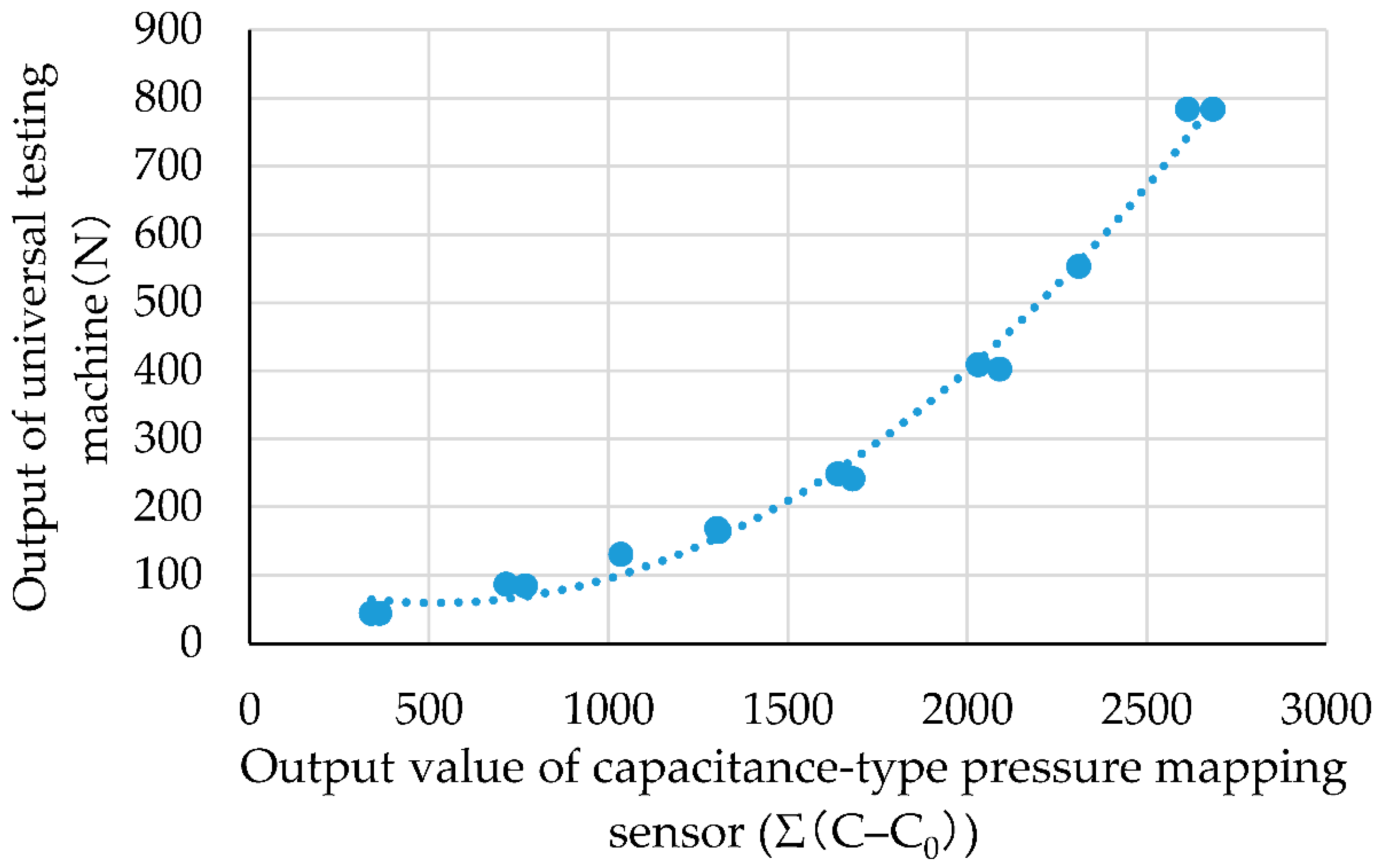
3.1. Comparison of Output Characteristics of Capacitive-Type Pressure-Mapping Sensor and Universal Testing Machine against Compressive Load
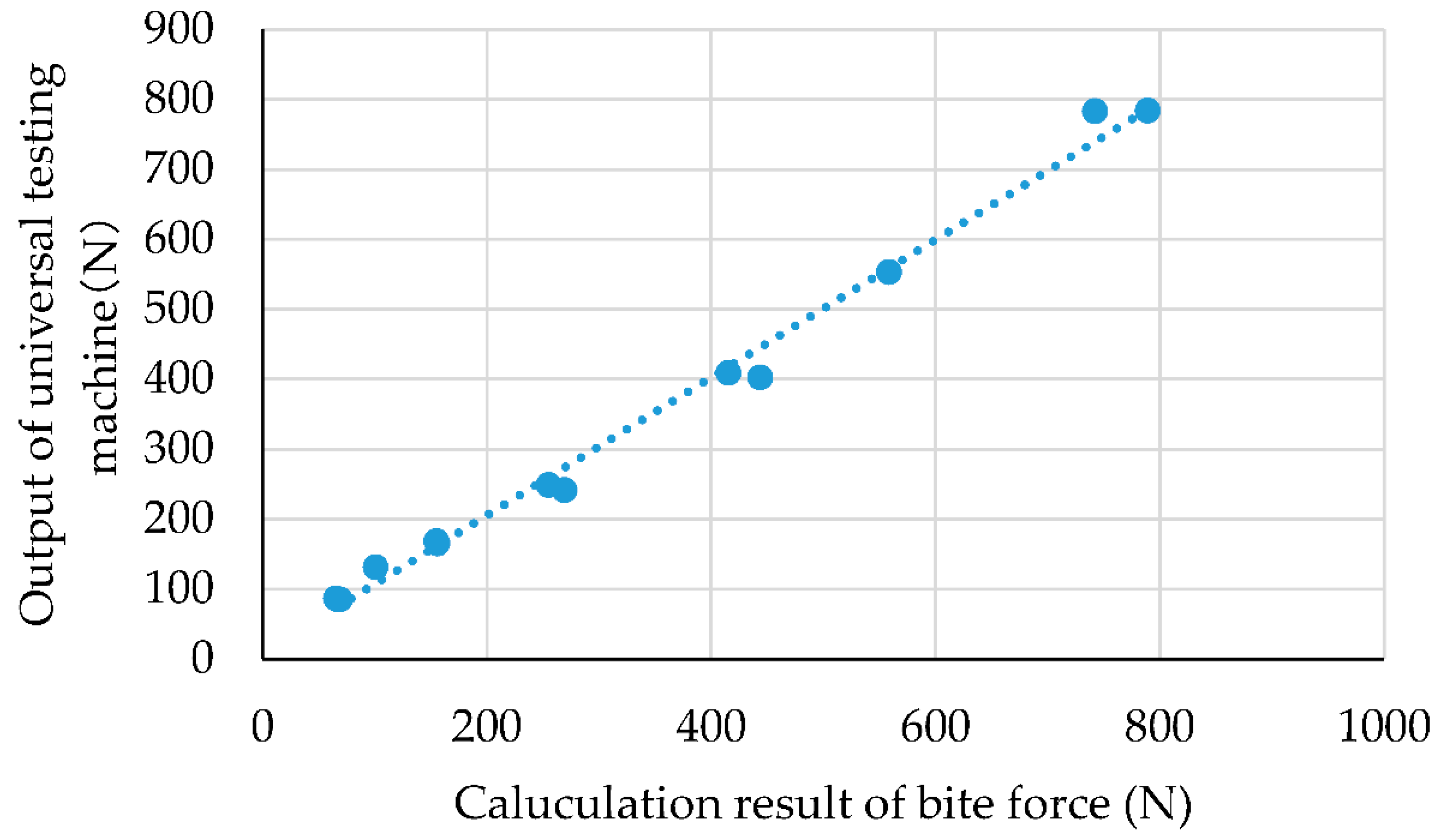
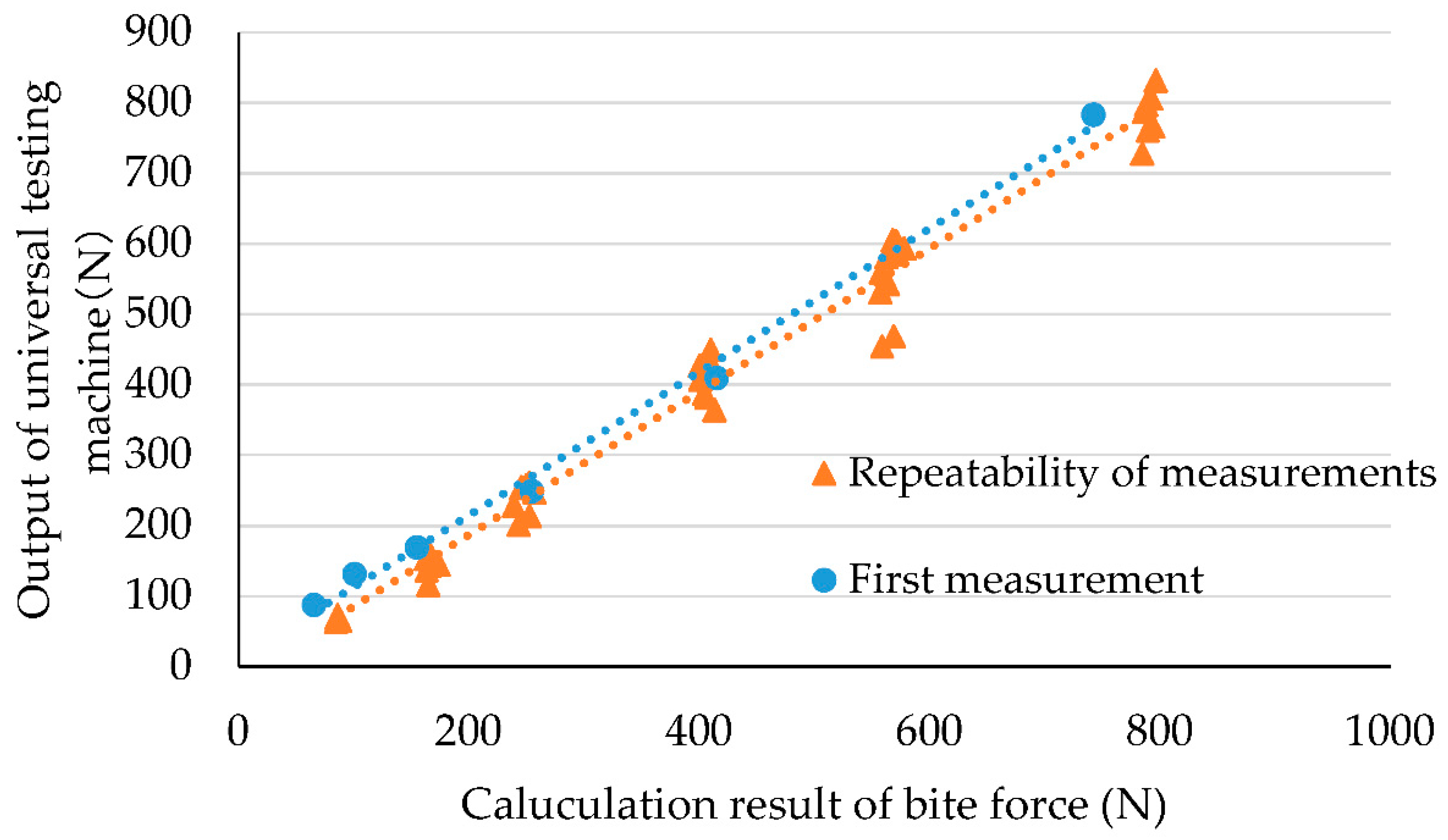
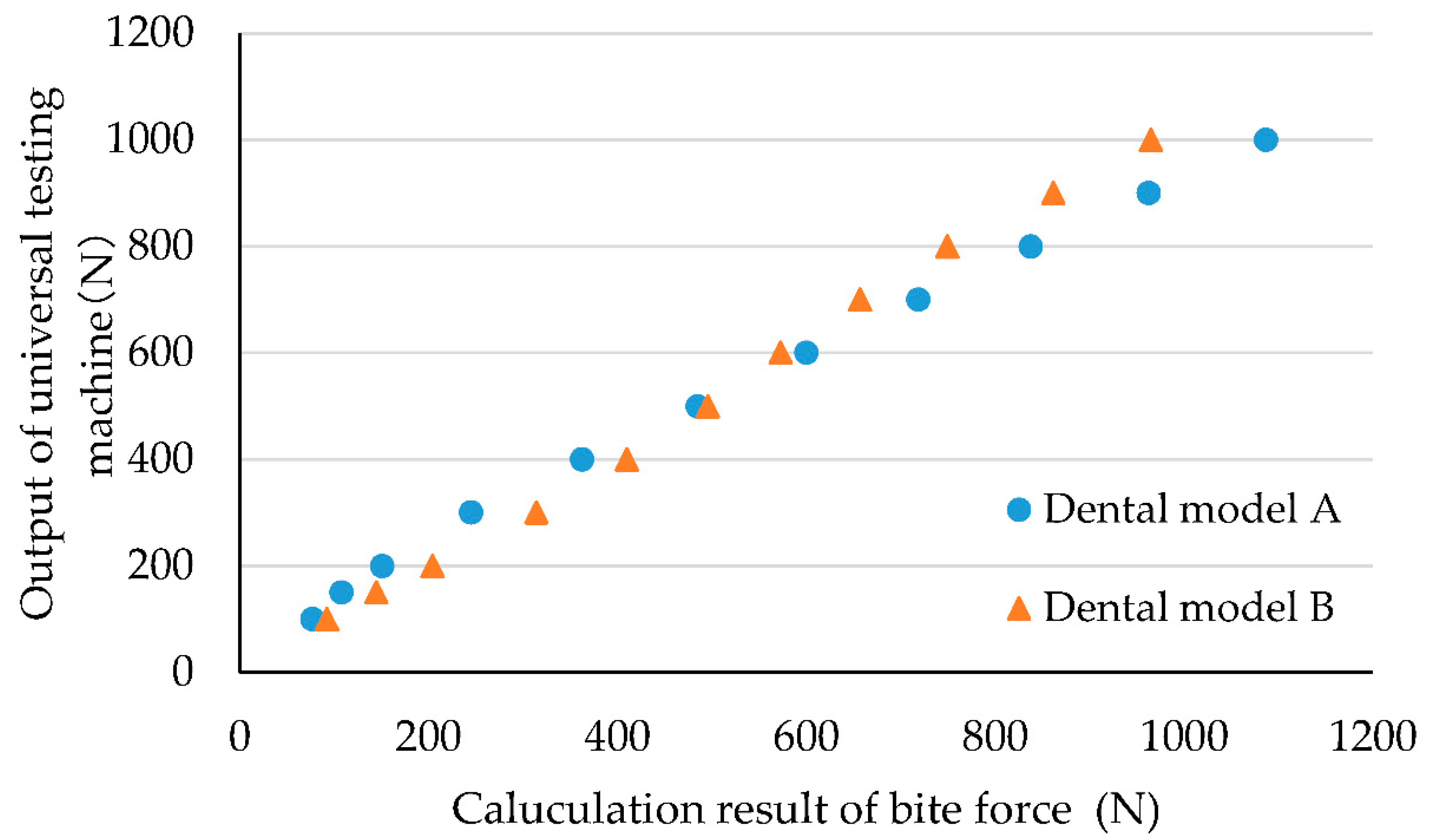
3.2. Characteristics of Bite Force Recorded by Capacitive-Type Pressure-Mapping Sensor
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kosaka, T.; Ono, T.; Kida, M.; Kikui, M.; Yamamoto, M.; Yasui, S.; Nokubi, T.; Maeda, Y.; Kokubo, Y.; Watanabe, M.; et al. A multifactorial model of masticatory performance: The Suita study. J. Oral Rehabil. 2015, 43, 340–347. [Google Scholar] [CrossRef] [PubMed]
- Hatch, J.; Shinkai, R.; Sakai, S.; Rugh, J.; Paunovich, E. Determinants of masticatory performance in dentate adults. Arch. Oral Biol. 2001, 46, 641–648. [Google Scholar] [CrossRef]
- Ikebe, K.; Matsuda, K.-I.; Kagawa, R.; Enoki, K.; Okada, T.; Yoshida, M.; Maeda, Y. Masticatory performance in older subjects with varying degrees of tooth loss. J. Dent. 2012, 40, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Ikebe, K.; Gondo, Y.; Kamide, K.; Masui, Y.; Ishizaki, T.; Arai, Y.; Inagaki, H.; Nakagawa, T.; Kabayama, M.; Ryuno, H.; et al. Occlusal force is correlated with cognitive function directly as well as indirectly via food intake in community-dwelling older Japanese: From the SONIC study. PLoS ONE 2018, 13, e0190741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inomata, C.; Ikebe, K.; Kagawa, R.; Okubo, H.; Sasaki, S.; Okada, T.; Takeshita, H.; Tada, S.; Matsuda, K.-I.; Kurushima, Y.; et al. Significance of occlusal force for dietary fibre and vitamin intakes in independently living 70-year-old Japanese: From SONIC Study. J. Dent. 2014, 42, 556–564. [Google Scholar] [CrossRef] [PubMed]
- Ohi, T.; Komiyama, T.; Miyoshi, Y.; Murakami, T.; Tsuboi, A.; Tomata, Y.; Tsuji, I.; Watanabe, M.; Hattori, Y. Maximum Occlusal Force and Incident Functional Disability in Older Adults: The Tsurugaya Project. JDR Clin. Transl. Res. 2018, 3, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Okada, T.; Ikebe, K.; Kagawa, R.; Inomata, C.; Takeshita, H.; Gondo, Y.; Ishioka, Y.; Okubo, H.; Kamide, K.; Masui, Y.; et al. Lower Protein Intake Mediates Association Between Lower Occlusal Force and Slower Walking Speed: From the Septuagenarians, Octogenarians, Nonagenarians Investigation with Centenarians Study. J. Am. Geriatr. Soc. 2015, 63, 2382–2387. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, S.; Kosaka, T.; Nakai, M.; Kida, M.; Fushida, S.; Kokubo, Y.; Watanabe, M.; Higashiyama, A.; Ikebe, K.; Ono, T.; et al. A lower maximum bite force is a risk factor for developing cardiovascular disease: The Suita study. Sci. Rep. 2021, 11, 7671. [Google Scholar] [CrossRef] [PubMed]
- Minakuchi, S.; Tsuga, K.; Ikebe, K.; Ueda, T.; Tamura, F.; Nagao, K.; Furuya, J.; Matsuo, K.; Yamamoto, K.; Kanazawa, M.; et al. Oral hypofunction in the older population: Position paper of the Japanese Society of Gerodontology in 2016. Gerodontology 2018, 35, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Lyons, M.F.; Sharkey, S.W.; Lamey, P.J. An evaluation of the T-Scan computerised occlusal analysis system. Int. J. Prosthodont. 1992, 5, 166–172. [Google Scholar] [PubMed]
- Martins, M.J.D.S.; Caramelo, F.J.; Da Fonseca, J.A.R.; Nicolau, P.M.G. In vitro study on the sensibility and reproducibility of the new T-Scan®III HD system. Rev. Port. Estomatol. Med. Dentária E Cir. Maxilofac. 2014, 55, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Verma, T.P.; Kumathalli, K.I.; Jain, V.; Kumar, R. Bite Force Recording Devices-A Review. J. Clin. Diagn. Res. 2017, 11, Ze01–Ze05. [Google Scholar] [CrossRef]
- T-Scan. Available online: http://www.tekscan.cz/sale_en.html (accessed on 17 November 2021).
- Ando, K.; Kurosawa, M.; Fuwa, Y.; Kondo, T.; Goto, S. A study on measuring occlusal contact area using silicone impression materials: An application of this method to the bite force measurement system using the pressure-sensitive sheet. Dent. Mater. J. 2007, 26, 898–905. [Google Scholar] [CrossRef] [Green Version]
- Dental Prescale (In Japanese). Available online: http://www.fordy.jp/products/detail2.php?sid=1971&call=2&no=123 (accessed on 17 November 2021).
- Pereira, L.J.; Pastore, M.G.; Bonjardim, L.R.; Castelo, P.M.; Gavião, M.B.D. Molar bite force and its correlation with signs of temporomandibular dysfunction in mixed and permanent dentition. J. Oral Rehabil. 2007, 34, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Serra, M.D.; Gambareli, F.R.; Gavião, M.B.D. A 1-year intraindividual evaluation of maximum bite force in children wearing a removable partial dental prosthesis. J. Dent. Child. 2008, 74, 171–176. [Google Scholar]
- Fastier-Wooller, J.; Phan, H.-P.; Dinh, T.; Nguyen, T.-K.; Cameron, A.; Oechsner, A.; Dao, D.V. Novel Low-Cost Sensor for Human Bite Force Measurement. Sensors 2016, 16, 1244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harada, K.; Watanabe, M.; Ohkura, K.; Enomoto, S. Measure of bite force and occlusal contact area before and after bilateral sagittal split ramus osteotomy of the mandible using a new pressure-sensitive device: A preliminary report. J. Oral Maxillofac. Surg. 2000, 58, 370–373. [Google Scholar] [CrossRef]
- Umesh, S.; Padma, S.; Asokan, S.; Srinivas, T. Fiber Bragg Grating based bite force measurement. J. Biomech. 2016, 49, 2877–2881. [Google Scholar] [CrossRef] [PubMed]
- Serra, C.M.; Manns, A.E. Bite force measurements with hard and soft bite surfaces. J. Oral Rehabilitation 2013, 40, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Shimadzu Cooperation. Shimadzu Universal Testers. Available online: https://www.quark-gulf.com/quark/public/storage/Products/gynGTetHuFjf0qnYm1f2BDZekbESroVJdtgRWX8n.pdf (accessed on 17 November 2021).
- Agilent Technologies. Agilent Impedance Measurement Handbook. Available online: https://indico.cern.ch/event/216963/sessions/35851/attachments/347577/484629/impedancemeasurementhandbook_2.pdf (accessed on 14 January 2022).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwasaki, M.; Maeda, I.; Kokubo, Y.; Tanaka, Y.; Ueno, T.; Takahashi, W.; Watanabe, Y.; Hirano, H. Capacitive-Type Pressure-Mapping Sensor for Measuring Bite Force. Int. J. Environ. Res. Public Health 2022, 19, 1273. https://doi.org/10.3390/ijerph19031273
Iwasaki M, Maeda I, Kokubo Y, Tanaka Y, Ueno T, Takahashi W, Watanabe Y, Hirano H. Capacitive-Type Pressure-Mapping Sensor for Measuring Bite Force. International Journal of Environmental Research and Public Health. 2022; 19(3):1273. https://doi.org/10.3390/ijerph19031273
Chicago/Turabian StyleIwasaki, Masanori, Ichinosuke Maeda, Yota Kokubo, Yoshitomo Tanaka, Tetsuji Ueno, Wataru Takahashi, Yutaka Watanabe, and Hirohiko Hirano. 2022. "Capacitive-Type Pressure-Mapping Sensor for Measuring Bite Force" International Journal of Environmental Research and Public Health 19, no. 3: 1273. https://doi.org/10.3390/ijerph19031273
APA StyleIwasaki, M., Maeda, I., Kokubo, Y., Tanaka, Y., Ueno, T., Takahashi, W., Watanabe, Y., & Hirano, H. (2022). Capacitive-Type Pressure-Mapping Sensor for Measuring Bite Force. International Journal of Environmental Research and Public Health, 19(3), 1273. https://doi.org/10.3390/ijerph19031273