
Impact of the COVID-19 Pandemic on Melanoma Diagnosis: Increased Breslow Thickness in Primary Melanomas—A Single Center Experience

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Data Extraction
2.2. Data Analysis
3. Results
3.1. Patient Characteristics before and during the Pandemic
3.2. Body Distribution of Melanomas before and during the Pandemic
3.3. Melanoma-Specific Histologic Characteristics before and during the Pandemic
4. Discussion
4.1. Main Findings
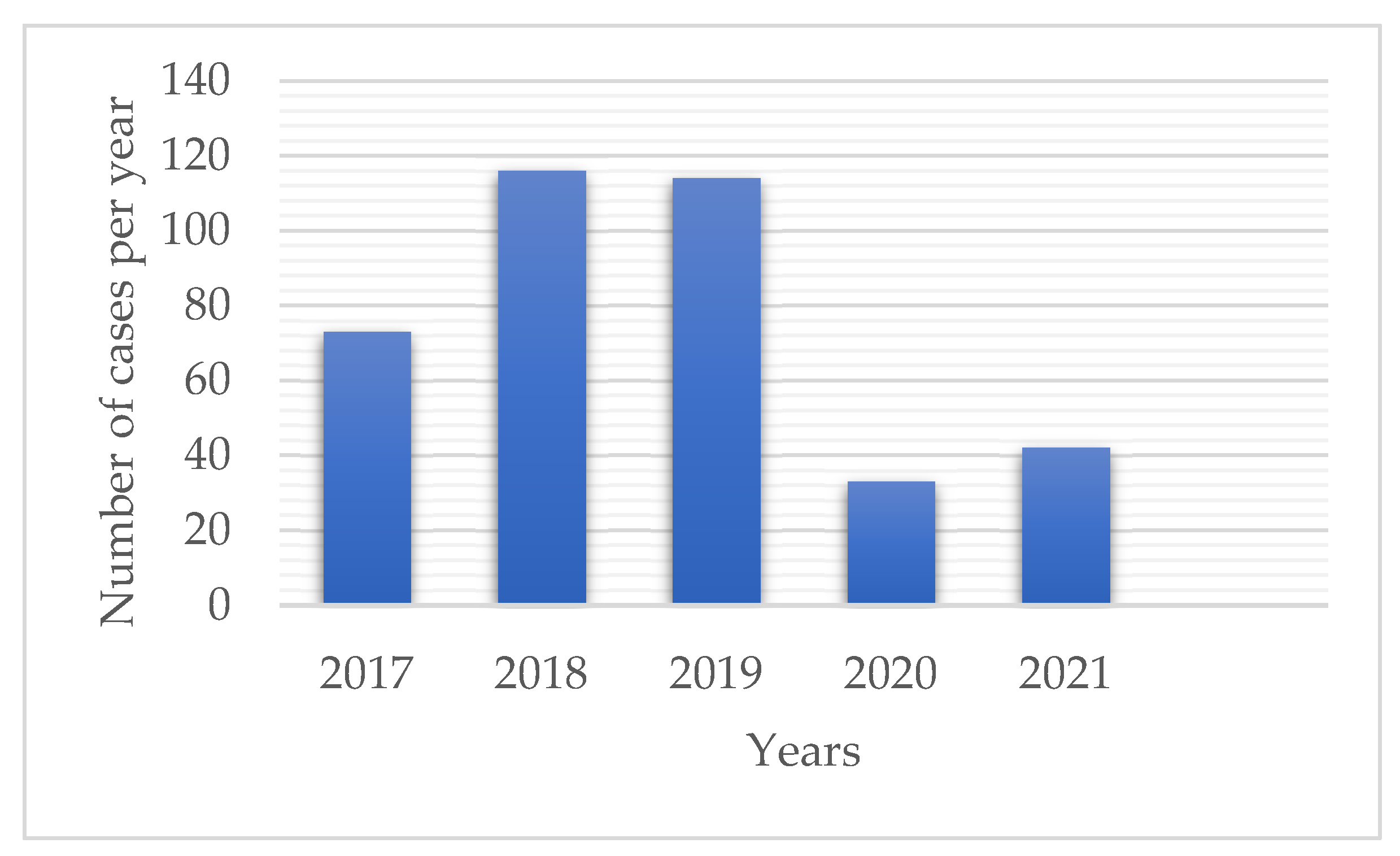
4.2. Impact of the COVID-19 Pandemic on Patient Referrals and the Number of Diagnosed Cases
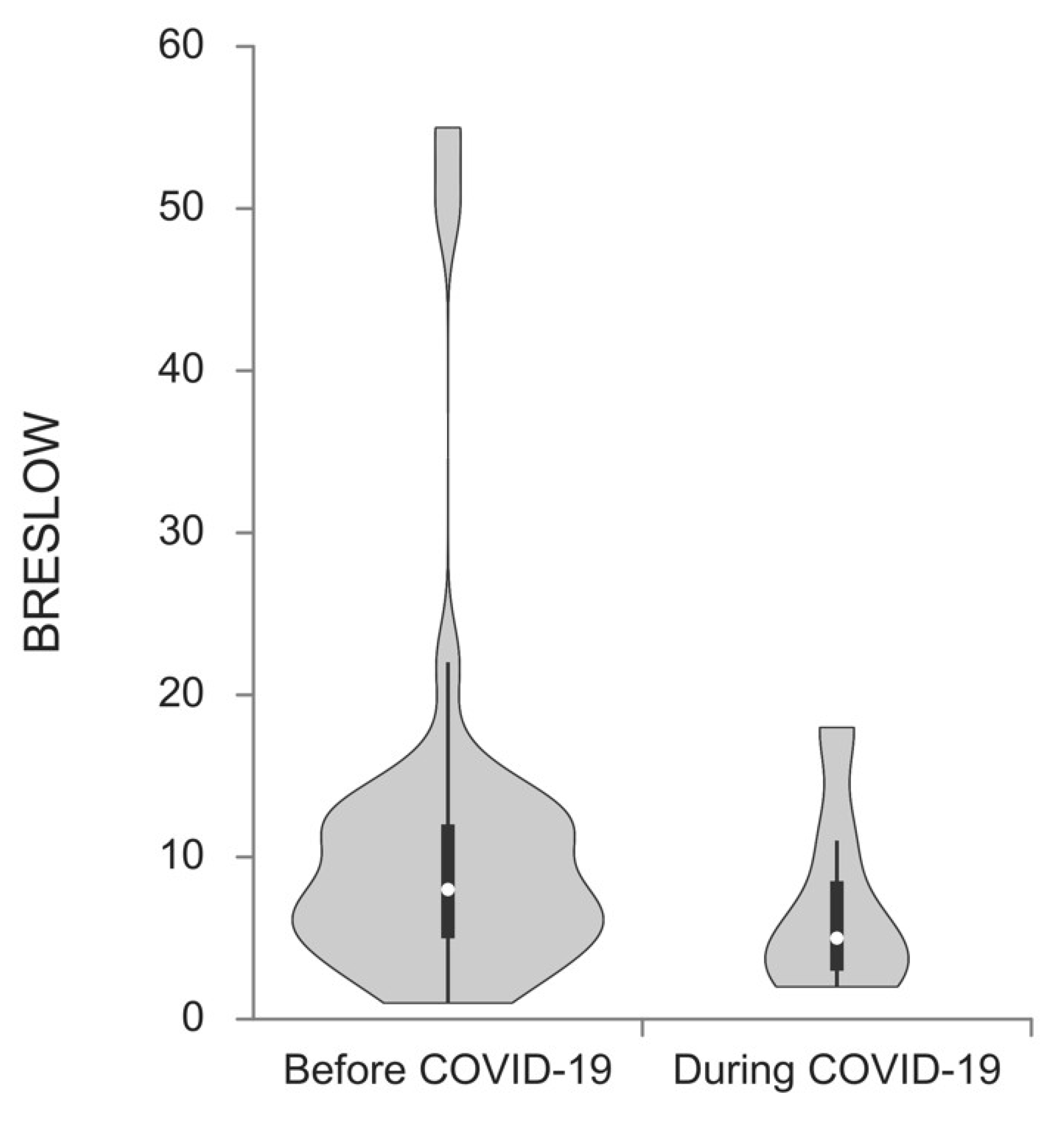
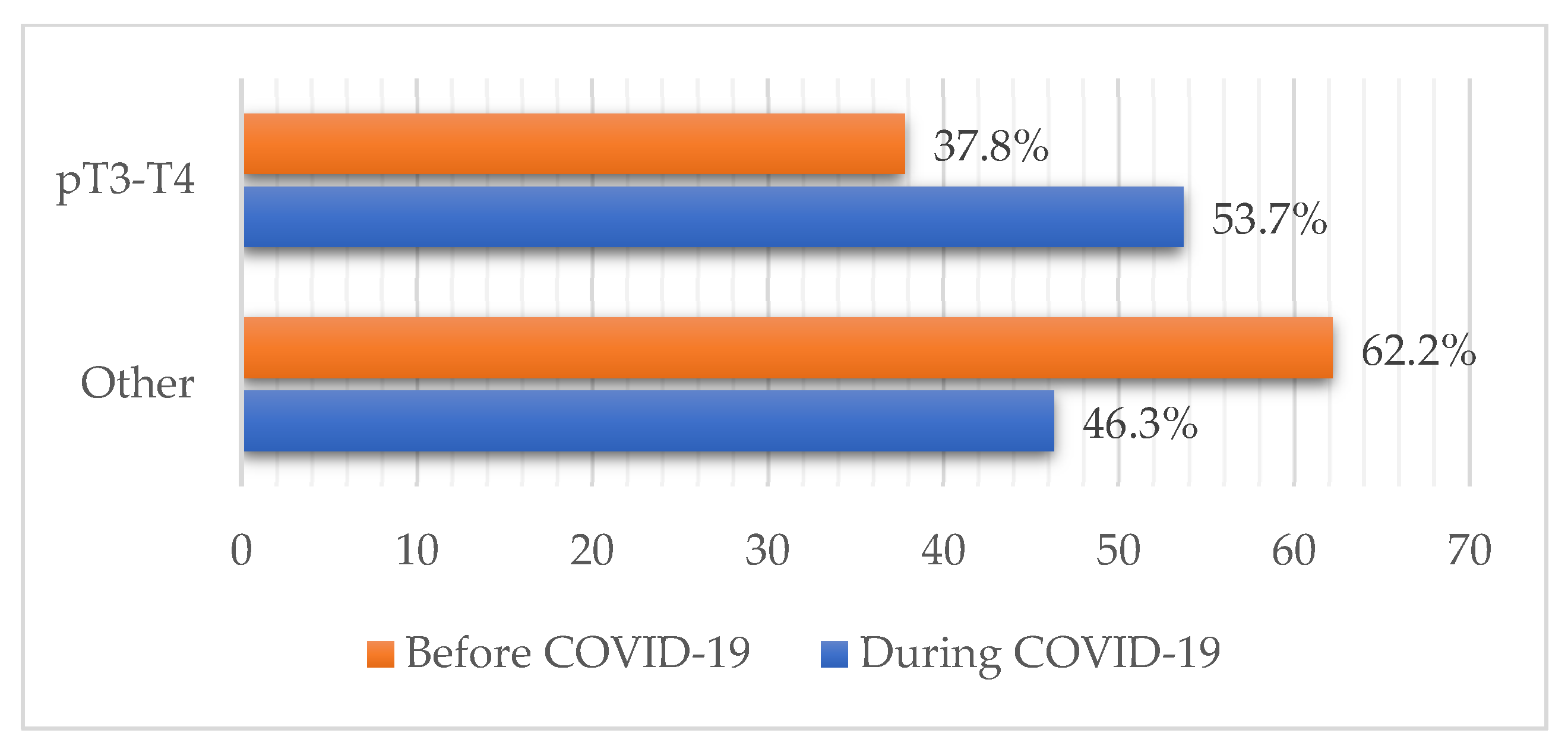
4.3. Melanoma-Specific Characteristics during the Pandemic
4.4. Strengths and Limitations of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Matthews, N.H.; Li, W.-Q.; Qureshi, A.A.; Weinstock, M.A.; Cho, E. Epidemiology of Melanoma. In Cutaneous Melanoma: Etiology and Therapy; Exon Publications: Brisbane City, Australia, 2017; Volume 1, pp. 3–22. [Google Scholar] [CrossRef]
- Aitken, J.F.; Elwood, M.; Baade, P.D.; Youl, P.; English, D. Clinical whole-body skin examination reduces the incidence of thick melanomas. Int. J. Cancer 2010, 126, 450–458. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, e359–e386. [Google Scholar] [CrossRef] [PubMed]
- Okhovat, J.-P.; Beaulieu, D.; Tsao, H.; Halpern, A.C.; Michaud, D.S.; Shaykevich, S.; Geller, A.C. The first 30 years of the American Academy of Dermatology skin cancer screening program: 1985–2014. J. Am. Acad. Dermatol. 2018, 79, 884–891.e3. [Google Scholar] [CrossRef] [PubMed]
- Erdmann, F.; Lortet-Tieulent, J.; Schüz, J.; Zeeb, H.; Greinert, R.; Breitbart, E.W.; Bray, F. International trends in the incidence of malignant melanoma 1953–2008 are recent generations at higher or lower risk? Int. J. Cancer 2012, 132, 385–400. [Google Scholar] [CrossRef] [PubMed]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef]
- Lo, S.N.; Scolyer, R.A.; Thompson, J.F. Long-Term Survival of Patients with Thin (T1) Cutaneous Melanomas: A Breslow Thickness Cut Point of 0.8 mm Separates Higher-Risk and Lower-Risk Tumors. Ann. Surg. Oncol. 2018, 25, 894–902. [Google Scholar] [CrossRef]
- Breitbart, E.W.; Waldmann, A.; Nolte, S.; Capellaro, M.; Greinert, R.; Volkmer, B.; Katalinic, A. Systematic skin cancer screening in Northern Germany. J. Am. Acad. Dermatol. 2012, 66, 201–211. [Google Scholar] [CrossRef]
- Esserman, L.J.; Thompson, I.M.; Reid, B.; Nelson, P.; Ransohoff, D.F.; Welch, H.G.; Hwang, S.; Berry, D.A.; Kinzler, K.W.; Black, W.C.; et al. Addressing overdiagnosis and overtreatment in cancer: A prescription for change. Lancet Oncol. 2014, 15, e234–e242. [Google Scholar] [CrossRef]
- Avilés-Izquierdo, J.A.; Molina-López, I.; Rodríguez-Lomba, E.; Marquez-Rodas, I.; Suarez-Fernandez, R.; Lazaro-Ochaita, P. Who detects melanoma? Impact of detection patterns on characteristics and prognosis of patients with melanoma. J. Am. Acad. Dermatol. 2016, 75, 967–974. [Google Scholar] [CrossRef]
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; de Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef]
- Coronavirus Statistics by Country-Worldometer. Available online: https://www.worldometers.info/coronavirus/country/serbia/ (accessed on 29 October 2022).
- Rosić, N.; Šantrić-Milićević, M. COVID-19 mortality in Belgrade. Srp. Med. Cas. Lek. Komore 2021, 2, 236–247. [Google Scholar] [CrossRef]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J.; Funk, S.; et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, e488–e496. [Google Scholar] [CrossRef]
- Flahault, A. COVID-19 cacophony: Is there any orchestra conductor? Lancet 2020, 395, 1037. [Google Scholar] [CrossRef]
- Layne, S.P.; Hyman, J.M.; Morens, D.M.; Taubenberger, J.K. New coronavirus outbreak: Framing questions for pandemic prevention. Sci. Transl. Med. 2020, 12, eabb1469. [Google Scholar] [CrossRef]
- Vlada Republike Srbije. Odluka o Proglašenju Vanrednog Stanja: 29/2020-3. Available online: https://www.pravno-informacioni-sistem.rs/SlGlasnikPortal/eli/rep/sgrs/predsednik/odluka/2020/29/1/reg (accessed on 14 July 2022).
- Đikić, M.; Gujaničić, D.; Milićević-Nešić, I.; Ercegovac, M.; Dželebdžić, S.; Lukić, I.; Andrić, B.; Miladinović, T. Triage at a non-covid hospital during the COVID-19 pandemic. Srp. Med. Cas. Lek. Komore 2021, 2, 220–227. [Google Scholar] [CrossRef]
- Gisondi, P.; Piaserico, S.; Conti, A.; Naldi, L. Dermatologists and SARS-CoV-2: The impact of the pandemic on daily practice. J. Eur. Acad. Dermatol. Venereol. 2020, 34, 1196–1201. [Google Scholar] [CrossRef]
- O’Reilly-Shah, V.N.; Van Cleve, W.; Long, D.R.; Moll, V.; Evans, F.M.; Sunshine, J.E.; Kassebaum, N.J.; Harrison, E.M.; Jabaley, C.S. Impact of COVID-19 response on global surgical volumes: An ongoing observational study. Bull. World Health Organ. 2020, 98, 671–682. [Google Scholar] [CrossRef]
- London, J.W.; Fazio-Eynullayeva, E.; Palchuk, M.B.; Sankey, P.; McNair, C. Effects of the COVID-19 Pandemic on Cancer-Related Patient Encounters. JCO Clin. Cancer Inform. 2020, 4, 657–665. [Google Scholar] [CrossRef]
- Carenzo, L.; Costantini, E.; Greco, M.; Barra, F.L.; Rendiniello, V.; Mainetti, M.; Bui, R.; Zanella, A.; Grasselli, G.; Lagioia, M.; et al. Hospital surge capacity in a tertiary emergency referral centre during the COVID-19 outbreak in Italy. Anaesthesia 2020, 75, 928–934. [Google Scholar] [CrossRef]
- Xu, S.; Glenn, S.; Sy, L.; Qian, L.; Hong, V.; Ryan, D.S.; Jacobsen, S. Impact of the COVID-19 Pandemic on Health Care Utilization in a Large Integrated Health Care System: Retrospective Cohort Study. J. Med. Internet Res. 2021, 23, e26558. [Google Scholar] [CrossRef]
- Stojanović, D.; Mitrović, N.; Stevanović, D.; Jašarović, D.; Milina, S.; Surla, D.; Radmilović, S.; Ilić, G.; Lazić, A.; Lukić, B.; et al. The role of surgeons during the COVID-19 pandemic: The experience of the Surgery Clinic of the Clinical Hospital Center ‘Zemun’. Srp. Med. Cas. Lek. Komore 2021, 2, 228–235. [Google Scholar] [CrossRef]
- Gomolin, T.; Cline, A.; Handler, M.Z. The danger of neglecting melanoma during the COVID-19 pandemic. J. Dermatol. Treat. 2020, 31, 444–445. [Google Scholar] [CrossRef] [PubMed]
- Maringe, C.; Spicer, J.; Morris, M.; Purushotham, A.; Nolte, E.; Sullivan, R.; Rachet, B.; Aggarwal, A. The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: A national, population-based, modelling study. Lancet Oncol. 2020, 21, 1023–1034. [Google Scholar] [CrossRef] [PubMed]
- Gisondi, P.; Cazzaniga, S.; Di Leo, S.; Piaserico, S.; Bellinato, F.; Pizzolato, M.; Gatti, A.; Eccher, A.; Brunelli, M.; Saraggi, D.; et al. Impact of the COVID-19 pandemic on melanoma diagnosis. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e714–e715. [Google Scholar] [CrossRef] [PubMed]
- Hoellwerth, M.; Kaiser, A.; Emberger, M.; Brandlmaier, M.; Laimer, M.; Egger, A.; Bauer, J.W.; Koelblinger, P. COVID-19-Induced Reduction in Primary Melanoma Diagnoses: Experience from a Dermatopathology Referral Center. J. Clin. Med. 2021, 10, 4059. [Google Scholar] [CrossRef]
- Aldecoa-Otalora, J.S.; Pascual, L.L.; Iturriagagoitia, A.C.; Bayona, J.Y. [Translated article] Has the COVID-19 Pandemic and Lockdown Affected Breslow Thickness in Cutaneous Melanoma? Actas Dermosifiliogr. 2022, 113, e107–e109. [Google Scholar] [CrossRef]
- Ricci, F.; Fania, L.; Paradisi, A.; Di Lella, G.; Pallotta, S.; Sobrino, L.; Panebianco, A.; Annessi, G.; Abeni, D. Delayed melanoma diagnosis in the COVID-19 era: Increased breslow thickness in primary melanomas seen after the COVID-19 lockdown. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e778–e779. [Google Scholar] [CrossRef]
- Shannon, A.B.; Sharon, C.E.; Straker, R.J.; Miura, J.T.; Ming, M.E.; Chu, E.Y.; Karakousis, G.C. The impact of the COVID-19 pandemic on the presentation status of newly diagnosed melanoma: A single institution experience. J. Am. Acad. Dermatol. 2021, 84, 1096–1098. [Google Scholar] [CrossRef]
- Weston, G.K.; Jeong, H.S.; Mu, E.W.; Polsky, D.; Meehan, S.A. Impact of COVID-19 on melanoma diagnosis. Melanoma Res. 2021, 31, 280–281. [Google Scholar] [CrossRef]
- Gualdi, G.; Porreca, A.; Amoruso, G.F.; Atzori, L.; Calzavara-Pinton, P.; De Tursi, M.; Di Buduo, A.; Di Marino, P.; Fabroncini, G.; Fantini, F.; et al. The Effect of the COVID-19 Lockdown on Melanoma Diagnosis in Italy. Clin. Dermatol. 2021, 39, 911–919. [Google Scholar] [CrossRef]
- Lamm, R.; Lyons, W.; So, W.; Willis, A.I. Advanced-Stage Melanoma at Presentation Following the Peak of the Pandemic: A COVID-19 Cancer Canary in a Coal Mine. World J. Surg. 2022, 46, 1820–1825. [Google Scholar] [CrossRef]
- Kostner, L.; Cerminara, S.E.; Pamplona, G.S.P.; Maul, J.-T.; Dummer, R.; Ramelyte, E.; Mangana, J.; Wagner, N.B.; Cozzio, A.; Kreiter, S.; et al. Effects of COVID-19 Lockdown on Melanoma Diagnosis in Switzerland: Increased Tumor Thickness in Elderly Females and Shift towards Stage IV Melanoma during Lockdown. Cancers 2022, 14, 2360. [Google Scholar] [CrossRef]
- Molinier, R.; Roger, A.; Genet, B.; Blom, A.; Longvert, C.; Chaplain, L.; Fort, M.; Saiag, P.; Funck-Brentano, E. Impact of the French COVID-19 pandemic lockdown on newly diagnosed melanoma delay and severity. J. Eur. Acad. Dermatol. Venereol. 2022, 36, e164–e166. [Google Scholar] [CrossRef]
- Ungureanu, L.; Apostu, A.P.; Vesa, C.; Cășeriu, A.E.; Frățilă, S.; Iancu, G.; Bejinariu, N.; Munteanu, M.; Șenilă, S.C.; Vasilovici, A. Impact of the COVID-19 Pandemic on Melanoma Diagnosis in Romania—Data from Two University Centers. Int. J. Environ. Res. Public Health 2022, 19, 15129. [Google Scholar] [CrossRef]
- Lallas, A.; Kyrgidis, A.; Manoli, S.-M.; Papageorgiou, C.; Lallas, K.; Sotiriou, E.; Vakirlis, E.; Sidiropoulos, T.; Ioannides, D.; Apalla, Z. Delayed skin cancer diagnosis in 2020 because of the COVID-19-related restrictions: Data from an institutional registry. J. Am. Acad. Dermatol. 2021, 85, 721–723. [Google Scholar] [CrossRef]
- Gaunt, N.; Green, R.; Motta, L.; Jamieson, L. Skin cancers in lockdown: No impact on pathological tumour staging. Br. J. Dermatol. 2021, 185, 844–846. [Google Scholar] [CrossRef]
- Sangers, T.E.; Wakkee, M.; Kramer-Noels, E.C.; Nijsten, T.; Louwman, M.W.; Jaspars, E.H.; Hollestein, L.M. Limited impact of COVID-19-related diagnostic delay on cutaneous melanoma and squamous cell carcinoma tumour characteristics: A nationwide pathology registry analysis. Br. J. Dermatol. 2022, 187, 196–202. [Google Scholar] [CrossRef]
- Gedeah, C.; Damsin, T.; Absil, G.; Somja, J.; Collins, P.; Rorive, A.; Marchal, N.; Seidel, L.; Nikkels, A.F. The impact of COVID-19 on the new diagnoses of melanoma. Eur. J. Dermatol. 2021, 31, 565–567. [Google Scholar] [CrossRef]
- McFeely, O.; Hollywood, A.; Stanciu, M.; O’Connell, M.; Paul, L. Comment on “The impact of the COVID-19 pandemic on the presentation status of newly diagnosed melanoma: A single institution experience”. J. Am. Acad. Dermatol. 2021, 85, e419. [Google Scholar] [CrossRef]
- Weissgerber, T.L.; Savic, M.; Winham, S.J.; Stanisavljevic, D.; Garovic, V.D.; Milic, N.M. Data visualization, bar naked: A free tool for creating interactive graphics. J. Biol. Chem. 2017, 292, 20592–20598. [Google Scholar] [CrossRef]
- Longo, C.; Pampena, R.; Fossati, B.; Pellacani, G.; Peris, K. Melanoma diagnosis at the time of COVID-19. Int. J. Dermatol. 2021, 60, e29–e30. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, G.; De Vincentiis, L.; Ambrosini-Spaltro, A.; Barbareschi, M.; Bertolini, V.; Contato, E.; Crivelli, F.; Feyles, E.; Mariani, M.P.; Morelli, L.; et al. Cancer Diagnostic Delay in Northern and Central Italy During the 2020 Lockdown Due to the Coronavirus Disease 2019 Pandemic: Assessment of the Magnitude of the Problem and Proposals for Corrective Actions. Am. J. Clin. Pathol. 2021, 155, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Arenbergerova, M.; Lallas, A.; Nagore, E.; Rudnicka, L.; Forsea, A.; Pasek, M.; Meier, F.; Peris, K.; Olah, J.; Posch, C. Position statement of the EADV Melanoma Task Force on recommendations for the management of cutaneous melanoma patients during COVID-19. J. Eur. Acad. Dermatol. Venereol. 2021, 35, e427–e428. [Google Scholar] [CrossRef] [PubMed]
- Rashid, S.; Tsao, H. Effect of the COVID-19 Pandemic on Delayed Skin Cancer Services. Dermatol. Clin. 2021, 39, 627–637. [Google Scholar] [CrossRef] [PubMed]
- Conforti, C.; Lallas, A.; Argenziano, G.; Dianzani, C.; Di Meo, N.; Giuffrida, R.; Kittler, H.; Malvehy, J.; Marghoob, A.A.; Soyer, H.P.; et al. Impact of the COVID-19 Pandemic on Dermatology Practice Worldwide: Results of a Survey Promoted by the International Dermoscopy Society (IDS). Dermatol. Pract. Concept. 2021, 11, e2021153. [Google Scholar] [CrossRef]
- The Global Coalition for Melanoma Patient Advocacy Survey Reveals One Fifth of Melanomas, Globally, Went Undiagnosed during COVID-19 Pandemic-Spot the Dot. Available online: https://spotthedot.org/en/news/survey-reveals-one-fifth-of-melanomas-globally-went-undiagnosed-during-covid-19-pandemic/ (accessed on 9 October 2022).
- Peacock, H.; Tambuyzer, T.; Verdoodt, F.; Calay, F.; Poirel, H.; De Schutter, H.; Francart, J.; Van Damme, N.; Van Eycken, L. Decline and incomplete recovery in cancer diagnoses during the COVID-19 pandemic in Belgium: A year-long, population-level analysis. ESMO Open 2021, 6, 100197. [Google Scholar] [CrossRef]
- Wargon, M.; Guidet, B.; Hoang, T.D.; Hejblum, G. A systematic review of models for forecasting the number of emergency department visits. Emerg. Med. J. 2009, 26, 395–399. [Google Scholar] [CrossRef]
- Diehl, A.K.; Morris, M.D.; Mannis, S.A. Use of Calendar and Weather Data to Predict Walk-In Attendance. South. Med. J. 1981, 74, 709–712. [Google Scholar] [CrossRef]
- Holleman, D.R.; Bowling, R.L.; Gathy, C. Predicting daily visits to a waik-in clinic and emergency department using calendar and weather data. J. Gen. Intern. Med. 1996, 11, 237–239. [Google Scholar] [CrossRef]
- Batal, H.; Tench, J.; McMillan, S.; Adams, J.; Mehler, P.S. Predicting Patient Visits to an Urgent Care Clinic Using Calendar Variables. Acad. Emerg. Med. 2001, 8, 48–53. [Google Scholar] [CrossRef]
- Wang, R.; Helf, C.; Tizek, L.; Neuhauser, R.; Eyerich, K.; Zink, A.; Eberlein, B.; Biedermann, T.; Brockow, K.; Boehner, A. The Impact and Consequences of SARS-CoV-2 Pandemic on a Single University Dermatology Outpatient Clinic in Germany. Int. J. Environ. Res. Public Health 2020, 17, 6182. [Google Scholar] [CrossRef]
- Chang, M.S.; Leachman, S.A.; Berry, E.G.; Curiel-Lewandrowski, C.; Geller, A.C.; Grossman, D.; Kim, C.C.; Stein, J.A.; Swetter, S.M.; Hartman, R.I. Changes in melanoma care practices during the COVID-19 pandemic: A multi-institutional cross-sectional survey. Dermatol. Online J. 2021, 27, 13030. [Google Scholar] [CrossRef]
- Barruscotti, S.; Giorgini, C.; Brazzelli, V.; Vassallo, C.; Michelerio, A.; Klersy, C.; Chiellino, S.; Tomasini, C.F. A significant reduction in the diagnosis of melanoma during the COVID-19 lockdown in a third-level center in the Northern Italy. Dermatol. Ther. 2020, 33, e14074. [Google Scholar] [CrossRef]
- Schauer, A.A.; Kulakov, E.L.; Martyn-Simmons, C.L.; Bunker, C.B.; Edmonds, E.V.J. Melanoma defies ‘lockdown’: Ongoing detection during Covid-19 in central London. Clin. Exp. Dermatol. 2020, 45, 900. [Google Scholar] [CrossRef]
- Teuscher, M.; Diehl, K.; Schaarschmidt, M.-L.; Weilandt, J.; Sasama, B.; Ohletz, J.; Könnecke, A.; Harth, W.; Hillen, U.; Peitsch, W.K. Effects of the COVID-19 pandemic on care of melanoma patients in Berlin, Germany: The Mela-COVID survey. Eur. J. Dermatol. 2021, 31, 521–529. [Google Scholar] [CrossRef]
- Nagore, E.; Martorell-Calatayud, A.; Botella-Estrada, R.; Guillén, C. Growth rate as an independent prognostic factor in localized invasive cutaneous melanoma. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 618–620. [Google Scholar] [CrossRef]
- Gualdi, G.; Panarese, F.; Meogrossi, G.; Marchioni, M.; De Tursi, M.; Di Martino, P.; Angelucci, D.; Amatetti, M.; Proietto, G.; Di Nicola, M.; et al. Speed rate (SR) as a new dynamic index of melanoma behavior. Pigment. Cell Melanoma Res. 2020, 33, 709–718. [Google Scholar] [CrossRef]
- Carlson, J.A. Tumor Doubling Time of Cutaneous Melanoma and its Metastasis. Am. J. Dermatopathol. 2003, 25, 291–299. [Google Scholar] [CrossRef]
- Ryu, E.B.; Chang, J.M.; Seo, M.; Kim, S.A.; Lim, J.H.; Moon, W.K. Tumour volume doubling time of molecular breast cancer subtypes assessed by serial breast ultrasound. Eur. Radiol. 2014, 24, 2227–2235. [Google Scholar] [CrossRef]
- Hong, J.H.; Park, S.; Kim, H.; Goo, J.M.; Park, I.K.; Kang, C.H.; Kim, Y.T.; Yoon, S.H. Volume and Mass Doubling Time of Lung Adenocarcinoma according to WHO Histologic Classification. Korean J. Radiol. 2021, 22, 464–475. [Google Scholar] [CrossRef]
- Matsui, T.; Yao, T.; Iwashita, A. Natural history of early colorectal cancer. World J. Surg. 2000, 24, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Coory, M.; Baade, P.; Aitken, J.; Smithers, B.M.; McLeod, G.R.C.; Ring, I. Trends for in situ and Invasive Melanoma in Queensland, Australia, 1982–2002. Cancer Causes Control 2006, 17, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Scoggins, C.R.; Ross, M.I.; Reintgen, D.S.; Noyes, R.D.; Goydos, J.; Beitsch, P.D.; Urist, M.M.; Ariyan, S.; Sussman, J.J.; Edwards, M.J.; et al. Gender-Related Differences in Outcome for Melanoma Patients. Ann. Surg. 2006, 243, 693. [Google Scholar] [CrossRef] [PubMed]
- Behbahani, S.; Maddukuri, S.; Cadwell, J.; Lambert, W.C.; Schwartz, R.A. Gender differences in cutaneous melanoma: Demographics, prognostic factors, and survival outcomes. Dermatol. Ther. 2020, 33, e14131. [Google Scholar] [CrossRef]
- Bellenghi, M.; Puglisi, R.; Pontecorvi, G.; De De Feo, A.; Carè, A.; Mattia, G. Sex and Gender Disparities in Melanoma. Cancers 2020, 12, 1819. [Google Scholar] [CrossRef]
- Tejera-Vaquerizo, A.; Nagore, E. Estimated effect of COVID-19 lockdown on melanoma thickness and prognosis: A rate of growth model. J. Eur. Acad. Dermatol. Venereol. 2020, 34, e351–e353. [Google Scholar] [CrossRef]
- NCCN. Clinical Practice Guidelines in Oncology: NMSC. Available online: https://www.nccn.org/guidelines/recently-published-guidelines (accessed on 9 October 2022).
- British Association of Dermatologists & British Society for Dermatological Surgery. COVID-19—Skin Cancer Surgery Guidance. Available online: https://www.bad.org.uk/covid-19 (accessed on 10 October 2022).
- Crawford, G.; Vinelli, G.; Lehrer, M. SDG Recommendations for Management of Skin Cancer during the COVID-19 Pandemic. Available online: https://www.padermatology.org/uploads/1/0/5/4/105403301/sdg_guidelines_for_nmsc_-__3_apr_2020.pdf (accessed on 10 October 2022).
- Garbe, C.; Amaral, T.; Peris, K.; Hauschild, A.; Arenberger, P.; Bastholt, L.; Bataille, V.; del Marmol, V.; Dréno, B.; Fargnoli, M.C.; et al. European consensus-based interdisciplinary guideline for melanoma. Part 2: Treatment—Update 2019. Eur. J. Cancer 2020, 126, 159–177. [Google Scholar] [CrossRef]
- Coit, D.G.; Thompson, J.A.; Albertini, M.R.; Barker, C.; Carson, W.E.; Contreras, C.; Daniels, G.A.; DiMaio, D.; Fields, R.C.; Fleming, M.D.; et al. Cutaneous Melanoma, Version 2.2019. JNCCN J. Natl. Compr. Cancer Netw. 2019, 17, 367–402. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Pre-COVID-19 | COVID-19 | |||
|---|---|---|---|---|
| Total | n = 339 | n = 54 | p | |
| (86.3%) | (13.7%) | Value | ||
| Average cases per year (mean ± SD) | 101 ± 24.3 | 37.5 ± 6.4 | 0.036 | |
| Age (mean ± SD) | 64.5 ± 15.8 | 65.7 ± 15.3 | ||
| Age groups: | 0.852 | |||
| ≤40 years | 39 (9.9%) | 34 (10.0%) | 5 (9.3%) | |
| 41–60 years | 104 (26.5%) | 92 (27.1%) | 12 (22.2%) | |
| 61–80 years | 191 (48.6%) | 162 (47.8%) | 29 (53.7%) | |
| >80 years | 59 (15%) | 51 (15.0%) | 8 (14.8%) | |
| Sex: | 0.978 | |||
| Male | 219 (55.7%) | 189 (55.8%) | 30 (55.6%) | |
| Female | 174 (44.3%) | 150 (44.2%) | 24 (44.4%) | |
| Body distribution: | 0.137 | |||
| Head and Neck | 81 (20.6%) | 68 (20.1%) | 13 (24.1%) | |
| Torso | 154 (39.2%) | 127 (37.5%) | 27 (50.0%) | |
| Upper extremities | 76 (19.3%) | 70 (20.6%) | 6 (11.1%) | |
| Lower extremities | 82 (20.9%) | 74 (21.8%) | 8 (14.8%) | |
| Melanoma subtype: | 0.282 | |||
| Superficial spreading | 258 (65.6%) | 227 (67.0%) | 31 (57.4%) | |
| Lentigo maligna | 38 (9.7%) | 31 (9.1%) | 7 (13.0%) | |
| Nodular | 73 (18.6%) | 59 (17.4%) | 14 (25.9%) | |
| Others | 24 (6.1%) | 22 (6.5%) | 2 (3.7%) | |
| Breslow thickness (median, 25th–75th percentile) | 1.80 (0.65–4.30) | 3.00 (1.5–5.30) | 0.010 | |
| Breslow thickness: | 0.088 | |||
| <1 mm | 111 (28.2%) | 160 (47.2%) | 19 (35.2%) | |
| 1.01–2 mm | 57 (14.5%) | 51 (15.0%) | 6 (11.1%) | |
| 2.01–4 mm | 64 (16.3%) | 51 (15.0%) | 13 (24.1%) | |
| >4 mm | 93 (23.7%) | 77 (22.7%) | 16 (29.6%) | |
| pT staging: | 0.088 | |||
| In situ | 68 (17.3%) | 57 (16.8%) | 11 (20.4%) | |
| T1 | 111 (28.2%) | 103 (30.4%) | 8 (14.8%) | |
| T2 | 57 (14.5%) | 51 (15.0%) | 6 (11.1%) | |
| T3 | 64 (16.3%) | 51 (15.0%) | 13 (24.1%) | |
| T4 | 93 (23.7%) | 77 (22.7%) | 16 (29.6%) | |
| Clark level: | 0.029 | |||
| I | 68 (17.3%) | 57 (16.8%) | 11 (20.4%) | |
| II | 61 (15.5%) | 58 (17.1%) | 3 (5.6%) | |
| III | 81 (20.6%) | 75 (22.1%) | 6 (11.1%) | |
| IV | 159 (40.5%) | 129 (38.1%) | 30 (55.6%) | |
| V | 24 (6.1%) | 20 (5.9%) | 4 (7.4%) | |
| Mitotic index rate (median, 25th–75th percentile): | 2 (0–5) | 5 (1–12) | <0.001 | |
| Ulcerations present: | 0.179 | |||
| Yes | 114 (35.1%) | 95 (33.7%) | 19 (44.2%) | |
| No | 211 (64.9%) | 187 (66.3%) | 24 (55.8%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeremić, J.; Suđecki, B.; Radenović, K.; Mihaljević, J.; Radosavljević, I.; Jovanović, M.; Milić, N.; Pavlović, V.; Brašanac, D.; Jović, M. Impact of the COVID-19 Pandemic on Melanoma Diagnosis: Increased Breslow Thickness in Primary Melanomas—A Single Center Experience. Int. J. Environ. Res. Public Health 2022, 19, 16806. https://doi.org/10.3390/ijerph192416806
Jeremić J, Suđecki B, Radenović K, Mihaljević J, Radosavljević I, Jovanović M, Milić N, Pavlović V, Brašanac D, Jović M. Impact of the COVID-19 Pandemic on Melanoma Diagnosis: Increased Breslow Thickness in Primary Melanomas—A Single Center Experience. International Journal of Environmental Research and Public Health. 2022; 19(24):16806. https://doi.org/10.3390/ijerph192416806
Chicago/Turabian StyleJeremić, Jelena, Branko Suđecki, Kristina Radenović, Jovan Mihaljević, Ivan Radosavljević, Milan Jovanović, Nataša Milić, Vedrana Pavlović, Dimitrije Brašanac, and Marko Jović. 2022. "Impact of the COVID-19 Pandemic on Melanoma Diagnosis: Increased Breslow Thickness in Primary Melanomas—A Single Center Experience" International Journal of Environmental Research and Public Health 19, no. 24: 16806. https://doi.org/10.3390/ijerph192416806
APA StyleJeremić, J., Suđecki, B., Radenović, K., Mihaljević, J., Radosavljević, I., Jovanović, M., Milić, N., Pavlović, V., Brašanac, D., & Jović, M. (2022). Impact of the COVID-19 Pandemic on Melanoma Diagnosis: Increased Breslow Thickness in Primary Melanomas—A Single Center Experience. International Journal of Environmental Research and Public Health, 19(24), 16806. https://doi.org/10.3390/ijerph192416806