
An Experimental Study Evaluating the Influence of Front-of-Package Warning Labels on Adolescent’s Purchase Intention of Processed Food Products


Abstract
:1. Introduction
2. Materials and Methods
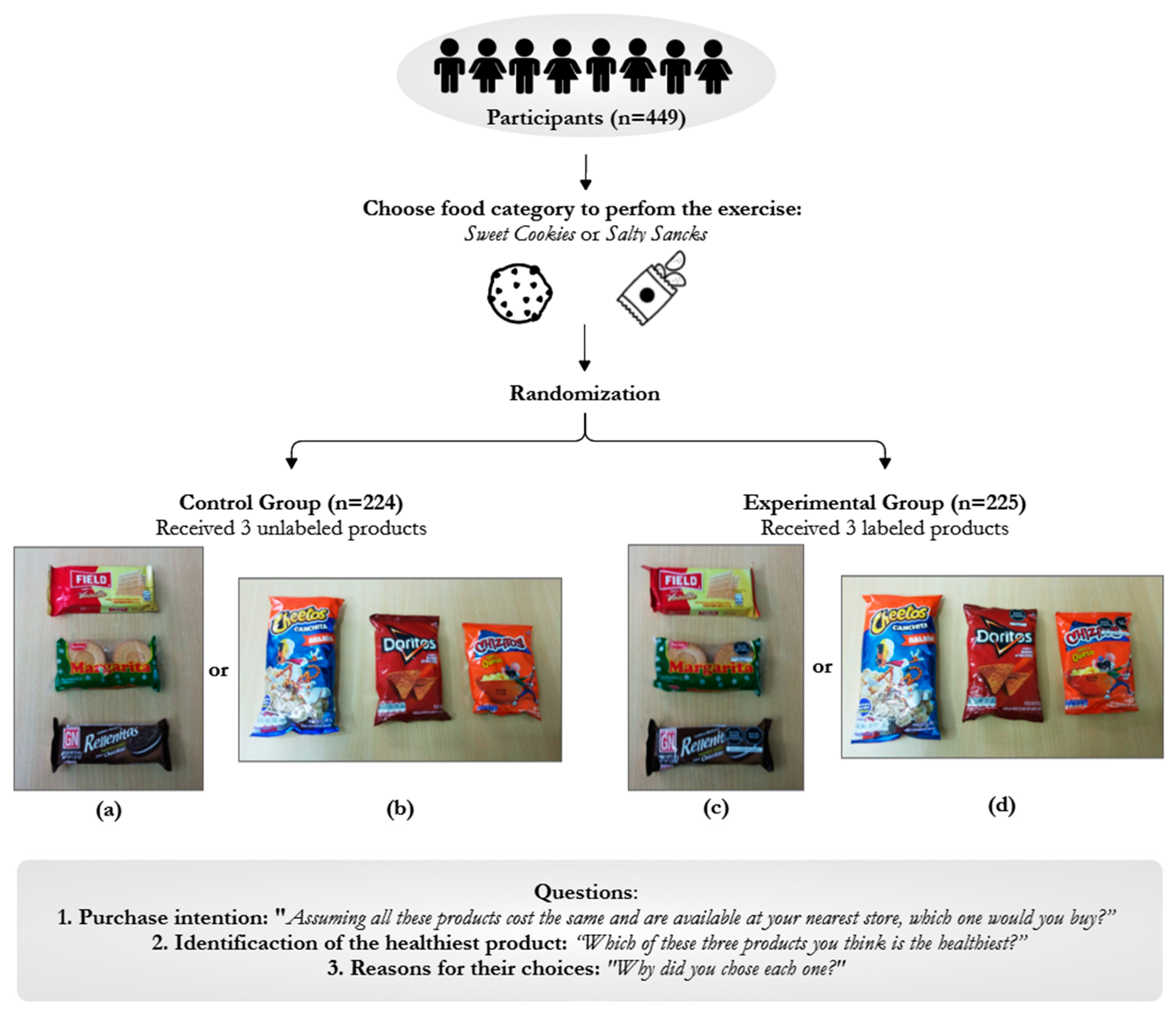
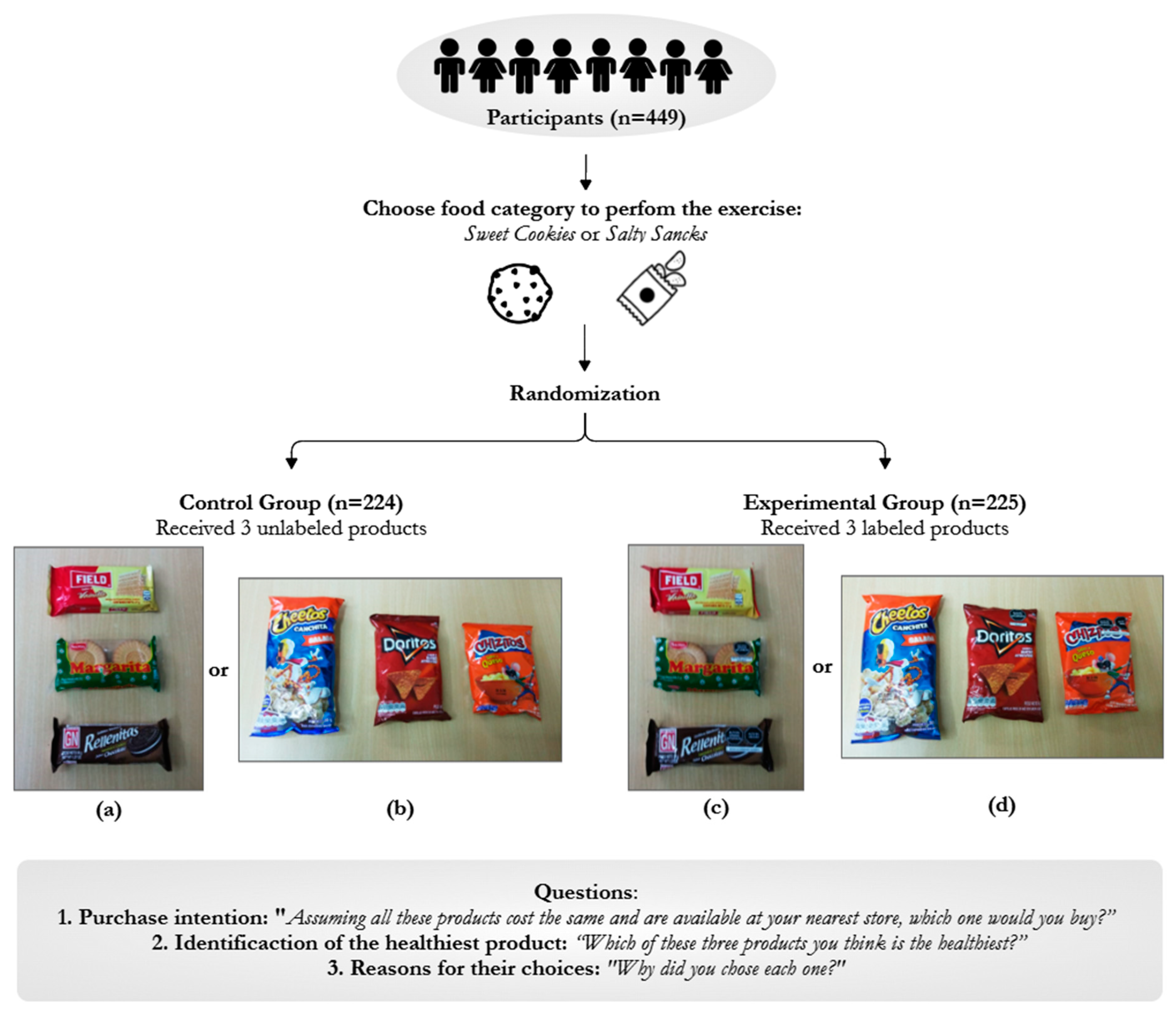
2.1. Design and Setting
2.2. Participants
2.3. Intervention
2.4. Product Selection
2.5. Outcomes and Analysis
3. Results
4. Discussion
4.1. Strenghts and Limitations
4.2. Public Health Implications
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cominato, L.; Di Biagio, G.F.; Lellis, D.; Franco, R.R.; Mancini, M.C.; de Melo, M.E. Obesity Prevention: Strategies and Challenges in Latin America. Curr. Obes. Rep. 2018, 7, 97–104. [Google Scholar] [CrossRef]
- Hieke, S.; Taylor, C.R. A Critical Review of the Literature on Nutritional Labeling. J. Consum. Aff. 2012, 46, 120–156. [Google Scholar] [CrossRef]
- Temple, N.J. Front-of-package food labels: A narrative review. Appetite 2020, 144, 104485. [Google Scholar] [CrossRef]
- Van Loo, E.J.; Grebitus, C.; Nayga, R.M.; Verbeke, W.; Roosen, J. On the Measurement of Consumer Preferences and Food Choice Behavior: The Relation Between Visual Attention and Choices. Appl. Econ. Perspect. Policy 2018, 40, 538–562. [Google Scholar] [CrossRef]
- Taillie, L.S.; Hall, M.G.; Popkin, B.M.; Ng, S.W.; Murukutla, N. Experimental Studies of Front-of-Package Nutrient Warning Labels on Sugar-Sweetened Beverages and Ultra-Processed Foods: A Scoping Review. Nutrients 2020, 12, 569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministerio de Salud Pública del Ecuador. Reglamento Sanitario Sustitutivo de Etiquetado de Alimentos Procesados Para el Consumo Humano 5103; Registro Oficial No. 318 (Segundo Suplemento); Ministerio de Salud Pública del Ecuador: Quito, Ecuador, 2014; Available online: https://www.controlsanitario.gob.ec/wp-content/uploads/downloads/2016/12/Reglamento-de-Etiquetado-de-Alimentos-procesados-para-consumo-humano.pdf (accessed on 7 November 2021).
- Ministerio de Salud de Chil. Ley 20.606 Sobre Composición Nutricional de los Alimentos y su Publicidad; Ministerio de Salud de Chile: Santiago, Chile, 2012; Available online: https://www.bcn.cl/leychile/navegar?idNorma=1041570&idVersion=2021-08-18&idParte= (accessed on 7 November 2021).
- Presidencia de la República del Perú. Manual de Advertencias Publicitarias en el Marco de lo Establecido en la Ley Nº 30021, Ley de Promoción de la Alimentación Saludable para Niños, Niñas y Adolescentes, y su Reglamento Aprobado por Decreto Supremo Nº 017-2017-SA; Decreto Supremo N° 012-2018-SA; Presidencia de la República del Perú: Lima, Perú, 2018; Available online: https://busquedas.elperuano.pe/download/url/aprueban-manual-de-advertencias-publicitarias-en-el-marco-de-decreto-supremo-n-012-2018-sa-1660606-1 (accessed on 7 November 2021).
- Cámara de Senadores de la República Oriental del Uruguay; Cámara de Representantes de la República de Uruguay. Ley N° 19.140 Alimentación Saludable en los Centros de Enseñanza; Ministerio de Educación y Cultura, Ministerio de Salud Pública: Montevideo, Uruguay, 2013; Available online: https://docs.bvsalud.org/leisref/2018/03/350/dieta-ley-no-19140.pdf (accessed on 7 November 2021).
- Congreso de la República del Perú. Ley de Promoción de la Alimentación Saludable Para Niños, Niñas y Adolescentes; Congreso de la República del Perú: Lima, Perú, 2013; Available online: http://www.codajic.org/sites/default/files/sites/www.codajic.org/files/Ley-de-Promocion-de-la-Alimentacion-Saludable-para-Ninos-Ninas-y-Adolescentes.pdf (accessed on 7 November 2021).
- Correa, T.; Fierro, C.; Reyes, M.; Dillman Carpentier, F.R.; Taillie, L.S.; Corvalan, C. Responses to the Chilean law of food labeling and advertising: Exploring knowledge, perceptions and behaviors of mothers of young children. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 21. [Google Scholar] [CrossRef]
- Taillie, L.S.; Reyes, M.; Colchero, M.A.; Popkin, B.; Corvalán, C. An evaluation of Chile’s Law of Food Labeling and Advertising on sugar-sweetened beverage purchases from 2015 to 2017: A before-and-after study. PLoS Med. 2020, 17, e1003015. [Google Scholar] [CrossRef]
- Cabrera, M.; Machín, L.; Arrúa, A.; Antúnez, L.; Curutchet, M.R.; Giménez, A.; Ares, G. Nutrition warnings as front-of-pack labels: Influence of design features on healthfulness perception and attentional capture. Public Health Nutr. 2017, 20, 3360–3371. [Google Scholar] [CrossRef] [Green Version]
- Lima, M.; Ares, G.; Deliza, R. How do front of pack nutrition labels affect healthfulness perception of foods targeted at children? Insights from Brazilian children and parents. Food Qual. Prefer. 2018, 64, 111–119. [Google Scholar] [CrossRef]
- Arrúa, A.; Curutchet, M.R.; Rey, N.; Barreto, P.; Golovchenko, N.; Sellanes, A.; Velazco, G.; Winokur, M.; Giménez, A.; Ares, G. Impact of front-of-pack nutrition information and label design on children’s choice of two snack foods: Comparison of warnings and the traffic-light system. Appetite 2017, 116, 139–146. [Google Scholar] [CrossRef]
- Freire, W.B.; Waters, W.F.; Rivas-Mariño, G.; Nguyen, T.; Rivas, P. A qualitative study of consumer perceptions and use of traffic light food labelling in Ecuador. Public Health Nutr. 2017, 20, 805–813. [Google Scholar] [CrossRef] [Green Version]
- Currie, C.; Zanotti, C.; Morgan, A.; Currie, D.; Looze, M.; Roberts, C.; Samdal, O.; Smith, O.R.F.; Barnekow, V. Social Determinants of Health and Well-Being among Young People. In Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey; WHO: Copenhagen, Denmark, 2012. [Google Scholar]
- Naderer, B.; Matthes, J.; Binder, A.; Marquart, F.; Mayrhofer, M.; Obereder, A.; Spielvogel, I. Shaping children’s healthy eating habits with food placements? Food placements of high and low nutritional value in cartoons, Children’s BMI, food-related parental mediation strategies, and food choice. Appetite 2018, 120, 644–653. [Google Scholar] [CrossRef] [PubMed]
- Dixon, H.; Scully, M.; Niven, P.; Kelly, B.; Chapman, K.; Donovan, R.; Martin, J.; Baur, L.A.; Crawford, D.; Wakefield, M. Effects of nutrient content claims, sports celebrity endorsements and premium offers on pre-adolescent children’s food preferences: Experimental research. Pediatr. Obes. 2014, 9, e47–e57. [Google Scholar] [CrossRef] [PubMed]
- Dixon, H.; Scully, M.; Wakefield, M.; Kelly, B.; Chapman, K.; Donovan, R. Parent’s responses to nutrient claims and sports celebrity endorsements on energy-dense and nutrient-poor foods: An experimental study. Public Health Nutr. 2011, 14, 1071–1079. [Google Scholar] [CrossRef] [Green Version]
- Khandpur, N.; Sato, P.D.; Mais, L.A.; Martins, A.P.; Spinillo, C.G.; Garcia, M.T.; Rojas, C.F.; Jaime, P.C. Are Front-of-Package Warning Labels More Effective at Communicating Nutrition Information than Traffic-Light Labels? A Randomized Controlled Experiment in a Brazilian Sample. Nutrients 2018, 10, 688. [Google Scholar] [CrossRef] [Green Version]
- Lima, M.; de Alcantara, M.; Martins, I.B.A.; Ares, G.; Deliza, R. Can front-of-pack nutrition labeling influence children’s emotional associations with unhealthy food products? An experiment using emoji. Food Res. Int. 2019, 120, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Egnell, M.; Talati, Z.; Gombaud, M.; Galan, P.; Hercberg, S.; Pettigrew, S.; Julia, C. Consumers’ Responses to Front-of-Pack Nutrition Labelling: Results from a Sample from The Netherlands. Nutrients 2019, 11, 1817. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Estadística e Informática. Planos Estratificados de Lima Metropolitana a Nivel de Manzanas 2020; Instituto Nacional de Estadística e Informática: Lima, Peru, 2020. [Google Scholar]
- Acton, R.B.; Hammond, D. The impact of price and nutrition labelling on sugary drink purchases: Results from an experimental marketplace study. Appetite 2018, 121, 129–137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamlin, R.; Hamlin, B. An Experimental Comparison of the Impact of ‘Warning’ and ‘Health Star Rating’ FoP Labels on Adolescents’ Choice of Breakfast Cereals in New Zealand. Nutrients 2020, 12, 1545. [Google Scholar] [CrossRef] [PubMed]
- Lima, M.; de Alcantara, M.; Ares, G.; Deliza, R. It is not all about information! Sensory experience overrides the impact of nutrition information on consumers’ choice of sugar-reduced drinks. Food Qual. Prefer. 2019, 74, 1–9. [Google Scholar] [CrossRef]
- Ares, G.; Varela, F.; Machin, L.; Antúnez, L.; Giménez, A.; Curutchet, M.R.; Aschemann-Witzel, J. Comparative performance of three interpretative front-of-pack nutrition labelling schemes: Insights for policy making. Food Qual. Prefer. 2018, 68, 215–225. [Google Scholar] [CrossRef]
- Balasubramanian, S.K.; Cole, C. Consumers’ Search and Use of Nutrition Information: The Challenge and Promise of the Nutrition Labeling and Education Act. J. Mark. 2002, 66, 112–127. [Google Scholar] [CrossRef] [Green Version]
- Ares, G.; Vidal, L.; Otterbring, T.; Aschemann-Witzel, J.; Curutchet, M.R.; Gimenez, A.; Bove, I. Communication Campaigns to Support the Use of Nutritional Warnings: Different Messages for Different People? Health Educ. Behav. 2021, 48, 584–594. [Google Scholar] [CrossRef] [PubMed]
- Saavedra-Garcia, L.; Meza-Hernandez, M.; Yabiku-Soto, K.; Hernandez-Vasquez, A.; Kesar, H.V.; Mejia-Victorio, C.; Diez-Canseco, F. Food and beverage supply and advertising in schools and their surroundings in Metropolitan Lima. An exploratory study. Rev. Peru. Med. Exp. Salud Pública 2020, 37, 726–732. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Characteristics | Control * (n = 224) | Experimental (n = 225) | p | |
|---|---|---|---|---|
| n (%) | n (%) | |||
| Gender (Female) | 135 (60.3) | 129 (57.3) | 0.528 | |
| Age (Years) | 10 | 43 (19.2) | 35 (15.6) | 0.342 |
| 11 | 40 (17.9) | 52 (23.1) | ||
| 12 | 69 (30.8) | 71 (31.6) | ||
| 13 | 48 (21.4) | 37 (16.4) | ||
| 14 | 24 (10.7) | 30 (13.3) | ||
| Educational level | Primary | 86 (38.4) | 87 (38.7) | 0.952 |
| Secondary | 138 (61.6) | 138 (61.3) | ||
| Buys food on his/her own | 196 (87.5) | 198 (88.0) | 0.872 | |
| Checks package information when buying food | 144 (73.5) | 149 (75.3) | 0.685 | |
| Chosen food category for experiment | Cookies | 142 (63.4) | 151 (67.1) | 0.408 |
| Snacks | 82 (36.6) | 74 (32.9) | ||
| Intention to Purchase | Identification of Healthiest Food | |||||
|---|---|---|---|---|---|---|
| Control * | Experimental | p | Control * | Experimental | p | |
| n (%) | n (%) | n (%) | n (%) | |||
| Cookies | 0.196 | 0.855 | ||||
| Vanilla cookies (0 WL) | 67 (47.2) | 65 (43.1) | 115 (81.0) | 126 (83.4) | ||
| Plain cookies (1 WL) | 41 (28.9) | 58 (38.4) | 24 (16.9) | 22 (14.6) | ||
| Chocolate-filled cookies (2 WL) | 34 (23.9) | 28 (18.5) | 3 (2.1) | 3 (2.0) | ||
| Savory Snacks | 0.950 | 0.113 | ||||
| Popcorn (0 WL) | 38 (46.4) | 36 (48.7) | 73 (89.0) | 62 (83.8) | ||
| Fried tortillas (1 WL) | 33 (40.2) | 29 (39.2) | 5 (6.1) | 2 (2.7) | ||
| Puffed corn snacks (2 WL) | 11 (13.4) | 9 (12.1) | 4 (4.9) | 10 (13.5) | ||
| All | 0.386 | 0.322 | ||||
| Vanilla cookies and popcorn (0 WL) | 105 (46.9) | 101 (44.9) | 188 (83.9) | 188 (83.5) | ||
| Plain cookies and fried tortillas (1 WL) | 74 (33.0) | 87 (38.7) | 29 (13.0) | 24 (10.7) | ||
| Chocolate filled cookies and puffed corn snack (2 WL) | 45 (20.1) | 37 (16.4) | 7 (3.1) | 13 (5.8) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saavedra-Garcia, L.; Moscoso-Porras, M.; Diez-Canseco, F. An Experimental Study Evaluating the Influence of Front-of-Package Warning Labels on Adolescent’s Purchase Intention of Processed Food Products. Int. J. Environ. Res. Public Health 2022, 19, 1094. https://doi.org/10.3390/ijerph19031094
Saavedra-Garcia L, Moscoso-Porras M, Diez-Canseco F. An Experimental Study Evaluating the Influence of Front-of-Package Warning Labels on Adolescent’s Purchase Intention of Processed Food Products. International Journal of Environmental Research and Public Health. 2022; 19(3):1094. https://doi.org/10.3390/ijerph19031094
Chicago/Turabian StyleSaavedra-Garcia, Lorena, Miguel Moscoso-Porras, and Francisco Diez-Canseco. 2022. "An Experimental Study Evaluating the Influence of Front-of-Package Warning Labels on Adolescent’s Purchase Intention of Processed Food Products" International Journal of Environmental Research and Public Health 19, no. 3: 1094. https://doi.org/10.3390/ijerph19031094
APA StyleSaavedra-Garcia, L., Moscoso-Porras, M., & Diez-Canseco, F. (2022). An Experimental Study Evaluating the Influence of Front-of-Package Warning Labels on Adolescent’s Purchase Intention of Processed Food Products. International Journal of Environmental Research and Public Health, 19(3), 1094. https://doi.org/10.3390/ijerph19031094