
Hyperkalemia and Electrocardiogram Manifestations in End-Stage Renal Disease

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Palmer, B. Managing hyperkalemia caused by inhibitors of the renin-angiotensin-aldosterone system. N. Engl. J. Med. 2014, 351, 585–592. [Google Scholar] [CrossRef] [PubMed]
- Lazich, I.; Bakris, G.L. Prediction and Management of Hyperkalemia Across the Spectrum of Chronic Kidney Disease. Semin. Nephrol. 2014, 34, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Hollander-Rodriguez, J.C.; Clavert, J.F., Jr. Hyperkalemia. Am. Fam. Physician 2006, 73, 283–290. [Google Scholar] [PubMed]
- Jain, N.; Kotla, S.; Little, B.; Weideman, R.A.; Brilakis, E.S.; Reilly, R.F.; Banerjee, S. Predictors of hyperkalemia and death in patients with cardiac and renal disease. Am. J. Cardiol. 2012, 109, 1510–1513. [Google Scholar] [CrossRef] [PubMed]
- Lehnhardt, A.; Kemper, M.J. Pathogenesis, diagnosis and management of hyperkalemia. Pediatr. Nephrol. 2011, 26, 377–384. [Google Scholar] [CrossRef]
- Putcha, N.; Allon, M. Management of hyperkalemia in dialysis patients. Semin. Dial. 2007, 20, 431–439. [Google Scholar] [CrossRef]
- Sarafidis, P.A.; Blacklock, R.; Wood, E.; Rumjon, A.; Simmonds, S.; Fletcher-Rogers, J.; Ariyanayagam, R.; Al-Yassin, A.; Sharpe, C.; Vinen, K. Prevalence and factors associated with hyperkalemia in predialysis patients followed in a low-clearance clinic. Clin. J. Am. Soc. Nephrol. 2012, 7, 1234–1241. [Google Scholar] [CrossRef]
- Welch, A.; Maroz, N.; Wingo, C.S. Hyperkalemia: Getting to the heart of the matter. Nephrol. Dial. Transplant. 2013, 28, 15–16. [Google Scholar] [CrossRef][Green Version]
- Huang, E.S.; Basu, A.; O’Grady, M.; Capretta, J.C. Projecting the Future Diabetes Population Size and Related Costs for the U.S. Diabetes Care 2009, 32, 2225–2229. [Google Scholar] [CrossRef]
- Rossignol, P.; Dobre, D.; McMurray, J.J.; Swedberg, K.; Krum, H.; van Veldhuisen, D.J.; Shi, H.; Messig, M.; Vincent, J.; Girerd, N.; et al. Incidence, determinants, and prognostic significance of hyperkalemia and worsening renal function in patients with heart failure receiving the mineralocorticoid receptor antagonist eplerenone or placebo in addition to optimal medical therapy: Results from the Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure (EMPHASIS-HF). Circ. Heart Fail. 2014, 7, 51–58. [Google Scholar]
- Desai, A.S. Hyperkalemia in patients with heart failure: Incidence, prevalence, and management. Curr. Heart Fail. Rep. 2009, 6, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Hoerger, T.J.; Simpson, S.A.; Yarnoff, B.O.; Pavkov, M.E.; Burrows, N.R.; Saydah, S.H.; Williams, D.E.; Zhou, X. The Future Burden of CKD in the United States: A Simulation Model for the CDC CKD Initiative. Am. J. Kidney Dis. 2015, 65, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Einhorn, L.M.; Zhan, M.; Walker, L.D.; Moen, M.F.; Seliger, S.L.; Weir, M.R.; Fink, J.C. The frequency of hyperkalemia and its significance in chronic kidney disease. Arch. Intern. Med. 2009, 169, 1156–1162. [Google Scholar] [CrossRef] [PubMed]
- Latts, L.M.; Reaven, N.L.; Funk, S.E.; McGaughey, K.J.; Adamson, R.R. Hyperkalemia is prevalent in patients with cardiorenal comorbidities. In Proceedings of the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) 20th Annual International Meeting, Philadelphia, PA, USA, 16–20 May 2015. [Google Scholar]
- El Sherif, N.; Turitto, G. Electrolyte disorders and arrhythmogenesis. Cardiol. J. 2011, 18, 233–245. [Google Scholar] [PubMed]
- Lott, C.; Truhlář, A.; Alfonzo, A.; Barelli, A.; González-Salvado, V.; Hinkelbein, J.; Nolan, J.P.; Paal, P.; Perkins, G.D.; Thies, K.C.; et al. ERC Special Circumstances Writing Group Collaborators. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation 2021, 161, 152–219. [Google Scholar] [CrossRef]
- Sterns, R.H.; Grieff, M.; Bernstein, P. Treatment of hyperkalemia: Something old, something new. Kidney Int. 2016, 89, 546–554. [Google Scholar] [CrossRef]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Adult Basic and Advanced Life Support Writing Group. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142 (Suppl. 2), S366–S468. [Google Scholar] [CrossRef]
- Goyal, A.; Spertus, J.A.; Gosch, K.; Venkitachalam, L.; Jones, P.G.; Van den Berghe, G.; Kosiborod, M. Serum potassium levels and mortality in acute myocardial infarction. JAMA 2012, 307, 157–164. [Google Scholar] [CrossRef]
- Singer, A.; Thode, H.C.; Peacock, W.F. A retrospective study of emergency department potassium disturbances: Severity, treatment, and outcomes. Clin. Exp. Emerg. Med. 2017, 4, 73–79. [Google Scholar] [CrossRef]
- Medford-Davis, L.; Rafique, Z. Derangements of potassium. Emerg. Med. Clin. N. Am. 2014, 32, 329–347. [Google Scholar] [CrossRef]
- Mushiyakh, Y.; Dangaria, H.; Qavi, S.; Ali, N.; Pannone, J.; Tompkins, D. Treatment and pathogenesis of acute hyperkalemia. J. Community Hosp. Intern. Med. Perspect. 2012, 1, 63–72. [Google Scholar]
- An, J.N.; Lee, J.P.; Jeon, H.J.; Kim, D.H.; Oh, Y.K.; Kim, Y.S.; Lim, C.S. Severe hyperkalemia requiring hospitalization: Predictors of mortality. Crit. Care 2012, 16, R225. [Google Scholar] [CrossRef] [PubMed]
- Parham, W.A.; Mehdirad, A.A.; Biermann, K.M.; Fredman, C.S. Hyperkalemia revisited. Tex. Heart Inst. J. 2006, 33, 40–47. [Google Scholar] [PubMed]
- Braun, H.A.; Surawicz, B.; Bellet, S. T waves in hyperpotassemia; their differentiation from simulating T waves in other conditions. Am. J. Med. Sci. 1955, 230, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Diercks, D.B.; Shumaik, G.M.; Harrigan, R.A.; Brady, W.J.; Chan, T.C. Electrocardiographic manifestations: Electrolyte abnormalities. J. Emerg. Med. 2004, 27, 153–160. [Google Scholar] [CrossRef]
- Dittrich, K.L.; Walls, R.M. Hyperkalemia: ECG manifestations and clinical considerations. J. Emerg. Med. 1986, 4, 449–455. [Google Scholar] [CrossRef]
- Mattu, A.; Brady, W.J.; Robinson, D.A. Electrocardiographic manifestations of hyperkalemia. Am. J. Emerg. Med. 2000, 18, 721–729. [Google Scholar] [CrossRef]
- McIntyre, W.F.; Femenia, F.; Arce, M.; Perez-Riera, A.R.; Baranchuk, A. Importance of early electrocardiographic recognition and timely management of hyperkalemia in geriatric patients. Exp. Clin. Cardiol. 2011, 16, 47–50. [Google Scholar]
- Von Knorring, J.; Kuhlback, B. Correlation between the hyperkalaemic ECG-changes and the potassium, magnesium and calcium levels in the serum in renal failure. Acta Med. Scand. 1967, 182, 539–547. [Google Scholar] [CrossRef]
- Tarail, R. Relation of abnormalities in concentration of serum potassium to electrocardiographic disturbances. Am. J. Med. 1948, 5, 828–837. [Google Scholar] [CrossRef]
- Szerlip, H.M.; Weiss, J.; Singer, I. Profound hyperkalemia without electrocardiographic manifestations. Am. J. Kidney Dis. 1986, 7, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Green, D.; Green, H.D.; New, D.I.; Kalra, P.A. The clinical significance of hyperkalaemia-associated repolarization abnormalities in end-stage renal disease. Nephrol. Dial. Transplant. 2013, 28, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Ngugi, N.N.; McLigeyo, S.O.; Kayima, J.K. Treatment of hyperglycaemia by altering the transcellular gradient in patients with renal failure: Effect of various therapeutic approaches. East Afr. Med. J. 1997, 74, 503–509. [Google Scholar] [PubMed]
- Montague, B.T.; Ouellette, J.R.; Buller, G.K. Retrospective review of the frequency of ECG changes in hyperkalemia. Clin. J. Am. Soc. Nephrol. 2008, 3, 324–330. [Google Scholar] [CrossRef]
- Durfey, N.; Lehnhof, B.; Bergeson, A.; Durfey, S.; Leytin, V.; McAteer, K.; Schwam, E.; Valiquet, J. Severe hyperkalemmia: Can the electrocardiogram risk stratify for short-term adverse events? West. J. Emerg. Med. 2017, 18, 963–971. [Google Scholar] [CrossRef]
- Aslam, S.; Friedman, E.A.; Ifudu, O. Electrocardiography is unreliable in detecting potentially lethal hyperkalaemia in haemodialysis patients. Nephrol. Dial. Transplant. 2002, 17, 1639–1642. [Google Scholar] [CrossRef]
- Nemati, E.; Taheri, S. Electrocardiographic manifestations of hyperkalemia in hemodialysis patients. Saudi J. Kidney Dis. Transpl. 2010, 21, 471–477. [Google Scholar]
- Tarif, N.; Yamani, H.; Bakhsh, A.J.; Al-Wakeel, J.S.; Sulaimani, F.; Memon, N.A.; Al Suwaida, A.K. Electrocardiography and serum potassium before and after hemodialysis sessions. Saudi J. Kidney Dis. Transpl. 2008, 19, 47–53. [Google Scholar]
- Attia, Z.; DeSimone, C.V.; Dillon, J.J.; Sapir, Y.; Somers, V.K.; Dungan, J.L.; Bruce, C.J.; Ackerman, M.J.; Asirvatham, S.J.; Striemer, B.L.; et al. Novel Bloodless Potassium Determination Using a Signal-Processed Singnal-Processed Single-Lead ECG. J. Am. Heart Assoc. 2016, 5, e002746. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value (%) |
|---|---|
| Age, years | |
| Mean ± SD | 46 ± 15 |
| Gender | |
| Male | 57 |
| Female | 39 |
| Race (Ethnicity) | |
| Hispanic | 89 (92.70) |
| Asian | 3 (3.13) |
| Black | 4 (4.17) |
| ECG Characteristics | |
| Normokalemia (K ≤ 5.3 mEq/L) | 10 (10.40) |
| Hyperkalemia (K ≥ 5.3 mEq/L) | 86 (89.60) |
| Patient Visits | 476 |
| Normokalemia (K ≤ 5.3 mEq/L) | 50 (10.50) |
| Hyperkalemia (K ≥ 5.3 mEq/L) | 426 (89.50) |
| Mean Serum Electrolytes ± SD | |
| Potassium | 6.20 ± 0.77 |
| Ionized Calcium | 0.97 ± 0.15 |
| Sodium | 135.90 ± 7.56 |
| Chloride | 107 ± 5.28 |
| Bicarbonate | 20.30 ± 4.32 |
| Glucose | 110.30 ± 49.00 |
| Blood Urea Nitrogen | 104.80 ± 29.40 |
| Creatinine | 12.40 ± 7.69 |
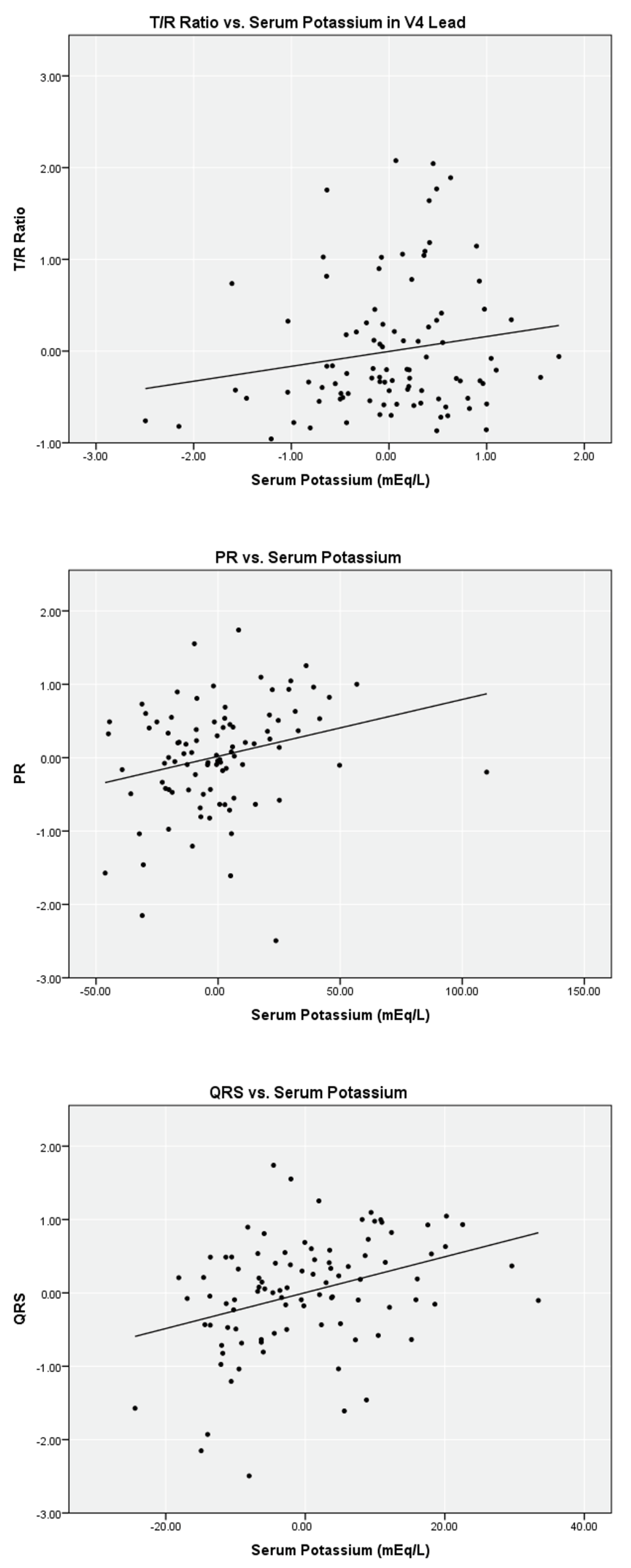
| Sample Size (N) | ECG Characteristic | Correlation Coefficient | Adjusted R Square | p-Value (2-Tailed) |
|---|---|---|---|---|
| T/R Ratio | ||||
| Lead | ||||
| n = 95 | V2 | 0.23 | 0.04 | 0.04 |
| n = 94 | V3 | 0.17 | 0.02 | 0.02 |
| n = 95 | V4 | 0.17 | 0.02 | 0.02 |
| n = 92 | PR | 0.26 | 0.06 | 0.06 |
| n = 95 | QRS | 0.35 | 0.12 | 0.12 |
| T/R Ratio | ||||
| Lead | ||||
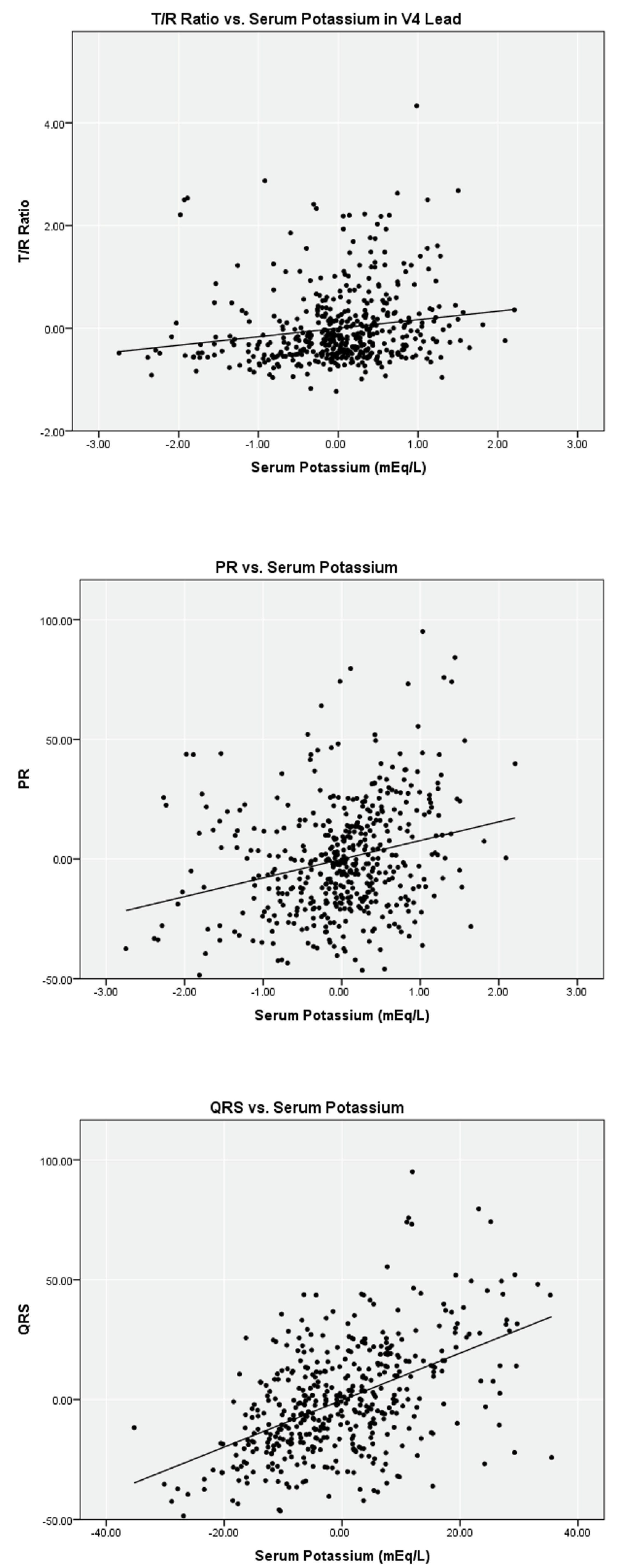
| n = 466 | V2 | 0.21 | 0.04 | <0.01 |
| n = 472 | V3 | 0.17 | 0.03 | <0.01 |
| n = 465 | V4 | 0.17 | 0.03 | <0.01 |
| n = 457 | PR | 0.29 | 0.06 | <0.01 |
| n = 469 | QRS | 0.31 | 0.09 | <0.01 |
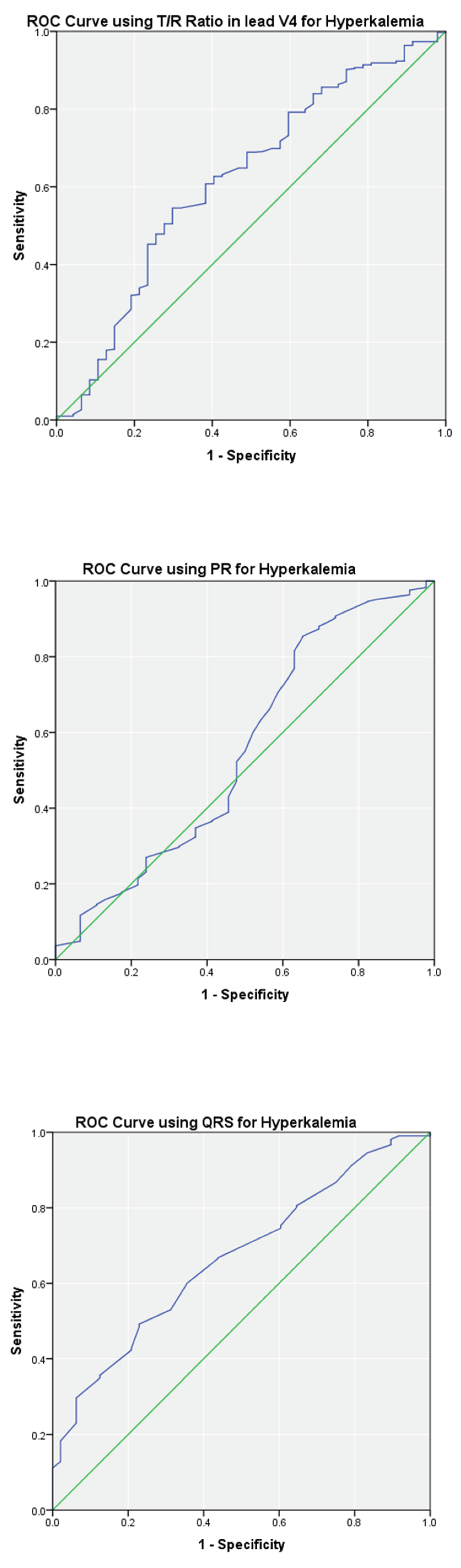
| Sample Size (N) | ECG Test Variable | Cutoff Threshold (Optimal) | Sensitivity (Optimal) | Specificity (Optimal) | Positive Predictive Value (Optimal) | Negative Predictive Value (Optimal) | Area Under ROC Curve (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|---|
| T/R Ratio | ||||||||
| Lead | ||||||||
| n = 95 | V2 | ≥0.75 (≥0.48) | 0.68 (0.82) | 0.80 (0.70) | 0.97 (0.96) | 0.23 (0.33) | 0.80 (0.65–0.94) | <0.01 |
| n = 94 | V3 | ≥0.75 (≥0.43) | 0.67 (0.91) | 0.60 (0.60) | 0.93 (0.95) | 0.18 (0.43) | 0.73 (0.55–0.92) | 0.02 |
| n = 95 | V4 | ≥0.75 (≥0.37) | 0.43 (0.73) | 0.78 (0.67) | 0.95 (0.96) | 0.13 (0.21) | 0.73 (0.54–0.92) | 0.02 |
| n = 92 | PR | ≥200 ms (≥144 ms) | 0.08 (0.86) | 1.00 (0.56) | 1.00 (0.95) | 0.11 (0.29) | 0.69 (0.48–0.90) | 0.07 |
| n = 95 | QRS | ≥120 ms (≥82 ms) | 0.02 (0.81) | 1.00 (0.60) | 1.00 (0.95) | 0.11 (0.27) | 0.71 (0.52–0.90) | 0.03 |
| T/R Ratio | ||||||||
| Lead | ||||||||
| n = 466 | V2 | ≥0.75 (≥0.57) | 0.67 (0.76) | 0.58 (0.52) | 0.93 (0.93) | 0.17 (0.20) | 0.68 (0.61–0.76) | <0.01 |
| n = 472 | V3 | ≥0.75 (≥0.58) | 0.64 (0.75) | 0.60 (0.56) | 0.93 (0.94) | 0.16 (0.22) | 0.68 (0.59–0.76) | <0.01 |
| n = 465 | V4 | ≥0.75 (≥0.51) | 0.39 (0.55) | 0.77 (0.70) | 0.94 (0.94) | 0.12 (0.15) | 0.62 (0.53–0.71) | <0.01 |
| n = 457 | PR | ≥200 ms (≥144) | 0.08 (0.85) | 0.94 (0.35) | 0.91 (0.92) | 0.10 (0.21) | 0.55 (0.46–0.65) | 0.23 |
| n = 469 | QRS | ≥120 ms (≥92) | 0.11 (0.49) | 1.00 (0.77) | 1.00 (0.95) | 0.10 (0.15) | 0.67 (0.59–0.74) | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rafique, Z.; Hoang, B.; Mesbah, H.; Pappal, R.; Peacock, F.W.; Juarez-Vela, R.; Szarpak, L.; Kuo, D.C. Hyperkalemia and Electrocardiogram Manifestations in End-Stage Renal Disease. Int. J. Environ. Res. Public Health 2022, 19, 16140. https://doi.org/10.3390/ijerph192316140
Rafique Z, Hoang B, Mesbah H, Pappal R, Peacock FW, Juarez-Vela R, Szarpak L, Kuo DC. Hyperkalemia and Electrocardiogram Manifestations in End-Stage Renal Disease. International Journal of Environmental Research and Public Health. 2022; 19(23):16140. https://doi.org/10.3390/ijerph192316140
Chicago/Turabian StyleRafique, Zubaid, Bryan Hoang, Heba Mesbah, Ryan Pappal, Frank W. Peacock, Raul Juarez-Vela, Lukasz Szarpak, and Dick C. Kuo. 2022. "Hyperkalemia and Electrocardiogram Manifestations in End-Stage Renal Disease" International Journal of Environmental Research and Public Health 19, no. 23: 16140. https://doi.org/10.3390/ijerph192316140
APA StyleRafique, Z., Hoang, B., Mesbah, H., Pappal, R., Peacock, F. W., Juarez-Vela, R., Szarpak, L., & Kuo, D. C. (2022). Hyperkalemia and Electrocardiogram Manifestations in End-Stage Renal Disease. International Journal of Environmental Research and Public Health, 19(23), 16140. https://doi.org/10.3390/ijerph192316140