
Serum Levels of CXCR4, SDF-1, MCP-1, NF-κB and ERK1/2 in Patients with Skeletal Fluorosis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Sample Collection and Processing
2.3. Measurement of Cytokines
2.4. Statistical Analysis
3. Results
3.1. Demographic Data
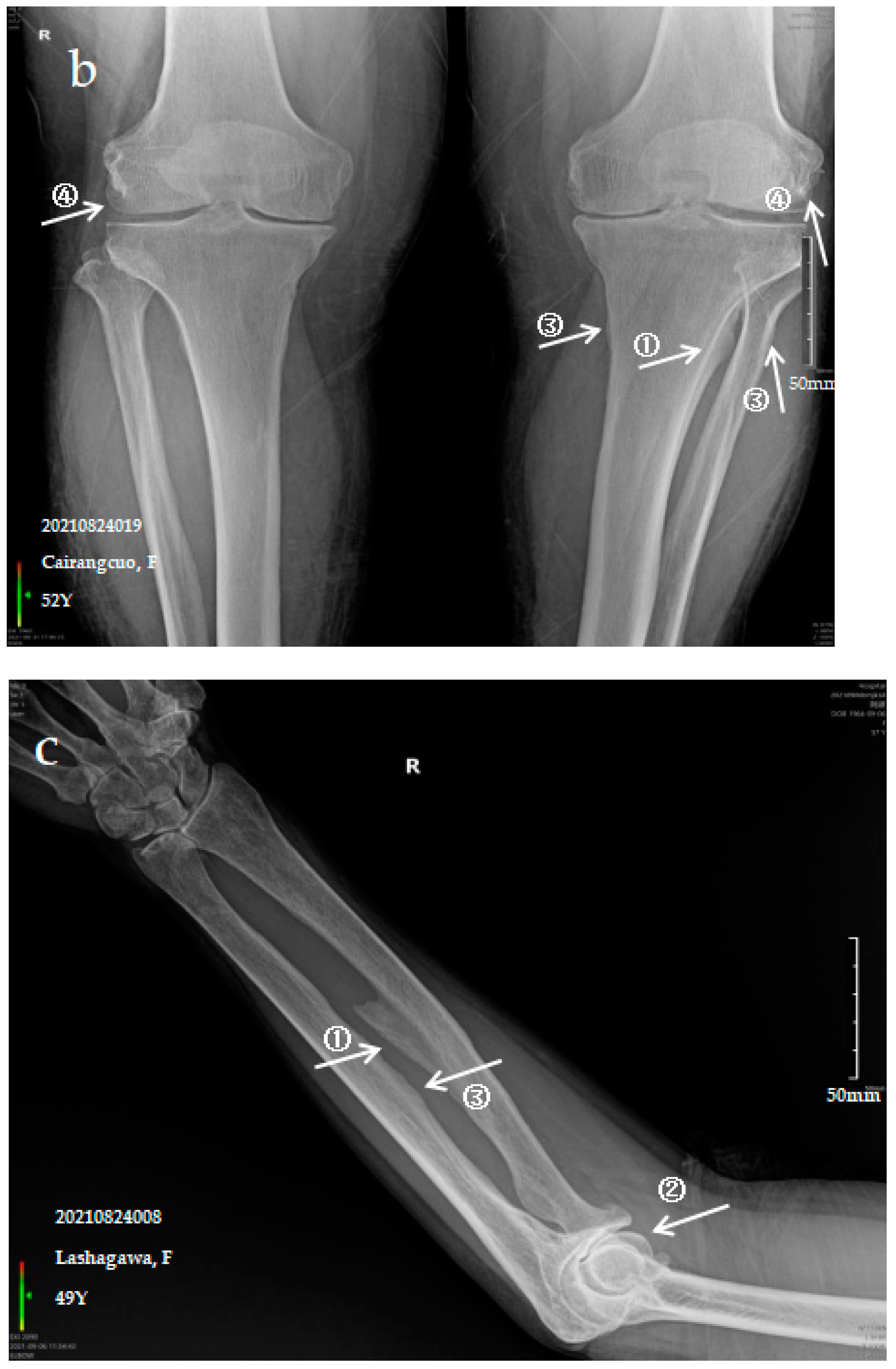
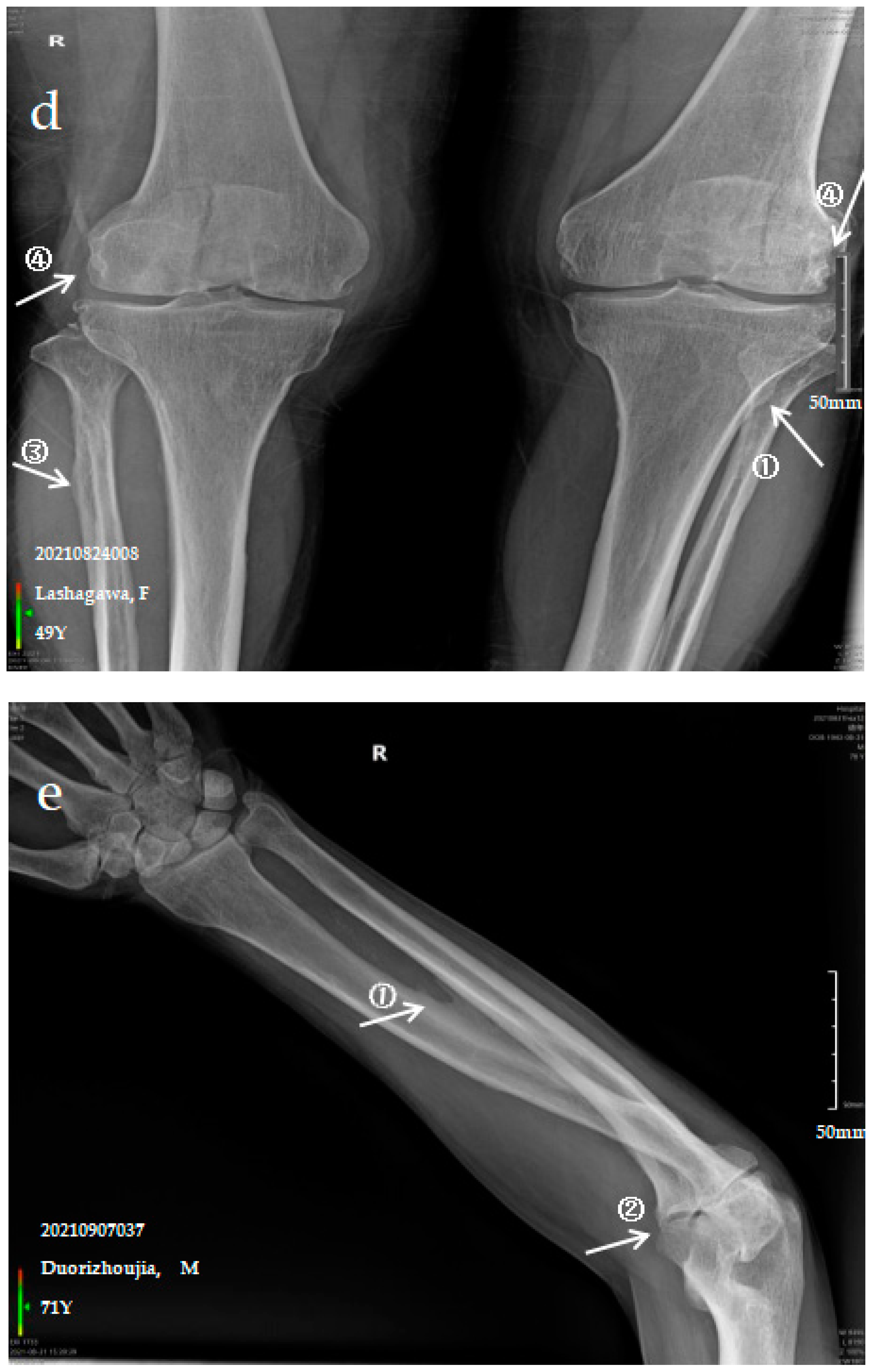
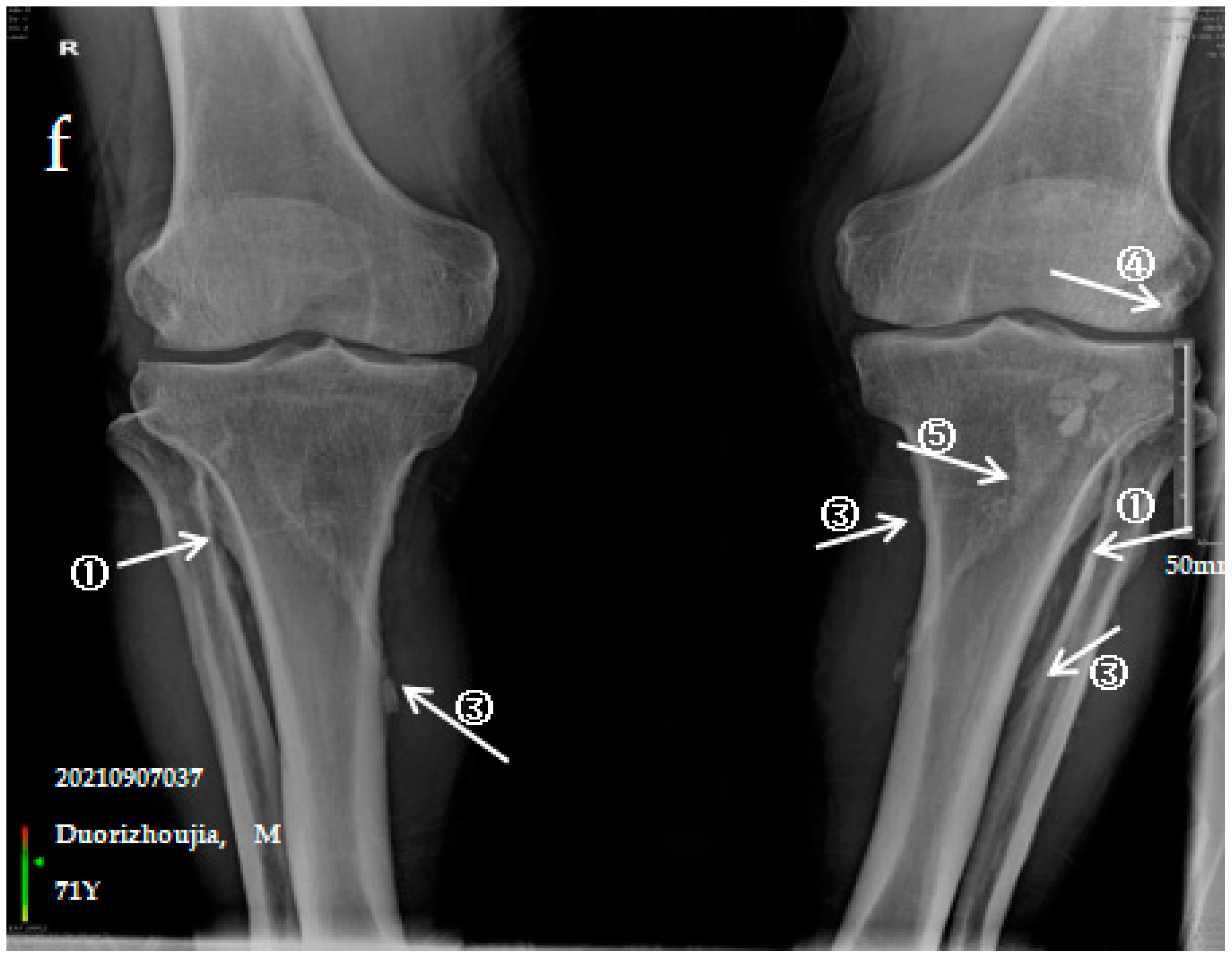
3.2. X-ray Imaging Analysis of SF Patients
3.2.1. Case Analysis of a Patient Diagnosed by X-ray with Mild SF
3.2.2. Case Analysis of a Patient Diagnosed by X-ray with Moderate SF
3.2.3. Case Analysis of a Patient Diagnosed by X-ray with Severe SF
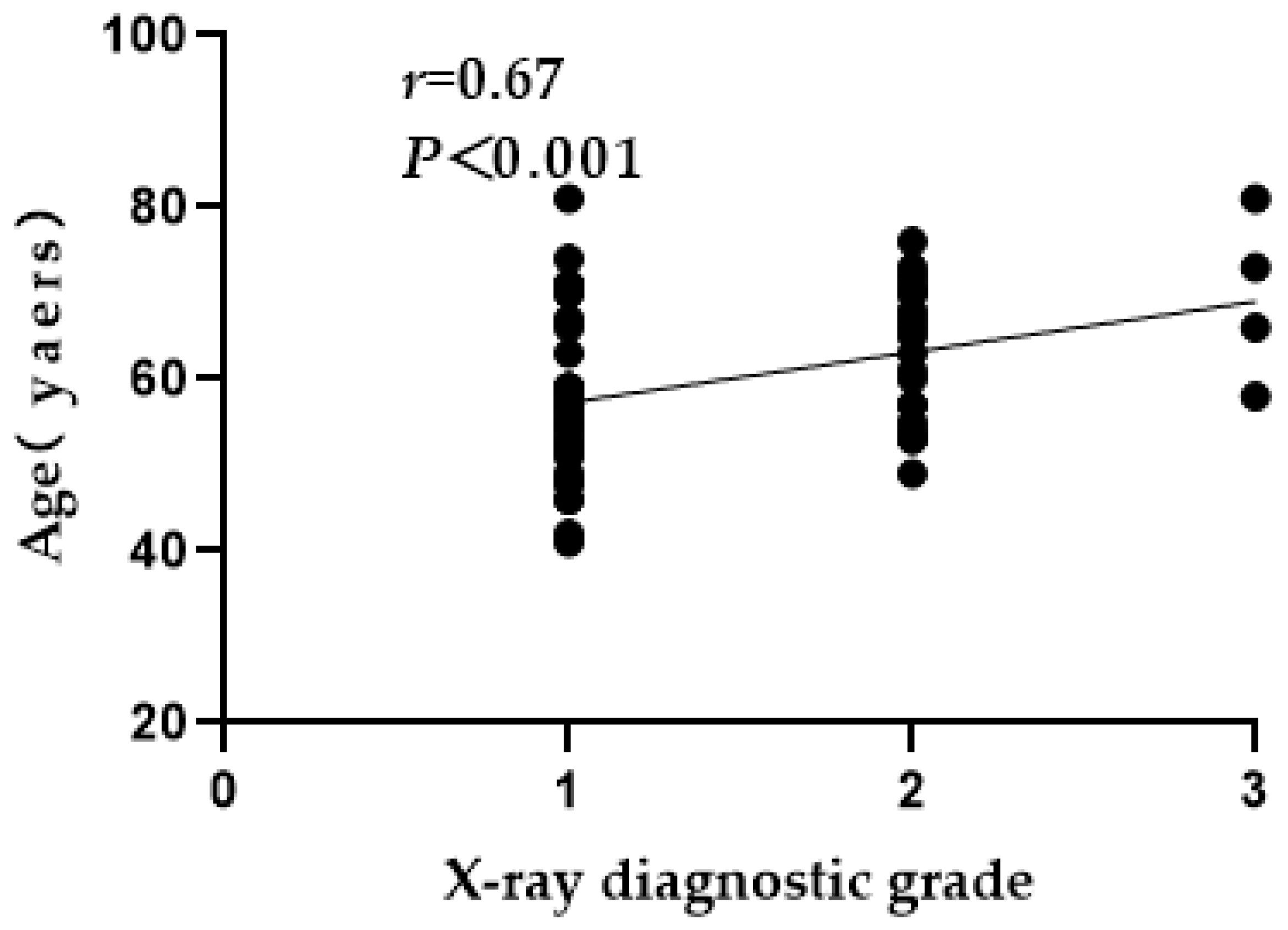
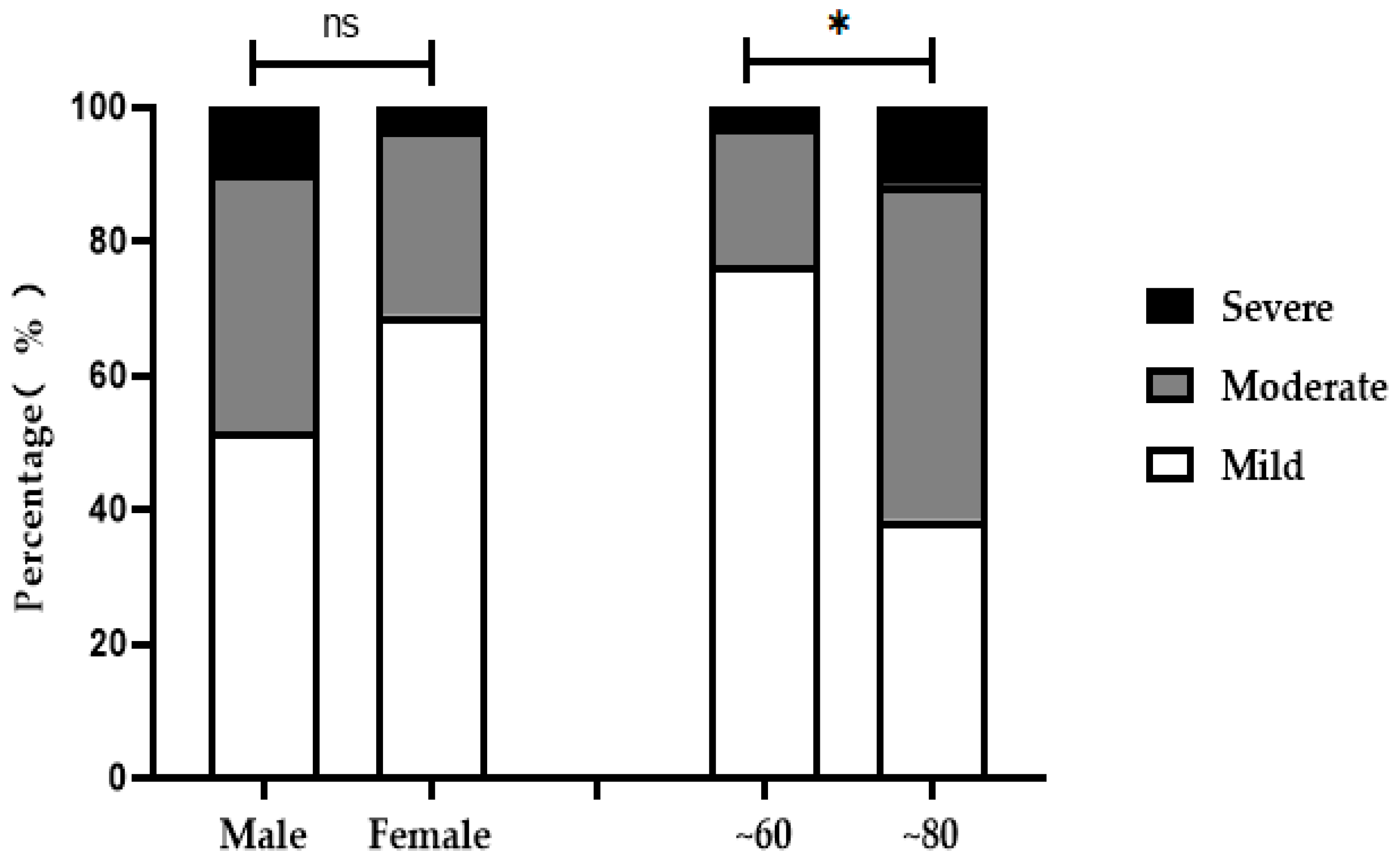
3.3. X-ray Grade Analysis of Ages, Age Groups and Sexes
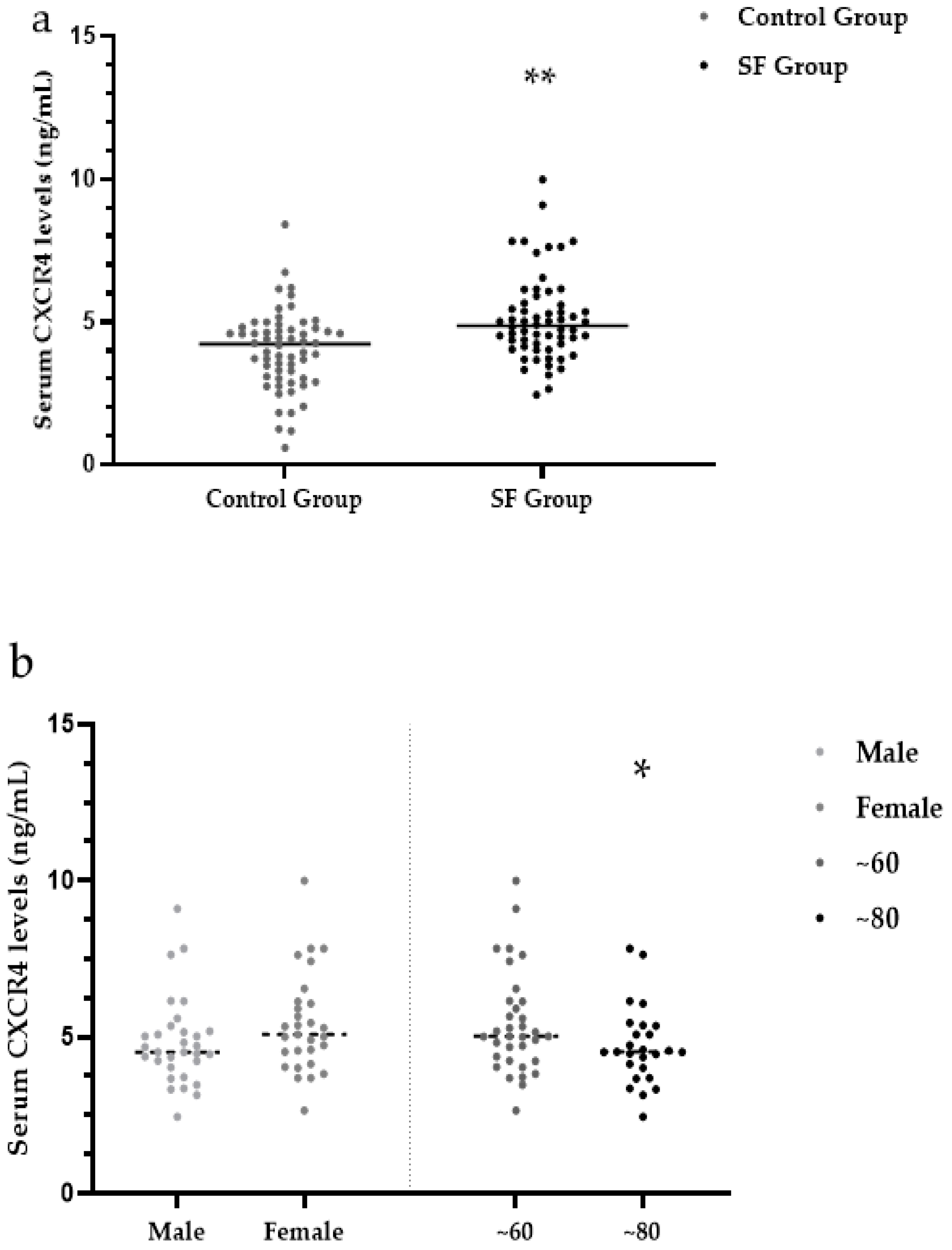
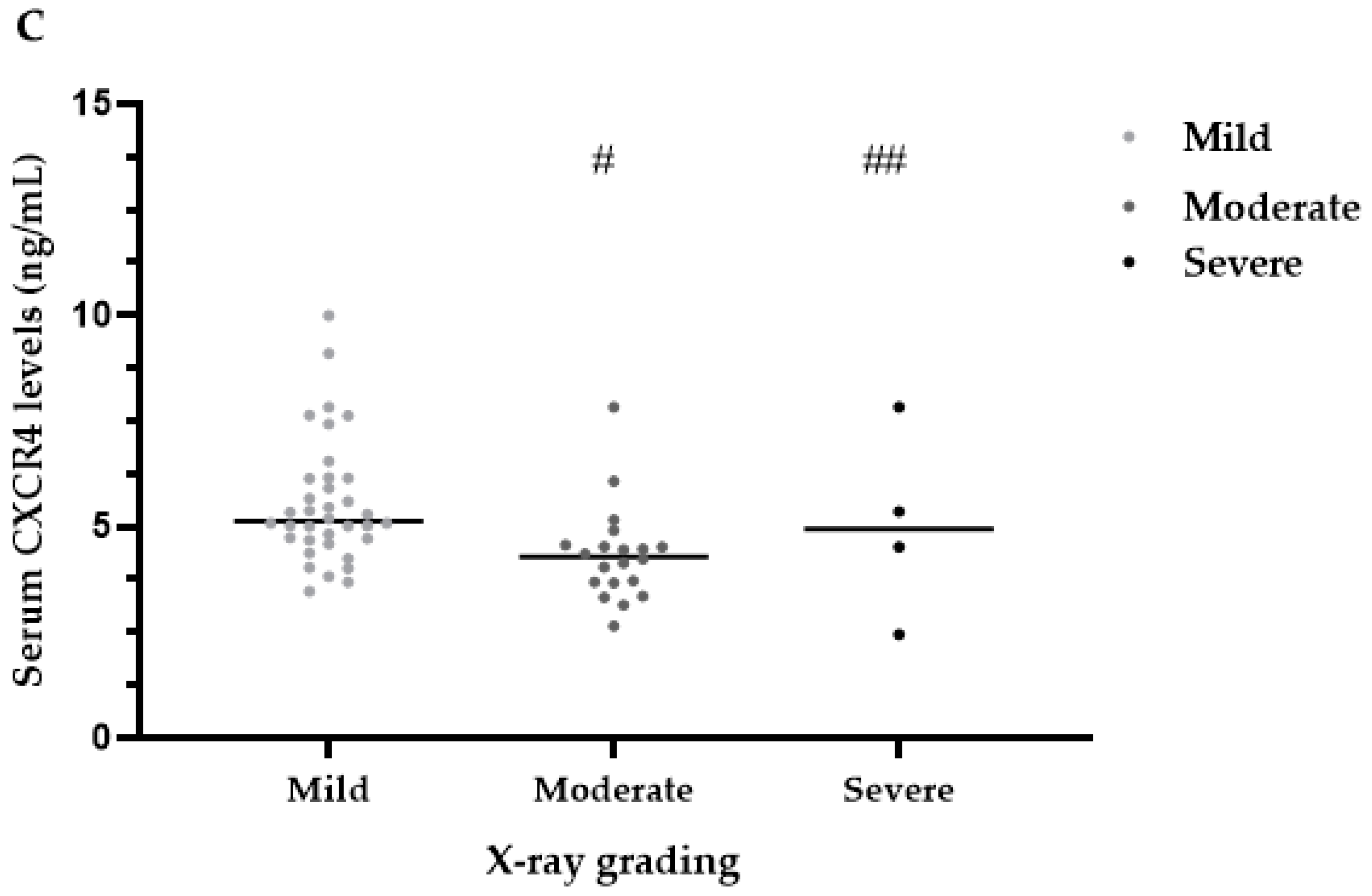
3.4. Serum CXCR4 Levels
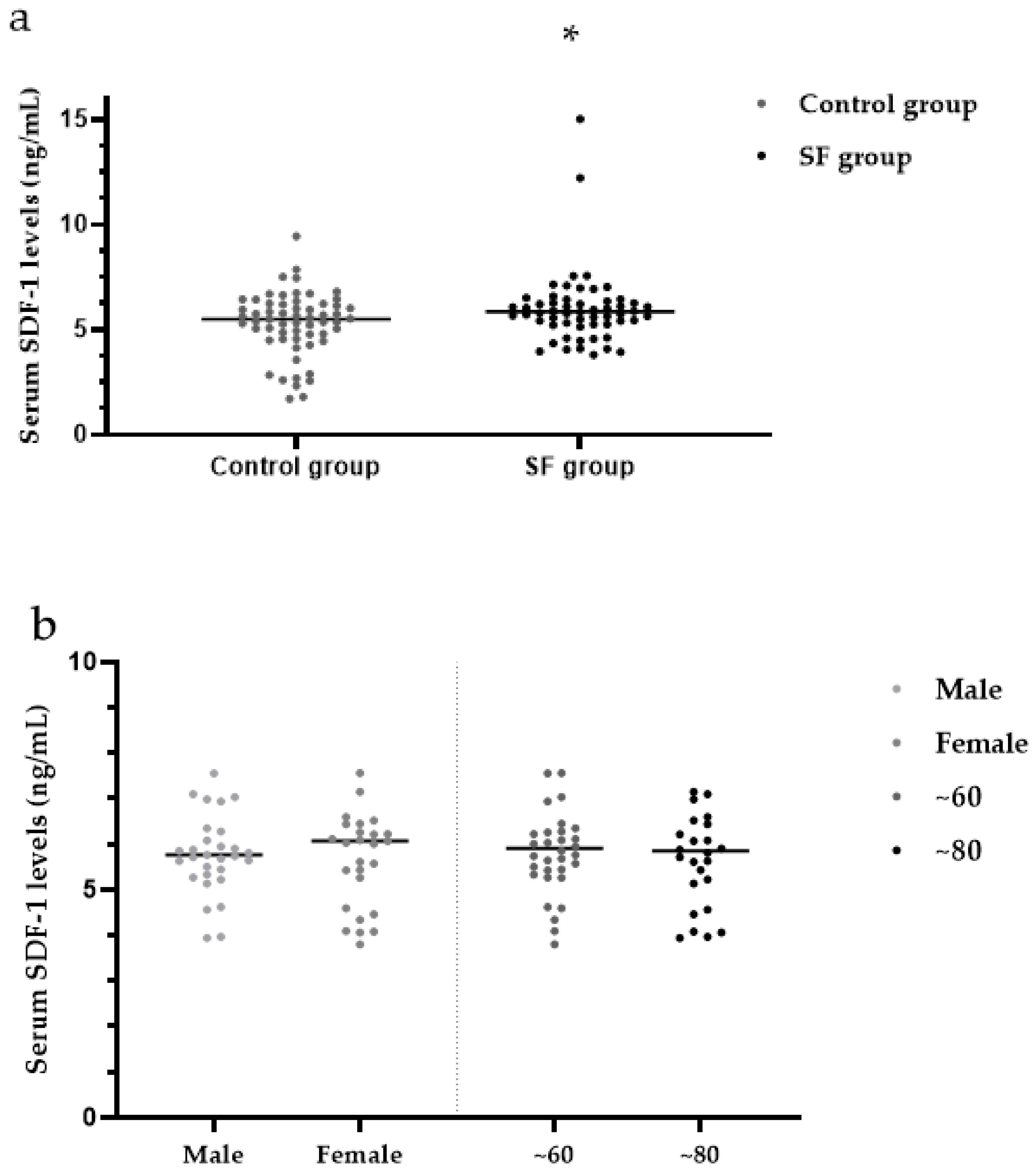
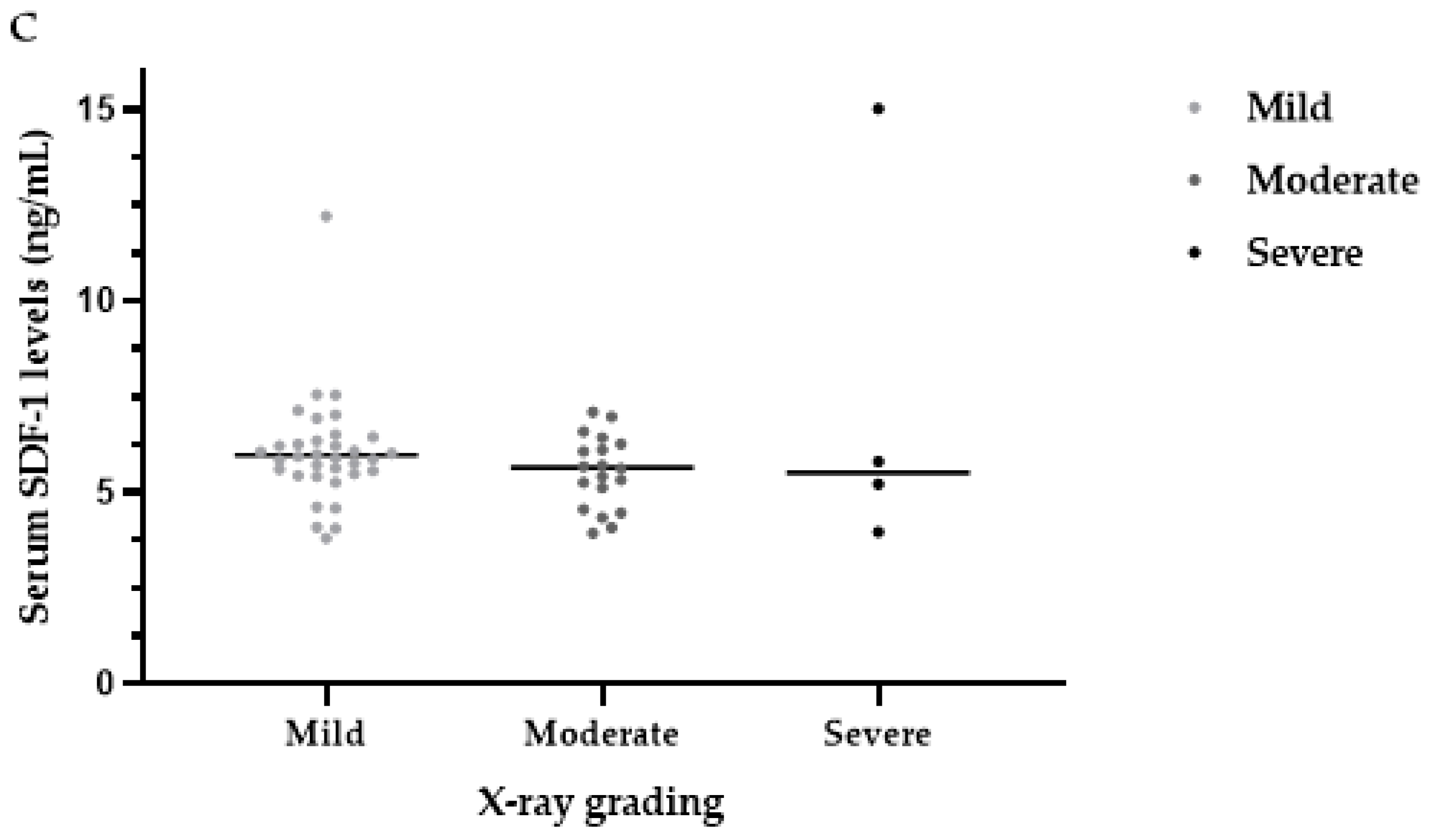
3.5. Serum SDF-1 Levels
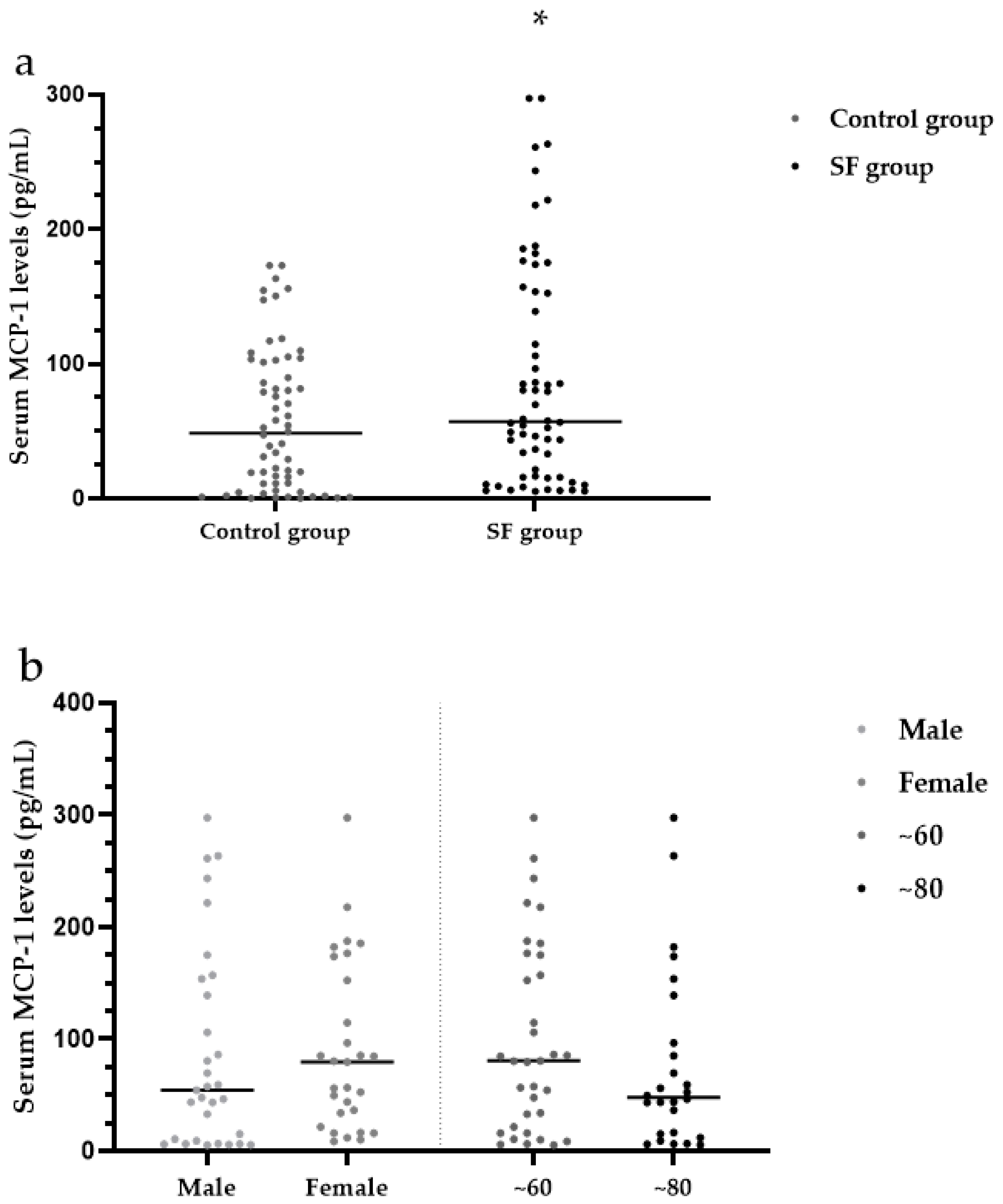
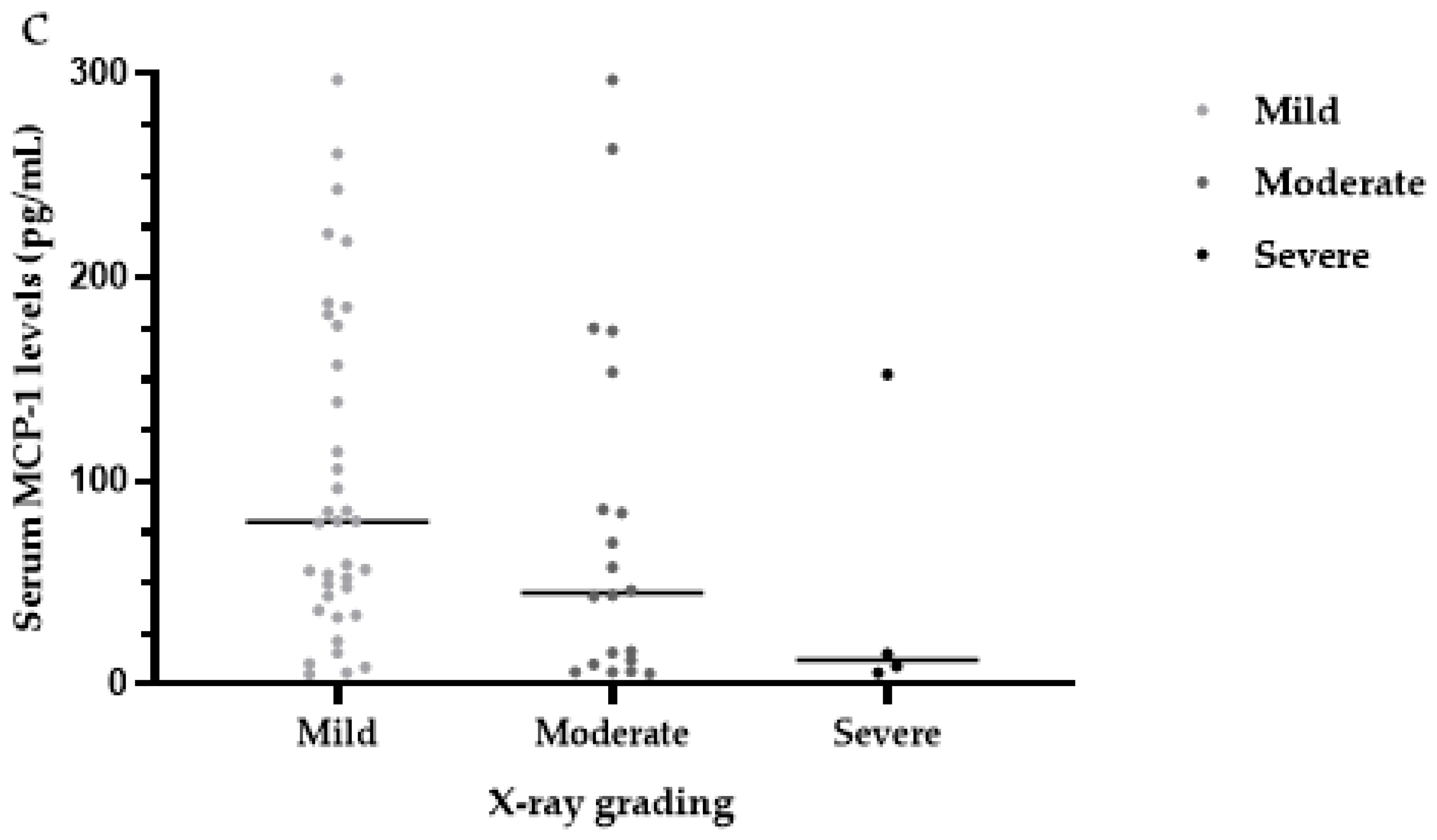
3.6. Serum MCP-1 Levels
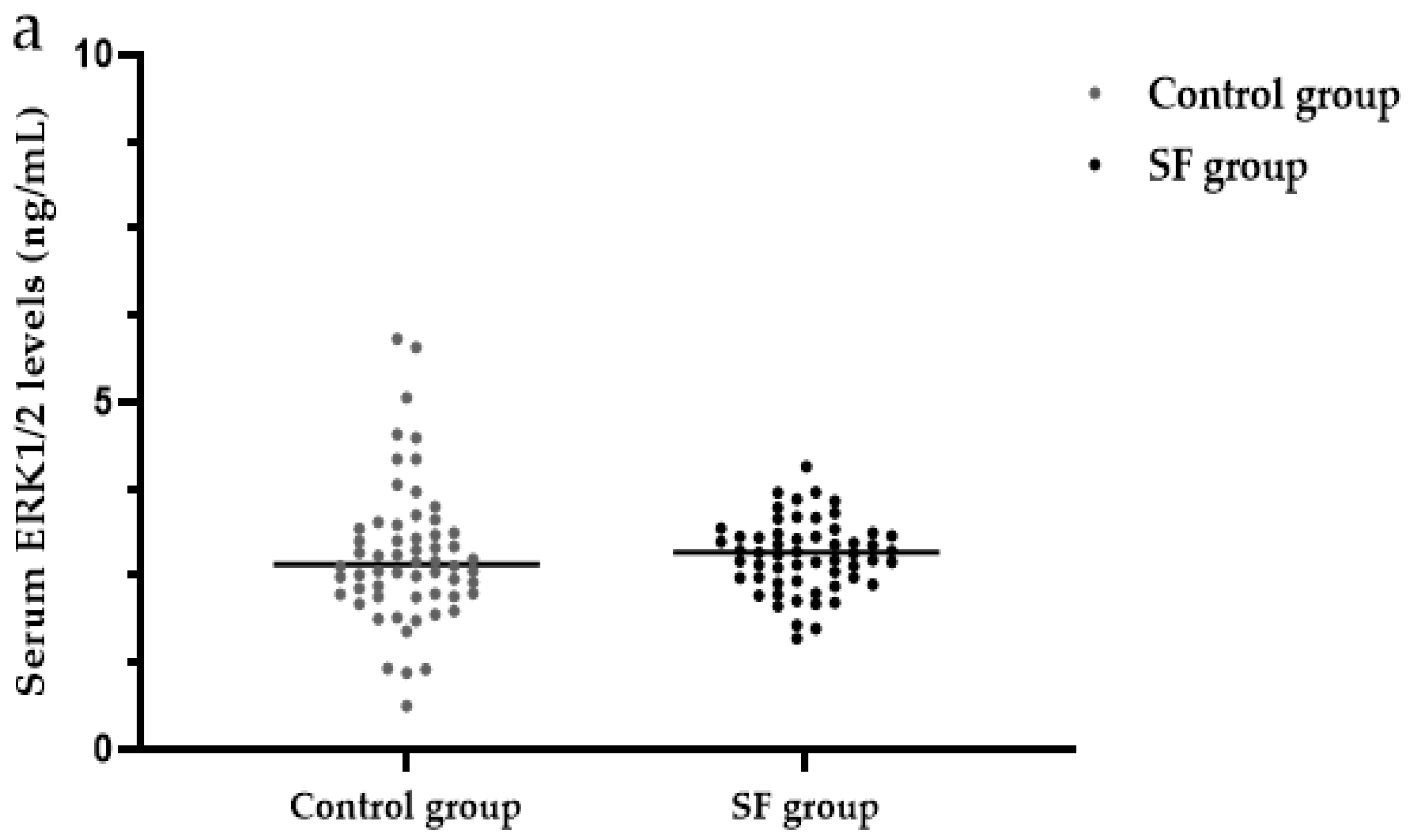
3.7. Serum ERK1/2 Levels
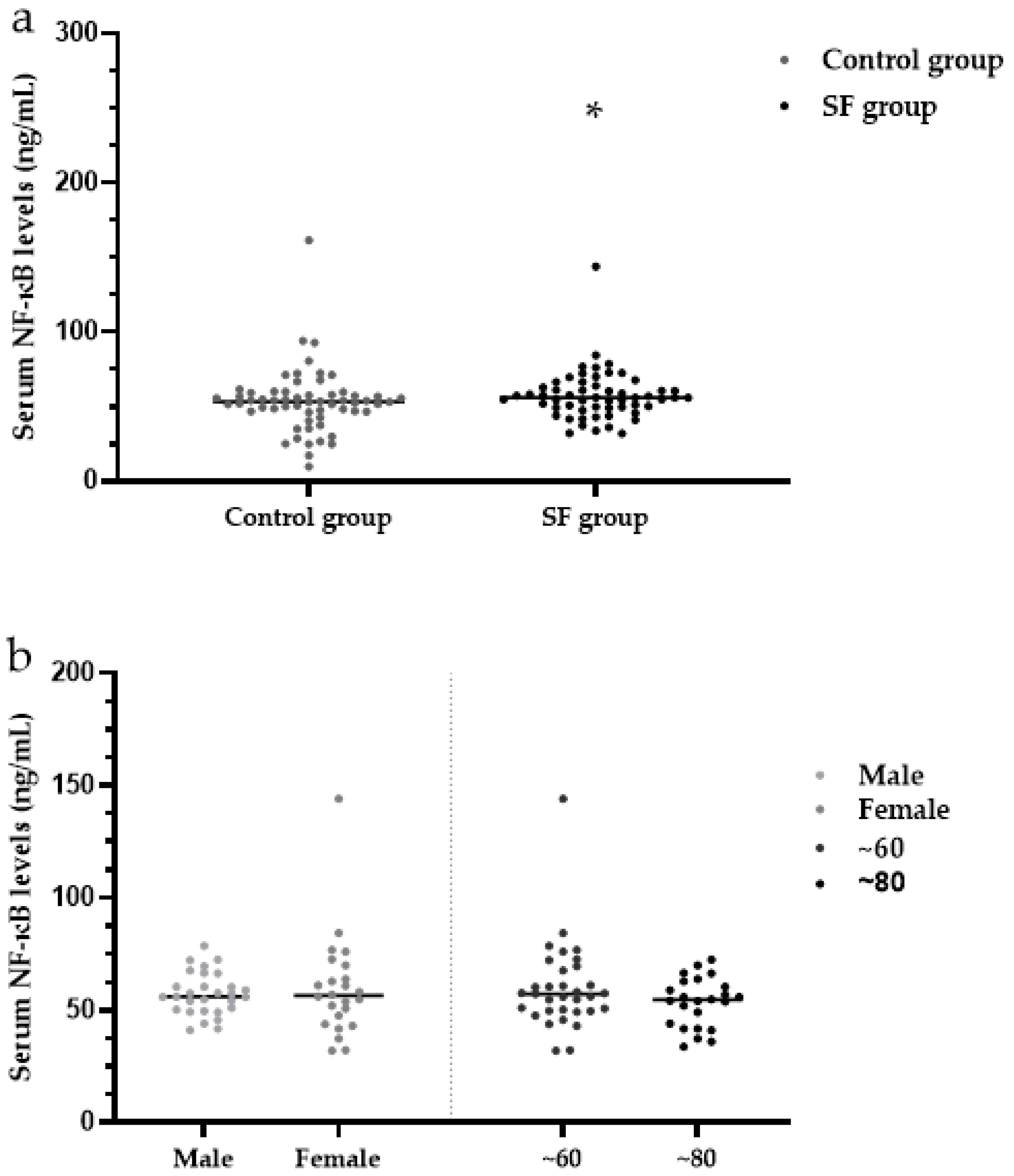
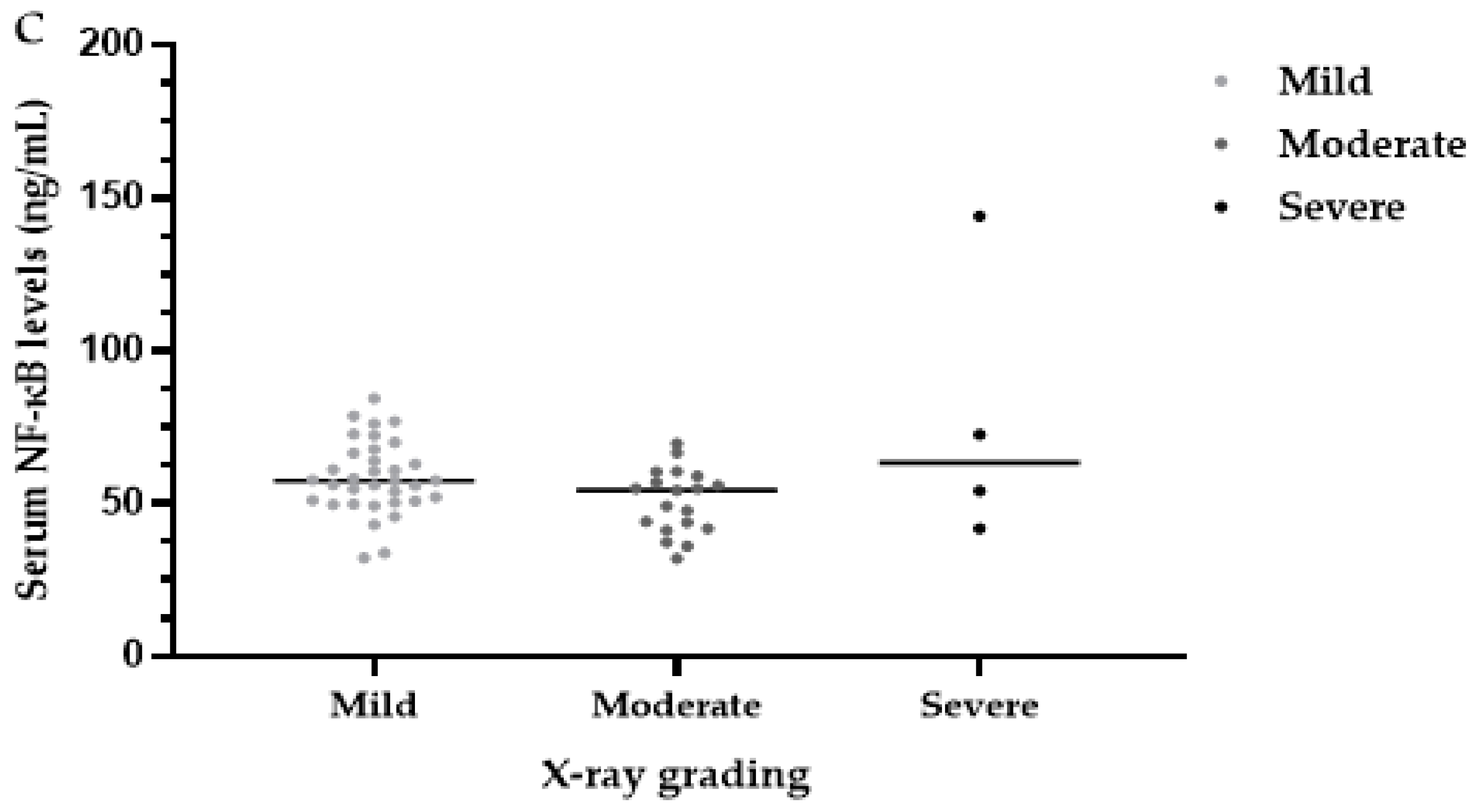
3.8. Serum NF-κB Levels
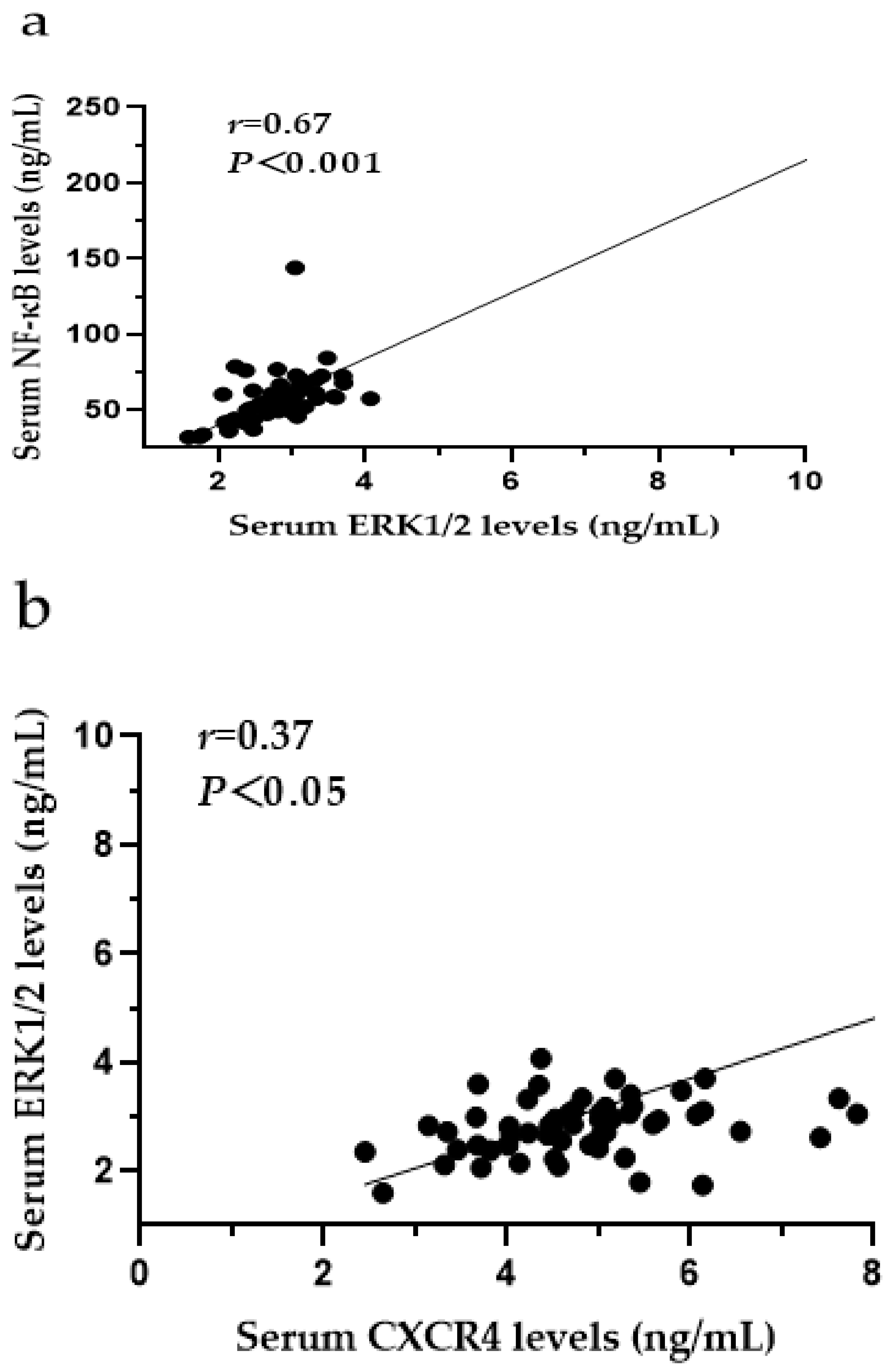
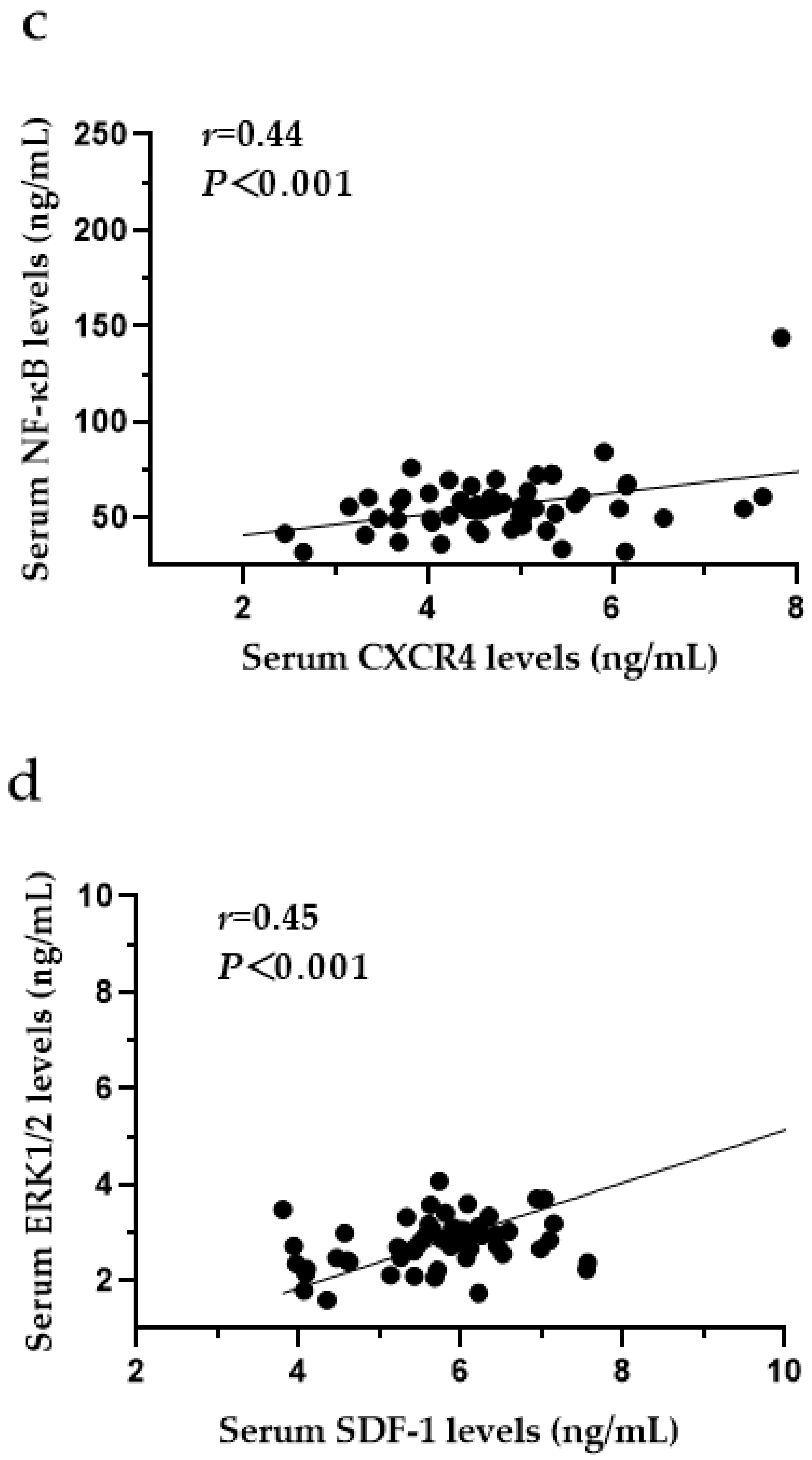
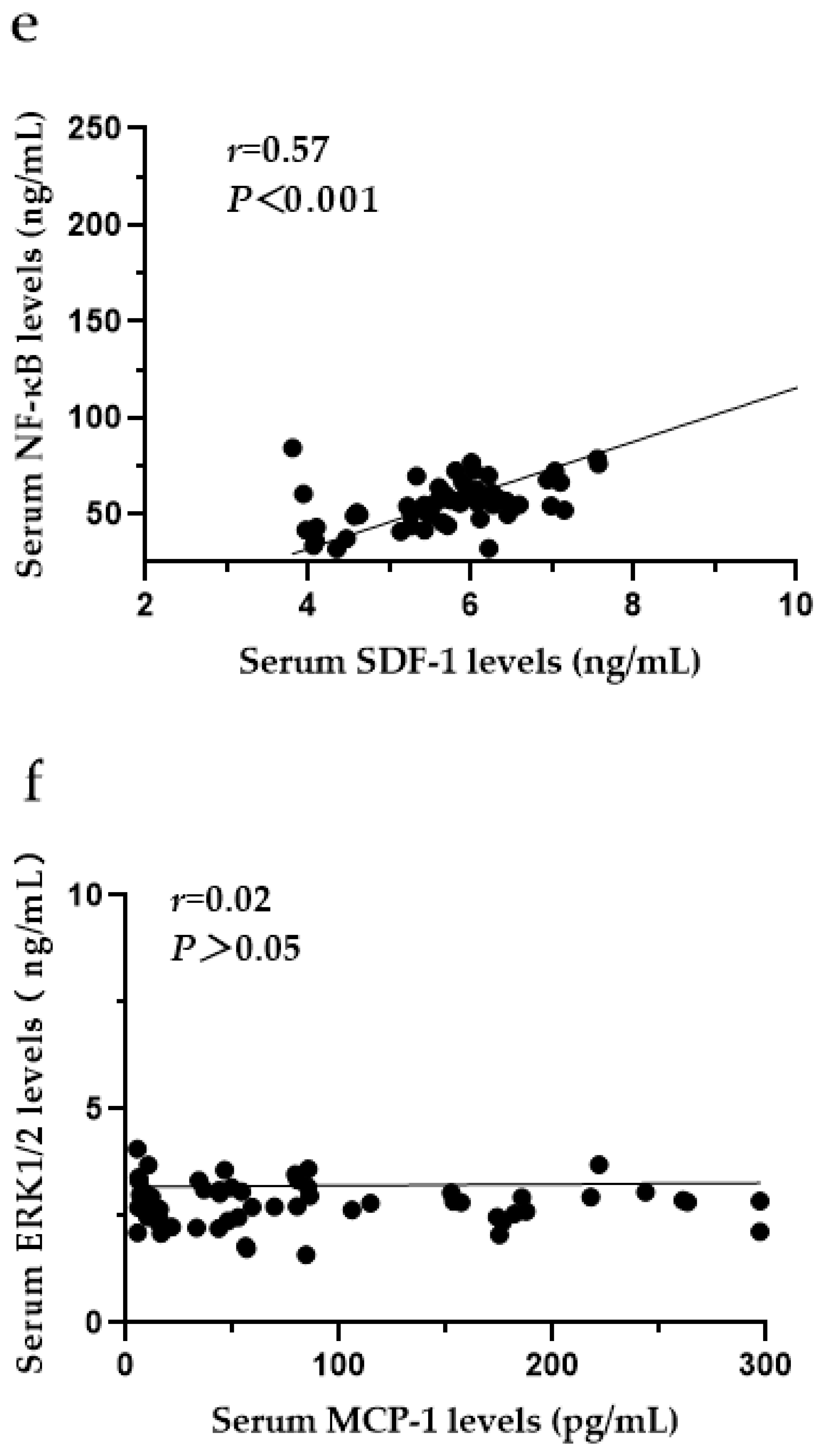
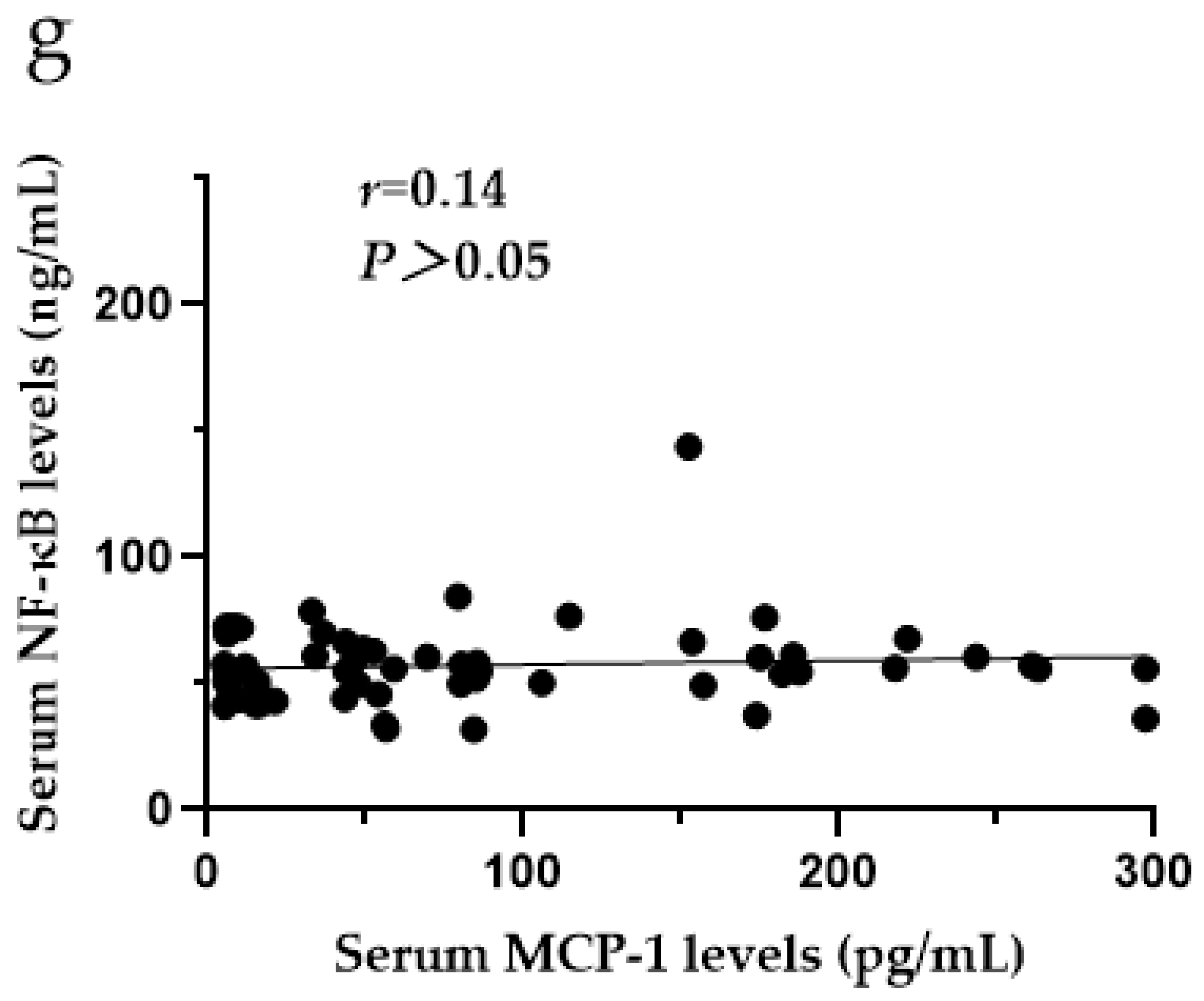
3.9. The Relationships among CXCR4, SDF-1, MCP-1, ERK1/2 and NF-κB in the Serum of SF Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnston, N.R.; Strobel, S.A. Principles of fluoride toxicity and the cellular response: A review. Arch. Toxicol. 2020, 94, 1051–1069. [Google Scholar] [CrossRef] [PubMed]
- Barbier, O.; Arreola-Mendoza, L.; Del Razo, L.M. Molecular mechanisms of fluoride toxicity. Chem. Biol. Interact. 2010, 188, 319–333. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Pei, M.; Luo, K.; Li, L. The State and Trend of Endemic Fluorosis from 1991 to 2012 in China. J. Chongqing Norm. Univ. (Nat. Sci. Ed.) 2016, 33, 142–151. [Google Scholar] [CrossRef]
- Pei, J.; Li, B.; Gao, Y.; Wei, Y.; Zhou, L.; Yao, H.; Wang, J.; Sun, D. Fluoride decreased osteoclastic bone resorption through the inhibition of NFATc1 gene expression. Environ. Toxicol. 2014, 29, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Jiang, N.; Yu, X.; Zhao, Z.; Zhang, X.; Xu, H. The role of TGFbeta receptor 1-smad3 signaling in regulating the osteoclastic mode affected by fluoride. Toxicology 2018, 393, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.F.; Huang, J.Z. Outline of control practice of endemic fluorosis in China. Soc. Sci. Med. 1995, 41, 1191–1195. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Kong, L.; Zhao, H.; Dong, R.; Li, J.; Jia, Z.; Ji, N.; Deng, S.; Sun, Z.; Zhou, J. Thoracic ossification of ligamentum flavum caused by skeletal fluorosis. Eur. Spine J. 2007, 16, 1119–1128. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Pang, S.; Sun, D. The pathogenesis of endemic fluorosis: Research progress in the last 5 years. J. Cell Mol. Med. 2019, 23, 2333–2342. [Google Scholar] [CrossRef]
- Mou, W.; Yan, H.; Zhang, L. The role of SDF-1/CXCR4 and downstream signaling pathways in the course. J. Pract. Med. 2011, 9, 158–160. [Google Scholar] [CrossRef]
- Sun, Y.; Yang, F.; Li, Y.; Lu, S.; Zhu, M.; Qiu, M. Expression of Fas, FasL, and NF-κB in the Process of Osteoclast-like Cell Apoptosis Effected by Sodium Fluoride. J. Chin. Acad. Med. Sci. 2002, 24, 491–494. [Google Scholar]
- Zhang, M.; Wang, A.; Xia, T.; He, P. Effects of fluoride on DNA damage, S-phase cell-cycle arrest and the expression of NF-kappaB in primary cultured rat hippocampal neurons. Toxicol. Lett. 2008, 179, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, W.; Chi, H.S.; Chen, J.; Denbesten, P.K. JNK/c-Jun signaling pathway mediates the fluoride-induced down-regulation of MMP-20 in vitro. Matrix Biol. 2007, 26, 633–641. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Karube, H.; Nishitai, G.; Inageda, K.; Kurosu, H.; Matsuoka, M. NaF activates MAPKs and induces apoptosis in odontoblast-like cells. J. Dent. Res. 2009, 88, 461–465. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Li, Y.; Xiang, Y.; Chen, Y.; Yang, X. The role of SDF-1/CXCR4 and downstream signaling pathways in the course of OA. J. Pract. Med. 2019, 35, 3563–3567. [Google Scholar] [CrossRef]
- Smith, J.T.; Schneider, A.D.; Katchko, K.M.; Yun, C.; Hsu, E.L. Environmental Factors Impacting Bone-Relevant Chemokines. Front. Endocrinol. 2017, 8, 22. [Google Scholar] [CrossRef] [PubMed]
- Gilchrist, A. Chemokines and Bone. Handb. Exp. Pharmacol. 2020, 262, 231–258. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y. The role of C-C motif chemokine ligand 2 in respiratory diseases. Int. J. Pediatr. 2018, 45, 204–207. [Google Scholar] [CrossRef]
- Nagasawa, T. CXCL12/SDF-1 and CXCR4. Front. Immunol. 2015, 6, 301. [Google Scholar] [CrossRef] [PubMed]
- Kucia, M.; Jankowski, K.; Reca, R.; Wysoczynski, M.; Bandura, L.; Allendorf, D.J.; Zhang, J.; Ratajczak, J.; Ratajczak, M.Z. CXCR4-SDF-1 signalling, locomotion, chemotaxis and adhesion. J. Mol. Histol. 2004, 35, 233–245. [Google Scholar] [CrossRef]
- Horuk, R. Chemokine receptors. Cytokine Growth Factor Rev. 2001, 12, 313–335. [Google Scholar] [CrossRef]
- Er, Z.J.; Yin, C.F.; Wang, W.J.; Chen, X.J. Serum CXCL12/SDF-1 level is positively related with lumbar intervertebral disc degeneration and clinical severity. Innate Immun. 2020, 26, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, W.; Bragg, R.; Elmansi, A.M.; McGee-Lawrence, M.E.; Isales, C.M.; Hamrick, M.W.; Hill, W.D.; Fulzele, S. Stromal cell-derived factor-1 (CXCL12) and its role in bone and muscle biology. Cytokine 2019, 123, 154783. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chen, H.; Zhang, D.; Xie, J.; Zhou, X. The role of stromal cell-derived factor 1 on cartilage development and disease. Osteoarthr. Cartil. 2021, 29, 313–322. [Google Scholar] [CrossRef]
- Yu, X.; Huang, Y.; Collin-Osdoby, P.; Osdoby, P. Stromal cell-derived factor-1 (SDF-1) recruits osteoclast precursors by inducing chemotaxis, matrix metalloproteinase-9 (MMP-9) activity, and collagen transmigration. J. Bone Min. Res. 2003, 18, 1404–1418. [Google Scholar] [CrossRef]
- Gschwandtner, M.; Derler, R.; Midwood, K.S. More Than Just Attractive: How CCL2 Influences Myeloid Cell Behavior Beyond Chemotaxis. Front. Immunol. 2019, 10, 2759. [Google Scholar] [CrossRef]
- Brylka, L.J.; Schinke, T. Chemokines in Physiological and Pathological Bone Remodeling. Front. Immunol. 2019, 10, 2182. [Google Scholar] [CrossRef]
- Mao, Z.; Zhou, R.; Zhao, X.; Wang, B. Research Developments of Monocyte Chemoattractant Protein-1 in Inflammatory Reaction. Med. Recapitul. 2013, 19, 964–966. [Google Scholar] [CrossRef]
- Binder, N.B.; Niederreiter, B.; Hoffmann, O.; Stange, R.; Pap, T.; Stulnig, T.M.; Mack, M.; Erben, R.G.; Smolen, J.S.; Redlich, K. Estrogen-dependent and C-C chemokine receptor-2-dependent pathways determine osteoclast behavior in osteoporosis. Nat. Med. 2009, 15, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Sul, O.J.; Ke, K.; Kim, W.K.; Kim, S.H.; Lee, S.C.; Kim, H.J.; Kim, S.Y.; Suh, J.H.; Choi, H.S. Absence of MCP-1 leads to elevated bone mass via impaired actin ring formation. J. Cell Physiol. 2012, 227, 1619–1627. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, J.A.; Partridge, N.C. CCL2/Monocyte Chemoattractant Protein 1 and Parathyroid Hormone Action on Bone. Front. Endocrinol. 2017, 8, 49. [Google Scholar] [CrossRef] [PubMed]
- Shaul, Y.D.; Seger, R. The MEK/ERK cascade: From signaling specificity to diverse functions. Biochim. Biophys. Acta (BBA)-Mol. Cell Res. 2007, 1773, 1213–1226. [Google Scholar] [CrossRef] [PubMed]
- Lu, N.; Malemud, C.J. Extracellular Signal-Regulated Kinase: A Regulator of Cell Growth, Inflammation, Chondrocyte and Bone Cell Receptor-Mediated Gene Expression. Int. J. Mol. Sci. 2019, 20, 3792. [Google Scholar] [CrossRef] [PubMed]
- Zheng, P.; Dong, Z.; Wang, J.; Lou, Y. Thyrocalcitonin regulates the cbfa1mRNA expression of osteoblasts via signal pathway of ERK-MAPK. J. Clin. Med. Pract. 2009, 13, 35–38. [Google Scholar] [CrossRef]
- Kim, G.W.; Han, M.S.; Park, H.R.; Lee, E.J.; Jung, Y.K.; Usmani, S.E.; Ulici, V.; Han, S.W.; Beier, F. CXC chemokine ligand 12a enhances chondrocyte proliferation and maturation during endochondral bone formation. Osteoarthr. Cartil. 2015, 23, 966–974. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Wang, X.; Niu, F.; Chen, M.; Song, N. Expression of stromal cell-derived factor 1, CXCR4 and ERK1/2 in pathologic scar tissue. Chin. J. Aesthetic Med. 2009, 18, 1638–1639. [Google Scholar] [CrossRef]
- Cao, X. Function of NF-κB Signaling Pathway in Bone and Bone Diseases. Sichuan J. Anat. 2015, 23, 30–35. [Google Scholar] [CrossRef]
- Novack, D.V. Role of NF-kappaB in the skeleton. Cell Res. 2011, 21, 169–182. [Google Scholar] [CrossRef]
- Boyce, B.F.; Xing, L.; Franzoso, G.; Siebenlist, U. Required and nonessential functions of nuclear factor-kappa B in bone cells. Bone 1999, 25, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Abu-Amer, Y. NF-kappaB signaling and bone resorption. Osteoporos. Int. 2013, 24, 2377–2386. [Google Scholar] [CrossRef] [PubMed]
- Chen, P. To Investigate the Tea-Based Fluorosis in Qinghai Province. Master’s Thesis, Shanxi Medical University, Taiyuan, China, 2012. [Google Scholar] [CrossRef]
- Chen, T.L. Inhibition of growth and differentiation of osteoprogenitors in mouse bone marrow stromal cell cultures by increased donor age and glucocorticoid treatment. Bone 2004, 35, 83–95. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.W.; Huang, H.X.; Wang, F.; Zhou, Q.L.; Huang, Y.Q.; Qin, R.Z. Elevated plasma CXCL12/SDF-1 levels are linked with disease severity of postmenopausal osteoporosis. Innate Immun. 2020, 26, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, L.; Chen, L.; Li, W.; Li, F.; Chen, Q. Stromal cell-derived factor-1 and its receptor CXCR4 are upregulated expression in degenerated intervertebral discs. Int. J. Med. Sci. 2014, 11, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Bragg, R.; Gilbert, W.; Elmansi, A.M.; Isales, C.M.; Hamrick, M.W.; Hill, W.D.; Fulzele, S. Stromal cell-derived factor-1 as a potential therapeutic target for osteoarthritis and rheumatoid arthritis. Ther. Adv. Chronic. Dis. 2019, 10, 2040622319882531. [Google Scholar] [CrossRef] [PubMed]
- Peng, L.; Zhu, N.; Mao, J.; Huang, L.; Yang, Y.; Zhou, Z.; Wang, L.; Wu, B. Expression Levels of CXCR4 and CXCL12 in Patients with Rheumatoid Arthritis and its Correlation with Disease Activity. Exp. Ther. Med. 2020, 20, 1925–1934. [Google Scholar] [CrossRef] [PubMed]
- Xiang, Y.; Li, Y.; Yang, L.; He, Y.; Jia, D.; Hu, X. miR-142-5p as a CXCR4-Targeted MicroRNA Attenuates SDF-1-Induced Chondrocyte Apoptosis and Cartilage Degradation via Inactivating MAPK Signaling Pathway. Biochem. Res. Int. 2020, 2020, 4508108. [Google Scholar] [CrossRef] [PubMed]
- Raghu, H.; Lepus, C.M.; Wang, Q.; Wong, H.H.; Lingampalli, N.; Oliviero, F.; Punzi, L.; Giori, N.J.; Goodman, S.B.; Chu, C.R.; et al. CCL2/CCR2, but not CCL5/CCR5, mediates monocyte recruitment, inflammation and cartilage destruction in osteoarthritis. Ann. Rheum. Dis. 2017, 76, 914–922. [Google Scholar] [CrossRef] [PubMed]
- Gao, J. Effect of CASR/MAPK Signaling Pathway on the Pathogenesis of Fluorosis. Master’s Thesis, Jilin University, Jilin, China, 2020. [Google Scholar]
- Chen, H.; Shao, X.; Li, L.; Zheng, C.; Xu, X.; Hong, X.; Li, X.; Wu, M. Electroacupuncture serum inhibits TNF-α-mediated chondrocyte inflammation via the Ras-Raf-MEK1/2-ERK1/2 signaling pathway. Mol. Med. Rep. 2017, 16, 5807–5814. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.C.; Wang, C.F.; Han, L.; Cao, G.P.; Shen, Q.R. Chondroprotective Effect of Wufu Decoction on Tumor Necrosis Factor-alpha-Induced Chondrocytes via the Extracellular Signal Regulated Kinase 1/2 Signaling Pathway. Orthop. Surg. 2020, 12, 1319–1326. [Google Scholar] [CrossRef] [PubMed]
- Alhusaini, A.; Faddaa, L.; Ali, H.M.; Hassan, I.; El Orabi, N.F.; Bassiouni, Y. Amelioration of the Protein Expression of Cox2, NFkappaB, and STAT-3 by Some Antioxidants in the Liver of Sodium Fluoride-Intoxicated Rats. Dose Response 2018, 16, 1559325818800153. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L. Research Progress on the Role of CCL2 and Its Signal Pathway in the Pathogenesis of Rheumatoid Arthritis and Periodontitis. Shandong Med. J. 2020, 60, 98–102. [Google Scholar] [CrossRef]




















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SF | Control | Z/χ* Value | p-Value | |
|---|---|---|---|---|
| Age (years) | 60.03 ± 9.67 | 57.42 ± 6.88 | 1.71 | >0.05 |
| Sex (Male/Female) | 31/29 | 28/32 | 3.00 | >0.05 |
| X-ray grade | ||||
| Mild | 36 | |||
| Moderate | 20 | |||
| Severe | 4 |
| Characteristic | SF Group N (%) | X-ray Grade | Χ* | p-Value | ||
|---|---|---|---|---|---|---|
| Mild | Moderate | Severe | ||||
| Sex | ||||||
| Male | 31 (51.67) | 16 | 12 | 3 | 2.18 | > 0.05 |
| Female | 29 (48.33) | 20 | 8 | 1 | ||
| Age (years) | ||||||
| ~60 | 34 (56.67) | 26 | 7 | 1 | 9.01 | < 0.05 |
| ~80 | 26 (43.33) | 10 | 13 | 3 | ||
| Group | N | CXCR4 (ng/mL) | SDF-1 (ng/mL) | MCP-1 (pg/mL) | ERK1/2 (ng/mL) | NF-κB (ng/mL) |
|---|---|---|---|---|---|---|
| Control group | 60 | 4.22 (3.03, 4.76) | 5.51 (4.62, 6.22) | 48.45 (11.07, 102.33) | 2.67 (2.24, 3.22) | 53.25 (46.68, 58.90) |
| SF group | 60 | 4.86 (4.16, 5.64) ** | 5.86 (5.28, 6.45) * | 57.11 (15.97, 153.30) * | 2.84 (2.47, 3.16) ** | 56.08 (49.29, 66.53) * |
| Z value | 3.74 | 2.12 | 1.99 | 1.07 | 2.05 | |
| p-value | <0.001 | <0.05 | <0.05 | >0.05 | <0.05 |
| Characteristic | SF Group N (%) | CXCR4 (ng/mL) | SDF-1 (ng/mL) | MCP-1 (pg/mL) | NF-κB (ng/mL) |
|---|---|---|---|---|---|
| Sex | |||||
| Male | 31 (51.67) | 4.52 (4.03, 5.18) | 5.77 (5.33, 6.35) | 54.27 (9.03, 153.60) | 57.25 (50.30, 66.55) |
| Female | 29 (48.33) | 5.08 (4.33, 6.10) | 6.07 (4.93, 6.49) | 79.34 (27.73, 163.15) | 54.85 (43.47, 66.98) |
| Age (years) | |||||
| ~60 | 34 (56.67) | 5.02 (4.34, 6.14) | 5.90 (5.40, 6.38) | 80.39 (20.01, 175.48) | 57.38 (49.81, 70.30) |
| ~80 | 26 (43.33) | 4.52 (3.93, 5.36) | 5.84 (4.99, 6.54) | 47.84 (14.29, 107.12) | 55.37 (43.67, 64.54) |
| X-ray grade | |||||
| Mild | 36 (60.00) | 5.13 (4.69, 6.14) | 5.98 (5.52, 6.50) | 79.82 (38.35, 171.71) | 57.58 (50.88, 69.48) |
| Moderate | 20 (33.33) | 4.29 (3.67, 4.55) | 5.66 (4.71, 6.40) | 45.11 (10.49, 136.71) | 54.55 (42.28, 59.95) |
| Severe | 4 (6.67) | 4.93 (2.96, 7.21) | 5.52 (4.28, 12.72) | 12.06 (6.66, 118.07) | 63.30 (44.89, 126.09) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Y.; Pu, G.; Li, Y.; Jiang, H.; Zhang, Q.; Chen, P.; Lu, Q.; Wang, M.; Yang, R. Serum Levels of CXCR4, SDF-1, MCP-1, NF-κB and ERK1/2 in Patients with Skeletal Fluorosis. Int. J. Environ. Res. Public Health 2022, 19, 16555. https://doi.org/10.3390/ijerph192416555
Zhao Y, Pu G, Li Y, Jiang H, Zhang Q, Chen P, Lu Q, Wang M, Yang R. Serum Levels of CXCR4, SDF-1, MCP-1, NF-κB and ERK1/2 in Patients with Skeletal Fluorosis. International Journal of Environmental Research and Public Health. 2022; 19(24):16555. https://doi.org/10.3390/ijerph192416555
Chicago/Turabian StyleZhao, Yaqian, Guanglan Pu, Yanan Li, Hong Jiang, Qiang Zhang, Ping Chen, Qing Lu, Mingjun Wang, and Rui Yang. 2022. "Serum Levels of CXCR4, SDF-1, MCP-1, NF-κB and ERK1/2 in Patients with Skeletal Fluorosis" International Journal of Environmental Research and Public Health 19, no. 24: 16555. https://doi.org/10.3390/ijerph192416555
APA StyleZhao, Y., Pu, G., Li, Y., Jiang, H., Zhang, Q., Chen, P., Lu, Q., Wang, M., & Yang, R. (2022). Serum Levels of CXCR4, SDF-1, MCP-1, NF-κB and ERK1/2 in Patients with Skeletal Fluorosis. International Journal of Environmental Research and Public Health, 19(24), 16555. https://doi.org/10.3390/ijerph192416555