
Effect of Fermented Sarco Oyster (Crassostrea gigas) Extract on Muscle Strength Enhancement in Postmenopausal Females: A Randomized, Double-Blind, Placebo-Controlled Trial

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Participant Eligibility
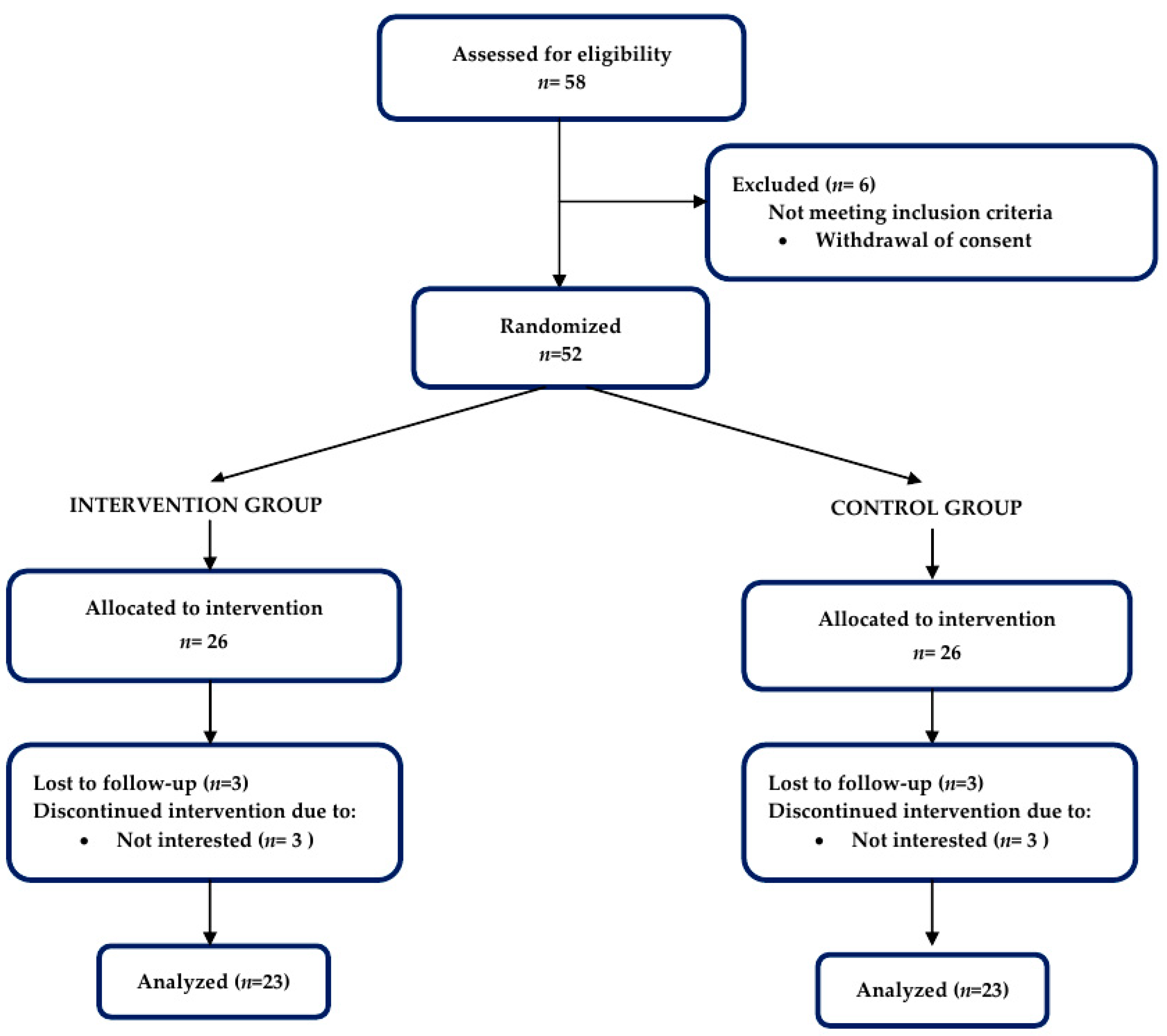
2.3. Randomization
2.4. Intervention
2.5. Procedures
2.5.1. Efficacy Measurement
2.5.2. Biomarker Measurement
2.5.3. Body Composition Analysis
2.5.4. Dietary Intake and Physical Activity Assessment
2.6. Sample Size Calculation
2.7. Safety Assement
2.8. Statistical Analysis
3. Results
3.1. Baseline Demogrpahic Characteristics
3.2. Primary Outcome
3.3. Secondary Outcome
3.4. Safety and Adverse Event
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dufour, A.B.; Hannan, M.T.; Murabito, J.; Kiel, D.; McLean, R.R. Sarcopenia Definitions Considering Body Size and Fat Mass Are Associated with Mobility Limitations: The Framingham Study. J. Gerontol. Ser. A 2012, 68, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Xue, Q.L.; Walston, J.D.; Fried, L.P.; Beamer, B.A. Prediction of risk of falling, physical disability, and frailty by rate of decline in grip strength: The women’s health and aging study. Arch. Intern. Med. 2011, 171, 1119–1121. [Google Scholar] [CrossRef] [PubMed]
- Giles, J.T.; Ling, S.M.; Ferrucci, L.; Bartlett, S.; Andersen, R.E.; Towns, M.; Muller, D.; Fontaine, K.R.; Bathon, J.M. Abnormal body composition phenotypes in older rheumatoid arthritis patients: Association with disease characteristics and pharmacotherapies. Arthritis Care Res. 2008, 59, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Sherlock, M.; Toogood, A.A. Aging and the growth hormone/insulin like growth factor-I axis. Pituitary 2007, 10, 189–203. [Google Scholar] [CrossRef]
- Schulz, K.F.; Altman, D.G.; Moher, D.; CONSORT Group. CONSORT 2010 statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed]
- Powers, M. GABA Supplementation and Growth Hormone Response. Med. Sport. Sci. 2012, 59, 36–46. [Google Scholar] [CrossRef]
- Athapaththu, A.M.G.K.; Molagoda, I.M.N.; Jayasooriya, R.G.P.T.; Choi, Y.H.; Jeon, Y.-J.; Park, J.-H.; Lee, B.-J.; Kim, G.-Y. Gamma-Aminobutyric Acid (GABA) Promotes Growth in Zebrafish Larvae by Inducing IGF-1 Expression via GABAA and GABAB Receptors. Int. J. Mol. Sci. 2021, 22, 11254. [Google Scholar] [CrossRef] [PubMed]
- Marini, M.; Sarchielli, E.; Brogi, L.; Lazzeri, R.; Salerno, R.; Sgambati, E.; Monaci, M. Role of adapted physical activity to prevent the adverse effects of the sarcopenia. A pilot study. Ital. J. Anat. Embryol. = Arch. Ital. Di Anat. Ed Embriol. 2008, 113, 217–225. [Google Scholar]
- Lee, Y.L.; Lee, S.Y. Effect of fermented oyster (Crassostrea gigas) extracts and regular walking on muscle strength and mass in older adults with relatively low muscle mass: A randomized controlled trial. Front. Nutr. 2022, 9, 935395. [Google Scholar] [CrossRef] [PubMed]
- Bang, J.S.; Choung, S.-Y. Inhibitory effect of oyster hydrolysate on wrinkle formation against UVB irradiation in human dermal fibroblast via MAPK/AP-1 and TGFβ/Smad pathway. J. Photochem. Photobiol. B: Biol. 2020, 209, 111946. [Google Scholar] [CrossRef] [PubMed]
- Molagoda, I.M.N.; Athapaththu, A.M.G.K.; Park, E.K.; Choi, Y.H.; Jeon, Y.-J.; Kim, G.-Y. Fermented Oyster (Crassostrea gigas) Extract Cures and Prevents Prednisolone-Induced Bone Resorption by Activating Osteoblast Differentiation. Foods 2022, 11, 678. [Google Scholar] [CrossRef] [PubMed]
- Jeong, A.; Park, B.-C.; Kim, H.-Y.; Choi, J.-Y.; Cheon, J.; Park, J.-H.; Lee, B.-J.; Kim, K.; Jeong, A.; Park, B.-C.; et al. Efficacy and safety of fermented oyster extract for height of children with short stature: A randomized placebo-controlled trial. Integr. Med. Res. 2021, 10, 100691. [Google Scholar] [CrossRef] [PubMed]
- Reid, S.N.S.; Park, J.-H.; Kim, Y.; Kwak, Y.S.; Jeon, B.H. In Vitro and In Vivo Effects of Fermented Oyster-Derived Lactate on Exercise Endurance Indicators in Mice. Int. J. Environ. Res. Public Health 2020, 17, 8811. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.; Choi, C.H.; Lee, B.-J.; Park, J.-H.; Son, K.-H.; Byun, K. Fermented Oyster Extract Attenuated Dexamethasone-Induced Muscle Atrophy by Decreasing Oxidative Stress. Molecules 2021, 26, 7128. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Jeon, B.H.; Kim, D.S.; Lee, B.J.; Her, J.S. Effects of Fermented Oyster Extract Supplementation on Body Composition, Muscular Strengths and Blood Muscle Growth Factors in Elderly Women. J. Mar. Biosci. Biotechnol. 2021, 13, 76–85. [Google Scholar]
- Rabinowitz, J.D.; Enerbäck, S. Lactate: The ugly duckling of energy metabolism. Nat. Metab. 2020, 2, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-H.; Ahn, J.; Ock, M.; Shin, S.; Park, J.; Luo, N.; Jo, M.-W. The EQ-5D-5L valuation study in Korea. Qual. Life Res. 2016, 25, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Chun, M.Y. Validity and Reliability of Korean Version of International Physical Activity Questionnaire Short Form in the Elderly. Korean J. Fam. Med. 2012, 33, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyzes using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.J.; Sabir, S.; Sharma, S. GABA Receptor. In StatPearls; StatPearls Publishing: Tampa, FL, USA, 2022. [Google Scholar]
- Harnedy, P.A.; FitzGerald, R.J. Bioactive peptides from marine processing waste and shellfish: A review. J. Funct. Foods 2012, 4, 6–24. [Google Scholar] [CrossRef]


{kind=link}
| FSO-Experiment | Placebo-Control | |
|---|---|---|
| Common Name | Fermented Sarco Oyster extract | Dextrin |
| Ingredients and Contents | Fermented Sarco Oyster extract 1000 mg/day | Dextrin 1000 mg/day |
| Type | 250 mg Capsule | Same as left |
| Administration Method | Take 4 capsules once a day after a meal | Same as left |
| Packing Unit | 196 capsules in 1 bottle | Same as left |
| Storage Method | Room temperature storage | Same as left |
| Expiration Period | 2 years | Same as left |
| Variables | Intention-to-Treat Population | Per-Protocol Population | ||||
|---|---|---|---|---|---|---|
| CG (n = 26) | EG (n = 26) | p | CG (n = 23) | EG (n = 23) | p | |
| Age (years) | 73.8 | 72.3 | 0.295 | 73.6 | 72.1 | 0.247 |
| Weight (kg) | 58.3 | 57.9 | 0.854 | 58.4 | 58.0 | 0.838 |
| Height (cm) | 153.5 | 153.4 | 0.949 | 153.5 | 153.6 | 0.930 |
| Variable | Observed Value | Change from the Baseline | ||||||
|---|---|---|---|---|---|---|---|---|
| CG (n = 23) | EG (n = 23) | p ** | CG (n = 23) | p * | EG (n = 23) | p * | p ** | |
| 60°/s knee extension peak TQ (R), Nm | 0.736 | 6.33 ± 11.10 | 0.015 | 0.037 | ||||
| Visit 2 | 53.45 ± 12.13 | 54.83 ± 12.01 | 0.628 | −1.41 ± 10.38 | ||||
| Visit 4 | 52.05 ± 14.29 | 61.17 ± 15.23 | 0.056 | |||||
| 60°/s knee extension peak TQ (L), Nm | 0.516 | −3.74 ± 12.66 | 0.171 | 0.734 | ||||
| Visit 2 | 57.17 ± 17.03 | 62.00 ± 14.80 | 0.310 | −2.26 ± 16.42 | ||||
| Visit 4 | 54.91 ± 12.99 | 58.26 ± 16.88 | 0.455 | |||||
| 60°/s knee flexion peak TQ (R), Nm | 0.096 | 1.50 ± 9.87 | 0.506 | 0.477 | ||||
| Visit 2 | 28.23 ± 9.44 | 32.50 ± 9.29 | 0.512 | 3.63 ± 9.46 | ||||
| Visit 4 | 31.86 ± 11.89 | 34.00 ± 13.66 | 0.956 | |||||
| 60°/s knee flexion peak TQ (L), Nm | 0.013 | −3.74 ± 8.23 | 0.007 | 0.824 | ||||
| Visit 2 | 31.8 ± 12.4 | 32.3 ± 13.5 | 0.892 | −4.26 ± 7.59 | ||||
| Visit 4 | 27.6 ± 10.7 | 27.9 ± 12.3 | 0.919 | |||||
| Variable | Observed Value | Change from the Baseline | ||||||
|---|---|---|---|---|---|---|---|---|
| CG (n = 26) | EG (n = 26) | p ** | CG (n = 26) | p * | EG (n = 26) | p * | p ** | |
| 60°/s knee extension peak TQ (R), Nm | 0.985 | 5.77 ± 10.58 | 0.010 | 0.048 | ||||
| Visit 2 | 52.88 ± 12.15 | 56.27 ± 12.13 | 0.320 | −0.04 ± 10.13 | ||||
| Visit 4 | 52.85 ± 13.66 | 62.04 ± 14.35 | 0.023 | |||||
| 60°/s knee extension peak TQ (L), Nm | 0.368 | −4.19 ± 11.98 | 0.087 | 0.625 | ||||
| Visit 2 | 57.58 ± 16.48 | 62.27 ± 14.89 | 0.287 | −2.31 ± 15.42 | ||||
| Visit 4 | 55.27 ± 12.70 | 58.08 ± 16.84 | 0.500 | |||||
| 60°/s knee flexion peak TQ (R), Nm | 0.118 | 1.50 ± 9.33 | 0.607 | 0.567 | ||||
| Visit 2 | 28.46 ± 9.24 | 31.00 ± 9.90 | 0.344 | 2.99 ± 9.43 | ||||
| Visit 4 | 31.46 ± 11.86 | 32.50 ± 13.29 | 0.768 | |||||
| 60°/s knee flexion peak TQ (L), Nm | 0.090 | −0.38 ± 5.32 | 0.230 | 0.203 | ||||
| Visit 2 | 29.73 ± 13.08 | 31.31 ± 13.29 | 0.668 | −2.88 ± 8.33 | ||||
| Visit 4 | 26.85 ± 10.34 | 10.31 ± 12.87 | 0.290 | |||||
| Variable | Observed Value | Change from the Baseline | ||||||
|---|---|---|---|---|---|---|---|---|
| CG (n = 23) | EG (n = 23) | p ** | CG (n = 23) | p * | EG (n = 23) | p * | p ** | |
| Grip Force (R), Nm | ||||||||
| visit 2 | 20.26 ± 2.46 | 19.91 ± 2.93 | 0.667 | 1.30 ± 2.07 | 0.006 | 2.70 ± 1.47 | 0.000 | 0.011 |
| visit 4 | 21.56 ± 3.56 | 22.61 ± 3.46 | 0.315 | |||||
| Grip Force (L), Nm | ||||||||
| visit 2 | 19.46 ± 2.49 | 19.34 ± 3.65 | 0.901 | 1.48 ± 2.31 | 0.006 | 3.00 ± 2.49 | 0.000 | 0.036 |
| visit 4 | 20.94 ± 3.09 | 22.35 ± 3.36 | 0.146 | |||||
| Total Body Fat, % | ||||||||
| visit 2 | 37.67 ± 4.56 | 35.40 ± 6.54 | 0.177 | 0.70 ± 1.61 | 0.051 | 0.87 ± 1.13 | 0.001 | 0.674 |
| visit 4 | 38.37 ± 4.62 | 36.27 ± 6.29 | 0.202 | |||||
| Visceral Fat Area, cm2 | ||||||||
| visit 2 | 118.4 ± 28.4 | 106.7 ± 39.8 | 0.260 | 9.77 ± 16.39 | 0.009 | 8.93 ± 7.96 | 0.000 | 0.827 |
| visit 4 | 128.2 ± 25.9 | 115.7 ± 41.3 | 0.226 | |||||
| ASM/height2 | ||||||||
| visit 2 | 118.4 ± 28.4 | 106.7 ± 39.8 | 0.260 | −0.01 ± 0.11 | 0.695 | −0.01 ± 0.13 | 0.592 | 0.882 |
| visit 4 | 128.2 ± 25.9 | 115.7 ± 41.3 | 0.226 | |||||
| ASM/weight x100 | ||||||||
| visit 2 | 10.45 ± 0.75 | 10.84 ± 1.05 | 0.152 | −0.17 ± 0.46 | 0.094 | −0.11 ± 6.62 | 0.388 | 0.729 |
| visit 4 | 10.28 ± 0.64 | 10.73 ± 0.92 | 0.061 | |||||
| IGF-1 (ng/mL) | ||||||||
| visit 2 | 104.04 ± 29.59 | 109.31 ± 45.91 | 0.646 | 7.13 ± 25.18 | 0.188 | 12.91 ± 23.36 | 0.015 | 0.424 |
| visit 4 | 111.17 ± 26.67 | 122.22 ± 46.43 | 0.329 | |||||
| hsCRP | ||||||||
| visit 2 | 0.15 ± 0.25 | 0.16 ± 0.36 | 0.924 | −0.032 ± 0.167 | 0.371 | 0.05 ± 0.343 | 0.369 | 0.228 |
| visit 4 | 0.12 ± 0.11 | 0.22 ± 0.69 | 0.473 | |||||
| EQ-5D-3L | ||||||||
| visit 2 | 0.822 ± 0.186 | 0.798 ± 0.178 | 0.663 | 0.049 ± 0.156 | 0.144 | 0.061 ± 0.124 | 0.027 * | 0.775 |
| visit 4 | 0.871 ± 0.173 | 0.859 ± 0.157 | 0.812 | |||||
| Variable | Observed Value | Change from the Baseline | ||||||
|---|---|---|---|---|---|---|---|---|
| CG (n = 26) | EG (n = 26) | p ** | CG (n = 26) | p * | EG (n = 26) | p * | p ** | |
| Grip Force (R), Nm | ||||||||
| visit 2 | 20.59 ± 2.83 | 19.97 ± 2.80 | 0.439 | 0.79 ± 2.94 | 0.192 | 2.58 ± 1.44 | 0.000 | 0.010 |
| visit 4 | 21.38 ± 3.47 | 22.55 ± 3.28 | 0.221 | |||||
| Grip Force (L), Nm | ||||||||
| visit 2 | 19.51 ± 2.79 | 19.34 ± 3.71 | 0853 | 1.15 ± 2.87 | 0.057 | 2.85 ± 2.39 | 0.000 | 0.025 |
| visit 4 | 20.66 ± 3.12 | 22.19 ± 3.62 | 0.112 | |||||
| Total Body Fat, % | ||||||||
| visit 2 | 37.63 ± 4.63 | 35.05 ± 6.51 | 0.066 | 0.66 ± 1.53 | 0.037 | 0.83 ± 1.09 | 0.001 | 0.674 |
| visit 4 | 38.29 ± 4.65 | 35.88 ± 6.37 | 0.074 | |||||
| Visceral Fat Area, cm2 | ||||||||
| visit 2 | 121.58 ± 30.87 | 107.59 ± 39.33 | 0.160 | 9.54 ± 15.84 | 0.008 | 9.68 ± 7.78 | 0.000 | 0.968 |
| visit 4 | 131.30 ± 28.53 | 117.27 ± 40.96 | 0163 | |||||
| ASM/height2 | ||||||||
| visit 2 | 2.59 ± 0.26 | 2.65 ± 0.24 | 0.428 | −0.02 ± 0.11 | 0.465 | −0.01 ± 0.12 | 0.696 | 0.839 |
| visit 4 | 2.58 ± 0.26 | 2.64 ± 0.22 | 0.357 | |||||
| ASM/weight x100 | ||||||||
| visit 2 | 10.40 ± 0.74 | 10.83 ± 1.03 | 0.085 | 0.18 ± 0.46 | 0.053 | −0.10 ± 0.53 | 0.379 | 0.580 |
| visit 4 | 10.22 ± 0.66 | 10.73 ± 0.91 | 0.023 | |||||
| IGF-1 (ng/mL) | ||||||||
| visit 2 | 105.75 ± 30.12 | 109.54 ± 44.92 | 0.733 | 7.03 ± 24.64 | 0.176 | 11.80 ± 22.77 | 0.013 | 0.422 |
| visit 4 | 112.77 ± 27.23 | 122.13 ± 45.41 | 0.391 | |||||
| hsCRP | ||||||||
| visit 2 | 0.15 ± 0.25 | 0.16 ± 0.35 | 0.830 | −0.03 ± 0.16 | 0.371 | 0.05 ± 0.33 | 0.440 | 0.276 |
| visit 4 | 0.12 ± 0.11 | 0.22 ± 0.68 | 0.463 | |||||
| EQ-5D-3L | ||||||||
| visit 2 | 0.827 ± 0.187 | 0.783 ± 0.205 | 0.426 | 0.041 ± 0.148 | 0.169 | 0.066 ± 0.128 | 0.014 * | 0.524 |
| visit 4 | 0.868 ± 0.179 | 0.849 ± 0.164 | 0.688 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rheu, K.-M.; Lee, B.-J.; Son, W.-H.; Kim, D.-S.; Park, H.-T.; Ha, M.-S.; Gong, B.-H.; Jeon, B.-H. Effect of Fermented Sarco Oyster (Crassostrea gigas) Extract on Muscle Strength Enhancement in Postmenopausal Females: A Randomized, Double-Blind, Placebo-Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 16450. https://doi.org/10.3390/ijerph192416450
Rheu K-M, Lee B-J, Son W-H, Kim D-S, Park H-T, Ha M-S, Gong B-H, Jeon B-H. Effect of Fermented Sarco Oyster (Crassostrea gigas) Extract on Muscle Strength Enhancement in Postmenopausal Females: A Randomized, Double-Blind, Placebo-Controlled Trial. International Journal of Environmental Research and Public Health. 2022; 19(24):16450. https://doi.org/10.3390/ijerph192416450
Chicago/Turabian StyleRheu, Kyoung-Min, Bae-Jin Lee, Woo-Hyeon Son, Dong-Seok Kim, Hyun-Tae Park, Min-Seong Ha, Byong-Hak Gong, and Byeong-Hwan Jeon. 2022. "Effect of Fermented Sarco Oyster (Crassostrea gigas) Extract on Muscle Strength Enhancement in Postmenopausal Females: A Randomized, Double-Blind, Placebo-Controlled Trial" International Journal of Environmental Research and Public Health 19, no. 24: 16450. https://doi.org/10.3390/ijerph192416450
APA StyleRheu, K.-M., Lee, B.-J., Son, W.-H., Kim, D.-S., Park, H.-T., Ha, M.-S., Gong, B.-H., & Jeon, B.-H. (2022). Effect of Fermented Sarco Oyster (Crassostrea gigas) Extract on Muscle Strength Enhancement in Postmenopausal Females: A Randomized, Double-Blind, Placebo-Controlled Trial. International Journal of Environmental Research and Public Health, 19(24), 16450. https://doi.org/10.3390/ijerph192416450